Characteristics of a Nationwide Voluntary Antibiotic Resistance Awareness Campaign in India; Future Paths and Pointers for Resource Limited Settings/Low and Middle Income Countries

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Campaign Participation
2.3. Campaign Characteristics
3. Results
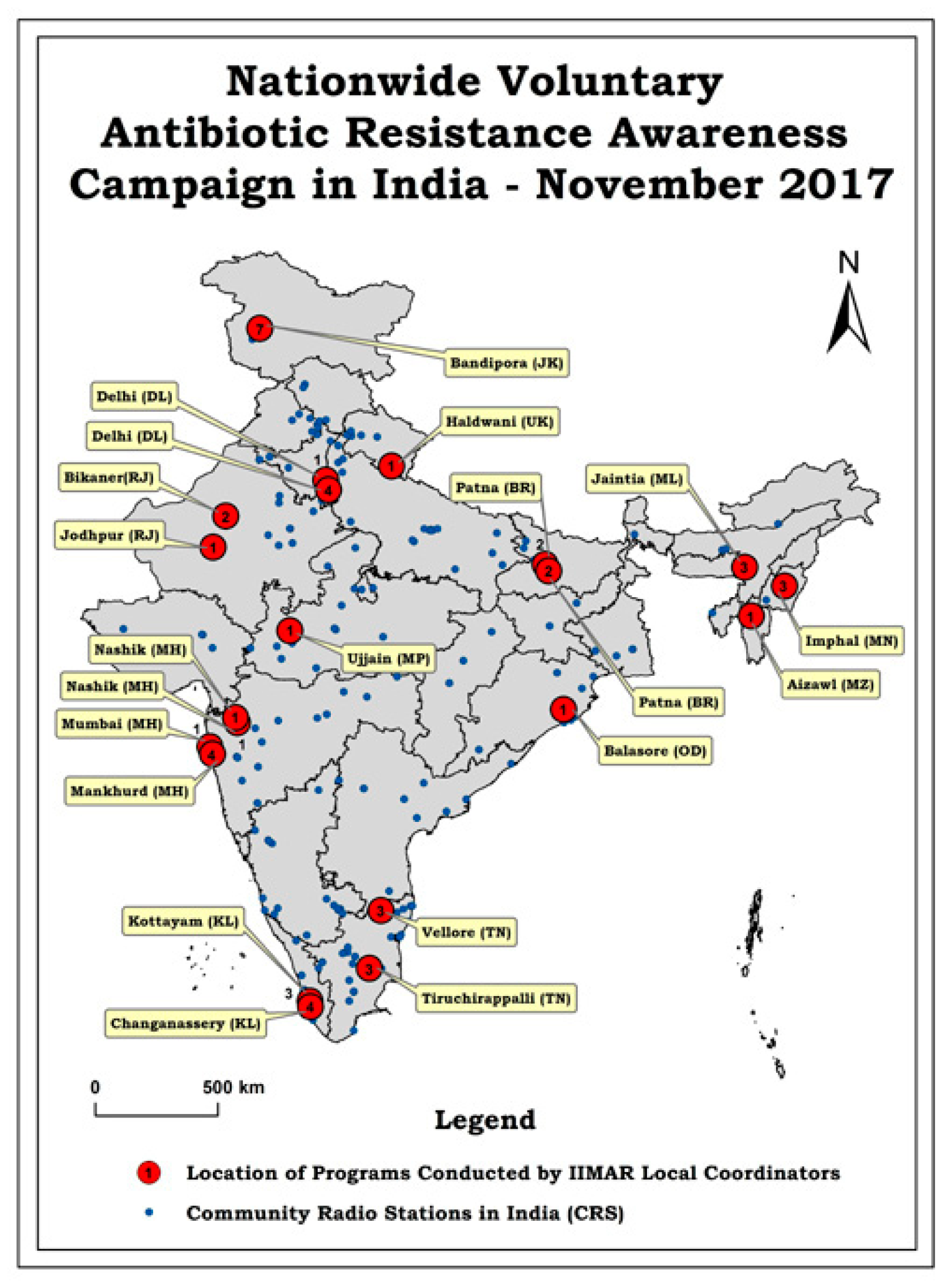
3.1. Campaign Participation and Spread
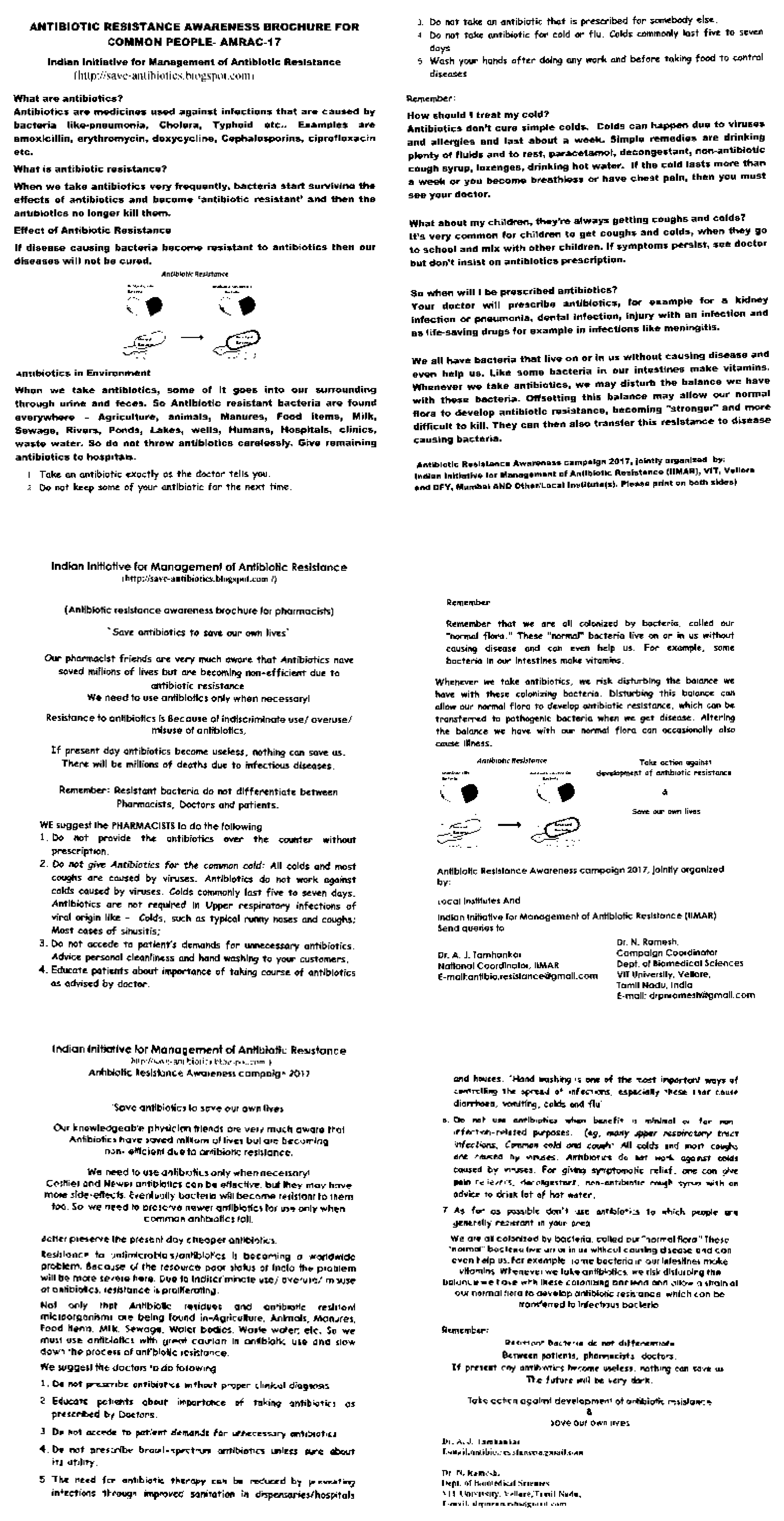
3.2. Campaign Components
3.3. Campaign Characteristics
4. Discussion
4.1. Campaign Components and Characteristics
4.2. Future Paths
5. Conclusions
Significance and Pointers for Resource Constrained Settings/Low and Middle Income Countries
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Available online: https://www.who.int/antimicrobial-resistance/en/ (accessed on 20 October 2019).
