Signage Interventions for Stair Climbing at Work: More than 700,000 Reasons for Caution



Abstract
:1. Introduction
1.1. Background
1.2. Estimates of the Effectiveness of Signage Interventions at Work
1.3. Effects of Pedestrian Movement on Stair Usage
1.4. Stair Climbing or Stair Usage
1.5. The Current Study
2. Methods
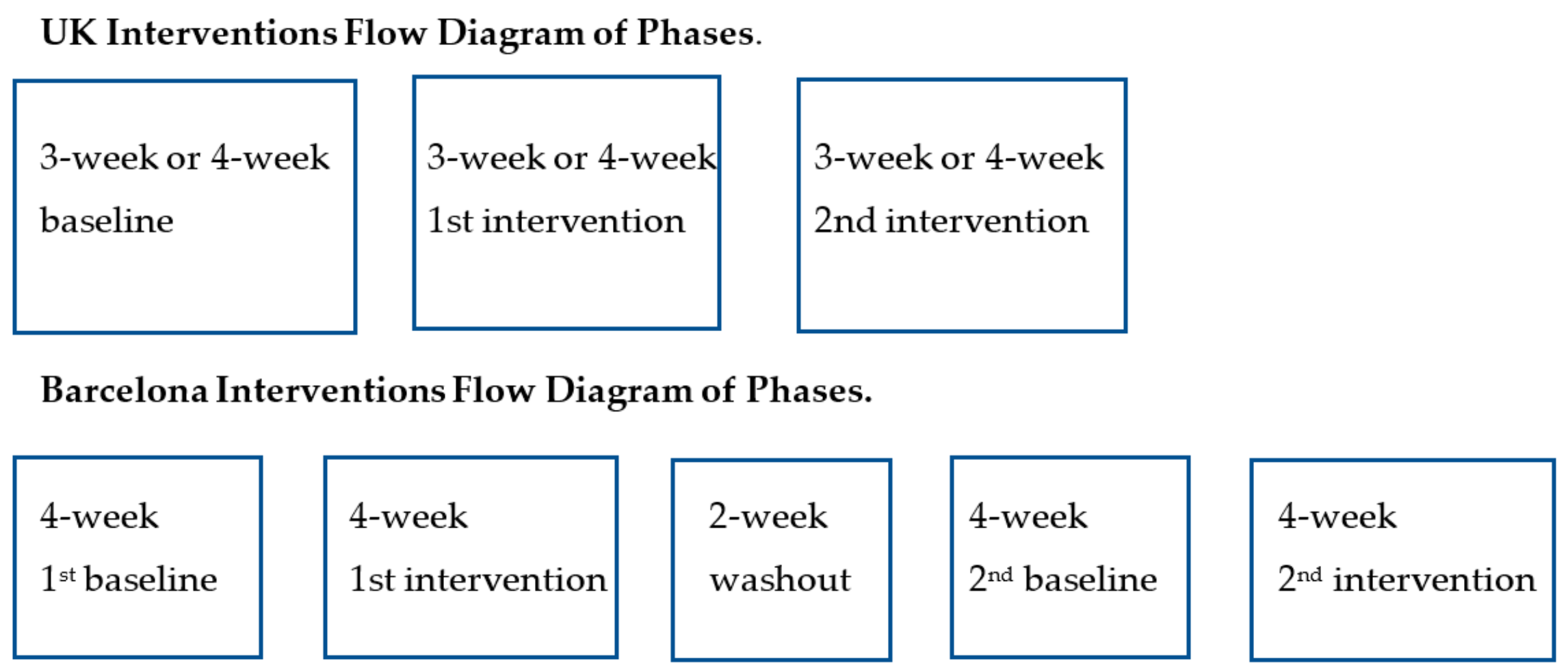
2.1. Interventions in the UK
2.2. Interventions in Barcelona, Spain
2.3. Data Reduction and Analyses
3. Results
3.1. Intervention in the UK
3.2. Intervention in Barcelona
4. Discussion
4.1. Effects of Signage Interventions on Stair Use
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- WHO. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.F.; Martin, B.W. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Bellicha, A.; Kieusseian, A.; Fontvieille, A.; Tataranni, A.; Charreire, H.; Oppert, J. Stair-use interventions in worksites and public settings—A systematic review of effectiveness and external validity. Prev. Med. 2015, 70, 3–13. [Google Scholar] [CrossRef]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating more physically active communities. Ann. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.M.; Paffenbarger, R.S. Physical activity and stroke incidence: The Harvard Alumni Health Study. Stroke 1998, 29, 2049–2054. [Google Scholar] [CrossRef] [PubMed]
- Paffenbarger, R.S., Jr.; Wing, A.L.; Hyde, R.T. Physical activity as an Index of heart attack risk in college alumni. Am. J. Epidemiol. 1978, 108, 161–175. [Google Scholar] [CrossRef]
- Boreham, C.A.G.; Kennedy, R.A.; Murphy, M.H.; Tully, M.; Wallace, W.F.M.; Young, I. Training effects of short bouts of stair climbing on cardiorespiratory fitness, blood lipids, and homocysteine in sedentary young women. Br. J. Sports Med. 2005, 39, 590–593. [Google Scholar] [CrossRef] [PubMed]
- Boreham, C.A.G.; Wallace, W.F.M.; Nevill, A. Training effects of accumulated daily stair-climbing exercise in previously sedentary young women. Prev. Med. 2000, 30, 277–281. [Google Scholar] [CrossRef]
