Pyruvate Kinase M2 Expression: A Potential Metabolic Biomarker to Differentiate Endometrial Precancer and Cancer that is Associated with Poor Outcomes in Endometrial Carcinoma

Abstract
:1. Introduction
2. Materials and Methods
2.1. Tissue Microarray
2.2. Immunohistochemistry Stain
2.3. Statistical Analysis
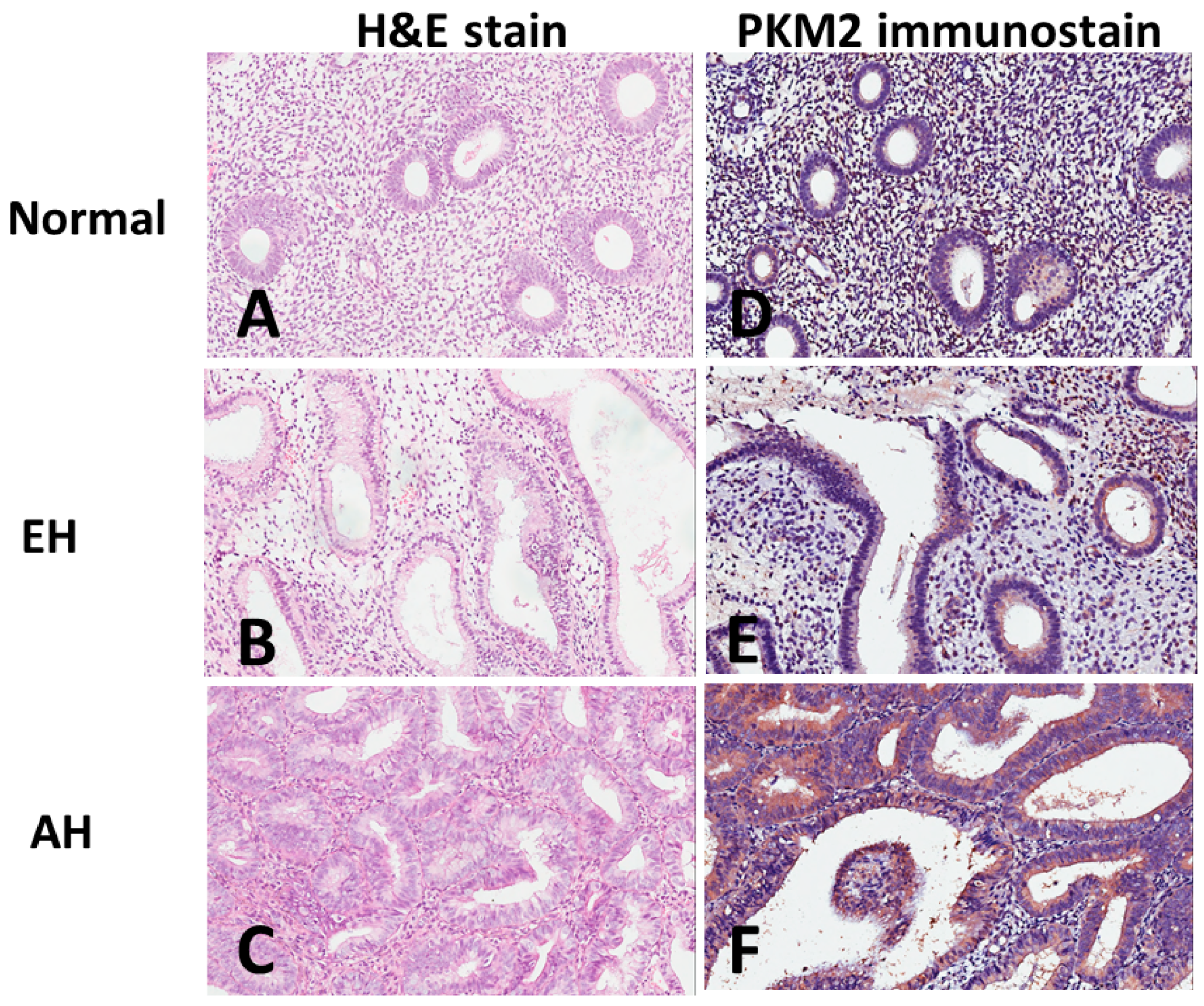
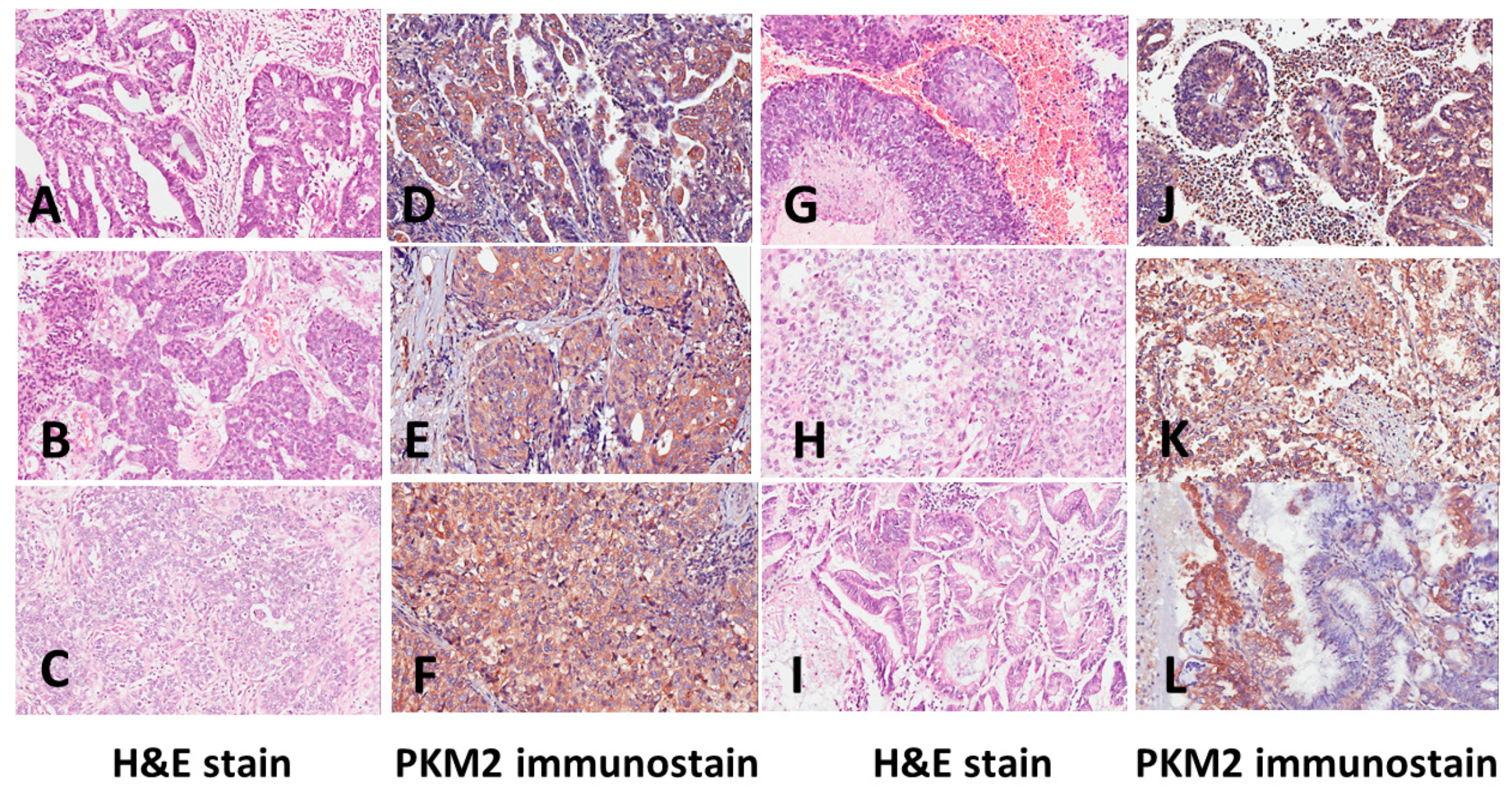
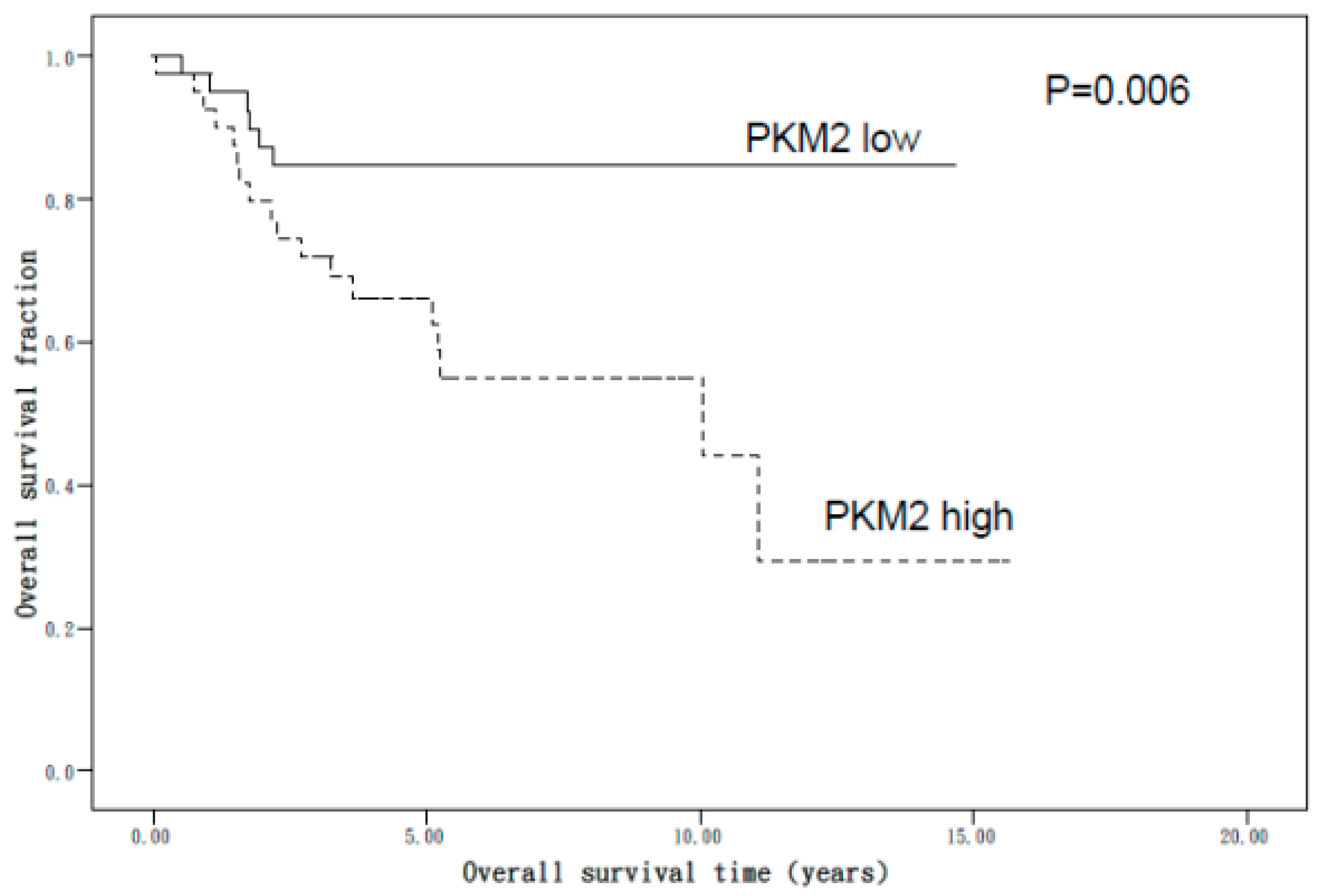
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Emons, G.; Fleckenstein, G.; Hinney, B.; Huschmand, A.; Heyl, W. Hormonal interactions in endometrial cancer. Endocr. Relat. Cancer 2000, 7, 227–242. [Google Scholar] [CrossRef] [PubMed]
- Kurman, R.J.; Kaminski, P.F.; Norris, H.J. The behavior of endometrial hyperplasia. A long-term study of “untreated” hyperplasia in 170 patients. Cancer 1985, 56, 403–412. [Google Scholar] [CrossRef]
- Mutter, G.L. Histopathology of genetically defined endometrial precancers. Int. J. Gynecol. Pathol. 2000, 19, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Mutter, G.L. Diagnosis of premalignant endometrial disease. J. Clin. Pathol. 2002, 55, 326–331. [Google Scholar] [CrossRef]
- Silverberg, S.G. Problems in the Differential Diagnosis of Endometrial Hyperplasia and Carcinoma. Mod. Pathol. 2000, 13, 309–327. [Google Scholar] [CrossRef]
- Sanderson, P.A.; Critchley, H.O.; Williams, A.R.; Arends, M.J.; Saunders, P.T. New concepts for an old problem: The diagnosis of endometrial hyperplasia. Hum. Reprod. Update 2017, 23, 232–254. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The Next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Pavlova, N.N.; Thompson, C.B. The Emerging Hallmarks of Cancer Metabolism. Cell Metab. 2016, 23, 27–47. [Google Scholar] [CrossRef]
- Noguchi, T.; Inoue, H.; Tanaka, T. The M1- and M2-type isozymes of rat pyruvate kinase are produced from the same gene by alternative RNA splicing. J. Boil. Chem. 1986, 261, 13807–13812. [Google Scholar]
