1. Introduction
Patient enablement refers, broadly speaking, to the process or the result of enabling patients to assess and manage their health conditions more competently, both as individuals and within the practitioner-patient relationship. Patient enablement is a core element of patient empowerment and patient activation [
1], and as such is an important goal of contemporary health policy. All three concepts, i.e., patient enablement, empowerment, and activation, can be (and have been) defined either as a process or as an emergent state. As e.g., Fumagalli et al. summarized several conceptualizations [
2,
3,
4,
5], patient enablement may be defined as the process of enabling patients by “(1) providing appropriate knowledge, skill and abilities to understand their conditions and make decisions; and (2) developing appropriate contexts that allow patients to learn such knowledge, skill and abilities.” [
1]. Patient enablement may also be defined as an emergent state reflecting “the gained measure in which patients understand their health conditions and feel able to cope with them” [
1,
6]. The same holds for the terms ‘patient empowerment’ and ‘patient activation’: Both can be conceptualized as either a process or an emergent state [
1].
The relevance of patient enablement in the health services context has been shown in numerous studies which have been analyzed and summarized by Hudon et al. in their concept analysis [
7] and in an integrative review by Frost et al. [
8]. According to Hudon et al., the consequences of patient enablement include, e.g., patient satisfaction, a feeling of self-efficacy, the development of certain skills, improvement in patients’ health condition and quality of life as well as in their participation in care, but also higher job satisfaction and self-confidence in health professionals [
7]. Other important consequences are a reduced dependency of patients on health services, better consultations [
8], and a reduced preference in patients for seeing a different doctor [
9].
But can we conceive ‘patient enablement’ on the one hand and ‘patient empowerment’ and ‘patient activation’ on the other hand as distinct concepts? One should keep in mind that existing conceptualizations of each of these terms are heterogeneous, in particular with regard to ‘patient empowerment’ [
10,
11]. However, it is broadly possible to detect some dominating tendencies in the usage of those concepts [
1,
11]. In past research, ‘patient enablement’ and ‘patient empowerment’ were often used as synonyms [
1]. Referring to the arguments of Fumagalli et al. [
