Perceived Community Support, Users’ Interactions, and Value Co-Creation in Online Health Community: The Moderating Effect of Social Exclusion


Abstract
:1. Introduction
2. Literature Review
2.1. User Participation in Online Communities
2.2. Interpersonal Interactions in Online Health Communities
3. Hypotheses Development
3.1. Perceived Community Support and User Interactions
3.2. Users’ Interaction and Value Co-Creation
3.3. Perceived Co-Created Value and Continuous Participation Intention
3.4. Role of User-Perceived Social Exclusion
4. Methods
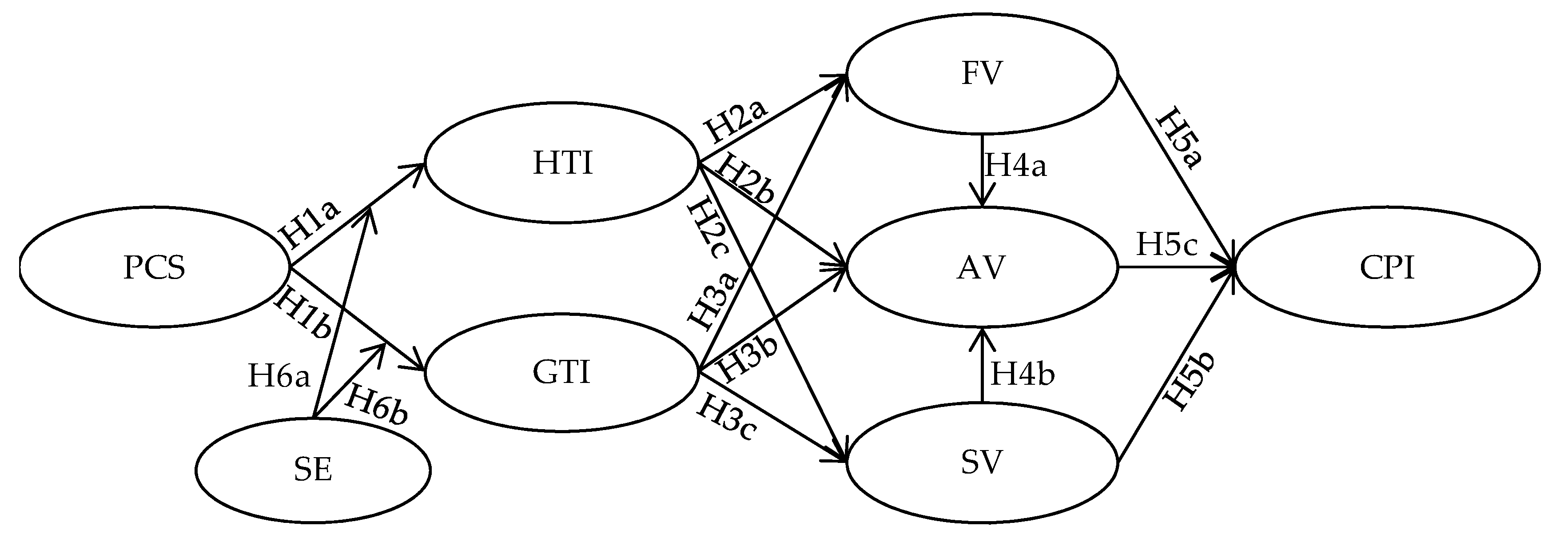