- Christofk, H.R.; Vander Heiden, M.G.; Harris, M.H.; Ramanathan, A.; Gerszten, R.E.; Wei, R.; Fleming, M.D.; Schreiber, S.L.; Cantley, L.C. The M2 splice isoform of pyruvate kinase is important for cancer metabolism and tumour growth. Nature 2008, 452, 230–233. [Google Scholar] [CrossRef]
- Anastasiou, D.; Yu, Y.; Israelsen, W.J.; Jiang, J.K.; Boxer, M.B.; Hong, B.S.; Tempel, W.; Dimov, S.; Shen, M.; Jha, A.; et al. Pyruvate kinase M2 activators promote tetramer formation and suppress tumorigenesis. Nat. Chem. Biol. 2012, 8, 839–847. [Google Scholar] [CrossRef] [PubMed]
- Chao, T.-K.; Huang, T.-S.; Liao, Y.-P.; Huang, R.-L.; Su, P.-H.; Shen, H.-Y.; Lai, H.-C.; Wang, Y.-C. Pyruvate kinase M2 is a poor prognostic marker of and a therapeutic target in ovarian cancer. PLoS ONE 2017, 12, e0182166. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo, A.; Piña, P.; Guerrero, G.; Lazos, M.; Salcedo, M. A simple method for the construction of small format tissue arrays. J. Clin. Pathol. 2003, 56, 144–146. [Google Scholar] [CrossRef] [PubMed]
- Scully, R.E.; Bonfiglio, T.A.; Kurman, R.J.; Silverberg, S.G.; Wilkinson, E.J. Uterine Corpus. Histological Typing of Female Genital Tract Tumours, 2nd ed.; Springer: Berlin/Heidelberg, Germany; New York, NY, USA, 1994; pp. 13–30. [Google Scholar]
- Pecorelli, S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int. J. Gynecol. Obstet. 2009, 105, 103–104. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.-S.; Hsieh, D.-S.; Loh, S.-H.; Chen, A.; Yao, C.-W.; Yen, C.-Y. Increasing expression of serine protease matriptase in ovarian tumors: Tissue microarray analysis of immunostaining score with clinicopathological parameters. Mod. Pathol. 2006, 19, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Sarmadi, S.; Izadi-Mood, N.; Sotoudeh, K.; Tavangar, S.M. Altered PTEN expression; a diagnostic marker for differentiating normal, hyperplastic and neoplastic endometrium. Diagn. Pathol. 2009, 4, 41. [Google Scholar] [CrossRef] [PubMed]