1] and Castro et al. [
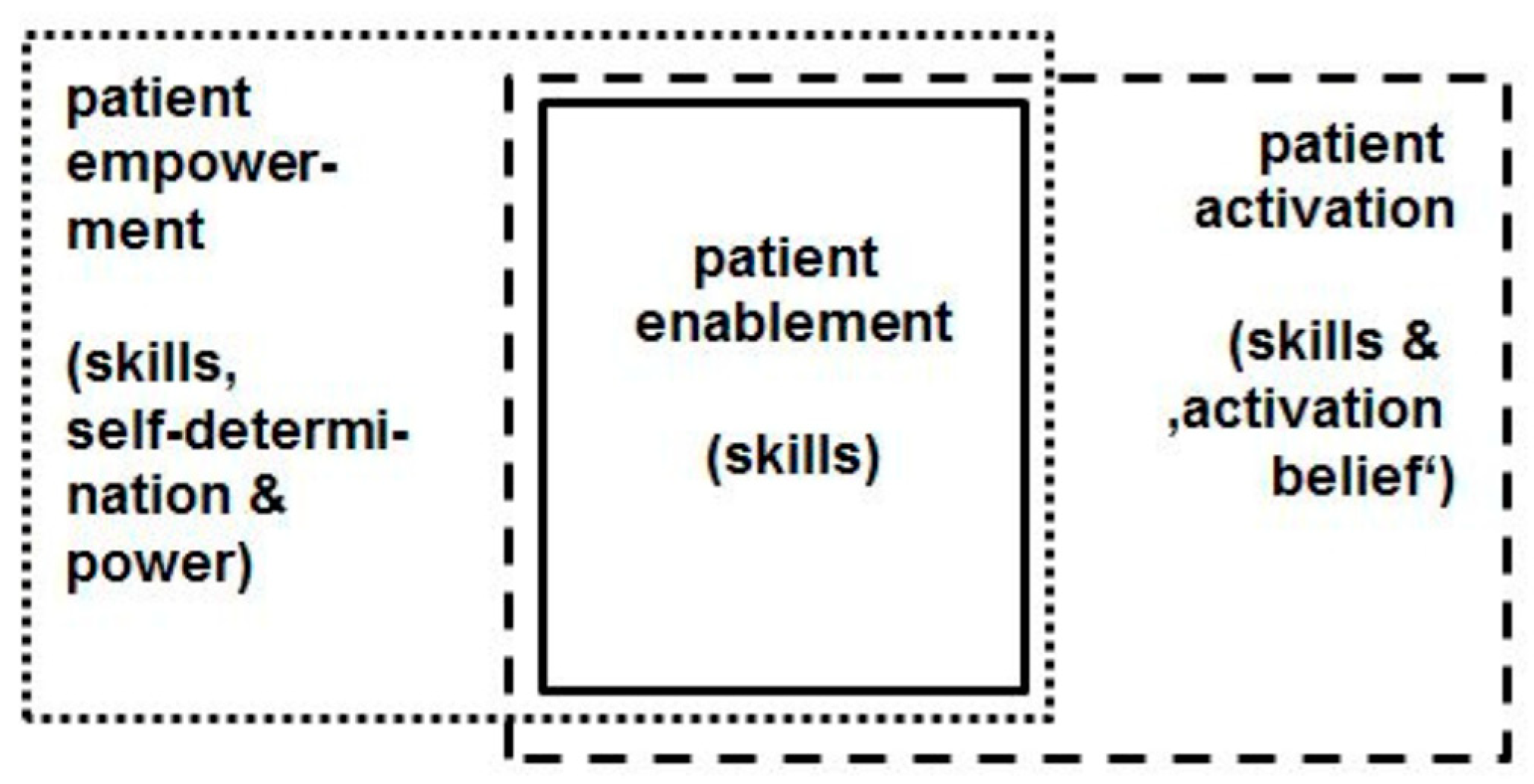
11] we can distinguish the two terms by referring to the elements of self-determination, power, motivation, and engagement: Patients are ‘enabled’ when they are
able to engage in self-care or to take part in shared decision-making, but not necessarily have the power and/or motivation to do so (because, e.g., they do not have a sufficiently strong desire for self-determination). In comparison, patients are ’empowered’ when they are not only able to engage in self-care and shared decision-making but also have a sufficiently strong desire for self-determination and the power—and thus the motivation—to do so. Lacking self-determination and power as defining attributes, the term ‘enabled patient’ has a narrower connotation (intension) but a larger conceptual scope (extension) than the term ‘empowered patient’.
The comparably recent concept ‘patient activation’, put forward in the preceding decade by Hibbard et al. [
12,
13,
14,
15], comes likewise very close to ‘patient enablement’: According to Hibbard’s conceptualization, activated patients “believe patients have important roles to play in self-managing care, collaborating with providers, and maintaining their health. They know how to manage their condition and maintain functioning and prevent health declines; and they have the skills and behavioral repertoire to manage their condition, collaborate with their health providers, maintain their health functioning, and access appropriate and high-quality care.” [
15]. Hibbard’s ‘Patient Activation Measure’ shows, even in its common short form (PAM-13) [
12], that the ‘belief component’ is crucial: Activated patients believe that they have a crucial role in managing their own healthcare; moreover they are confident that they are able to apply their knowledge and skills, and therefore are motivated to do so. The importance of the belief component is reflected e.g., in the first two items of the PAM-13 questionnaire: (i) “When all is said and done, I am the person who is responsible for managing my health condition” and (ii) “Taking an active role in my own healthcare is the most important factor in determining my health and ability to function” [
12]. Unlike ‘patient enablement’, the term ‘patient activation’ conceives a specific belief as a key attribute—in addition to knowledge and skills. Thus we may conclude that the connotation of the ‘enabled patient’ is also narrower than the connotation of the ‘activated patient’, implying its scope is larger than the conceptual scope of the ‘activated patient’.