- Rao, M.; Rao, K.D.; Kumar, A.S.; Chatterjee, M.; Sundararaman, T. Human resources for health in India. Lancet 2011, 377, 587–598. [Google Scholar] [CrossRef]
- Morgan, D.J.; Okeke, I.N.; Laxminarayan, R.; Perencevich, E.N.; Weisenberg, S. Non-prescription antimicrobial use worldwide: A systematic review. Lancet Infect. Dis. 2011, 11, 692–701. [Google Scholar] [CrossRef] [Green Version]
- Khare, S.; Purohit, M.; Sharma, M.; Tamhankar, A.J.; Lundborg, C.S.; Diwan, V.; Pathak, A. Antibiotic Prescribing by Informal Healthcare Providers for Common Illnesses: A Repeated Cross-Sectional Study in Rural India. Antibiotics 2019, 8, 139. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.who.int/drugresistance/documents/surveillancereport/en/ (accessed on 5 August 2019).
- O’Neill, J. Antimicrobial resistance: Tackling a crisis for the health and wealth of nations. Rev. Antimicrob. Resist. 2014, 20, 1–16. Available online: http://amr-review.org/Publications (accessed on 5 August 2019).
- Available online: http://www.wpro.who.int/entity/drug_resistance/resources/global_action_plan_eng.pdf (accessed on 5 August 2019).
- Available online: www.searo.who.int/india/topics/antimicrobial_resistance/nap_amr.pdf (accessed on 5 August 2019).
- Available online: http://save-antibiotics.blogspot.com/2017/08/ (accessed on 5 August 2019).
- Available online: http://www.who.int/campaigns/world-antibiotic-awareness-week/2017/event/en/ (accessed on 5 August 2019).
- Rogers Van Katwyk, S.; Grimshaw, J.M.; Nkangu, M.; Nagi, R.; Mendelson, M.; Taljaard, M.; Hoffman, S.J. Government policy interventions to reduce human antimicrobial use: A systematic review and evidence map. PLoS Med. 2019, 16, e1002819. [Google Scholar] [CrossRef] [Green Version]
- Available online: http://worldpopulationreview.com/countries/india-population/ (accessed on 5 August 2019).
- Available online: https://docs.google.com/forms/d/e/1FAIpQLScnwZpTOFtV-gjY_iISdr53-ykjZCMUDjyTmqyko9IEVHp_Yg/viewform?vc=0&c=0&w=1 (accessed on 5 August 2019).
- Available online: http://save-antibiotics.blogspot.com (accessed on 5 August 2019).
- Smith, R.A.; Quesnell, M.; Glick, L.; Hackman, N.; Mikanatha, N.M. Preparing for Antibiotic Resistance Campaigns: A Person-centered Approach to Audience Segmentation. J. Health Commun. 2015, 20, 1433–1440. [Google Scholar] [CrossRef] [Green Version]
- Gerding, D.N. The search for good antimicrobial stewardship. Jt. Comm. J. Qual. Improv. 2001, 27, 403–404. [Google Scholar] [CrossRef]
- Kotler, P.; Lee, N. Social Marketing: Influencing Behaviors for Good, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2008. [Google Scholar]
- Anand, S.; Fan, V. The Health Workforce in India. Human Resources for Health Observer, Series no. 16; World Health Organization: Geneva, Switzerland, 2016; ISBN 978 92 4 151052 3. [Google Scholar]
- Tabing, L. How to do Community Radio: A Primer for CR Operators. UNESCO 2002, 11, 24–36. [Google Scholar]
- Available online: https://mib.gov.in/sites/default/files/List%20of%20238%20Operational%20CRS%20as%20on%2023.08.18.pdf (accessed on 5 August 2019).
