A Scoping Review on How to Make Hospitals Health Literate Healthcare Organizations


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Identifying the Research Questions
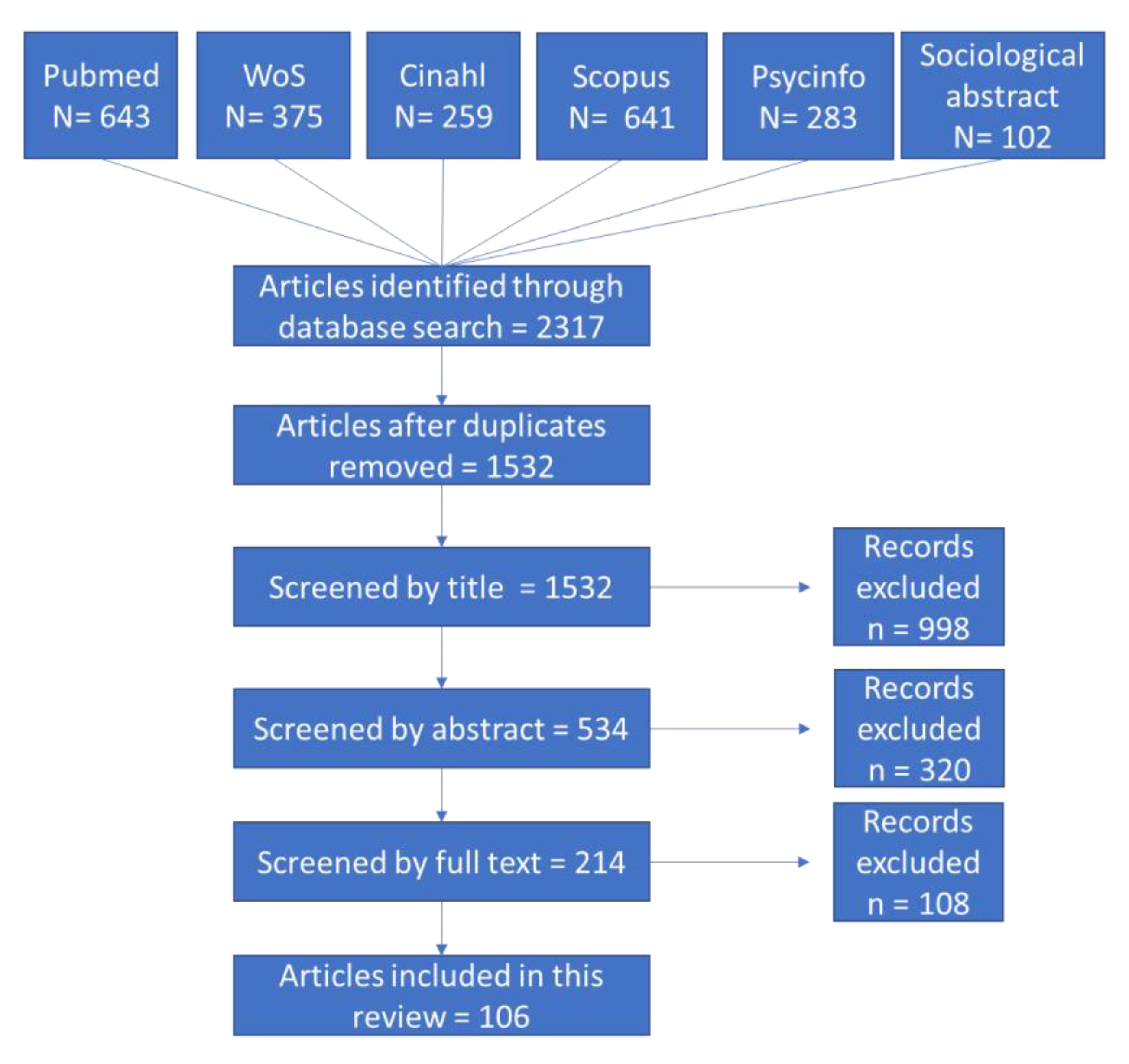
2.2. Identifying Relevant Studies
2.3. Selecting Articles
- Attribute 1 (leadership): studies whose aim was to involve leadership or to assess the effect of leadership involvement;
- Attribute 2 (planning): interventions whose aim was to introduce or test the effect of planning activities related to health literacy. This also includes every intervention aimed at developing or using tools/instruments for assessing organizational health literacy;
- Attribute 3 (workforce): every intervention could evaluate the impact of health literacy training on healthcare workers (HCWs), or whose aim was to develop, change, or adopt health literacy training;
- Attribute 4 (population): studies whose aim was to include the population in the design, implementation, and evaluation of health information and services, or every study assessing the effects of population engagement;
- Attribute 5 (meets the needs of the population): studies whose purpose was to assess the effect of interventions that meet “the needs of populations with a range of health literacy skills while avoiding stigmatization”;
- Attribute 6 (communication): studies whose aim was to implement a communication technique or that assess the effect of implementing communication techniques;
- Attribute 7 (navigation): studies whose aim was to implement or evaluate the impact of interventions to provide easy access to health information, both in the physical and electronic environment;
- Attribute 8 (contents easy to understand): every study whose aim was to assess the suitability of materials for their target audience or the impact of the development/use of suitable material;
- Attribute 9 (high-risk situations): every study where the intervention or outcomes were related to high-risk situations, such as informed consent for surgery, administration of medicines, advanced directives, and transitions in care, such as discharge from the hospital.
- Attribute 10 (payment transparency): studies whose aim was to clarify communications about health service costs to patients or evaluate the impact of interventions that make communications about insurance coverage and costs more transparent.