- Allison, K.H.; Reed, S.D.; Voigt, L.F.; Jordan, C.D.; Newton, K.M.; Garcia, R.L. Diagnosing endometrial hyperplasia: Why is it so difficult to agree? Am. J. Surg. Pathol. 2008, 32, 691–698. [Google Scholar] [CrossRef]
- Kendall, B.S.; Ronnett, B.M.; Isacson, C.; Cho, K.R.; Hedrick, L.; Diener-West, M.; Kurman, R.J. Reproducibility of the diagnosis of endometrial hyperplasia, atypical hyperplasia, and well-differentiated carcinoma. Am. J. Surg. Pathol. 1998, 22, 1012–1019. [Google Scholar] [CrossRef]
- Suh-Burgmann, E.; Hung, Y.Y.; Armstrong, M.A. Complex atypical endometrial hyperplasia: The risk of unrecognized adenocarcinoma and value of preoperative dilation and curettage. Obstet. Gynecol. 2009, 114, 523–529. [Google Scholar] [CrossRef]
- Taylor, P.J.; Gomel, V. 2 Endometrial ablation: Indications and preliminary diagnostic hysteroscopy. Baillière’s Clin. Obstet. Gynaecol. 1995, 9, 251–260. [Google Scholar] [CrossRef]
- Teng, Y.; Ai, Z.; Wang, Y.; Wang, J.; Luo, L. Proteomic identification of PKM2 and HSPA5 as potential biomarkers for predicting high-risk endometrial carcinoma. J. Obstet. Gynaecol. Res. 2013, 39, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Matias-Guiu, X.; Catasus, L.; Bussaglia, E.; Lagarda, H.; Garcia, A.; Pons, C.; Muñoz, J.; Argüelles, R.; Machin, P.; Prat, J. Molecular pathology of endometrial hyperplasia and carcinoma. Hum. Pathol. 2001, 32, 569–577. [Google Scholar] [CrossRef] [PubMed]
- Hecht, J.L.; Mutter, G.L. Molecular and Pathologic Aspects of Endometrial Carcinogenesis. J. Clin. Oncol. 2006, 24, 4783–4791. [Google Scholar] [CrossRef] [PubMed]