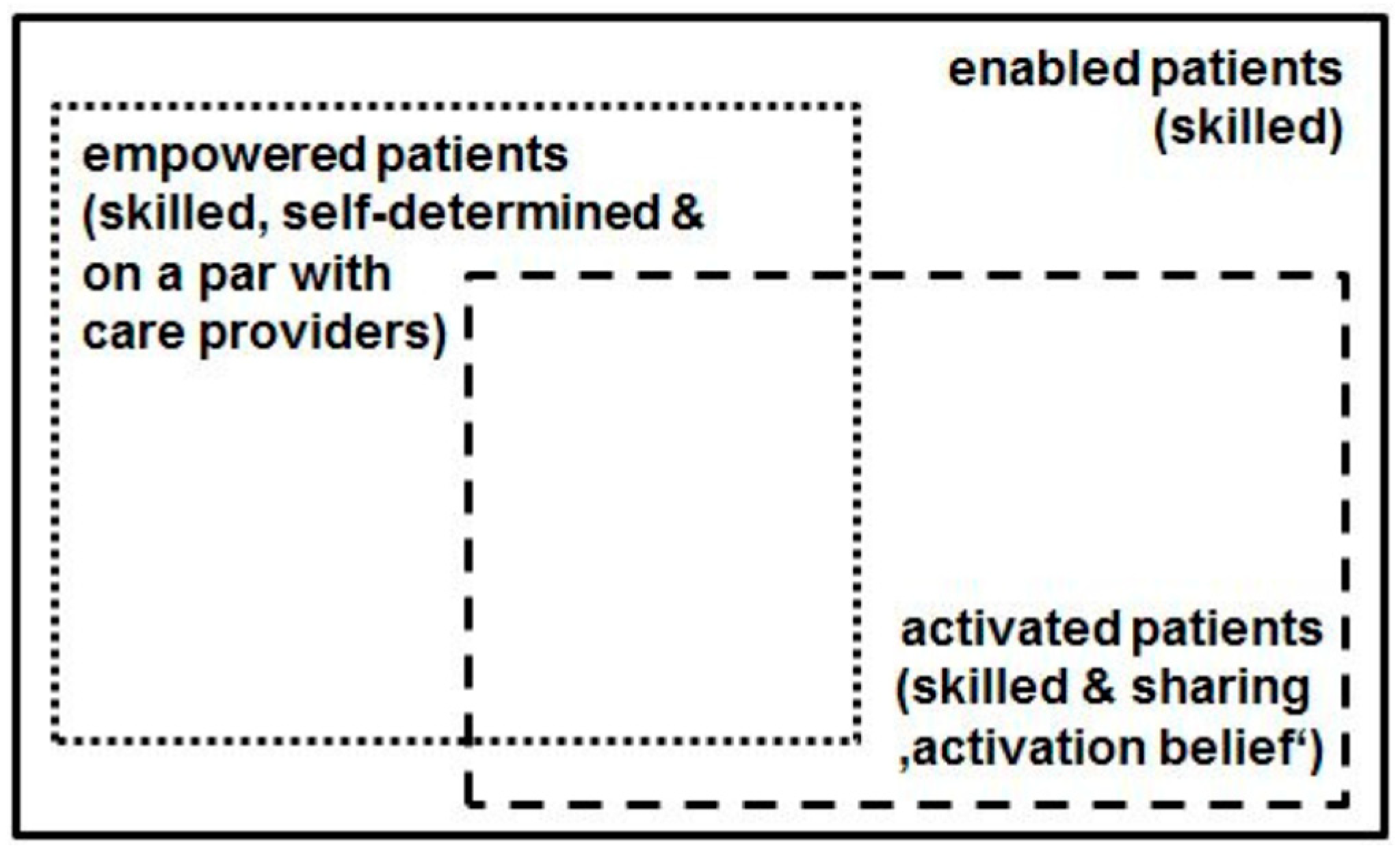
Figure 1 and
Figure 2 illustrate our argument:
Figure 1 provides a connotation map of the terms ‘patient enablement’, ‘patient empowerment’, and ‘patient activation’;
Figure 2 shows a scheme of the conceptual scopes of the terms ‘enabled patient’, ‘empowered patient’, and ‘activated patient’.