2.4. Charting the Data
2.5. Collating, Summarising, and Reporting the Results
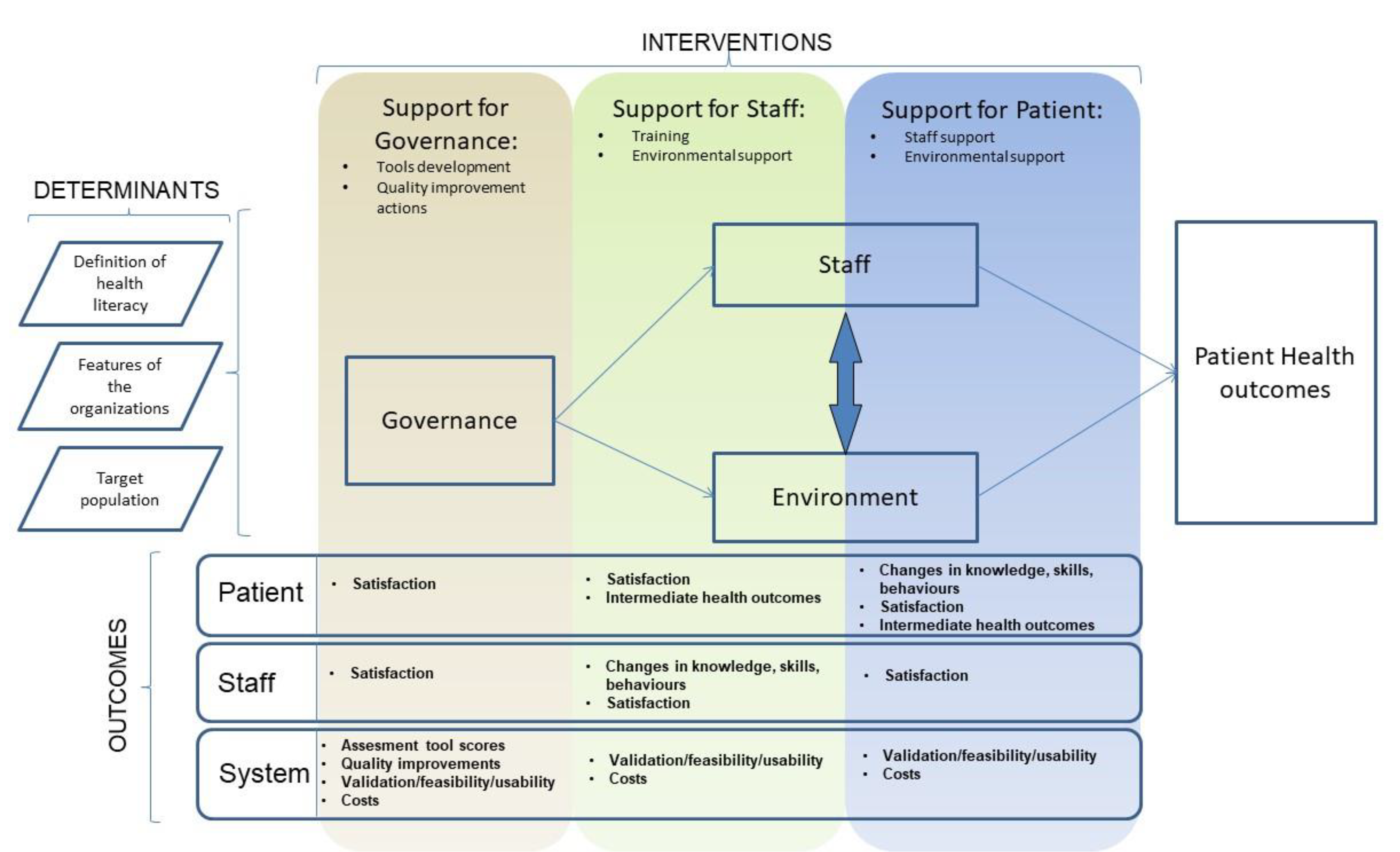
- Support for patients: every intervention was designed to help patients access and use health information better. Patients may receive support directly by health professionals (staff support) or by material, electronic tools, conditions, and objects belonging to the hospital’s structure (environmental support);
- Support for staff: interventions aimed at facilitating health professionals in helping patients. This can be achieved by health literacy training, or by tools/technologies/environments that improve the healthcare worker–patient relationship.
- Support for governance: interventions designed to better evaluate and manage system efforts in becoming an HLHO. This includes all the interventions aimed at developing tools/instruments for assessing organizational health literacy, as well as quality improvement actions related to health literacy: establishing measures, setting aims, specific assessment analysis, forming teams, communicating awareness, developing health literacy improvement plan, testing changes, and tracking progress.
- Patient outcomes: divided into changes in knowledge/skills/behaviors, perception of intervention satisfaction, and patient health outcomes.
- Staff outcomes: including perception of intervention satisfaction and changes in knowledge/skills/behaviors.
- System outcomes: including changes in the scores for tools that assess organizational health literacy, the quality improvements perceived/obtained, measures of validation for the tools developed, and costs.
3. Results
3.1. Interventions (See Table 3 for References)
3.2. Outputs/Outcomes (See Table 4 for References)
3.3. Attributes (See Table 5 for References)
3.4. Logical Framework (Figure 2)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Simonds, S.K. Health education as social policy. Health Educ. Monogr. 1974, 2, 1–25. [Google Scholar] [CrossRef]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H.; (HLS-EU) Consortium Health Literacy Project European. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institute of Medicine. Health Literacy: A Prescription to End Confusion; National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- Batterham, R.W.; Hawkins, M.; Collins, P.A.; Buchbinder, R.; Osborne, R.H. Health literacy: Applying current concepts to improve health services and reduce health inequalities. Public Health 2016, 132, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Baker, D.W. The meaning and the measure of health literacy. J. Gen. Intern. Med. 2006, 21, 878–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nutbeam, D. The evolving concept of health literacy. Soc. Sci. Med. 2008, 67, 2072–2078. [Google Scholar] [CrossRef] [PubMed]
- Rudd, R.E.; Renzulli, D.; Pereira, A.; Daltory, L. Literacy demands in health care settings: The patient perspective. In Understanding Health Literacy: Implications for Medicine and Public Health; Schwartzberg, J.G., Van Geest, J.B., Wang, C.C., Eds.; AMA Press: Chicago, IL, USA, 2005. [Google Scholar]
- Brach, C.; Keller, D.; Hernandez, L.M.; Baur, C.; Parker, R.; Dreyer, B.; Schyve, P.; Lemerise, A.J.; Schillinger, D. Ten Attributes of Health Literate Health Care Organizations; Institute of Medicine of the National Academies: Washington, DC, USA, 2012. [Google Scholar]
- Batterham, R.W.; Buchbinder, R.; Beauchamp, A.; Dodson, S.; Elsworth, G.R.; Osborne, R.H. The OPtimising HEalth LIterAcy (Ophelia) process: Study protocol for using health literacy profiling and community engagement to create and implement health reform. BMC Public Health 2014, 14, 694. [Google Scholar] [CrossRef] [Green Version]
- Abrams, M.A.; Kurtz-Rossi, S.; Riffenburgh, A.; Savage, B.A. Building Health Literate Organizations: A Guidebook to Achieving Organizational Change; UnityPoint Health: West Des Moines, IA, USA, 2014. [Google Scholar]
- Kowalski, C.; Lee, S.Y.; Schmidt, A.; Wesselmann, S.; Wirtz, M.A.; Pfaff, H.; Ernstmann, N. The health literate health care organization 10 item questionnaire (HLHO-10): Development and validation. BMC Health Serv. Res. 2015, 15, 47. [Google Scholar] [CrossRef] [Green Version]
- Altin, S.V.; Lorrek, K.; Stock, S. Development and validation of a brief screener to measure the Health Literacy Responsiveness of Primary Care Practices (HLPC). BMC Fam. Pract. 2015, 16, 122. [Google Scholar] [CrossRef] [Green Version]
- Kripalani, S.; Wallston, K.A.; Cavanaugh, K.L.; Osborn, C.Y.; Mulvaney, S.; McDougald Scott, A.; Rothman, R.L. Measures to Assess a Health Literate Organization Commissioned Report; National Academy of Medicine: Washington, DC, USA, 2014; Available online: http://www.nationalacademies.org/hmd/~/media/Files/Activity%20Files/PublicHealth/HealthLiteracy/Commissioned-Papers/Measures_Assess_HLO.pdf (accessed on 1 July 2019).