- Horn, L.-C.; Meinel, A.; Handzel, R.; Einenkel, J. Histopathology of endometrial hyperplasia and endometrial carcinoma. Ann. Diagn. Pathol. 2007, 11, 297–311. [Google Scholar] [CrossRef]
- Banno, K.; Kisu, I.; Yanokura, M.; Tsuji, K.; Masuda, K.; Ueki, A.; Kobayashi, Y.; Yamagami, W.; Nomura, H.; Tominaga, E.; et al. Biomarkers in endometrial cancer: Possible clinical applications (Review). Oncol. Lett. 2012, 3, 1175–1180. [Google Scholar] [CrossRef]
- Vander Heiden, M.G.; Cantley, L.C.; Thompson, C.B. Understanding the Warburg effect: The metabolic requirements of cell proliferation. Science 2009, 324, 1029–1033. [Google Scholar] [CrossRef]
- Christofk, H.R.; Vander Heiden, M.G.; Wu, N.; Asara, J.M.; Cantley, L.C. Pyruvate kinase M2 is a phosphotyrosine-binding protein. Nature 2008, 452, 181–186. [Google Scholar] [CrossRef]
- Liu, L.; Ulbrich, J.; Müller, J.; Wüstefeld, T.; Aeberhard, L.; Kress, T.R.; Muthalagu, N.; Rycak, L.; Rudalska, R.; Moll, R.; et al. Deregulated MYC expression induces dependence upon AMPK-related kinase 5. Nature 2012, 483, 608–612. [Google Scholar] [CrossRef]
- Lee, J.; Kim, H.K.; Han, Y.-M.; Kim, J. Pyruvate kinase isozyme type M2 (PKM2) interacts and cooperates with Oct-4 in regulating transcription. Int. J. Biochem. Cell Boil. 2008, 40, 1043–1054. [Google Scholar] [CrossRef]
- Lim, J.Y.; Yoon, S.O.; Seol, S.Y.; Hong, S.W.; Kim, J.W.; Choi, S.H.; Cho, J.Y. Overexpression of the M2 isoform of pyruvate kinase is an adverse prognostic factor for signet ring cell gastric cancer. World J. Gastroenterol. 2012, 18, 4037–4043. [Google Scholar] [CrossRef]
- Li, W.; Liu, J.; Jackson, K.; Shi, R.; Zhao, Y. Sensitizing the Therapeutic Efficacy of Taxol with Shikonin in Human Breast Cancer Cells. PLoS ONE 2014, 9, e94079. [Google Scholar] [CrossRef]
- Cheng, T.Y.; Yang, Y.C.; Wang, H.P.; Tien, Y.W.; Shun, C.T.; Huang, H.Y.; Hsiao, M.; Hua, K.T. Pyruvate kinase M2 promotes pancreatic ductal adenocarcinoma invasion and metastasis through phosphorylation and stabilization of PAK2 protein. Oncogene 2018, 37, 1730–1742. [Google Scholar] [CrossRef]