- Available online: https://mib.gov.in/sites/default/files/AMS%20Report%20on%20CRS.pdf (accessed on 5 August 2019).
- Available online: www.censusindia.gov.in/2011census/hh-series/HH-1/DDW-HH01-0000-2011.XLS (accessed on 5 August 2019).
- Available online: https://www.collinsdictionary.com/dictionary/english/campaign (accessed on 5 August 2019).
- Stålsby Lundborg, C.; Tamhankar, A.J. Understanding and changing human behaviour—Antibiotic mainstreaming as an approach to facilitate modification of provider and consumer behavior. Upsala. J. Med. Sci. 2014, 119, 125–133. [Google Scholar] [CrossRef]
- Available online: https://www.who.int/selection_medicines/committees/expert/21/applications/s6_antibiotic_awareness_campaigns.pdf (accessed on 5 August 2019).
- Huttner, B.; Harbarth, S. Antibiotics Are Not Automatic Anymore—The French National Campaign to Cut Antibiotic Overuse. PLoS Med. 2009, 6, e1000080. [Google Scholar] [CrossRef] [Green Version]
- Molstad, S.; Lofmark, S.; Carin, K.; Erntell, M.; Aspevall, O.; Blad, L.; Hanberger, H.; Hedin, K.; Hellman, J.; Norman, C.; et al. Lessons learnt during 20 years of the Swedish strategic programme against antibiotic resistance. Bull. World Health Organ. 2017, 95, 764–773. [Google Scholar] [CrossRef]
- Chaintarli, K.; Ingle, S.M.; Bhattacharya, A.; Ashiru-Oredope, D.; Oliver, I.; Gobin, M. Impact of a United Kingdom-wide campaign to tackle antimicrobial resistance on self-reported knowledge and behavior change. BMC Public Health 2016, 16, 393. [Google Scholar] [CrossRef] [Green Version]
- Plachouras, D.; Antoniadou, A.; Giannitsioti, E.; Galani, L.; Katsarolis, I.; Kavatha, L.; Koukos, J.; Panagopoulos, P.; Papadopoulos, A.; Poulakou, G. Promoting prudent use of antibiotics: The experience from a multifaceted regional campaign in Greece. BMC Public Health 2014, 14, 866. [Google Scholar] [CrossRef] [Green Version]
- Adriaenssens, N.; De Corte, S.; Coenen, S.; Grieten, E.; Goossens, H. Implementation of e-Bug in Belgium. J. Antimicrob. Chemother. 2011, 66, v51–v53. [Google Scholar] [CrossRef]
- Sumpradit, N.; Chongtrakul, P.; Anuwong, K.; Pumtong, S.; Kongsomboon, K.; Butdeemee, P.; Khonglormyati, J.; Chomyong, C.; Tongyoung, P.; Losiriwat, S. Antibiotics Smart Use: A workable model for promoting the rational use of medicines in Thailand. Bull. World Health Organ. 2012, 90, 905–913. [Google Scholar] [CrossRef]
- Travasso, C. India draws a red line under antibiotic misuse. BMJ 2016, 352, i1202. [Google Scholar] [CrossRef]
- Curry, M.; Sung, L.; Arroll, B.; Goodyear-Smith, F.; Kerse, N.; Norris, P. Public views and use of antibiotics for the common cold before and after an education campaign in New Zealand. N. Z. Med. J. 2006, 119, U1957. [Google Scholar]
- Available online: https://www.safetyandquality.gov.au/our-work/healthcare-associated-infection/antimicrobial-stewardship/antibiotic-awareness-week/ (accessed on 5 August 2019).
