Analysis of Health in Environmental Assessments—A Literature Review and Survey with a Focus on Denmark


Abstract
:1. Introduction
2. Materials and Methods
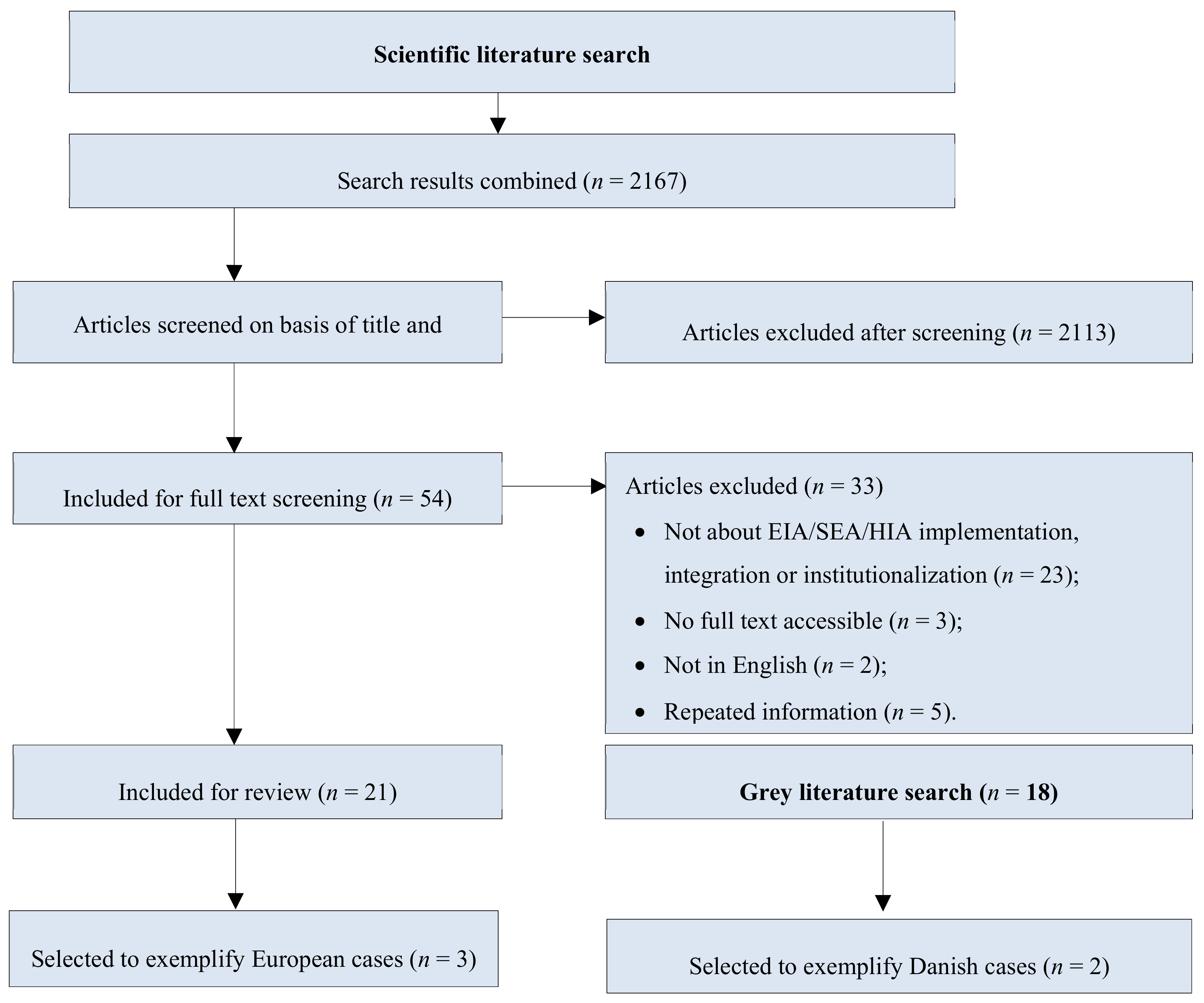
2.1. Literature Review
2.2. Survey
- The survey link was distributed via email to participants of the 2018 one-day workshop “Miljøvurderingsdag” (Environmental Assessment Day) in Denmark. Participants of the workshop were EIA and SEA practitioners and researchers who discussed challenges and opportunities within EIA.