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.J.; Godfrey, C.M.; McInerney, P.; Soares, C.B.; Khalil, H.; Parker, D. The Joanna Briggs Institute Reviewers’ Manual 2015: Methodology for JBI Scoping Reviews; Joanna Briggs Institute: Adelaide, Australia, 2015. [Google Scholar]
- Briss, P.A.; Zaza, S.; Pappaioanou, M.; Fielding, J.; Wright-De Agüero, L.; Truman, B.I.; Hopkins, D.P.; Mullen, P.D.; Thompson, R.S.; Woolf, S.H.; et al. Developing an evidence-based guide to community preventive services—methods 1 2. Am. J. Prev. Med. 2000, 18, 35–43. [Google Scholar] [CrossRef]
- Zaza, S.; Carande-Kulis, V.G.; Sleet, D.A.; Sosin, D.M.; Elder, R.W.; Shults, R.A.; Dinh-Zarr, T.B.; Nichols, J.L.; Thompson, R.S. Methods for conducting systematic reviews of the evidence of effectiveness and economic efficiency of interventions to reduce injuries to motor vehicle occupants. Am. J. Prev. Med. 2001, 21 (Suppl. S4), 23–30. [Google Scholar] [CrossRef]
- Bailey, S.C.; Sarkar, U.; Chen, A.H.; Schillinger, D.; Wolf, M.S. Evaluation of Language Concordant, Patient-Centered Drug Label Instructions. J. Gen. Intern. Med. 2012, 27, 1707–1713. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.P.; Schnipper, J.L.; Goggins, K.; Bian, A.; Shintani, A.; Kripalani, S. Effect of Pharmacist Counseling Intervention on Health Care Utilization Following Hospital Discharge: A Randomized Control Trial. J. Gen. Intern. Med. 2016, 31, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Bickmore, T.W.; Pfeifer, L.M.; Jack, B.W. Taking the time to care. In Proceedings of the 27th International Conference on Human Factors in Computing Systems—CHI 09, Boston, MA, USA, 3–9 April 2009. [Google Scholar] [CrossRef]
- Cawthon, C.; Walia, S.; Osborn, C.Y.; Niesner, K.J.; Schnipper, J.L.; Kripalani, S. Improving Care Transitions: The Patient Perspective. J. Health Commun. 2012, 17 (Suppl. S3), 312–324. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Bakken, S. Web-based education for low-literate parents in Neonatal Intensive Care Unit: Development of a website and heuristic evaluation and usability testing. Int. J. Med. Inform. 2010, 79, 565–575. [Google Scholar] [CrossRef] [Green Version]
- Cordasco, K.M.; Asch, S.M.; Bell, D.S.; Guterman, J.J.; Gross-Schulman, S.; Ramer, L.; Elkayam, U.; Franco, I.; Leatherwood, C.L.; Mangione, C.M. A Low-Literacy Medication Education Tool for Safety-Net Hospital Patients. Am. J. Prev. Med. 2009, 37, S209–S216. [Google Scholar] [CrossRef] [Green Version]
- Dankner, R.; Drory, Y.; Geulayov, G.; Ziv, A.; Novikov, I.; Zlotnick, A.Y.; Moshkovitz, Y.; Elami, A.; Schwammenthal, E.; Goldbourt, U. A controlled intervention to increase participation in cardiac rehabilitation. Eur. J. Prev. Cardiol. 2014, 22, 1121–1128. [Google Scholar] [CrossRef]
- Foertsch, L.Y.; Hoffmann, R.L.; Ren, D.; Stolar, J.; Tuite, P.K. Evaluation of a Surgical Site Discharge Teaching Tool Using Pictures and a Mirror. Clin. Nurse Spec. 2016, 30, 101–105. [Google Scholar] [CrossRef]
- Gallagher, R.; Roach, K.; Belshaw, J.; Kirkness, A.; Sadler, L.; Warrington, D. A pre-test post-test study of a brief educational intervention demonstrates improved knowledge of potential acute myocardial infarction symptoms and appropriate responses in cardiac rehabilitation patients. Aust. Crit. Care 2013, 26, 49–54. [Google Scholar] [CrossRef]
- Herman, A.; Young, K.D.; Espitia, D.; Fu, N.; Farshidi, A. Impact of a Health Literacy Intervention on Pediatric Emergency Department Use. Pediatr. Emerg. Care 2009, 25, 434–438. [Google Scholar] [CrossRef] [Green Version]
- Hopmans, W.; Damman, O.C.; Timmermans, D.R.; Haasbeek, C.J.; Slotman, B.J.; Senan, S. Communicating cancer treatment information using the Web: Utilizing the patient’s perspective in website development. BMC Med. Inform. Decis Mak. 2014, 14, 116. [Google Scholar] [CrossRef] [Green Version]
- Hu, H.; Wu, F.-L.L.; Hu, F.-C.; Yang, H.-Y.; Lin, S.-W.; Shen, L.-J. Effectiveness of Education Programs about Oral Antibiotic Suspensions in Pediatric Outpatient Services. Pediatr. Neonatol. 2013, 54, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.-H.S.; Crowther, M.; Allen, R.S.; DeCoster, J.; Kim, G.; Azuero, C.; Ang, X.; Kvale, E. A Pilot Feasibility Intervention to Increase Advance Care Planning among African Americans in the Deep South. J. Palliat. Med. 2016, 19, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Jibaja-Weiss, M.L.; Volk, R.J.; Granchi, T.S.; Neff, N.E.; Robinson, E.K.; Spann, S.J.; Aoki, N.; Friedman, L.C.; Beck, J.R. Entertainment education for breast cancer surgery decisions: A randomized trial among patients with low health literacy. Patient Educ. Couns. 2011, 84, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Joseph, G.; Beattie, M.S.; Lee, R.; Braithwaite, D.; Wilcox, C.; Metrikin, M.; Lamvik, K.; Luce, J. Pre-counseling Education for Low Literacy Women at Risk of Hereditary Breast and Ovarian Cancer (HBOC): Patient Experiences Using the Cancer Risk Education Intervention Tool (CREdIT). J. Genet. Couns. 2010, 19, 447–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kheir, N.; Awaisu, A.; Radoui, A.; El Badawi, A.; Jean, L.; Dowse, R. Development and evaluation of pictograms on medication labels for patients with limited literacy skills in a culturally diverse multiethnic population. Res. Soc. Adm. Pharm. 2014, 10, 720–730. [Google Scholar] [CrossRef]
- Kripalani, S. Effect of a Pharmacist Intervention on Clinically Important Medication Errors After Hospital Discharge. Ann. Intern. Med. 2012, 157, 1. [Google Scholar] [CrossRef]
- Kripalani, S.; Robertson, R.; Love-Ghaffari, M.H.; Henderson, L.E.; Praska, J.; Strawder, A.; Katz, M.G.; Jacobson, T.A. Development of an illustrated medication schedule as a low-literacy patient education tool. Patient Educ. Couns. 2007, 66, 368–377. [Google Scholar] [CrossRef]