- Kennedy, R.A.; Boreham, C.A.G.; Murphy, M.H.; Young, I.S.; Mutrie, N. Evaluating the effects of a low volume stair climbing programme on measures of health-related fitness in sedentary office workers. J. Sports Sci. Med. 2007, 6, 448–454. [Google Scholar]
- Meyer, P.; Kayser, B.; Kossovsky, M.P.; Sigaud, P.; Carballo, D.; Keller, P.F.; Eric Martin, X.; Farpour-Lambert, N.; Pichard, C.; Mach, F. Stairs instead of elevators at workplace: Cardioprotective effects of a pragmatic intervention. Eur. J. Cardiovasc. Prev. Rehab. 2010, 17, 569–575. [Google Scholar] [CrossRef]
- Centres for Disease Control—Workplace Health—Implementation—Physical Activity. 2013. Available online: www.cdc.gov/workplacehealthpromotion/implementation/topics/physical-activity.html (accessed on 24 August 2018).
- National Institute for Health and Clinical Excellence Public Health Guidance 13. Workplace Health Promotion. 2008. Available online: www.nice.org.uk (accessed on 24 August 2018).
- Kerr, J.; Eves, F.; Carroll, D. Six-month observational study of prompted stair climbing. Prev. Med. 2001, 33, 422–427. [Google Scholar] [CrossRef]
- Bauman, A.E.; Milton, K.; Kariuki, M.; Fedel, K.; Lewicka, M. Is there sufficient evidence regarding signage-based stair-use interventions? A sequential meta-analysis. BMJ Open 2016, 7, e012459. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, R.; McKenzie, S.; Allender, S.; Brown, K.; Foulkes, C. Systematic review of incidental physical activity community interventions. Prev. Med. 2014, 67, 46–64. [Google Scholar] [CrossRef] [PubMed]
- Nocon, M.; Muller-Riemenschneider, F.; Nitzschke, K.; Willich, S.N. Increasing physical activity with point-of-choice prompts—A systematic review. Scand. J. Public Health 2010, 38, 633–638. [Google Scholar] [CrossRef]
- Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Scientific Report; Promoting Regular Physical Activity; Department of Health and Human Services: Washington, DC, USA, 2018; Chapter 11; Part F, pp. 1–104.