- The link to the survey was shared through the LinkedIn group “HIA—Health Impact Assessment Group”. Members of this group consist of practitioners and researchers in the field of HIA.
- The link to the survey was distributed to all participants of the “Human Health in Environmental Impact Assessment” conference, which took place in March 2019 at the WHO European Centre for Environment and Health office in Germany.
Comparative Analysis
3. Results
3.1. Literature Search
3.1.1. European Environmental Assessments
3.1.2. Danish Environmental Assessments
3.2. Survey
4. Discussion
4.1. Integrating Health into Environmental Assessments
4.2. Engagement of Health Professionals
4.3. Guidance Documents
4.4. Political Support
5. Conclusions
- Additional or enhanced guidance documents,
- Engagement of health professionals in the environmental sector,
- Health-related training, and
- Political support.
Author Contributions
Funding
Conflicts of Interest
Appendix A

Appendix B

{kind=link}
| Health in Environmental Impact Assessment Thank you for taking 10 min time to answer this questionnaire about health and environmental impact assessments. About us: We are two MSc. Public Health students, Sarah Humboldt-Dachroeden and Birgitte Fischer-Bonde at the University of Southern Denmark. As a part of our master thesis we are conducting this survey to identify the needs of practitioners and researchers regarding the inclusion of health into Environmental Impact Assessment. Through the survey we will be able to compare the perceived needs of practitioners and researchers. If you have questions or feedback regarding the survey or our master thesis feel free to contact us via our email addresses [email protected] or [email protected]. By answering the questionnaire, you accept that the data from this survey will be used for the master thesis as well as our future work. This survey is anonymous, and all answers will be handled confidentially. Do you want to see this text in Danish? | |
| Yes | |
| No | |
| If answer “yes” from above: Tak fordi du vil bruge 10 minutter på at svare på vores spørgeskema om sundhed og miljøkonsekvensvurderinger (EIA). Lidt om os: Vi er to kandidatstuderende, Sarah Humboldt-Dachroeden og Birgitte Fischer-Bonde. Vi læser Folkesundhedsvidenskab på Syddansk Universitet. Dette spørgeskema er en del af vores specialeprojekt, hvor vi vil forsøge at klarlægge forskellen mellem praktikere og forskeres opfattelse af behov i forhold til at integrere sundhed i EIAs. Hvis du har spørgsmål eller feedback til spørgeskemaet er du velkommen til at kontakte os på enten [email protected] eller [email protected]. Ved at svare på spørgeskemaet accepterer du, at dine svar må bruges til vores speciale samt i vores fremtidige arbejde. Spørgeskemaet er anonymt, og alle svar vil blive håndteret fortroligt. | |
| Definitions Environmental Impact Assessment (EIA) and Strategical Impact Assessment (SEA), referred to as EIA throughout this survey, are mandatory in the European Union (EU) since they were implemented into EU directives. EIA and SEA are both tools to assess the environmental impacts of plans, programmes and projects (PPPs). They ensure that possible implications on the environment are revealed to support the decision-making process of the PPPs. While EIA is mainly conducted for projects, the SEA is conducted for plans and programmes. Health Impact Assessment (HIA) is a tool, similar in its application method to EIA, for assessing the health impacts of plans, programmes, projects and policies. HIA support decision and policy making with recommendations and they aim to promote and protect health. In contrast to EIA, HIA is mainly conducted on a voluntary basis. Do you want to see this text in Danish? | |
| Yes | |
| No | |