- Earnshaw, S.; Monnet, D.L.; Duncan, B.; O’Toole, J.; Ekdahl, K.; Goossens, H. European Antibiotic Awareness Day Technical Advisory Committee; European Antibiotic Awareness Day Collaborative Group. European Antibiotic Awareness Day, 2008-the first Europe-wide public information campaign on prudent antibiotic use: Methods and survey of activities in participating countries. Euro. Surveill. 2009, 14, 19280. [Google Scholar]
- Huttner, B.; Goossens, H.; Verheij, T.; Harbarth, S.; CHAMP consortium. Characteristics and outcomes of public campaigns aimed at improving the use of antibiotics in outpatients in high-income countries. Lancet Infect. Dis. 2010, 10, 17–31. [Google Scholar] [CrossRef]
- Formoso, G.; Paltrinieri, B.; Maria, A.; Gagliotti, C.; Pan, A.; Moro, M.L.; Capelli, O.; Magrini, M. Feasibility and effectiveness of a low cost campaign on antibiotic prescribing in Italy: Community level, controlled, non-randomised trial. BMJ 2013, 5391, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Lambert, M.F.; Masters, G.A.; Brent, S.L. Can mass media campaigns change antimicrobial prescribing? A regional evaluation study. J. Antimicrob. Chemother. 2007, 59, 537–543. [Google Scholar] [CrossRef] [Green Version]
- Mcnulty, C.A.M.; Nichols, T.; Boyle, P.J.; Woodhead, M.; Davey, P. The English antibiotic awareness campaigns: Did they change the public’s knowledge of and attitudes to antibiotic use? J. Antimicrob. Chemother. 2010, 65, 1526–1533. [Google Scholar] [CrossRef]
- Sabuncu, E.; David, J.; Bernède-Bauduin, C.; Pépin, S.; Leroy, M.; Boëlle, P.Y.; Watier, L.; Guillemot, D. Significant reduction of antibiotic use in the community after a nationwide campaign in France, 2002–2007. PLoS Med. 2009, 6, e1000084. [Google Scholar] [CrossRef] [Green Version]
- Kardas-Sloma, L.; Boëlle, P.-Y.; Opatowski, L.; Guillemot, D.; Temime, L. Antibiotic reduction campaigns do not necessarily decrease bacterial resistance: The example of methicillin-resistant Staphylococcus aureus. Antimicrob. Agents. Chemother. 2013, 57, 4410–4416. [Google Scholar] [CrossRef] [Green Version]
- Haenssgen, M.J.; Charoenboon, N.; Zanello, G.; Mayxay, M.; Tsochas, F.R.; Jones, C.O.H.; Kosaikanont, R.; Praphattong, P.; Manohan, P.; Lubell, Y.; et al. Antibiotics and activity spaces: Protocol of an exploratory study of behaviour, marginalisation and knowledge diffusion. BMJ Glob. Health 2018, 3, e000621. [Google Scholar] [CrossRef] [Green Version]
- Laxminarayan, R.; Sridhar, D.; Blaser, M.; Wang, M.; Woolhouse, M. Achieving global targets for antimicrobial resistance. Science 2016, 353, 874–875. [Google Scholar] [CrossRef] [Green Version]
- Gandra, S.; Joshi, J.; Trett, A.; Laxminarayan, R. Scoping Report on Antimicrobial Resistance in India; Center for Disease Dynamics, Economics Policy: Washington, DC, USA, 2017. [Google Scholar]
- Team, C. Chennai Declaration: 5-year plan to tackle the challenge of anti-microbial resistance. Indian J. Med. Microbiol. 2014, 32, 221–228. [Google Scholar] [CrossRef]
- Van Boeckel, T.P.; Gandra, S.; Ashok, A.; Caudron, Q.; Grenfell, B.T.; Levin, S.A.; Laxminarayan, R. Global antibiotic consumption 2000 to 2010: An analysis of national pharmaceutical sales data. Lancet Infect. Dis. 2014, 14, 742–750. [Google Scholar] [CrossRef]
- Farooqui, H.H.; Selvaraj, S.; Mehta, A.; Heymann, D.L. Community level antibiotic utilization in India and its comparison vis-à-vis European countries: Evidence from pharmaceutical sales data. PLoS ONE 2018, 13, e0204805. [Google Scholar] [CrossRef] [Green Version]
- Tamhankar, A.J.; Karnik, S.S.; Stålsby Lundborg, C. Determinants of Antibiotic Consumption-Development of a Model using Partial Least Squares Regression based on Data from India. Sci. Rep. 2018, 8, 6421. [Google Scholar] [CrossRef] [Green Version]
- Available online: http://antibioticguardian.com/ (accessed on 5 August 2019).