The reason for the present study was our experience with an own trend study, in which we surveyed patient-related outcomes in an integrated healthcare system in Germany [
16]. Here, we originally wanted to include a measure of either patient activation or patient enablement as these were strategic aims of the integrated healthcare system management. Furthermore, we sought a generic instrument applicable across health indications and valid for persons with chronic or acute conditions. So we took a closer look at Hibbard’s PAM-13 [
12] and its German version [
13] and at Howie’s seminal ‘Patient Enablement Instrument’ (PEI) [
2,
17]. We decided not to use PAM-13 because of three reasons: First, some items of PAM-13 seem to match patients in chronic conditions very well [
12,
15] whereas they do not so well apply to patients with non-chronic conditions (e.g., item “I know what each of my prescribed medications do”). Second, the PAM-13 questionnaire is provided by a commercial company and therefore is not free to use [
14]. And third, after a closer look at the ‘confidence’ and ‘belief’ items we thought it might be more reasonable to focus on (self-perceived) knowledge, skills, and abilities, and to leave the ‘belief’ component aside: e.g., the PAM-13 item “Taking an active role in my own healthcare is the most important factor in determining my health and ability to function” may be perceived as overstated or overgeneralized, reflecting rather an ideology than an empirically verifiable generalization. Howie’s PEI, on the other hand, is a well-established instrument measuring patient enablement with six items. Derived from qualitative research with patients on what mattered most to them in terms of consultation outcomes [
17], the PEI has a high internal consistency (Cronbach’s alpha = 0.93 [
2]). Meanwhile, the PEI has been translated into many other languages and tested in different countries where its high internal consistency has been confirmed [
9,
18,
19,
20,
21,
22,
23], with the respective Cronbach’s alpha values ranging from 0.84 (Chinese version [
22]) to 0.93 (English original version [
2] and French version [
19]). Although test-retest reliability has sometimes been found only moderate [
19,
21], the different PEI versions have good psychometric properties. A disadvantage of the PEI, however, seems to be that it requires a prior intervention (e.g., a physician-patient consultation) as the questionnaire items directly measure patients’ perceived change in skills etc. in response to a given intervention. The PEI, then, is a
direct measure of perceived change in enablement and does not measure a given level of enablement, as Enthoven et al. clearly stated [
18]. This might lead to findings that seem paradoxical when the PEI is taken as an indicator of patient enablement: Thus, e.g., patients with less experience and knowledge of their disease might be more likely to improve in terms of the PEI score than patients who have experienced problems for a longer time, have tried several (self-) treatment options and might be real ‘experts’ of their own disease [
18]. However, because the PEI is a direct measure of change of enablement (and not of the level of enablement), the first patient in our example might appear to be ‘more enabled’ than the second one—on the grounds of the PEI. For the same reason, the PEI cannot serve well as a simple survey instrument in a population which has not been subjected to a particular intervention. Furthermore, since PEI comprises only six items, it might be a too ‘general’ or ‘global’ measure for some specific ends. For example, none of the six PEI items explicitly refers to a patient’s ability to appropriately interact with health professionals—an aspect which might be considered an important enablement component (e.g., [
5,
7]). For these reasons we decided to develop and validate a new generic measure of patient enablement which is more detailed than PEI and not bound to a previous intervention.
In addition, to support widespread quality improvement efforts and monitoring of patient enablement in the population [
24], the new instrument should be freely available. As we planned to use this new measure first in a German healthcare setting, we designed it in German language. But from our own experiences in European research projects we conclude that there is a demand to translate and validate the instrument also in other languages.
4. Discussion
In our study we developed and validated a measure of patient enablement to assess it in a comprehensive manner; the use of this measure is independent of a previous intervention and conceptually distinct from both patient activation and patient empowerment.
Our results show that the Patient Enablement Scale-13 items (PEN-13) is suitable for providing reliable and valid results for the measurement of patient enablement in a sample with different types and severity of medical conditions.