| If answer “yes” from above: Definitioner I spørgeskemaet, som i øvrigt er på engelsk, vil du støde på følgende begreber: EIA: Environmental Impact Assessment eller miljøkonsekvensvurdering på dansk. SEA: Strategic Environmental Assessment eller strategisk miljøvurdering på dansk. Både EIA og SEA er obligatoriske for lande der er medlem af EU. Begge er værktøjer, der vurderer påvirkninger på miljøet af planer, programmer og projekter (PPPs). De er med til at sikre, at eventuelle miljømæssige påvirkninger bliver synliggjorte, hvilket kan være med til at informere beslutninger angående PPPs. EIA bliver primært brugt i forbindelse med projekter, hvor SEA bliver brugt til planer og programmer. HIA: Health Impact Assessment eller sundhedskonsekvensvurdering på dansk. HIA er et værktøj, der i sin anvendelse minder meget om EIA, hvor formålet er at vurdere de sundhedsmæssige påvirkninger af planer, programmer, projekter og politikker. HIA er udviklet for at understøtte beslutningsprocesser samt politik og har til formål at fremme og beskytte folkesundheden. I modsætning til EIAs, bliver HIAs primært udført på frivillig basis. | |
| Q1 How old are you? | |
| Years | |
| Don’t want to answer | |
| Q2 Choose the highest level of education you have obtained | |
| Less than a high school diploma | |
| High school degree or equivalent | |
| Bachelor’s degree | |
| Master’s degree | |
| Doctorate | |
| Other, please specify | |
| Don’t want to answer | |
| Q3 Where are you currently working? | |
| Africa | |
| Antarctica | |
| Asia | |
| Europe | |
| North America | |
| Oceania | |
| South America | |
| Don’t want to answer | |
| Q4 What is the main country you work from? Note: Please write the full name of the country in English. | |
| Country | |
| Don’t want to answer | |
| Q5 Do you consider yourself more as a/an | |
| EIA practitioner | |
| EIA researcher | |
| HIA practitioner | |
| HIA researcher | |
| IA practitioner (other impact assessment), please specify | |
| IA researcher (other impact assessment), please specify | |
| None of the above | |
| If answer “None of the above” from above: Thank you very much for participating in our survey. You are not working with EIA, HIA or other types of impact assessments. Therefore, this survey is not addressed to you. If you have questions or comments, you are welcome to send us an email: [email protected] or [email protected]. Please click “next” to complete the survey and send in your responses. | |
| Q6 How long have you been an EIA/HIA practitioner? (years) | |
| Q7 Where do you work? | |
| National health authority | |
| Regional/local health authority | |
| Regional/local environmental authority | |
| National environmental authority | |
| Health/Environment inspectorate | |
| Public health institute | |
| Environmental institute | |
| Independent public health consultant/private company | |
| Academic unit | |
| HIA licensed assessor | |
| Licensed environmental assessor | |
| International health organisation | |
| International environmental organisation | |
| Environmental consultant / private company | |
| Non-governmental organization (NGO) | |
| Other private company | |
| Other, please specify | |
| Q8 Before this survey, had you heard about Health Impact Assessment (HIA)? | |
| Yes | |
| No | |
| Have heard about it, but not sure what it is | |
| Q9 Do you think HIA should be conducted within EIA? | |
| Yes. Please specify why | |
| No. Please specify why | |
| Maybe, depending on the context | |
| Q10 With which of the below have you worked with? (Unlimited answers) | |
| EIA | |
| SEA | |
| HIA | |
| Integrated, please specify (for example HIA within an EIA) | |
| Other impact assessments, please specify | |
| None of the above | |
| Q11 (Practitioners) Have you ever consulted with public health/health professionals in the process of conducting an EIA? (Only one answer) | |
| Yes | |
| No | |
| Don’t know | |
| Q11 (Researchers) Have you ever assisted in the process of conducting an EIA? (Only one answer) | |
| Yes | |
| No | |
| Don’t know | |
| Q12 (Practitioners) Which areas have you conducted EIAs in? (Unlimited answers) | |
| Agriculture, forestry and fishery | |
| Energy industry | |
| Extractive industry | |
| Other industry (e.g., chemicals, food, minerals, metals, rubber, textile, leather, wood and/or paper industry) | |
| Infrastructure projects | |
| Telecommunications | |
| Tourism and leisure | |
| Waste management | |
| Water management | |
| Sectoral policies | |