- Kuppermann, M.; Pena, S.; Bishop, J.T.; Nakagawa, S.; Gregorich, S.E.; Sit, A.; Vargas, J.; Caughey, A.B.; Sykes, S.; Pierce, L.; et al. Effect of Enhanced Information, Values Clarification, and Removal of Financial Barriers on Use of Prenatal Genetic Testing. Obstet. Gynecol. Surv. 2015, 70, 7–9. [Google Scholar] [CrossRef] [Green Version]
- Marcantoni, J.R.; Finney, K.; Lane, M.A. Using Health Literacy Guidelines to Improve Discharge Education and the Post-Hospital Transition. Am. J. Med. Qual. 2013, 29, 86. [Google Scholar] [CrossRef] [Green Version]
- Miller, M.J.; Abrams, M.A.; Earles, B.; Phillips, K.; McCleeary, E.M. Improving Patient-Provider Communication for Patients Having Surgery. J. Patient Saf. 2011, 7, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Mueller, S.K.; Giannelli, K.; Boxer, R.; Schnipper, J.L. Readability of patient discharge instructions with and without the use of electronically available disease-specific templates. J. Am. Med. Inform. Assoc. 2015, 22, 857–863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, M.D.; Young, J.; Hoke, S.; Tu, W.; Weiner, M.; Morrow, D.; Stroupe, K.T.; Wu, J.; Clark, D.; Smith, F.; et al. Pharmacist Intervention to Improve Medication Adherence in Heart Failure. Ann. Intern. Med. 2007, 146, 714. [Google Scholar] [CrossRef] [PubMed]
- Press, V.G.; Arora, V.M.; Shah, L.M.; Lewis, S.L.; Charbeneau, J.; Naureckas, E.T.; Krishnan, J.A. Teaching the Use of Respiratory Inhalers to Hospitalized Patients with Asthma or COPD: A Randomized Trial. J. Gen. Intern. Med. 2012, 27, 1317–1325. [Google Scholar] [CrossRef] [Green Version]
- Roberts, N.; Partridge, M. Evaluation of a paper and electronic pictorial COPD action plan. Chronic Respir. Dis. 2011, 8, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Sahm, L.J.; Wolf, M.S.; Curtis, L.M.; Behan, R.; Brennan, M.; Gallwey, H.; Mc Carthy, S. What’s in a label? An exploratory study of patient-centered drug instructions. Eur. J. Clin. Pharmacol. 2011, 68, 777–782. [Google Scholar] [CrossRef]
- Send, A.F.J.; Schwab, M.; Gauss, A.; Rudofsky, G.; Haefeli, W.E.; Seidling, H.M. Pilot study to assess the influence of an enhanced medication plan on patient knowledge at hospital discharge. Eur. J. Clin. Pharmacol. 2014, 70, 1243–1250. [Google Scholar] [CrossRef]
- Seth, N. A Health Literacy Strategy to Empower the Underserved Gynecological Surgery Patients to Reduce 7-Day Readmissions. ProQuest Dissertations Publishing, Wilmington University, New Castle, DE, USA, 2015. [Google Scholar]
- Sox, C.M.; Gribbons, W.M.; Loring, B.A.; Mandl, K.D.; Batista, R.; Porter, S.C. Patient-Centered Design of an Information Management Module for a Personally Controlled Health Record. J. Med. Internet Res. 2010, 12, e36. [Google Scholar] [CrossRef]
- Sudore, R.L.; Landefeld, C.S.; Barnes, D.E.; Lindquist, K.; Williams, B.A.; Brody, R.; Schillinger, D. An advance directive redesigned to meet the literacy level of most adults: A randomized trial. Patient Educ. Couns. 2007, 69, 165–195. [Google Scholar] [CrossRef] [Green Version]
- Van der Vaart, R.; Drossaert, C.H.; Taal, E.; Drossaers-Bakker, K.W.; Vonkeman, H.E.; van de Laar, M.A. Impact of patient-accessible electronic medical records in rheumatology: Use, satisfaction and effects on empowerment among patients. BMC Musculoskelet. Disord. 2014, 15, 102. [Google Scholar] [CrossRef] [Green Version]
- Williams, A.; Manias, E.; Liew, D.; Gock, H.; Gorelik, A. Working with CALD groups: Testing the feasibility of an intervention to improve medication selfmanagement in people with kidney disease, diabetes, and cardiovascular disease. Ren. Soc. Australas. J. 2012, 8, 62–69. [Google Scholar]
- Wolf, M.S.; Bailey, S.C.; Serper, M.; Smith, M.; Davis, T.C.; Russell, A.L.; Manzoor, B.S.; Lambert, B. Comparative Effectiveness of Patient-centered Strategies to Improve FDA Medication Guides. Med. Care 2014, 52, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Yin, H.S.; Dreyer, B.P.; Moreira, H.A.; van Schaick, L.; Rodriguez, L.; Boettger, S.; Mendelsohn, A.L. Liquid Medication Dosing Errors in Children: Role of Provider Counseling Strategies. Acad. Pediatr. 2014, 14, 262–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, H.S.; Dreyer, B.P.; van Schaick, L.; Foltin, G.L.; Dinglas, C.; Mendelsohn, A.L. Randomized Controlled Trial of a Pictogram-Based Intervention to Reduce Liquid Medication Dosing Errors and Improve Adherence Among Caregivers of Young Children. Arch. Pediatr. Adolesc. Med. 2008, 162, 814. [Google Scholar] [CrossRef]
- Zullig, L.L.; McCant, F.; Melnyk, S.D.; Danus, S.; Bosworth, H.B. A health literacy pilot intervention to improve medication adherence using Meducation® technology. Patient Educ. Couns. 2014, 95, 288–291. [Google Scholar] [CrossRef]
- Axelrod, D.A.; Kynard-Amerson, C.S.; Wojciechowski, D.; Jacobs, M.; Lentine, K.L.; Schnitzler, M.; Peipert, J.D.; Waterman, A.D. Cultural competency of a mobile, customized patient education tool for improving potential kidney transplant recipients’ knowledge and decision-making. Clin. Transplant. 2017, 31, e12944. [Google Scholar] [CrossRef]
- Davis, T.; Hancock, J.; Morris, J.; Branim, P.; Seth, A.; Rademaker, A.; Arnold, C. Impact of Health Literacy-directed Colonoscopy Bowel Preparation Instruction Sheet. Am. J. Health Behav. 2017, 41, 301–308. [Google Scholar] [CrossRef]
- Felicitas-Perkins, J.Q.; Palalay, M.P.; Cuaresma, C.; Ho, R.C.; Chen, M.S.; Dang, J., Jr.; Loui, W.S. A Pilot Study to Determine the Effect of an Educational DVD in Philippine Languages on Cancer Clinical Trial Participation among Filipinos in Hawai’i. Hawaii J. Med. Public Health 2017, 76, 171–177. [Google Scholar]