- Eves, F.F. All choices are not equal; Effects of context on point-of-choice prompts for stair climbing. Obes. Rev. 2008, 9, 83–84. [Google Scholar] [CrossRef] [PubMed]
- Eves, F.F. Point-of-decision prompts to increase stair use. Am. J. Prev. Med. 2010, 38, 573–574. [Google Scholar] [CrossRef] [PubMed]
- Bellicha, A.; Kieusseian, A.; Fontvieille, A.; Tataranni, A.; Copini, N.; Charreire, H.; Oppert, J. A multistage controlled intervention to increase stair climbing at work: Effectiveness and process evaluation. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 47. [Google Scholar] [CrossRef] [PubMed]
- Blake, H.; Lee, S.; Stanton, T.; Gorely, T. Workplace intervention to promote stair-use in an NHS setting. Int. J. Workplace Health Manag. 2008, 1, 162–175. [Google Scholar] [CrossRef]
- Boutelle, K.N.; Jeffrey, R.W.; Murray, D.M.; Schmitz, M.K. Using signs, artwork, and music to promote stair use in a public building. Am. J. Public Health 2001, 91, 2004–2006. [Google Scholar] [CrossRef]
- Cohen, S.M. Examining the effects of a health promotion intervention on the use of stairs. JASNH 2013, 10, 17–24. [Google Scholar]
- Coleman, K.J.; Gonzalez, E.C. Promoting stair use in a U.S. Mexico border community. Am. J. Public Health 2001, 91, 2007–2009. [Google Scholar] [CrossRef]
- Cooley, P.D.; Foley, S.J.; Magnussen, C.G. Increasing stair usage in a professional workplace: A test of the efficacy of positive and negative message prompts to change pedestrian choices. Health Promot. J. Austr. 2008, 19, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Eves, F.F.; Olander, E.K.; Webb, O.J.; Griffin, C.; Chambers, J. Likening stairs in buildings to climbing a mountain: Self-reports of expected effects on stair climbing and objective measures of effectiveness. Psychol. Sport Exerc. 2012, 13, 170–176. [Google Scholar] [CrossRef]
- Kerr, J.; Eves, F.; Carroll, D. Can posters prompt stair use in a worksite environment? J. Occup. Health 2001, 43, 205–207. [Google Scholar] [CrossRef]
- Marshall, A.L.; Bauman, A.E.; Patch, C.; Wilson, J.; Chen, J. Can motivational signs prompt increases in incidental physical activity in an Australian health-care facility? Health Educ. Res. 2002, 17, 743–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olander, E.K.; Eves, F.F. Elevator availability and its impact on stair use in a workplace. J. Environ. Psychol. 2011, 31, 200–206. [Google Scholar] [CrossRef]
- Eves, F.F.; Lewis, A.L.; Griffin, C. Modeling effects of stair width on rates of stair climbing in a train station. Prev. Med. 2008, 47, 270–272. [Google Scholar] [CrossRef]
- Webb, O.J.; Eves, F.F.; Kerr, J. A statistical summary of mall-based stair-climbing interventions. J. Phys. Act. Health 2011, 8, 558–565. [Google Scholar] [CrossRef]
- Lewis, A.L.; Eves, F.F. Prompts to increase stair climbing in stations; the effect of message complexity. J. Phys. Act. Health 2012, 9, 954–961. [Google Scholar] [CrossRef]
- Eves, F.F.; Webb, O.J.; Griffin, C.; Chambers, J. A Multi-component intervention targeting calorific expenditure with stair climbing; Effects on behavior, attitudes and intentions. BMC Pub. Health 2012, 12, 423. [Google Scholar] [CrossRef]
- Eves, F.F.; Webb, O.J. Worksite interventions to increase stair climbing; reasons for caution. Prev. Med. 2006, 43, 4–7. [Google Scholar] [CrossRef]
- Eves, F.F.; Webb, O.J.; Mutrie, N. A workplace intervention to promote stair climbing: Greater effects in the overweight. Obesity 2006, 14, 2210–2216. [Google Scholar] [CrossRef] [PubMed]
- Teh, K.C.; Aziz, A.R. Heart rate, oxygen uptake, and energy cost of ascending and descending the stairs. Med. Sci. Sports Exerc. 2002, 34, 695–699. [Google Scholar] [PubMed]
- Thomas, E.L.; Puig Ribera, A.; Senye-Mir, A.; Greenfield, S.; Eves, F.F. Testing messages to promote stair climbing at work. Int. J. Workplace Health Manag. 2015, 8, 189–205. [Google Scholar] [CrossRef]