| Q12 (Researchers) Which areas have you conducted EIA research in? (Unlimited answers) | |
| Agriculture, forestry and fishery | |
| Energy industry | |
| Extractive industry | |
| Other industry (e.g., chemicals, food, minerals, metals, rubber, textile, leather, wood and/or paper industry) | |
| Infrastructure projects | |
| Telecommunications | |
| Tourism and leisure | |
| Waste management | |
| Water management | |
| Sectoral policies | |
| Q13 Are you aware of the EIA and SEA directives by the European Commission? | |
| Yes | |
| No | |
| Q14 Are you aware of the amendment made regarding health in the EIA Directive 2014/52/EU? | |
| Yes | |
| No | |
| The EU’s EIA Directive 2014/52/EU specifically notes population and human health instead of human beings which was written in the 2011/92/EU directive. Since the directives are a legal act of the EU, they must be translated into national law. All European countries have established regulatory frameworks for EIA and SEA and have implemented/translated them into national law. However, the extent to which the EU member countries have translated the directives into national law varies. Do you want to see this text in Danish? | |
| Yes | |
| No | |
| If answer “yes” from above: Den Europæiske Unions EIA-direktiv 2014/52/EU indeholder specifikt begreberne population health (folkesundhed) og human health (menneskelig sundhed) i stedet for bare human beings (mennesker), hvilket var skrevet i den tidligere udgave af direktivet 2011/92/EU. Eftersom direktiverne er lovmæssigt bindende, skal medlemslandene implementere dem i deres egen lovgivning. Dette har alle medlemslandene gjort, dog i varierende grad inden for de rammer, der er tilladt. | |
| Q15 According to your knowledge, do you know how the EC directives (EIA Directive: 2014/52/EU and SEA Directive: 2001/42/EC) transposed into your country legislation by a statute (law, ordinance, etc.)? | |
| Yes | |
| No | |
| Don’t know | |
| Q16 In the context of EIA/HIA, do you agree with the definition of human health provided by the World Health Organisation: “Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”? | |
| Yes | |
| No | |
| Don’t know | |
| Q17 There is no universally agreed definition of population health. Which of the following definitions do you prefer? | |
| “The health of the population measured by health status indicators; it is influenced by physical, biological, social, and economic factors in the environment, by personal health behaviour, and by access to and effectiveness of health care services” | |
| “The prevailing or aspired level of health in the population of a specified country or region or in a defined subset of that population. [...]” | |
| Both definitions | |
| Other, please specify | |
| Q18 (Practitioners) Have you ever integrated health/HIA into an EIA? | |
| Yes | |
| No | |
| Q18 (Researchers) Have you ever conducted research on the integration of health/HIA into EIA? | |
| Yes | |
| No | |
| Don’t know | |
| Q19 In your opinion, what are the main barriers for the inclusion of health/HIA into EIA? (Max. 3 answers) | |
| Lack of guidance documents | |
| Lack of awareness | |
| Lack of training | |
| Lack of experience/competencies within the field of health | |
| Lack of political support | |
| Lack of resources | |
| Institutional barriers between different sectors | |
| Others, please specify | |
| Q20 In your opinion, what are the main facilitators for the inclusion of health/HIA into EIA? (Max. 3 answers) | |
| Guidance documents | |
| Awareness | |
| Training | |
| Experience | |
| Political support | |
| Resources | |
| Collaboration between different sectors | |
| Others, please specify | |
| Q21 Which health determinants do you think are most important to include into an EIA? (Max. 3 answers) | |
| General social, economic and political factors | |
| Environmental factors | |
| Built environment and housing | |
| Health services | |
| Other public services | |
| Private services and local economy | |
| Employment and livelihood | |
| Family and community structure | |
| Behavioral risk factors | |
| Biological factors | |
| Q22 (Practitioners) Which of the following health determinants have you never included into an EIA? (Unlimited answers) | |