The results of the exploratory factor analysis show that the PEN-13 is characterized by two factors. The internal consistency of both factors achieved good to excellent values; its level is comparable to that of the PEI (see the ‘Introduction’ section) and the PAM-13 [
12,
13,
14,
47,
48,
49,
50,
51,
52,
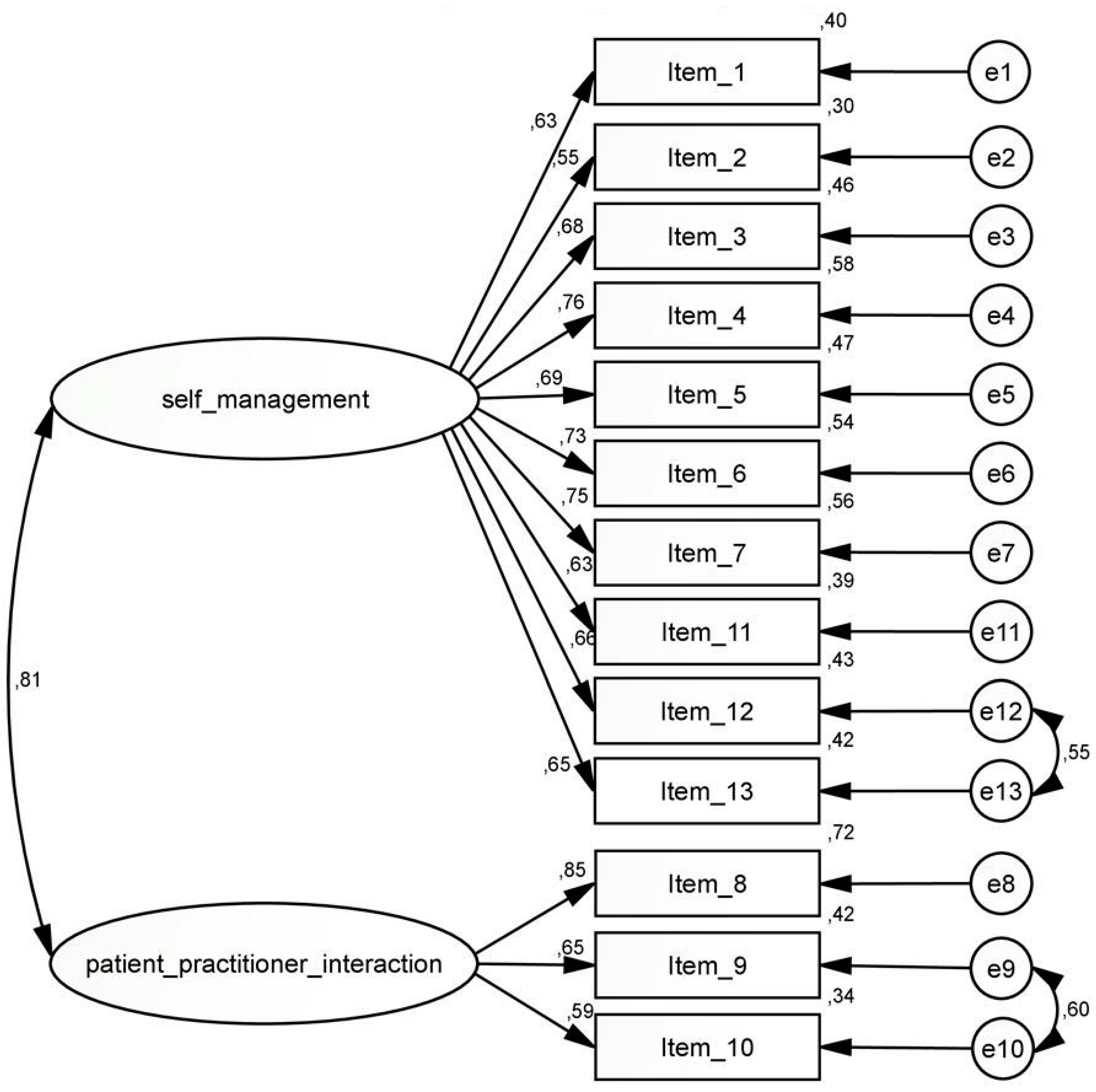
53]. The confirmatory factor analysis verified the two factors self-management and patient-practitioner interaction. Adjustments to this two-factor model additionally improved the values for model fit. Due to the high correlations between the original and re-weighted factor scores we assume that the adjustments had no relevant impact on the score. Since no practical effects on the scores are expected, these adjustments were permitted in favor of a slightly improved model fit. The application of these adjustments in other samples must be verified. Further validation studies will be helpful to confirm or reject the two additional correlations.