- Wong, N.; De Melo, J.; Tang, D. PKM2, a Central Point of Regulation in Cancer Metabolism. Int. J. Cell Boil. 2013, 2013, 242513. [Google Scholar] [CrossRef] [Green Version]
- Hosseini Nasab, S.; Jooya, N.; Esmaeili, A.; Zarrin Khameh, N.; Diaz-Arrastia, C.; Momeni, M. Using Pyruvate Kinase as a Predictor for Patient with Endometrial Cancer Having Complex Hyperplasia with Atypia to Prevent Hysterectomy and Preserve Fertility: Retrospective Immunohistochemical Study. Reprod. Sci. 2018, 25, 1286–1291. [Google Scholar] [CrossRef]
- Yang, W.; Lu, Z. Pyruvate kinase M2 at a glance. J. Cell Sci. 2015, 128, 1–6. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| PKM2 low n. (%) | PKM2 high n. (%) | p Value | |
|---|---|---|---|
| <0.001 | |||
| Normal | 30 (100.0) | 0(0) | |
| EH | 36 (100.0) | 0(0) | |
| AH | 28 (87.5) | 4 (12.5) | |
| EC | 54 (50.0) | 54 (50.0) |
| PKM2 Expression Low | PKM2 Expression High | p Value | |
|---|---|---|---|
| Characteristic | 0+, 1+ | 2+, 3+, 4+, 6+ | |
| Patients (no.) | 42 | 43 | |
| Age (years) | 0.009 | ||
| Range | 21–81 | 32–89 | |
| Mean ± SEM | 52.21 ± 1.60 | 58.77 ± 1.85 | |
| FIGO Stage [no. (%)] | 0.712 | ||
| I, II | 28 (51.9) | 26 (48.1) | |
| III, IV | 14 (45.2) | 17 (54.8) | |
| Nuclear grade [no. (%)] | |||
| G1 | 24 (58.5) | 17 (41.5) | 0.202 |
| G2 | 9 (47.4) | 10 (52.6) | |
| G3 | 9 (36.0) | 16 (64.0) | |
| Histological type [no. (%)] | 0.135 a | ||
| CC | 1 (12.5) | 7 (87.5) | |
| EmAC | 34 (53.1) | 30 (46.9) | |
| MC | 1 (50.0) | 1 (50) | |
| SC | 6 (54.5) | 5 (45.5) | |
| Histological type [no. (%)] | 0.345 | ||
| EmAC | 34 (53.1) | 30 (46.9) | |
| Non- EmAC | 8 (38.1) | 13 (61.9) |
| Variable | Univariate Analysis Crude HR (95% CI) | Multivariate Adjusted HR (95% CI) |