| General social, economic and political factors | |
| Environmental factors | |
| Built environment and housing | |
| Health services | |
| Other public services | |
| Private services and local economy | |
| Employment and livelihood | |
| Family and community structure | |
| Behavioral risk factors | |
| Biological factors | |
| Q22 (Researchers) Which of the following health determinants have you never conducted research on regarding EIA? (Unlimited answers) | |
| General social, economic and political factors | |
| Environmental factors | |
| Built environment and housing | |
| Health services | |
| Other public services | |
| Private services and local economy | |
| Employment and livelihood | |
| Family and community structure | |
| Behavioral risk factors | |
| Biological factors | |
| Q23 (Policy/Strategy) Please indicate how frequently you assess the four types of documentations in your practice. 1: Very often; 2: Often; 3: Sometimes; 4: Rarely; 5: Very rarely; 6: Never. | |
| 1 | |
| 2 | |
| 3 | |
| 4 | |
| 5 | |
| 6 | |
| Don’t know | |
| Q23 (Plan) Please indicate how frequently you assess the four types of documentations in your practice. 1: Very often; 2: Often; 3: Sometimes; 4: Rarely; 5: Very rarely; 6: Never. | |
| 1 | |
| 2 | |
| 3 | |
| 4 | |
| 5 | |
| 6 | |
| Don’t know | |
| Q23 (Programme) Please indicate how frequently you assess the four types of documentations in your practice. 1: Very often; 2: Often; 3: Sometimes; 4: Rarely; 5: Very rarely; 6: Never. | |
| 1 | |
| 2 | |
| 3 | |
| 4 | |
| 5 | |
| 6 | |
| Don’t know | |
| Q23 (Project) Please indicate how frequently you assess the four types of documentations in your practice. 1: Very often; 2: Often; 3: Sometimes; 4: Rarely; 5: Very rarely; 6: Never. | |
| 1 | |
| 2 | |
| 3 | |
| 4 | |
| 5 | |
| 6 | |
| Don’t know | |
| Q24 (Practitioners) Which sources do you usually use when conducting EIA? (Unlimited answers) | |
| Scientific literature | |
| Guidance documents | |
| Expert opinion | |
| Grey literature | |
| Policy document | |
| Statistical databases | |
| Other, please specify | |
| Q24 (Researchers) Which sources do you think should be used when conducting EIAs? (Unlimited answers) | |
| Scientific literature | |
| Guidance documents | |
| Expert opinion | |
| Grey literature | |
| Policy document | |
| Statistical databases | |
| Other, please specify | |
| Q25 Do you think there is a need for more guidance documents regarding the inclusion of health/HIA into EIA? | |
| Yes | |
| No | |
| Don’t know | |
| Q26 When including health/HIA into EIA, do you think there is a need for guidance documents to better distinguish between the different types? Types of documentation of EIA: Policy/strategy, plan, programme, project. | |
| Yes | |
| No | |
| Don’t know | |
| Q27 When including health/HIA into EIA, do you think there is a need for guidance documents to better distinguish between the different areas? Areas of EIA: Agriculture, forestry and fishery, energy industry, extractive industry, other industry, infrastructure projects, telecommunications, tourism and leisure, waste management, water management, sectoral policies. | |
| Yes | |
| No | |
| Don’t know | |
| Introduction The SEA Directive 2001/42/EC and the EIA Directive 2014/52/EU both mention the consideration of plans and programmes (SEA) or projects (EIA) which are likely to have significant effects on the environment. Do you want to see this text in Danish? | |
| Yes | |
| No | |
| If answer “yes” from above: Introduktion: De to direktiver SEA 2001/42/EC og EIA 2014/52/EU beskriver begge, at planer og programmer (SEA) og projekter (EIA), der har en signifikant effekt på miljøet, skal vurderes i henhold til den pågældende konsekvensvurdering (2,3). | |
| Q28 (Epidemiological significance) To what degree do you associate the significance of a health effect with the following? 1: Very strong; 2: Strong; 3: Medium; 4: Little; 5: Very little; 6: None. | |
| 1 | |
| 2 | |
| 3 | |
| 4 | |
| 5 | |
| 6 | |
| Don’t know | |