- Lindquist, L.A.; Ramirez-Zohfeld, V.; Sunkara, P.D.; Forcucci, C.; Campbell, D.S.; Mitzen, P.; Ciolino, J.D.; Kricke, G.; Seltzer, A.; Ramirez, A.V.; et al. Helping Seniors Plan for Posthospital Discharge Needs Before a Hospitalization Occurs: Results from the Randomized Control Trial of PlanYourLifespan.org. J. Hosp. Med. 2017, 12, 911–917. [Google Scholar] [CrossRef] [Green Version]
- Mcwilliams, A.; Reeves, K.; Shade, L.; Burton, E.; Tapp, H.; Courtlandt, C.; Gunter, A.; Dulin, M.F. Patient and Family Engagement in the Design of a Mobile Health Solution for Pediatric Asthma: Development and Feasibility Study. JMIR mHealth uHealth 2018, 6, e68. [Google Scholar] [CrossRef] [Green Version]
- Phillippi, J.C.; Doersam, J.K.; Neal, J.L.; Roumie, C.L. Electronic Informed Consent to Facilitate Recruitment of Pregnant Women into Research. J. Obstet. Gynecol. Neonatal Nurs. 2018, 47, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Press, V.G.; Kelly, C.A.; Kim, J.J.; White, S.R.; Meltzer, D.O.; Arora, V.M. Virtual Teach-To-Goal™ Adaptive Learning of Inhaler Technique for Inpatients with Asthma or COPD. J. Allergy Clin. Immunol. Pract. 2017, 5, 1032–1039. [Google Scholar] [CrossRef] [PubMed]
- Priegue, M.; Almuedo, A.; Rodríguez, I.; Rovira, O.; Soler, N.; Pardo, C.; Pola, N.; Mas, P.; Modamio, P.; Mariño, E.L. Pharmacist intervention in patients receiving treatment for Chagas disease: An emerging challenge for non-endemic countries. Infect. Dis. Health 2017, 22, 219–226. [Google Scholar] [CrossRef]
- Spellecy, R.; Tarima, S.; Denzen, E.; Moore, H.; Abhyankar, S.; Dawson, P.; Foley, A.; Gersten, I.; Horwitz, M.; Idossa, L.; et al. Easy-to-Read Informed Consent Form for Hematopoietic Cell Transplantation Clinical Trials: Results from the Blood and Marrow Transplant Clinical Trials Network 1205 Study. Biol. Blood Marrow Transplant. 2018, 24, 2145–2151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srisuk, N.; Cameron, J.; Ski, C.F.; Thompson, D.R. Randomized controlled trial of family-based education for patients with heart failure and their carers. J. Adv. Nurs. 2016, 73, 857–870. [Google Scholar] [CrossRef] [PubMed]
- Unaka, N.; Statile, A.; Jerardi, K.; Dahale, D.; Morris, J.; Liberio, B.; Jenkins, A.; Simpson, B.; Mullaney, R.; Kelley, J.; et al. Improving the readability of pediatric hospital medicine discharge instructions. J. Hosp. Med. 2017, 12, 551–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, H.S.; Gupta, R.S.; Mendelsohn, A.L.; Dreyer, B.; Schaick, L.V.; Brown, C.R.; Encalada, K.; Sanchez, D.C.; Warren, C.M.; Tomopoulos, S. Use of a low-literacy written action plan to improve parent understanding of pediatric asthma management: A randomized controlled study. J. Asthma 2017, 54, 919–929. [Google Scholar] [CrossRef]
- Hicks, B.L.; Brittan, M.S.; Knapp-Clevenger, R. Group Style Central Venous Catheter Education Using the GLAD Model. J. Pediatr. Nurs. 2019, 45, 67–72. [Google Scholar] [CrossRef]
- Khan, A.; Spector, N.D.; Baird, J.D.; Ashland, M.; Starmer, A.J.; Rosenbluth, G.; Garcia, B.M.; Litterer, K.P.; Rogers, J.E.; Dalal, A.K.; et al. Patient safety after implementation of a coproduced family centered communication programme: Multicenter before and after intervention study. BMJ 2018, 363, k4764. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.S.; Nápoles, A.; Mutha, S.; Pérez-Stable, E.J.; Gregorich, S.E.; Livaudais-Toman, J.; Karliner, L.S. Hospital discharge preparedness for patients with limited English proficiency: A mixed methods study of bedside interpreter-phones. Patient Educ. Couns. 2018, 101, 25–32. [Google Scholar] [CrossRef]
- Mcevoy, A.; Sauder, M.B.; Mcdonald, K.; Suter, P.; Pouliot, A.; Zemek, R.; Kanigsberg, N.; Vaillancourt, R.; Ramien, M.L. Derivation, Evaluation, and Validation of Illustrations of Key Counselling Points for a Pediatric Eczema Action Plan. J. Cutan. Med. Surg. 2017, 22, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Merchant, R.C.; Liu, T.; Clark, M.A.; Carey, M.P. Facilitating HIV/AIDS and HIV testing literacy for emergency department patients: A randomized, controlled, trial. BMC Emerg. Med. 2018, 18, 21. [Google Scholar] [CrossRef] [PubMed]
- Plate, J.F.; Ryan, S.P.; Bergen, M.A.; Hong, C.S.; Attarian, D.E.; Seyler, T.M. Utilization of an Electronic Patient Portal Following Total Joint Arthroplasty Does Not Decrease Readmissions. J. Arthroplast. 2019, 34, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Scalia, P.; Durand, M.-A.; Faber, M.; Kremer, J.A.; Song, J.; Elwyn, G. User-testing an interactive option grid decision aid for prostate cancer screening: Lessons to improve usability. BMJ Open 2019, 9, e026748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staynova, R.A.; Gueorguiev, S.R.; Petkova-Gueorguieva, E.S.; Vasileva, E.V.; Stoimenova, A.H.; Yanatchkova, V.E.; Madzharov, V.G. Written Health Education Materials for Women with Gestational Diabetes Mellitus—Evaluation of Usefulness and Patients’ Satisfaction. Folia Med. 2019, 61, 127–133. [Google Scholar] [CrossRef]
- Wallace, A.S.; Pierce, N.L.; Davisson, E.; Manges, K.; Tripp-Reimer, T. Social resource assessment: Application of a novel communication tool during hospital discharge. Patient Educ. Couns. 2019, 102, 542–549. [Google Scholar] [CrossRef]
- Alberti, T.L.; Nannini, A. Patient comprehension of discharge instructions from the emergency department: A literature review. J. Am. Acad. Nurse Pract. 2012, 25, 186–194. [Google Scholar] [CrossRef]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low Health Literacy and Health Outcomes: An Updated Systematic Review. Ann. Intern. Med. 2011, 155, 97. [Google Scholar] [CrossRef]
- Chan, H.K.; Hassali, M.A.; Lim, C.J.; Saleem, F.; Tan, W.L. Using pictograms to assist caregivers in liquid medication administration: A systematic review. J. Clin. Pharm. Ther. 2015, 40, 266–272. [Google Scholar] [CrossRef]