- Olander, E.K.; Eves, F.F. Effectiveness and cost of two stair climbing interventions—Less is more. Am. J. Health Prom. 2011, 25, 231–236. [Google Scholar] [CrossRef]
- Lewis, A.; Eves, F.F. Prompt before the choice is made; Effects of a stair climbing intervention in university buildings. Br. J. Health Psychol. 2012, 17, 631–643. [Google Scholar] [CrossRef]
- Chinn, S. A simple method for converting an odds ratio to effect size for use in meta-analysis. Stat. Med. 2000, 19, 3127–3131. [Google Scholar] [CrossRef]
- Lewis, A.L.; Eves, F.F. Specific effects of a calorie-based intervention in overweight commuters. Ann. Behav. Med. 2011, 42, 257–261. [Google Scholar] [CrossRef]
- Lewis, A.L.; Eves, F.F. Testing the theory underlying the success of point-of-choice prompts: A multi-component stair climbing intervention. Psychol. Sport Exerc. 2012, 13, 126–132. [Google Scholar] [CrossRef]
- Webb, O.J.; Cheng, T.F. An informational stair climbing intervention with greater effects in overweight pedestrians. Health Educ. Res. 2010, 25, 936–944. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Self-Efficacy: The Exercise of Control; W.H. Freeman Press: Basingstoke, UK, 1997. [Google Scholar]
- McAuley, E. Self-efficacy and the maintenance of exercise participation in older adults. J. Behav. Med. 1993, 16, 103–113. [Google Scholar] [CrossRef]
- Sniehotta, F.F.; Scholz, U.; Schwarzer, R. Bridging the intention-behaviour gap: Planning, self-efficacy and action control in the adoption and maintenance of physical exercise. Psychol. Health 2005, 20, 143–160. [Google Scholar] [CrossRef]
- Trost, S.G.; Owen, N.; Bauman, A.E.; Sallis, J.F.; Brown, W. Correlates of adults’ participation in physical activity: Review and update. Med. Sci. Sports Exerc. 2002, 34, 1996–2001. [Google Scholar] [CrossRef] [PubMed]
- Eves, F.F. Is there any Proffitt in stair climbing? A headcount of studies testing for demographic differences in choice of stairs. Psychonom. Bull. Rev. 2014, 21, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Cohen, D.; Shi, Y.; Pearson, M.; Sturm, R. Economic analysis of physical activity interventions. Am. J. Prev. Med. 2011, 40, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Dolan, M.S.; Weiss, L.A.; Lewis, R.A.; Pietrobelli, A.; Heo, M.; Faith, M.S. ‘Take the stairs instead of the escalator’: Effect of environmental prompts on community stair use and implications for a national ‘Small Steps’ campaign. Obes. Rev. 2006, 7, 25–32. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Behavior | Baseline | Intervention 1 | Intervention 2 |
|---|---|---|---|
| Stair climbing (%) | 45.1 a (44.7, 45.5) | 43.3 (42.8, 43.7) | 44.8 (44.4, 45.2) |
| Stair descending (%) | 67.7 (67.4, 68.1) | 69.8 (69.4, 70.2) | 70.1 (69.7, 70.5) |
| Variable | Up Step 1 | Up Step 2 | Up Step 3 | Down Step 1 | Down Step 2 | Down Step 3 |
|---|---|---|---|---|---|---|
| 1st intervention (baseline) | 0.926 a *** (0.906, 0.946) | 0.919 *** (0.899, 0.939) | 0.989 (0.968, 1.011) | 1.101 *** (1.075, 1.129) | 1.098 *** (1.070, 1.124) | 1.098 *** (1.069, 1.125) |
| Traffic up (min−1) | - | 0.911 *** (0.906, 0.915) | 0.902 *** (0.898, 0.908) | - | 0.934 *** (0.929, 0.940) | 0.930 *** (0.924, 0.937) |
| Traffic down (min−1) | - | 1.027 *** (1.020, 1.033) | 1.042 *** (1.035, 1.049) | - | 1.031 *** (1.023, 1.037) | 1.029 *** (1.022, 1.035) |
| Time of day (hour) | - | - | 0.974 *** (0.970, 0.978) | - | - | 1.010 *** (1.006, 1.015) |
| Number of elevators | - | - | 0.659 *** (0.640, 0.677) | - | - | 0.655 *** (0.633, 0.677) |
| Number of floors | - | - | 0.761 *** (0.754, 0.770) | - | - | 0.952 *** (0.942, 0.963) |
| Variable | Up Step 1 | Up Step 2 | Up Step 3 | Down Step 1 | Down Step 2 | Down Step 3 |
|---|---|---|---|---|---|---|
| 2nd intervention (1st intervention) | 1.064 a *** (1.042, 1.088) | 1.082 *** (1.059, 1.104) | 1.059 ** (1.037, 1.082) | 1.017 (0.993, 1.041) | 1.019 (0.996, 1.044) | 1.014 (0.991, 1.039) |