4.1. Research Model and Measurement
4.2. Samples
4.3. Test of Reliability and Validity
5. Hypothesis Test
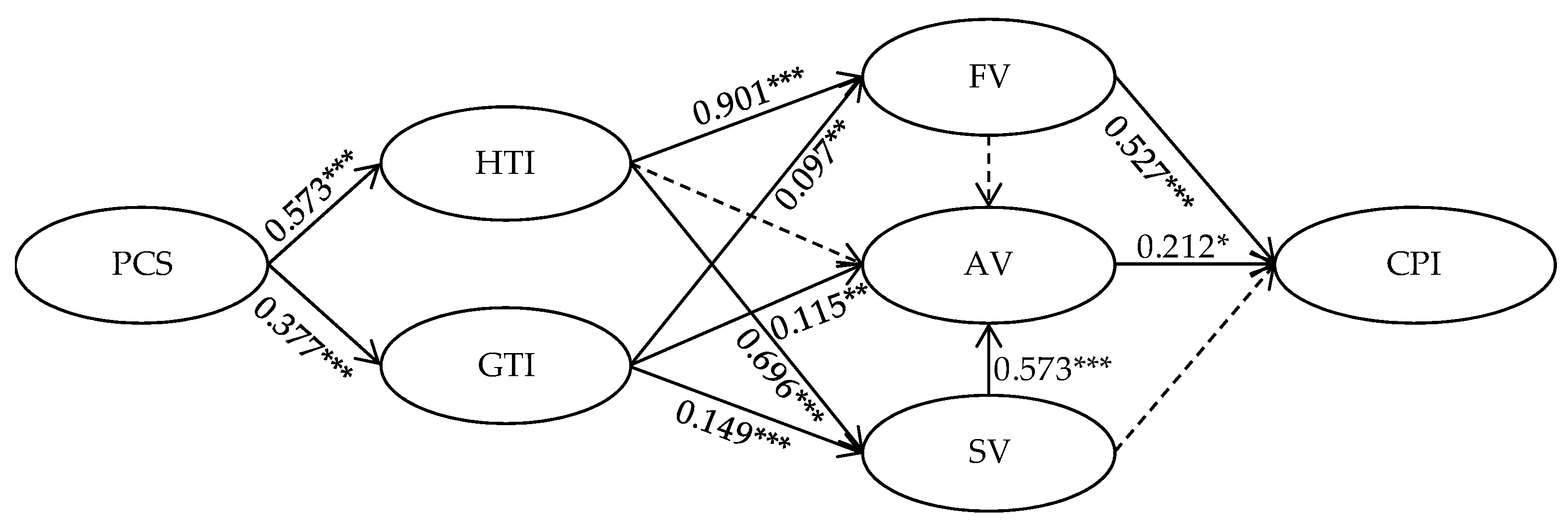
5.1. Summary of Path Analysis Results
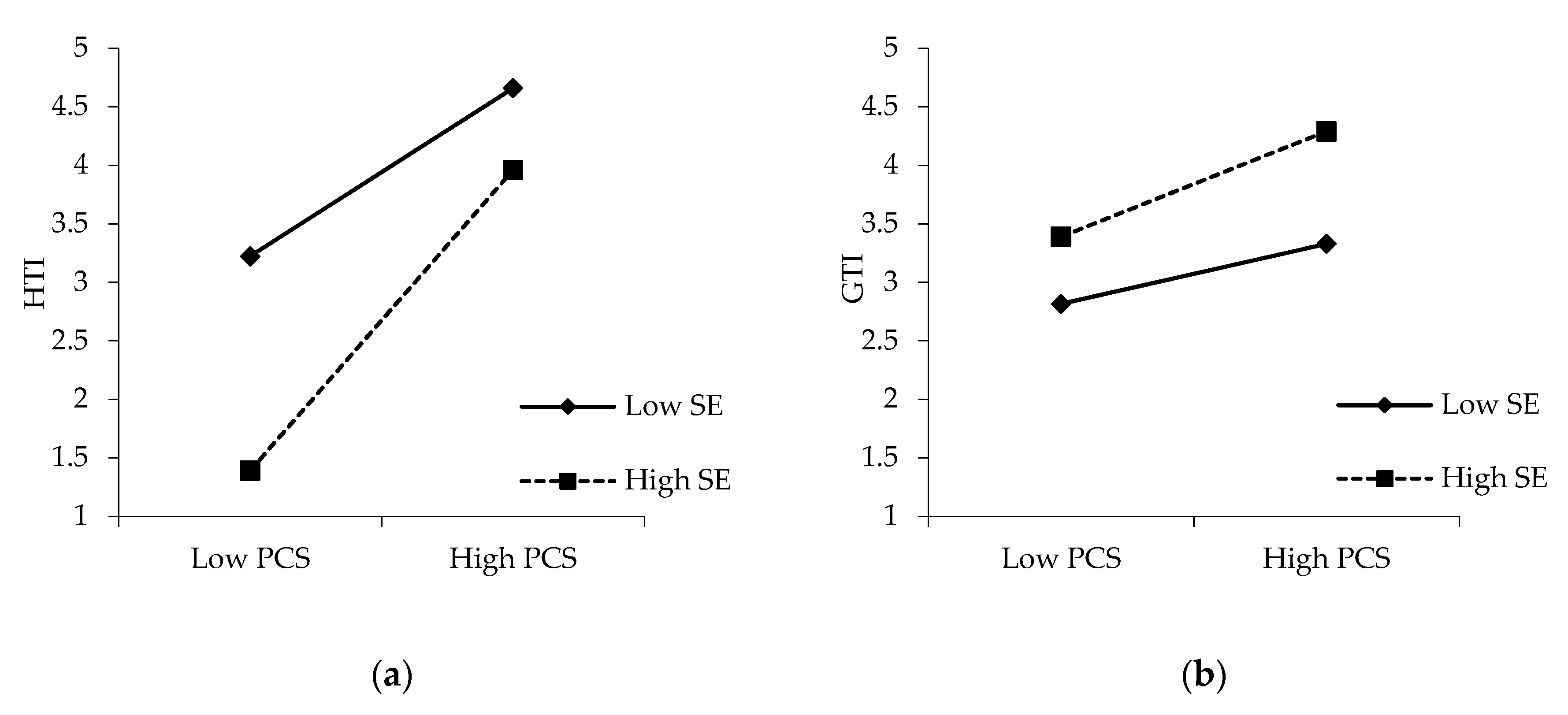
5.2. Moderating Effect of Social Exclusion
6. Discussion
6.1. Theoretical Implications
6.2. Practical Implications
6.3. Limitations and Future Research
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pew Research Center. Health Online 2013. Available online: https://www.pewinternet.org/2013/01/15/health-online-2013/ (accessed on 15 January 2013).