- Jacobs, R.J.; Lou, J.Q.; Ownby, R.L.; Caballero, J. A systematic review of eHealth interventions to improve health literacy. Health Inform. J. 2014, 22, 81–98. [Google Scholar] [CrossRef]
- Santo, A.; Laizner, A.M.; Shohet, L. Exploring the value of audiotapes for health literacy: A systematic review. Patient Educ. Couns. 2005, 58, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, S.L.; Halpern, D.J.; Viera, A.J.; Berkman, N.D.; Donahue, K.E.; Crotty, K. Interventions for Individuals with Low Health Literacy: A Systematic Review. J. Health Commun. 2011, 16 (Suppl. S3), 30–54. [Google Scholar] [CrossRef] [PubMed]
- Wilson, E.A.; Makoul, G.; Bojarski, E.A.; Bailey, S.C.; Waite, K.R.; Rapp, D.N.; Baker, D.W.; Wolf, M.S. Comparative analysis of print and multimedia health materials: A review of the literature. Patient Educ. Couns. 2012, 89, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Curran, J.A.; Gallant, A.J.; Zemek, R.; Newton, A.S.; Jabbour, M.; Chorney, J.; Murphy, A.; Hartling, L.; Macwilliams, K.; Plint, A.; et al. Discharge communication practices in pediatric emergency care: A systematic review and narrative synthesis. Syst. Rev. 2019, 8, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, J.P.; Cheng, K.K.F.; Siah, R.C. A systematic review and meta-analysis on the effectiveness of education on medication adherence for patients with hypertension, hyperlipidaemia and diabetes. J. Adv. Nurs. 2019, 75. [Google Scholar] [CrossRef] [PubMed]
- Chan, B.; Goldman, L.E.; Sarkar, U.; Schneidermann, M.; Kessell, E.; Guzman, D.; Critchfield, J.; Kushel, M. The Effect of a Care Transition Intervention on the Patient Experience of Older Multi-Lingual Adults in the Safety Net: Results of a Randomized Controlled Trial. J. Gen. Intern. Med. 2015, 30, 1788–1794. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, B.; Foster, J.; Boyd, R.; Atlantis, E. Implementation challenges in delivering team-based care (“TEAMcare”) for patients with chronic obstructive pulmonary disease in a public hospital setting: A mixed methods approach. BMC Health Serv. Res. 2016, 16, 347. [Google Scholar] [CrossRef] [Green Version]
- Daley, C.M. A Hybrid Transitional Care Program. Crit. Pathw. Cardiol. 2010, 9, 231–234. [Google Scholar] [CrossRef]
- Jack, B.W. A Reengineered Hospital Discharge Program to Decrease Rehospitalization. Ann. Intern. Med. 2009, 150, 178. [Google Scholar] [CrossRef]
- Johnson, R.W.; Zhao, Y.; Newby, L.K.; Granger, C.B.; Granger, B.B. Reasons for Noncompletion of Advance Directives in a Cardiac Intensive Care Unit. Am. J. Crit. Care 2012, 21, 311–320. [Google Scholar] [CrossRef]
- Masterson Creber, R.M.; Patey, M.; Lee, C.S.; Riegel, B. Motivational Interviewing to Improve Self-care for Patients with Chronic Heart Failure: MITI-HF Randomized Controlled Trial. J. Card Fail. 2015, 21, S78. [Google Scholar] [CrossRef] [Green Version]
- Micklethwaite, A.; Brownson, C.A.; O’Toole, M.L.; Kilpatrick, K.E. The Business Case for a Diabetes Self-Management Intervention in a Community General Hospital. Popul. Health Manag. 2012, 15, 230–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oancea, C.; Fira-Mladinescu, O.; Timar, B.; Tudorache, V. Impact of medical education program on COPD patients: A cohort prospective study. Wien. Klin Wochenschr. 2015, 127, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, M.S.; Catallozzi, M.; Larson, E.; Rodriguez, C.; Subramony, A.; Martinez, R.A.; Martinez, E.; Barrett, A.; Meyer, D. Effect of a URI-related educational intervention in early head start on ED visits. Pediatrics 2014, 133, e1233–e1240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, M.S.; Seligman, H.; Davis, T.C.; Fleming, D.A.; Curtis, L.M.; Pandit, A.U.; Parker, R.M.; Schillinger, D.; Dewalt, D.A. Clinic-Based Versus Outsourced Implementation of a Diabetes Health Literacy Intervention. J. Gen. Intern. Med. 2013, 29, 59–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, J. Engage2: Implementing a Health Literacy Protocol for Patient Assessment and Engagement. J. Consum. Health Internet 2017, 21, 338–349. [Google Scholar] [CrossRef]
- Dingemans, A.J.; Reck, C.A.; Vilanova-Sanchez, A.; Gonzalez, D.O.; Gasior, A.C.; Weaver, L.J.; Gagnon, R.; Hoover, E.; Sraha, G.; Levitt, M.A.; et al. Does clinic visit education within a multidisciplinary center improve health literacy scores in caregivers of children with complex colorectal conditions? J. Pediatr. Surg. 2017, 52, 1997–2000. [Google Scholar] [CrossRef]
- Lee, J.S.; Pérez-Stable, E.J.; Gregorich, S.E.; Crawford, M.H.; Green, A.; Livaudais-Toman, J.; Karliner, L.S. Increased Access to Professional Interpreters in the Hospital Improves Informed Consent for Patients with Limited English Proficiency. J. Gen. Intern. Med. 2017, 32, 863–870. [Google Scholar] [CrossRef] [Green Version]
- Navaneethan, S.D.; Jolly, S.E.; Schold, J.D.; Arrigain, S.; Nakhoul, G.; Konig, V.; Hyland, J.; Burrucker, Y.K.; Dann, P.D.; Tucky, B.H.; et al. Pragmatic Randomized, Controlled Trial of Patient Navigators and Enhanced Personal Health Records in CKD. Clin. J. Am. Soc. Nephrol. 2017, 12, 1418–1427. [Google Scholar] [CrossRef] [Green Version]
- Kripalani, S.; Chen, G.; Ciampa, P.; Theobald, C.; Cao, A.; Mcbride, M.; Dittus, R.S.; Speroff, T. A transition care coordinator model reduces hospital readmissions and costs. Contemp. Clin. Trials 2019, 81, 55–61. [Google Scholar] [CrossRef]
- Rayan-Gharra, N.; Balicer, R.D.; Tadmor, B.; Shadmi, E. Association between cultural factors and readmissions: The mediating effect of hospital discharge practices and care-transition preparedness. BMJ Qual. Saf. 2019, 28. [Google Scholar] [CrossRef] [PubMed]