- Wernli, D.; Jørgensen, P.S.; Morel, C.M.; Carroll, S.; Harbarth, S.; Levrat, N.; Pittet, D. Mapping global policy discourse on antimicrobial resistance. BMJ Global Health 2017, 2, e000378. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Range | Median |
|---|---|---|
| Coordinator’s age (Years) | 25–73 | 40 |
| Number of Co-Coordinators | 1–10 | 2 |
| Number of Volunteers | 1–10 | 3 |
| Expenditure 1/Event (INR)(USD) *** | Nil *–50,000 (775) | 3000 (47) |
| Planning and organization 2 (days) | 1–15 | 1 |
| Programme (days)/Time (h) | 1–7/2–8 | 4/4 |
| Direct Outreach of the message (Individuals/Event) | 50–200,000 ** | 250 |
| Indirect outreach of the message (Individuals/Event) | 10–50,000 | 500 |
| Positive change in Antibiotic related behavior (Individuals/Event) 3 | 50–4500 | 100 |
| Characteristic | Yes (%) | No (%) | Maybe (%) |
|---|---|---|---|
| Did you face difficulties in conducting the program? | 53 | 47 | 0 |
| Will you participate in the campaign again? | 84 | 16 | 0 |
| Will you be supported again by the same funders? | 90 | 0 | 10 |
| Did any other agency conduct awareness programs at your place during the AMR week? | 5 + 5 * | 58 | 32 ** (Did not know) |
| Did the campaign create adequate awareness about prudent use of antibiotics? | 84 | 5 | 11 |
| Did the campaign create adequate awareness about antibiotic resistance? | 79 | 5 | 16 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamhankar, A.J.; Nachimuthu, R.; Singh, R.; Harindran, J.; Meghwanshi, G.K.; Kannan, R.; Senthil Kumar, N.; Negi, V.; Jacob, L.; Bhattacharyya, S.; et al. Characteristics of a Nationwide Voluntary Antibiotic Resistance Awareness Campaign in India; Future Paths and Pointers for Resource Limited Settings/Low and Middle Income Countries. Int. J. Environ. Res. Public Health 2019, 16, 5141. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245141
Tamhankar AJ, Nachimuthu R, Singh R, Harindran J, Meghwanshi GK, Kannan R, Senthil Kumar N, Negi V, Jacob L, Bhattacharyya S, et al. Characteristics of a Nationwide Voluntary Antibiotic Resistance Awareness Campaign in India; Future Paths and Pointers for Resource Limited Settings/Low and Middle Income Countries. International Journal of Environmental Research and Public Health. 2019; 16(24):5141. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245141
Chicago/Turabian StyleTamhankar, Ashok J., Ramesh Nachimuthu, Ravikant Singh, Jyoti Harindran, Gautam Kumar Meghwanshi, Rajesh Kannan, Nachimuthu Senthil Kumar, Vikrant Negi, Lijy Jacob, Sayan Bhattacharyya, and et al. 2019. "Characteristics of a Nationwide Voluntary Antibiotic Resistance Awareness Campaign in India; Future Paths and Pointers for Resource Limited Settings/Low and Middle Income Countries" International Journal of Environmental Research and Public Health 16, no. 24: 5141. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16245141