- Yang, H.; Guo, X.; Wu, T.; Ju, X. Exploring the effects of patient-generated and system-generated information on patients’ online search, evaluation and decision. Electron. Commer. Res. Appl. 2015, 14, 192–203. [Google Scholar] [CrossRef]
- Yan, L.; Tan, Y. Feeling blue? Go online: An empirical study of social support among patients. Inf. Syst. Res. 2014, 25, 690–709. [Google Scholar] [CrossRef]
- Guo, X.; Guo, S.; Vogel, D.; Li, Y. Online healthcare community interaction dynamics. J. Manag. Sci. Eng. 2016, 1, 58–74. [Google Scholar] [CrossRef]
- Malinen, S. Understanding user participation in online communities: A systematic literature review of empirical studies. Comput. Hum. Behav. 2015, 46, 228–238. [Google Scholar] [CrossRef]
- Huh, J.; Kwon, B.C.; Kim, S.H.; Lee, S.; Choo, J.; Kim, J.; Choi, M.; Yi, J.S. Personas in online health communities. J. Biomed. Inform. 2016, 63, 212–225. [Google Scholar] [CrossRef] [PubMed]
- Yan, Z.; Wang, T.; Chen, Y.; Zhang, H. Knowledge sharing in online health communities: A social exchange theory perspective. Inf. Manag. 2016, 53, 643–653. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, S.; Deng, Z.; Chen, X. Knowledge sharing motivations in online health communities: A comparative study of health professionals and normal users. Comput. Hum. Behav. 2017, 75, 797–810. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, S.; Chen, X.; Wang, L.; Gao, B.; Zhu, Q. Health information privacy concerns, antecedents, and information disclosure intention in online health communities. Inf. Manag. 2018, 55, 482–493. [Google Scholar] [CrossRef]
- Luo, N.; Zhang, M.; Hu, M.; Wang, Y. How community interactions contribute to harmonious community relationships and customers’ identification in online brand community. Int. J. Inf. Manag. 2016, 36, 673–685. [Google Scholar] [CrossRef]
- Yang, X.; Li, G.; Huang, S.S. Perceived online community support, member relations, and commitment: Differences between posters and lurkers. Inf. Manag. 2017, 54, 154–165. [Google Scholar] [CrossRef]
- Ye, H.J.; Feng, Y.; Choi, B.C.F. Understanding knowledge contribution in online knowledge communities: A model of community support and forum leader support. Electron. Commer. Res. Appl. 2015, 14, 34–45. [Google Scholar] [CrossRef]
- Eisenberger, R.; Huntington, R.; Hutchison, S.; Sowa, D. Perceived organizational support. J. Appl. Psychol. 1986, 71, 500–507. [Google Scholar] [CrossRef]
- Eisenberger, R.; Armeli, S.; Rexwinkel, B.; Lynch, P.D.; Rhoades, L. Reciprocation of perceived organizational support. J. Appl. Psychol. 2001, 86, 42–51. [Google Scholar] [CrossRef]
- Robert, W.H. Supportive organizational climate and managerial assessment of MBO effectiveness. Acad. Manag. J. 1976, 19, 560–576. [Google Scholar] [CrossRef]
- Chiu, C.; Huang, H.; Cheng, H.; Sun, P. Understanding online community citizenship behaviors through social support and social identity. Int. J. Inf. Manag. 2015, 35, 504–519. [Google Scholar] [CrossRef]
- Fiedler, M.; Sarstedt, M. Influence of community design on user behaviors in online communities. J. Bus. Res. 2014, 67, 2258–2268. [Google Scholar] [CrossRef]
- Guan, T.; Wang, L.; Jin, J.; Song, X. Knowledge contribution behavior in online Q&A communities: An empirical investigation. Comput. Hum. Behav. 2018, 81, 137–147. [Google Scholar] [CrossRef]
- Jadin, T.; Gnambs, T.; Batinic, B. Personality traits and knowledge sharing in online communities. Comput. Hum. Behav. 2013, 29, 210–216. [Google Scholar] [CrossRef]
- Kuo, Y.; Feng, L. Relationships among community interaction characteristics, perceived benefits, community commitment, and oppositional brand loyalty in online brand communities. Int. J. Inf. Manag. 2013, 33, 948–962. [Google Scholar] [CrossRef]
- Lai, H.; Chen, T.T. Knowledge sharing in interest online communities: A comparison of posters and lurkers. Comput. Hum. Behav. 2014, 35, 295–306. [Google Scholar] [CrossRef]