| Traffic up (min−1) | - | 0.886 *** (0.881, 0.890) | 0.876 *** (0.871, 0.881) | - | 0.911 *** (0.905, 0.916) | 0.908 *** (0.902, 0.913) |
| Traffic down (min−1) | - | 1.009 ** (1.003, 1.016) | 1.031 *** (1.023, 1.039) | - | 1.016 *** (1.009, 1.022) | 1.014 *** (1.007, 1.020) |
| Time of day (hour) | - | - | 0.975 *** (0.970, 0.978) | - | - | 1.011 *** (1.006, 1.015) |
| Number of elevators | - | - | 0.694 *** (0.675, 0.714) | - | - | 0.689 *** (0.668, 0.712) |
| Number of floors | - | - | 0.751 *** (0.744, 0.758) | - | - | 0.978 *** (0.968, 0.989) |
| Behavior | Baseline 1 | Intervention 1 | Washout Period | Intervention 2 |
|---|---|---|---|---|
| Stair climbing.30 min−1 | 7.22 a (6.82, 7.61) | 8.09 (7.79, 8.39) | 8.56 (8.17, 8.94) | 8.70 (8.38, 9.03) |
| Stair descent.30 min−1 | 10.37 (9.95, 10.81) | 11.11 (10.81, 11.42) | 10.80 (10.43, 11.17) | 11.16 (10.83, 11.48) |
| Variable | Up Step 1 | Up Step 2 | Up Step 3 | Down Step 1 | Down Step 2 | Down Step 3 |
|---|---|---|---|---|---|---|
| 1st intervention (baseline) | 0.092 ** a (0.026, 0.164) | 0.047 (−0.003, 0.098) | 0.040 (−0.009, 0.086) | 0.118 *** (0.048, 0.183) | 0.069 * (0.005, 0.131) | 0.058 * (0.002, 0.115) |
| Elevator traffic in direction of travel (30 min−1) | - | 0.723 *** (0.689, 0.758) | 0.608 *** (0.574, 0.643) | - | 0.483 *** (0.451, 0.517) | 0.423 *** (0.384, 0.462) |
| Elevator traffic opposite to direction of travel (30 min−1) | - | −0.115 *** (−0.143, −0.089) | −0.100 *** (−0.129, −0.071) | - | 0.062 ** (0.029, 0.094) | −0.000 (−0.048, 0.045) |
| Stair traffic opposite to direction of travel (30 min−1) | - | - | 0.130 *** (0.098, 0.157) | - | - | 0.198 *** (0.152, 0.241) |
| Time of day (hour) | - | - | −0.253 *** (−0.275, −0.230) | - | - | 0.192 *** (0.163, 0.221) |
| Change in R2 | 0.002 ** | 0.466 *** | 0.058 *** | 0.003 ** | 0.236 *** | 0.037 *** |
| Variable | Up Step 1 | Up Step 2 | Up Step 3 | Down Step 1 | Down Step 2 | Down Step 3 |
|---|---|---|---|---|---|---|
| 2nd intervention (washout). | 0.077 ** a (0.016, 0.141) | 0.021 (−0.026, 0.065) | 0.019 (−0.025, 0.063) | 0.114 *** (0.053, 0.175) | 0.065 * (0.018, 0.114) | 0.055 * (0.008, 0.101) |
| Elevator traffic in direction of travel (30 min−1) | - | 0.632 *** (0.598, 0.665) | 0.531 *** (0.501, 0.565) | - | 0.491 *** (0.461, 0.522) | 0.462 *** (0.432, 0.494) |
| Elevator traffic opposite to direction of travel (30 min−1) | - | −0.033 * (−0.059, −0.005) | −0.058 ** (−0.089, −0.028) | - | 0.130 *** (0.103, 0.158) | 0.073 *** (0.035, 0.106) |
| Stair traffic opposite to direction of travel (30 min−1) | - | - | 0.149 *** (0.121, 0.179) | - | - | 0.184 *** (0.152, 0.218) |
| Time of day (hour) | - | - | −0.265 *** (−0.286, −0.244) | - | - | 0.192 *** (0.169, 0.215) |
| Change in R2 | 0.001 ** | 0.415 *** | 0.070 *** | 0.003 ** | 0.340 *** | 0.037 *** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puig-Ribera, A.; Señé-Mir, A.M.; Taylor-Covill, G.A.H.; De Lara, N.; Carroll, D.; Daley, A.; Holder, R.; Thomas, E.; Milà, R.; Eves, F.F. Signage Interventions for Stair Climbing at Work: More than 700,000 Reasons for Caution. Int. J. Environ. Res. Public Health 2019, 16, 3782. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193782
Puig-Ribera A, Señé-Mir AM, Taylor-Covill GAH, De Lara N, Carroll D, Daley A, Holder R, Thomas E, Milà R, Eves FF. Signage Interventions for Stair Climbing at Work: More than 700,000 Reasons for Caution. International Journal of Environmental Research and Public Health. 2019; 16(19):3782. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193782
Chicago/Turabian StylePuig-Ribera, Anna, Anna M. Señé-Mir, Guy A. H. Taylor-Covill, Núria De Lara, Douglas Carroll, Amanda Daley, Roger Holder, Erica Thomas, Raimon Milà, and Frank F. Eves. 2019. "Signage Interventions for Stair Climbing at Work: More than 700,000 Reasons for Caution" International Journal of Environmental Research and Public Health 16, no. 19: 3782. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16193782