| Q28 (Evidence from research) To what degree do you associate the significance of a health effect with the following? 1: Very strong; 2: Strong; 3: Medium; 4: Little; 5: Very little; 6: None. | |
| 1 | |
| 2 | |
| 3 | |
| 4 | |
| 5 | |
| 6 | |
| Don’t know | |
| Q28 (Official thresholds) To what degree do you associate the significance of a health effect with the following? 1: Very strong; 2: Strong; 3: Medium; 4: Little; 5: Very little; 6: None. | |
| 1 | |
| 2 | |
| 3 | |
| 4 | |
| 5 | |
| 6 | |
| Don’t know | |
| Q28 (Professional judgment) To what degree do you associate the significance of a health effect with the following? 1: Very strong; 2: Strong; 3: Medium; 4: Little; 5: Very little; 6: None. | |
| 1 | |
| 2 | |
| 3 | |
| 4 | |
| 5 | |
| 6 | |
| Don’t know | |
| Q29 Is there anything else you associate with significance of health effects? (Open ended) | |
| Yes, please specify | |
| No | |
| Q30 What competencies do you think should be required to assess population and human health within EIA? (Unlimited answers) | |
| Medical background | |
| Public Health background | |
| Health related training | |
| Health related workshop | |
| No health-related competencies | |
| Other, please specify | |
| Q31 (Practitioners) What do you need to include health into EIA? | |
| Your needs | |
| Don’t know | |
| Q31 (Researchers) What do you think practitioners need to include health into EIA? | |
| Your thoughts | |
| Don’t know | |
| Further questions Thank you very much for participating in the survey! If you wish, you can now give us feedback or provide us with your email address. Providing your email is voluntarily, and we will only contact you in case we have a question regarding your answers. Please click “next” to complete the survey and send in your responses. For this survey, the following sources were used:
| |
| Do you have comments or wish to tell us anything? | |
References
- Masson-Delmotte, V.; Zhai, P.; Pörtner, H.O.; Roberts, D.; Skea, J.; Shukla, P.R.; Pirani, A.; Moufouma-Okia, W.; Péan, C.; Pidcock, R. IPCC, 2018: Summary for Policymakers; The Intergovernmental Panel on Climate Change: Geneva, Switzerland, 2018. [Google Scholar]
- Global Burden of Disease (GBD). Available online: http://www.healthdata.org/gbd (accessed on 4 March 2019).
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef]
- Environmental Impact Assessment, Directive 2014/52/EU. Environmental Impact Assessment: Brussels, Belgium, 2014; Volume OJ L 124, 25.4.2014. 2014.
- Environmental Impact Assessment, Directive 2011/92/EU. Environmental Impact Assessment: Brussels, Belgium, 2012; Volume OJ L 26, 28.1.2012. 2012.
- Cave, B.; Fothergill, J.; Pyper, R.; Gibson, G.; Saunders, P. Health in Environmental Impact Assessment: A Primer for a Proportionate Approach; Ben Cave Associates Ltd.; IEMA; The Faculty of Public Health: Lincoln, UK, 2017. [Google Scholar]
- Nowacki, J. The Integration of Health into Environmental Assessments—With a Special Focus on Strategic Environmental Assessment; WHO Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- Vohra, S.; Nowacki, J.; Martuzzi, M. Health Impact Assessments and Health Integration into Environmental Assessments—Developing Further Implementation Strategies; Meeting Report of the Expert Meeting; WHO Regional Office for Europe: Bonn, Germany, 2015. [Google Scholar]
- WHO. Constitution of the World Health Organisation. With Amendments Adopted by the Fifty-First World Health Assembly, September 2005; WHO—World Health Organization: New York, NY, USA, 1946. [Google Scholar]
- Whitehead, M.; Dahlgren, G. What can be done about inequalities in health? Lancet 1991, 338, 1059–1063. [Google Scholar] [CrossRef]
- Barton, H.; Grant, M. A health map for the local human habitat. J. R. Soc. Promot. Health 2006, 126, 252–253. [Google Scholar] [CrossRef] [PubMed]
- SEA. SEA Directive; SEA: Singapore, 2001; Volume OJL. [Google Scholar]
- Danish EIA Law; Bekendtgørelse af Lov om Miljøvurdering af Planer og Programmer og af Konkrete Projekter (VVM); Law Number 1225. The Danish Parliament, Copenhagen, Denmark. 2018. Available online: https://www.retsinformation.dk/Forms/R0710.aspx?id=203447#idcc7ca7b9-afba-42a0-8bb4-262b1b3a91ac (accessed on 18 November 2019).