- Yuan, D.; Lin, Z.; Zhuo, R. What drives consumer knowledge sharing in online travel communities?: Personal attributes or e-service factors? Comput. Hum. Behav. 2016, 63, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Molly, W.; Samer, F. Why should I share? Examining social capital and knowledge contribution in electronic networks of practice. MIS Q. 2005, 29, 35–57. [Google Scholar] [CrossRef]
- Busser, J.A.; Shulga, L.V. Co-created value: Multidimensional scale and nomological network. Tour. Manag. 2018, 65, 69–86. [Google Scholar] [CrossRef]
- Zhang, X.; Wu, Y.; Liu, S. Exploring short-form video application addiction: Socio-technical and attachment perspectives. Telemat. Inf. 2019, 42, 101243. [Google Scholar] [CrossRef]
- Yilmaz, R. Knowledge sharing behaviors in e-learning community: Exploring the role of academic self-efficacy and sense of community. Comput. Hum. Behav. 2016, 63, 373–382. [Google Scholar] [CrossRef]
- Chen, C.; Hung, S. To give or to receive? Factors influencing members’ knowledge sharing and community promotion in professional virtual communities. Inf. Manag. 2010, 47, 226–236. [Google Scholar] [CrossRef]
- Chiu, C.; Hsu, M.; Wang, E.T.G. Understanding knowledge sharing in virtual communities: An integration of social capital and social cognitive theories. Decis. Support Syst. 2006, 42, 1872–1888. [Google Scholar] [CrossRef]
- Marett, K.; Joshi, K.D. The decision to share information and rumors: Examining the role of motivation in an online discussion forum. Commun. Assoc. Inf. Syst. 2009, 24, 47–68. [Google Scholar] [CrossRef] [Green Version]
- Oh, S. The characteristics and motivations of health answerers for sharing information, knowledge, and experiences in online environments. J. Am. Soc. Inf. Sci. Technol. 2012, 63, 543–557. [Google Scholar] [CrossRef]
- Phang, C.; Kankanhalli, A.; Sabherwal, R. Usability and sociability in online communities: A comparative study of knowledge seeking and contribution. J. Assoc. Inf. Syst. 2009, 10, 721–747. [Google Scholar] [CrossRef]
- Nambisan, S.; Baron, R.A. Virtual customer environments: Testing a model of voluntary participation in value co-creation activities. J. Prod. Innov. Manag. 2009, 26, 388–406. [Google Scholar] [CrossRef]
- McAlexander, J.H.; Schouten, J.W.; Koenig, H.F. Building brand community. J. Mark. 2018, 66, 38–54. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.L. Social media engagement: What motivates user participation and consumption on YouTube? Comput. Hum. Behav. 2017, 66, 236–247. [Google Scholar] [CrossRef]
- Kim, M.; Kim, H. The effect of online fan community attributes on the loyalty and cooperation of fan community members: The moderating role of connect hours. Comput. Hum. Behav. 2017, 68, 232–243. [Google Scholar] [CrossRef]
- Yadav, M.S.; Varadarajan, R. Interactivity in the electronic marketplace: An exposition of the concept and implications for research. J. Acad. Mark. Sci. 2005, 33, 585–603. [Google Scholar] [CrossRef]
- Phang, C.W.; Zhang, C.; Sutanto, J. The influence of user interaction and participation in social media on the consumption intention of niche products. Inf. Manag. 2013, 50, 661–672. [Google Scholar] [CrossRef]
- Sun, N.; Rau, P.P.; Ma, L. Understanding lurkers in online communities: A literature review. Comput. Hum. Behav. 2014, 38, 110–117. [Google Scholar] [CrossRef]
- Lin, T.; Hsu, J.S.; Cheng, H.; Chiu, C. Exploring the relationship between receiving and offering online social support: A dual social support model. Inf. Manag. 2015, 52, 371–383. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, M.; Luo, N.; Wang, Y.; Niu, T. Understanding the formation mechanism of high-quality knowledge in social question and answer communities: A knowledge co-creation perspective. Int. J. Inf. Manag. 2019, 48, 72–84. [Google Scholar] [CrossRef]