|---|---|---|
| Age (years) | 1.04 (1.00–1.07) * | 1.04 (1.00–1.08) |
| PKM2 expression a | ||
| Low | 1.00 (Ref.) | 1.00 (Ref.) |
| High | 3.40 (1.35–8.56) * | 1.96 (0.71–5.37) |
| FIGO Stage | ||
| I, II | 1.00 (Ref.) | 1.00 (Ref.) |
| III, IV | 8.41 (3.28–21.58) * | 7.97 (2.71–23.48) * |
| Nuclear grade | ||
| G1 | 1.00 (Ref.) | 1.00 (Ref.) |
| G2 | 1.54 (0.47–5.07) | 0.89 (0.24–3.28) |
| G3 | 4.78 (1.79–12.76) * | 4.04 (0.96–16.99) |
| Histological type | ||
| EmAC | 1.00 (Ref.) | 1.00 (Ref.) |
| Non-EmAC | 2.90 (1.27–6.63) * | 0.32 (0.08–1.30) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, Y.-J.; Chou, Y.-C.; Lin, Y.-J.; Yu, M.-H.; Ou, Y.-C.; Chu, P.-W.; Wu, C.-C.; Wang, Y.-C.; Chao, T.-K. Pyruvate Kinase M2 Expression: A Potential Metabolic Biomarker to Differentiate Endometrial Precancer and Cancer that is Associated with Poor Outcomes in Endometrial Carcinoma. Int. J. Environ. Res. Public Health 2019, 16, 4589. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234589
Lai Y-J, Chou Y-C, Lin Y-J, Yu M-H, Ou Y-C, Chu P-W, Wu C-C, Wang Y-C, Chao T-K. Pyruvate Kinase M2 Expression: A Potential Metabolic Biomarker to Differentiate Endometrial Precancer and Cancer that is Associated with Poor Outcomes in Endometrial Carcinoma. International Journal of Environmental Research and Public Health. 2019; 16(23):4589. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234589
Chicago/Turabian StyleLai, Yu-Ju, Yu-Ching Chou, Yi-Jia Lin, Mu-Hsien Yu, Yu-Che Ou, Po-Wei Chu, Chia-Chun Wu, Yu-Chi Wang, and Tai-Kuang Chao. 2019. "Pyruvate Kinase M2 Expression: A Potential Metabolic Biomarker to Differentiate Endometrial Precancer and Cancer that is Associated with Poor Outcomes in Endometrial Carcinoma" International Journal of Environmental Research and Public Health 16, no. 23: 4589. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16234589