Due to the high correlation between the two factors (
r = 0.81), it could also be justified to group the items into one factor. In this case, however, a poorer model fit resulted. In addition, the aim of the study was to find out more about the principle—and the ‘inner structure’—of the ‘enabled patient’. The comparison with the one-factor model showed then that the conceptualization of two underlying factors should be preferred to the one-factor conceptualization. As the items are not bound to a specific treatment situation or health indication, the PEN-13 matches persons with acute or chronic illness. Nevertheless, it should be noted that participants who stated that they did not suffer from any chronic disease completed the scale less often than participants who indicated a chronic disease (see
Table 3 for missing values in item 5 and the last paragraph in
Section 3.2.).
For the construct validation with correlation analyses, positive correlations with the Generalized Self-efficacy Scale (GSE) and the 16-item version of the European Health Literacy Survey Questionnaire (HLS-EU-Q16) were expected. Due to the similarity of the item formulations of the GSE, a high correlation was assumed and confirmed with
r = 0.57. A moderate to high correlation was expected between the PEN-13 score and the health literacy score; the result in our study (
r = 0.60,
p < 0.001) confirmed these expectations. Moreover, health literacy seems to be closely linked to patient empowerment [
54]. Finally, a low positive correlation between PEN-13 and level of education could be shown, as well as a moderate positive correlation between patient enablement and current health status (EQ-VAS). A positive correlation between enablement (PEI score) and level of education has also been found in the study of Groene et al. [
55]. A relevant positive correlation between patient enablement, measured by the PEI, and overall health status was also found in two other studies [
56,
57] but not in a pilot study [
58]. Mead et al. even suggest that enablement may be a possible predictor of health-related quality of life, which should be further investigated [
59].
In comparison to the PEI [
2,
17], PEN-13 describes patient enablement in greater detail; at the same time, it does not presuppose any prior intervention but can be used as a general patient-reported outcome across (and independently from) specific medical conditions. PEN-13 is also the first German-language instrument measuring patient enablement. A study published in 2017 [
60] indicates that there is an interest in patient enablement assessment. Furthermore, PEN-13 could also be an alternative to PAM-13 for those researchers who consider to assess a patient-related outcome but are not bound and determined to specifically assess patient activation (including the ‘belief component’) or patient empowerment (including the ‘power’ component). As the connotation of the ‘enabled patient’ is smaller than the connotation of both the ‘activated patient’ and ‘empowered patient’, hence its conceptual scope is larger—as has been explained in the introduction (see
Figure 1 and
Figure 2). Under certain research conditions and perspectives, this could be an advantage.
So far, only one aspect of reliability (internal consistency) has been checked; thus PEN-13′s test-retest reliability remains to be demonstrated. This holds also for the responsiveness of the instrument.
We should be aware of a possible response bias in our study: Participants who responded to our survey are likely to be those who are concerned with health care and personal health and have a greater interest in these issues. Furthermore, it is unclear whether and to what extent the selection of the survey participants as enrollees of a regional integrated health care system limits the external validity of the results. Therefore we consider it reasonable to verify the results in a different sample or setting. Furthermore, the study design did not allow insights into the process, causalities and predictive power of patient enablement. In future studies, the responsiveness of the instrument should be checked.

 ,
, 




{kind=link}
{kind=link}
{kind=link}