- Shin, Y.; Hur, W.M.; Moon, T.W.; Lee, S. A motivational perspective on job insecurity: Relationships between job insecurity, intrinsic motivation, and performance and behavioral outcomes. Int. J. Environ. Res. Public Health 2019, 16, 1812. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Fang, Y.; Lim, K.H. Understanding knowledge contributors’ satisfaction in transactional virtual communities: A cost–benefit trade-off perspective. Inf. Manag. 2014, 51, 441–450. [Google Scholar] [CrossRef]
- Yuqing, R.; Kraut, R.; Kiesler, S. Applying common identity and bond theory to design of online communities. Organ. Stud. 2007, 28, 377–408. [Google Scholar] [CrossRef]
- Yao, T.; Zheng, Q.; Fan, X. The impact of online social support on patients’ quality of life and the moderating role of social exclusion. J. Serv. Res. 2015, 18, 369–383. [Google Scholar] [CrossRef]
- Johnson, S.L.; Safadi, H.; Faraj, S. The emergence of online community leadership. Inf. Syst. Res. 2015, 26, 165–187. [Google Scholar] [CrossRef] [Green Version]
- Sen, Y.; Elmas, S. Effects of supportive organizational climate and positive psychological capital on organizational citizenship behavior. Eu. J. Bus. Manag. 2015, 7, 62–67. [Google Scholar]
- Feng, Y.; Ye, H. Why do you return the favor in online knowledge communities? A study of the motivations of reciprocity. Comput. Hum. Behav. 2016, 63, 342–349. [Google Scholar] [CrossRef]
- Gu, D.; Deng, S.; Zheng, Q.; Liang, C.; Wu, J. Impacts of case-based health knowledge system in hospital management: The mediating role of group effectiveness. Inf. Manag. 2019, 56, 1–12. [Google Scholar] [CrossRef]
- Yoo, J.; Arnold, T.J.; Frankwick, G.L. Effects of positive customer-to-customer service interaction. J. Bus. Res. 2012, 65, 1313–1320. [Google Scholar] [CrossRef]
- Georgi, D.; Mink, M. eCCIq: The quality of electronic customer-to-customer interaction. J. Retail. Consum. Serv. 2013, 20, 11–19. [Google Scholar] [CrossRef]
- Wei, W.; Lu, Y.; Miao, L.; Cai, L.A.; Wang, C. Customer-customer interactions (CCIs) at conferences: An identity approach. Tour. Manag. 2017, 59, 154–170. [Google Scholar] [CrossRef] [Green Version]
- Rihova, I.; Buhalis, D.; Gouthro, M.B.; Moital, M. Customer-to-customer co-creation practices in tourism: Lessons from customer-dominant logic. Tour. Manag. 2018, 67, 362–375. [Google Scholar] [CrossRef]
- Lehto, X.Y.; Choi, S.; Lin, Y.; MacDermid, S.M. Vacation and family functioning. Ann. Tour. Res. 2009, 36, 459–479. [Google Scholar] [CrossRef]
- Rosenbaum, M.S. Exploring the social supportive role of third places in consumers’ lives. J. Serv. Res. 2006, 9, 59–72. [Google Scholar] [CrossRef]
- Williams, P.; Soutar, G.N. Value, satisfaction and behavioral intentions in an adventure tourism context. Ann. Tour. Res. 2009, 36, 413–438. [Google Scholar] [CrossRef]
- Sheth, J.N.; Newman, B.I.; Gross, B.L. Why we buy what we buy: A theory of consumption values. J. Bus. Res. 1991, 22, 159–170. [Google Scholar] [CrossRef]
- Schau, H.J.; Muñiz, A.M.; Arnould, E.J. How brand community practices create value. J. Mark. 2009, 73, 30–51. [Google Scholar] [CrossRef]
- Reichenberger, I. C2C value co-creation through social interactions in tourism. Int. J. Tour. Res. 2017, 19, 629–638. [Google Scholar] [CrossRef]
- Zhang, T.C.; Jahromi, M.F.; Kizildag, M. Value co-creation in a sharing economy: The end of price wars? Int. J. Hosp. Manag. 2018, 71, 51–58. [Google Scholar] [CrossRef]
- Muniz, A.M.; O’Guinn, T.C. Brand community. J. Consum. Res. 2001, 27, 412–432. [Google Scholar] [CrossRef]
- Yen, H.R.; Hsu, S.H.; Huang, C. Good soldiers on the web: Understanding the drivers of participation in online communities of consumption. Int. J. Electron. Commer. 2014, 15, 89–120. [Google Scholar] [CrossRef]