- Grice, G.R.; Tiemeier, A.; Hurd, P.; Berry, T.M.; Voorhees, M.; Prosser, T.R.; Sailors, J.; Gattas, N.M.; Duncan, W. Student Use of Health Literacy Tools to Improve Patient Understanding and Medication Adherence. Consult Pharm. 2014, 29, 240–253. [Google Scholar] [CrossRef] [PubMed]
- Kornburger, C.; Gibson, C.; Sadowski, S.; Maletta, K.; Klingbeil, C. Using “Teach-Back” to Promote a Safe Transition From Hospital to Home: An Evidence-Based Approach to Improving the Discharge Process. J. Pediatr. Nurs. 2013, 28, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Krajic, K.; Straßmayr, C.; Trummer, U.; Novak-Zezula, S.; Pelikan, J. Improving ethnocultural competence of hospital staff by training: Experiences from the European ’Migrant-friendly Hospitals’ project. Div. Health Soc. Care 2005, 2, 279–290. [Google Scholar]
- Kripalani, S.; Jacobson, K.L.; Brown, S.; Manning, K.; Rask, K.J.; Jacobson, T.A. Development and Implementation of a Health Literacy Training Program for Medical Residents. Med. Educ. Online 2006, 11, 4612. [Google Scholar] [CrossRef]
- Lori, J.R.; Munro, M.L.; Chuey, M.R. Use of a facilitated discussion model for antenatal care to improve communication. Int. J. Nurs. Stud. 2016, 54, 84–94. [Google Scholar] [CrossRef] [Green Version]
- Shipman, J.P.; Kurtz-Rossi, S.; Funk, C.J. The health information literacy research project. J. Med. Libr. Assoc. 2009, 97, 293–301. [Google Scholar] [CrossRef]
- Stikes, R.; Arterberry, K.; Logsdon, M.C. A Nurse Leadership Project to Improve Health Literacy on a Maternal-Infant Unit. J. Obstet. Gynecol. Neonatal Nurs. 2015, 44, 665–676. [Google Scholar] [CrossRef]
- Trummer, U.F.; Mueller, U.O.; Nowak, P.; Stidl, T.; Pelikan, J.M. Does physician–patient communication that aims at empowering patients improve clinical outcome? Patient Educ. Couns. 2006, 61, 299–306. [Google Scholar] [CrossRef]
- Grabeel, K.L.; Beeler, C.J. Taking the Pulse of the University of Tennessee Medical Center’s Health Literacy Knowledge. Med. Ref. Serv. Q. 2018, 37, 89–96. [Google Scholar] [CrossRef]
- Klingbeil, C.; Gibson, C. The Teach Back Project: A System-wide Evidence Based Practice Implementation. J. Pediatr. Nurs. 2018, 42, 81–85. [Google Scholar] [CrossRef]
- Roberts, N.J.; Evans, G.; Blenkhorn, P.; Partridge, M.R. Development of an electronic pictorial asthma action plan and its use in primary care. Patient Educ. Couns. 2010, 80, 141–146. [Google Scholar] [CrossRef]
- Beauchamp, A.; Batterham, R.W.; Dodson, S.; Astbury, B.; Elsworth, G.R.; Mcphee, C.; Jacobson, J.; Buchbinder, R.; Osborne, R.H. Systematic development and implementation of interventions to OPtimise Health Literacy and Access (Ophelia). BMC Public Health 2017, 17, 230. [Google Scholar] [CrossRef] [Green Version]
- Gazmararian, J.A.; Beditz, K.; Pisano, S.; Carreón, R. The Development of a Health Literacy Assessment Tool for Health Plans. J. Health Commun. 2010, 15 (Suppl. S2), 93–101. [Google Scholar] [CrossRef] [PubMed]
- Innis, J.; Barnsley, J.; Berta, W.; Daniel, I. Measuring health literate discharge practices. Int. J. Health Care Qual. Assur. 2017, 30, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Weidmer, B.A.; Brach, C.; Slaughter, M.E.; Hays, R.D. Development of Items to Assess Patients’ Health Literacy Experiences at Hospitals for the Consumer Assessment of Healthcare Providers and Systems (CAHPS) Hospital Survey. Med. Care 2012, 50, S12–S21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oelschlegel, S.; Grabeel, K.L.; Tester, E.; Heidel, R.E.; Russomanno, J. Librarians Promoting Changes in the Health Care Delivery System through Systematic Assessment. Med. Ref. Serv. Q. 2018, 37, 142–152. [Google Scholar] [CrossRef]
- Palumbo, R.; Annarumma, C.; Musella, M. Exploring the meaningfulness of healthcare organizations: A multiple case study. Int. J. Public Sect. Manag. 2017, 30, 503–518. [Google Scholar] [CrossRef]
- Hayran, O.; Özer, O. Organizational health literacy as a determinant of patient satisfaction. Public Health 2018, 163, 20–26. [Google Scholar] [CrossRef]
- Jessup, R.L.; Osborne, R.H.; Buchbinder, R.; Beauchamp, A. Using co-design to develop interventions to address health literacy needs in a hospitalised population. BMC Health Serv. Res. 2018, 18, 989. [Google Scholar] [CrossRef] [Green Version]
- Innis, J.; Barnsley, J.; Berta, W.; Daniel, I. Development of Indicators to Measure Health Literate Discharge Practices. J. Nurs. Care Qual. 2017, 32, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Seligman, H.K.; Wallace, A.S.; Dewalt, D.A.; Schillinger, D.; Arnold, C.L.; Shilliday, B.B.; Delgadillo, A.; Bengal, N.; Davis, T.C. Facilitating Behavior Change with Low-literacy Patient Education Materials. Am. J. Health Behav. 2007, 31, 69–78. [Google Scholar] [CrossRef] [Green Version]
- Chin, J.; Moeller, D.D.; Johnson, J.; Duwe, E.A.G.; Graumlich, J.F.; Murray, M.D.; Morrow, D.G. A Multi-faceted Approach to Promote Comprehension of Online Health Information among Older Adults. Gerontologist 2017, 58, 686–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naccarella, L.; Biuso, C.; Jennings, A.; Patsamanis, H. Improving access to important recovery information for heart patients with low health literacy: Reflections on practice-based initiatives. Aust. Health Rev. 2019, 43, 323–327. [Google Scholar] [CrossRef]
- Thomacos, N.; Zazryn, T. Enliven Organisational Health Literacy Self-Assessment Audit Resource; Enliven & School of Primary Health Care, Monash University: Melbourne, Australia, 2013. [Google Scholar]
- Pelikan, J.; Dietscher, C. [Why should and how can hospitals improve their organizational health literacy?] Warum Sollten Und Wie Konn Krankenhauser Ihre Organ Gesundheitskompetenz Verbessern? Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2015, 58, 989–995. [Google Scholar] [CrossRef]