- Høringsdetaljer—Høringsportalen Udkast til Vejledning til lov om Miljøvurdering af Planer og Programmer og af Konkrete Projekter (VVM) 2. Del Konkrete Projekter. Available online: https://hoeringsportalen.dk/Hearing/Details/62356 (accessed on 12 April 2019).
- Vallgårda, S.; Koch, L. Research Methods in Public Health; Munksgaard: København, Danmark, 2008. [Google Scholar]
- Josimović, B.; Krunić, N.; Nenković-Riznić, M. The impact of airport noise as part of a strategic environmental assessment, case study: The Tivat (Montenegro) airport expansion plan. Transp. Res. Part D Transp. Environ. 2016, 49, 271–279. [Google Scholar] [CrossRef]
- Carvalho, S.; Partidario, M.; Sheate, W. High speed rail comparative strategic assessments in EU member states. Environ. Impact Assess. Rev. 2017, 66, 1–13. [Google Scholar] [CrossRef]
- Josimović, B.; Marić, I.; Milijić, S. Multi-criteria evaluation in strategic environmental assessment for waste management plan, a case study: The city of Belgrade. Waste Manag. 2015, 36, 331–342. [Google Scholar] [CrossRef] [PubMed]
- COWI. VVM Raport DSB Nyt Værksted Fredericia; COWI; EIA: Lyngby, Denmark, 2019.
- Biogasanlæg Kragekærvej. Available online: https://www.svendborg.dk/nyheder/borger/biogasanlaeg-kragekaervej (accessed on 13 May 2019).
- Josimović, B.; Crnčević, T. Implementation of Strategic Environmental Assessment in Serbia with Special Reference to the Regional Plan of Waste Management, Environmental Management; Sarkar, S.K., Ed.; SCIYO: Belgrade, Serbia, 2010. [Google Scholar]
- Sundhedskonsekvensvurderinger. SDU. Available online: https://www.sdu.dk:443/da/sif/rapporter/2005/sundhedskonsekvensvurderinger (accessed on 23 May 2019).
- Carvalho, S.A.P. High Speed Rail Comparative Strategic Assessments in EU Member States. Ph.D. Thesis, Instituto Superior Técnico, Lisbon, Portugal, 2015. [Google Scholar]
- Varneckas, T. European Gauge Railway Line between Kaunas and the Lithuanian-Latvian Border. Strategic Environmental Assessment. Information for the Notification under the Protocol on Strategic Environmental Assessment to the Convention on Environmental Impact Assessment in a Transboundary Context; Sweco Lietuva: Vilinus, Lithuania, 2013. [Google Scholar]
- Fehr, R.; Viliani, F.; Nowacki, J.; Martuzzi, M. Health in Impact Assessments: Opportunities not to Be Missed; WHO Regional Office for Europe: Copenhagen, Danmark, 2014. [Google Scholar]
- European Commission. Environmental Impact Assessment of Projects—Guidance on the Preparation of the Environmental Impact Assessment Report; European Commission: Luxembourg, 2017. [Google Scholar]
- EC. European Neighbourhood Policy and Enlargement Negotiations. European Neighbourhood Policy And Enlargement Negotiations—European Commission. 2019. Available online: https://ec.europa.eu/neighbourhood-enlargement/countries/check-current-status_en (accessed on 28 May 2019).