- Jin, B.; Park, J.Y.; Kim, H. What makes online community members commit? A social exchange perspective. Behav. Inf. Technol. 2010, 29, 587–599. [Google Scholar] [CrossRef]
- Gu, D.; Guo, J.; Liang, C.; Lu, W.; Zhao, S.; Liu, B.; Long, T. Social media-based health management systems and sustained health engagement: TPB perspective. Int. J. Environ. Res. Public Health. 2019, 16, 1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathwick, C.; Wiertz, C.; de Ruyter, K. Social capital production in a virtual P3 community. J. Consum. Res. 2008, 34, 832–849. [Google Scholar] [CrossRef] [Green Version]
- Kandaurova, M.; Lee, S.H. The effects of Virtual Reality (VR) on charitable giving: The role of empathy, guilt, responsibility, and social exclusion. J. Bus. Res. 2019, 100, 571–580. [Google Scholar] [CrossRef]
- Lin, X.; Li, S.; Qu, C. Social network sites influence recovery from social exclusion: Individual differences in social anxiety. Comput. Hum. Behav. 2017, 75, 538–546. [Google Scholar] [CrossRef]
- Williams, K.D.; Nida, S.A. Ostracism. Curr. Dir. Psychol. Sci. 2011, 20, 71–75. [Google Scholar] [CrossRef]
- Hwang, Y.; Mattila, A.S. Feeling left out and losing control: The interactive effect of social exclusion and gender on brand attitude. Int. J. Hosp. Manag. 2019, 77, 303–310. [Google Scholar] [CrossRef]
- Chiou, W.; Lee, C.; Liao, D. Facebook effects on social distress: Priming with online social networking thoughts can alter the perceived distress due to social exclusion. Comput. Hum. Behav. 2015, 49, 230–236. [Google Scholar] [CrossRef]
- Wright, K. Computer-mediated social support, older adults, and coping. J. Commun. 2000, 50, 100–118. [Google Scholar] [CrossRef]
- Fang, C.; Zhang, J. Users‘ continued participation behavior in social Q&A communities: A motivation perspective. Comput. Hum. Behav. 2019, 92, 87–109. [Google Scholar] [CrossRef]
- Nunnally, J.C. Psychometric Theory; Mcgraw Hill: New York, NY, USA, 1978. [Google Scholar]
- Bagozzi, R.P. Causal Models in Marketing; John Wiley and Sons: New York, NY, USA, 1980. [Google Scholar]
- Podsako, N. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef] [PubMed]
- Gu, D.; Li, J.; Li, X.; Liang, C. Visualizing the knowledge structure and evolution of big data research in healthcare informatics. Int. J. Med. Inform. 2017, 98, 22–32. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Context | Participation Type | Method/Samples | Antecedents | Consequences | Source |
|---|---|---|---|---|---|
| Wikipedia: free online encyclopedia | Knowledge sharing | Survey/256 users | Trendsetting, opinion leadership, prosocial value orientation, intrinsic motivations | -- | [19] |
| Douban: product review community | Level of participation | Secondary data/106 pages of book comment | Inclusiveness, reciprocity, centralization, centralization, core-periphery | Consumption intention | [37] |
| Seven automobile online communities | Product information sharing | Survey/283 users | -- | Learning benefits, social benefits, self-esteem benefits, hedonic benefits | [20] |
| Mobile01: topic-free online community | Knowledge sharing | Survey/324 users | Reputation, reciprocity, enjoyment in helping others, knowledge self-efficacy, moderator’s enthusiasm, offline activities, enjoyability | -- | [21] |
| -- | Online participation | Literature review/-- | Nature of the online community, individual characteristics, degree of commitment, quality requirement | -- | [38] |
| 470 online communities | On-topic discussion, off-topic discussion, generalized reciprocity, direct reciprocity, | Survey/1160 users | Common identity, common bond | -- | [17] |
| Six online knowledge communities | Knowledge contribution | Survey/169 users | Perceived community support, perceived leader support | -- | [12] |
| Online support communities focusing on pregnancy | Willingness to offer support | Survey/212 users | Action-facilitating support, nurturant support, self-efficacy, community identification | -- | [39] |