- Rudd, R. Navigating hospitals: Literacy barriers. Lit. Harvest 2004, Fall, 19–24. [Google Scholar]
- Howard, D.H.; Gazmararian, J.; Parker, R.M. The impact of low health literacy on the medical costs of Medicare managed care enrollees. Am. J. Med. 2005, 118, 371–377. [Google Scholar] [CrossRef]
- Haun, J.N.; Patel, N.R.; French, D.D.; Campbell, R.R.; Bradham, D.D.; Lapcevic, W.A. Association between health literacy and medical care costs in an integrated healthcare system: A regional population based study. BMC Health Serv. Res. 2015, 15, 249. [Google Scholar] [CrossRef] [Green Version]
- Adsul, P.; Wray, R.; Gautam, K.; Jupka, K.; Weaver, N.; Wilson, K. Becoming a health literate organization: Formative research results from healthcare organizations providing care for undeserved communities. Health Serv. Manag. Res. 2017, 30, 188–196. [Google Scholar] [CrossRef]
- Brach, C. The Journey to Become a Health Literate Organization: A Snapshot of Health System Improvement. Stud. Health Technol. Inform. 2017, 240, 203–237. [Google Scholar]



{kind=link}
{kind=link}
| An HLHO |
|---|
|
| Strings | Database |
|---|---|
| ((“health literacy” AND implementation) OR (“Health Literacy/nursing”[Mesh] OR “Health Literacy/organization and administration”[Mesh] OR “Health Literacy/utilization”[Mesh]) OR “health literate” OR (“health literacy” AND (organizat * OR organisat *)) AND (“hospitals”[MeSH Terms] OR “hospitals”[All Fields] OR “hospital”[All Fields] OR hospital * OR “health facility *” OR “Health Facilities”[Mesh]) | Pubmed |
| ((“health literacy” AND implementation) OR (“Health Literacy” AND nursing) OR ((“Health Literacy” OR “health literate”) AND (organizat * OR administrat * OR utilizat *))) AND (hospital * OR “health facility *”) | WoS, Cinahl, Scopus, Psycinfo |
| “health literacy” OR “health literate” | Sociological Abstract |
| Intervention | Subcategories | Code | Ref. | No. of Studies |
|---|---|---|---|---|
| Support for patient | Environmental | 1a | [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83] | 66 |
| Staff | 1b | [19,21,24,28,29,30,34,40,41,49,51,61,63,66,67,68,75,80,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99] | 35 | |
| Support for staff | Training | 2a | [67,80,100,101,102,103,104,105,106,107,108,109] | 12 |
| Environmental | 2b | [50,64,67,68,76,110] | 6 | |
| Support for governance | Developing/usig tools/instruments for assessing organizational health literacy | 3a | [11,108,111,112,113,114,115,116,117,118] | 10 |
| Actions for quality improvements | 3b | [50,111,116,119,120,121,122] | 7 |
| Target | Subcategories | Code | Ref. | No. of Studies |
|---|---|---|---|---|
| Patient | Knowledge/skills/behaviour | 1a | [18,22,23,24,25,26,27,29,30,31,32,33,35,36,37,38,40,41,42,43,44,46,47,49,50,51,52,53,54,55,57,59,60,61,63,65,66,68,70,75,76,77,78,79,80,81,82,83,87,88,93,95,96,121,122] | 57 |
| Satisfaction/acceptability/helpfulness/ | 1b | [20,21,22,28,30,31,47,48,54,56,59,63,67,73,79,81,84,85,94,106,107,117,120] | 23 | |
| Patient health outcomes | 1c | [19,27,34,37,41,45,63,66,71,76,80,86,87,89,90,91,92,93,97,98,99] | 22 | |
| Staff | Knowledge/skills/behaviour | 2a | [38,64,67,68,101,102,103,105,108,109,110,122] | 12 |
| Staff perception of satisfaction/helpfulness | 2b | [23,100,101,102,103,104] | 6 | |
| System | Assessment tools scores (organisation) | 3a | [11,84,94,116,117,121] | 11 |
| Quality improvements perceived/gained | 3b | [108,111,116,118,119,122] | 6 | |
| Validation/feasibility/usability/ | 3c | [39,58,69,72,114,117] | 8 | |
| Costs | 3d | [40,80,98] | 3 |
| N | Description | No. of Studies | Ref. |
|---|---|---|---|
| 1 | Leadership | 7 | [65,105,106,111,114,115,116] |
| 2 | Planning | 19 | [11,69,72,73,88,94,106,107,110,111,112,113,114,115,116,117,119,121,122] |
| 3 | Workforce | 13 | [67,80,94,100,101,102,103,104,105,106,107,109,110] |
| 4 | Population | 10 | [11,28,38,42,50,56,58,59,67,118] |
| 5 | Meets the needs of the population | 0–106 | * |
| 6 | Communication | 25 | [19,36,38,41,49,51,61,63,67,78,79,80,82,89,90,93,94,96,99,100,101,102,104,107,109] |
| 7 | Navigation | 36 | [19,20,21,24,28,30,31,32,34,36,38,40,46,48,53,54,56,57,58,59,60,63,68,72,82,84,86,87,89,90,97,98,99,112,121,122] |
| 8 | Contents easy to understand | 67 | [18,19,20,22,23,24,25,26,27,28,29,30,31,32,33,35,36,37,38,39,40,41,42,43,44,45,47,49,50,51,52,53,54,55,56,57,58,60,61,62,63,64,65,66,67,69,70,72,73,74,75,76,77,78,79,80,81,82,83,90,93,110,112,118,120,121,122] |
| 9 | High-risk situations | 53 | [18,19,20,21,23,25,26,27,28,32,34,35,37,38,39,40,41,43,44,45,49,52,54,59,61,62,63,64,65,66,67,68,74,75,76,80,82,83,84,85,86,87,88,90,91,92,93,95,96,98,99,113,119] |
| 10 | Payment transparency | 0 | / |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zanobini, P.; Lorini, C.; Baldasseroni, A.; Dellisanti, C.; Bonaccorsi, G. A Scoping Review on How to Make Hospitals Health Literate Healthcare Organizations. Int. J. Environ. Res. Public Health 2020, 17, 1036. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17031036
Zanobini P, Lorini C, Baldasseroni A, Dellisanti C, Bonaccorsi G. A Scoping Review on How to Make Hospitals Health Literate Healthcare Organizations. International Journal of Environmental Research and Public Health. 2020; 17(3):1036. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17031036
Chicago/Turabian StyleZanobini, Patrizio, Chiara Lorini, Alberto Baldasseroni, Claudia Dellisanti, and Guglielmo Bonaccorsi. 2020. "A Scoping Review on How to Make Hospitals Health Literate Healthcare Organizations" International Journal of Environmental Research and Public Health 17, no. 3: 1036. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17031036