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Mentioning EIA, SEA, HIA | Only mentioning risk assessment |
| About policy, plan, programme, project, proposal and EIA, SEA, HIA | Only focusing on EIA, SEA, HIA appraisal/development of approach instead of implementation |
| About institutionalisation, integration or implementation of EIA, SEA, HIA | Only mentioning SIA, SA, HRIA, economic assessment or LCA 1 |
| EIA, SEA mentioning HIA or health assessment | Only focusing on outcome or process evaluation |
| Scope |
|---|
| General social, economic and political factors |
| Environmental factors |
| Built environment and housing |
| Health services |
| Other public services and local economy |
| Private services and local economy factors |
| Employment and livelihood factors |
| Family and community structure |
| Behavioural risk factors |
| Biological factors |
| Author | Year | Country | Study Design | Population | Intervention | Outcome |
|---|---|---|---|---|---|---|
| Josimović et al. [16] | 2016 | Montenegro | Case study | Tivat Municipality: about 14,000 | SEA | Health determinants: Environmental factors; built environment and housing; health services; other public services |
| Considerations of vulnerable groups: Yes 1 | ||||||
| Incentive: Legislation | ||||||
| Carvalho et al. [17] | 2017 | Lithuania/Latvia | Case study | N/A | SEA | Health determinants: Environmental factors; built environment; employment and livelihood |
| Considerations of vulnerable groups: No | ||||||
| Incentive: EU accession | ||||||
| Josimović et al. [18] | 2015 | Serbia | Case study | City of Belgrade: 1,621,396 | SEA | Health determinants: Environmental factors; built environment; employment and livelihood |
| Considerations of vulnerable groups: No | ||||||
| Incentive: EU accession | ||||||
| COWI [19] | 2019 | Denmark | Case study/report | N/A | EIA | Health determinants: Environmental factors |
| Considerations of vulnerable groups: No | ||||||
| Incentive: Legislation | ||||||
| Dansk Biogasrådgivning A/S [20] | 2019 | Denmark | Case study/report | N/A | EIA | Health determinants: Environmental factors; biological factors |
| Considerations of vulnerable groups: No | ||||||
| Incentive: Legislation |
| Number of all participants (n) | 42 |
| Number of EU practitioners (n) | 7 |
| Number of Danish practitioners (n) | 25 |
| Number of researchers (n) | 10 |
| Average age | 46 |
| Age range | 29–64 |
| Workplace | Europe |
| % of All Practitioners (N = 32) | % of All Researchers (N = 10) | ||
|---|---|---|---|
| Barriers | Lack of experiences/competencies within the field | 50% (n = 16) | 50% (n = 5) |
| Lack of guidance documents | 44% (n = 14) | / | |
| Lack of awareness | 41% (n = 13) | / | |
| Institutional barriers between different sectors | / | 60% (n = 6) | |
| Lack of training | / | 50% (n = 5) | |
| Facilitators | Guidance documents | 53% (n = 17) | 50% (n = 5) |
| Collaboration between different sectors | 41% (n = 13) | 80% (n = 8) | |
| Political support | 41% (n = 13) | 50% (n = 5) | |
| Sources for conducting EIA/SEA | Guidance documents | 94% (n = 30) | 70% (n = 7) |
| Scientific literature | 78% (n = 25) | 80% (n = 8) | |
| Expert opinion | 78% (n = 25) | 80% (n = 8) | |
| Grey literature | 66% (n = 21) | 70% (n = 7) | |
| Policy documents | 63% (n = 20) | 70% (n = 7) | |
| Statistical databases | 56% (n = 18) | 80% (n = 8) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Humboldt-Dachroeden, S.; Fischer-Bonde, B.; Gulis, G. Analysis of Health in Environmental Assessments—A Literature Review and Survey with a Focus on Denmark. Int. J. Environ. Res. Public Health 2019, 16, 4570. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224570
Humboldt-Dachroeden S, Fischer-Bonde B, Gulis G. Analysis of Health in Environmental Assessments—A Literature Review and Survey with a Focus on Denmark. International Journal of Environmental Research and Public Health. 2019; 16(22):4570. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224570
Chicago/Turabian StyleHumboldt-Dachroeden, Sarah, Birgitte Fischer-Bonde, and Gabriel Gulis. 2019. "Analysis of Health in Environmental Assessments—A Literature Review and Survey with a Focus on Denmark" International Journal of Environmental Research and Public Health 16, no. 22: 4570. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16224570