| Online support communities for pregnant women | Online community citizenship behaviors | Survey/159 users | Subjective well-being, community identification | -- | [16] |
| Facebook learning community | Knowledge-sharing behaviors | Survey/316 undergraduate students | Self-efficacy, sense of community | -- | [26] |
| Bbs.feeyo.com: airline passenger online community | Knowledge sharing | Survey/364 users | Innovativeness, subjective knowledge, perceived ease of use, perceived usefulness | -- | [22] |
| Smartphone’s online brand community | Product-information interaction, human-computer interaction, interpersonal interaction | Survey/665 users | -- | Customer-brand relationship, customer-other customer relationship | [10] |
| Phoenix Health and Sweet Home: OHCs | General knowledge- sharing, specific knowledge-sharing | Survey/323 users | Sense of self-worth, face concern, reputation, social support, cognitive costs, execution costs | -- | [7] |
| Good Doctor, Baby Tree, DXY: OHCs | Knowledge-sharing | Survey/443 users | Reputation, reciprocity, knowledge self-efficacy, altruism, empathy | -- | [8] |
| Zhihu: social Q&A community | Knowledge contribution | Secondary data/3000 users | Identity-based trust, social feedback, identity communication, social exposure, norms of reciprocity | -- | [18] |
| Zhihu: social Q&A community | Knowledge-sharing, knowledge integration | Survey/382 users | Knowledge self-efficacy, topic richness, Personalized recommendation, social interactivity | Community knowledge quality | [40] |
| Construct | Measurement Items | Sources | |
|---|---|---|---|
| Perceived community support (PCS) | PCS1: The online health community provides various types of support for users to interact with each other, such as discussions, comments, reposting, likes, etc. PCS2: The online health community provides various modules to support user interactions on health and other topics PCS3: The online health community provides active users with proper rewards that represent their reputation or status | [7,11] | |
| User interactions | Health topic interactions (HTI) | HTI1: When participating in the online health community, I usually actively share and discuss health information, treatment experience with others. HTI2: When discussing problems related to medical treatment and medical experience, I usually engage in subsequent interactions. | [7,17] |
| General topic interactions (GTI) | GTI1: Members of the online health community interact actively with others on daily life and emotion-related topics. GTI2: Members in the online health community discuss actively public information, such as social, cultural, educational issues. | ||
| Co-created value | Functional value (FV) | FV1: It allows me to increase my knowledge of the disease through members’ interactions FV2: It helps me solve problems associated with my disease through members’ interactions FV3: It helps increase my general knowledge besides health through members’ interactions | [7,20,39] |
| Social value (SV) | SV1: I feel connected through members’ interactions in the online health community SV2: I can expand my social network through participation in community interactions. SV3: I can make friends in the online health community with whom I share common values or interests. | ||
| Affective value (AV) | AV1: I get comfort and care from other members through interactions AV2: I gain happiness through the interactions with other members AV3: I feel a sense of belonging through interactions with other members | ||
| Continuous participation intention (CPI) | CPI1: I will continue participating in the community members’ interactions CPI2: I will take an active part in the discussions in this online health community CPI3: I will continue contributing my knowledge to other members and the community | [12,71] | |
| Social exclusion (SE) | SE1: I feel uneasy when being with others because of my disease SE2: I feel lonely because I have no one to turn to SE3: People are around me but not with me | [40,44] | |
| Demographic Profile | Categories | Frequency | Percent (%) |
|---|---|---|---|
| Gender | Male | 135 | 46.2 |
| Female | 157 | 53.8 | |
| Age | Less than 25 | 21 | 7.2 |
| 26–35 | 106 | 36.3 | |
| 36–45 | 117 | 40.1 | |
| 46 or above | 48 | 16.4 | |
| Education | High school or below | 99 | 33.9 |
| University college | 169 | 57.9 | |
| Graduate school | 24 | 8.2 | |
| Monthly income (RMB) | Less than 3500 | 21 | 7.2 |
| 3501–5000 | 77 | 26.4 | |
| 5001–8000 | 104 | 35.6 | |
| 8000 or above | 90 | 30.8 | |
| Experience in this OHC | Less than 3 months | 26 | 8.9 |
| 3 months-1 year | 138 | 47.3 | |
| 1 year or above | 128 | 43.8 |
| Construct | Items | Cronbach’s α | Convergent Validity | ||
|---|---|---|---|---|---|
| Factor Loading | Composite Reliability | Average Variance Extracted | |||
| PCS | PCS1 | 0.877 | 0.897 | 0.861 | 0.674 |
| PCS2 | 0.789 | ||||
| PCS3 | 0.772 | ||||
| HTI | HTI1 | 0.872 | 0.887 | 0.872 | 0.773 |
| HTI2 | 0.871 | ||||
| GTI | GTI1 | 0.773 | 0.697 | 0.782 | 0.646 |
| GTI2 | 0.898 | ||||
| FV | FV1 | 0.928 | 0.914 | 0.933 | 0.823 |
| FV2 | 0.899 | ||||
| FV3 | 0.908 | ||||
| SV | SV1 | 0.921 | 0.944 | 0.923 | 0.800 |
| SV2 | 0.879 | ||||
| SV3 | 0.858 | ||||
| AV | AV1 | 0.913 | 0.915 | 0.913 | 0.778 |
| AV2 | 0.849 | ||||
| AV3 | 0.881 | ||||
| CPI | CPI1 | 0.901 | 0.878 | 0.885 | 0.719 |
| CPI2 | 0.855 | ||||
| CPI3 | 0.810 | ||||
| SE | SE1 | 0.901 | 0.917 | 0.904 | 0.759 |
| SE2 | 0.834 | ||||
| SE3 | 0.861 | ||||
| χ2/df = 2.263, GFI = 0.905, RFI = 0.919, TLI = 0.953, CFI = 0.967, RMR = 0.036, RMSEA = 0.066 | |||||
| Variables | Mean | SD | SCC | HTI | GTI | FV | SV | AV | CPI | SE |
|---|---|---|---|---|---|---|---|---|---|---|
| SCC | 4.326 | 0.695 | 0.821 | |||||||
| HTI | 3.938 | 0.941 | 0.436 ** | 0.879 | ||||||
| GTI | 4.116 | 0.784 | 0.307 ** | 0.370 ** | 0.804 | |||||
| FV | 3.804 | 0.949 | 0.438 ** | 0.808 ** | 0.389 ** | 0.907 | ||||
| SV | 3.710 | 0.986 | 0.389 ** | 0.644 ** | 0.307 ** | 0.668 ** | 0.894 | |||
| AV | 3.796 | 0.889 | 0.439 ** | 0.703 ** | 0.392 ** | 0.726 ** | 0.789 ** | 0.882 | ||
| CPI | 3.693 | 0.868 | 0.538 ** | 0.767 ** | 0.406 ** | 0.811 ** | 0.688 ** | 0.754 ** | 0.848 | |
| SE | 4.457 | 0.707 | 0.736 ** | 0.191 ** | 0.325 ** | 0.192 ** | 0.273 ** | 0.376 ** | 0.324 ** | 0.871 |
| Effect | Path | Standardized Estimate (β) | Unstandardized Estimate | Lower Bound | Upper Bound | p |
|---|---|---|---|---|---|---|
| Total effect | SV→CPI | 0.226 | 0.174 | 0.118 | 0.231 | 0.001 |
| Direct effect | SV→CPI | 0.105 | 0.081 | −0.027 | 0.187 | 0.122 |
| Indirect effect | SV→AV→CPI | 0.121 | 0.093 | 0.020 | 0.168 | 0.012 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, W.; Fan, X.; Ji, R.; Jiang, Y. Perceived Community Support, Users’ Interactions, and Value Co-Creation in Online Health Community: The Moderating Effect of Social Exclusion. Int. J. Environ. Res. Public Health 2020, 17, 204. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010204
Liu W, Fan X, Ji R, Jiang Y. Perceived Community Support, Users’ Interactions, and Value Co-Creation in Online Health Community: The Moderating Effect of Social Exclusion. International Journal of Environmental Research and Public Health. 2020; 17(1):204. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010204
Chicago/Turabian StyleLiu, Wenlong, Xiucheng Fan, Rongrong Ji, and Yi Jiang. 2020. "Perceived Community Support, Users’ Interactions, and Value Co-Creation in Online Health Community: The Moderating Effect of Social Exclusion" International Journal of Environmental Research and Public Health 17, no. 1: 204. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17010204