Children Exposed to Intimate Partner Violence: Association Among Battered Mothers’ Parenting Competences and Children’s Behavior


Abstract
:1. Introduction
1.1. Violence Experienced by Children in the Context of IPV
1.2. The Present Study
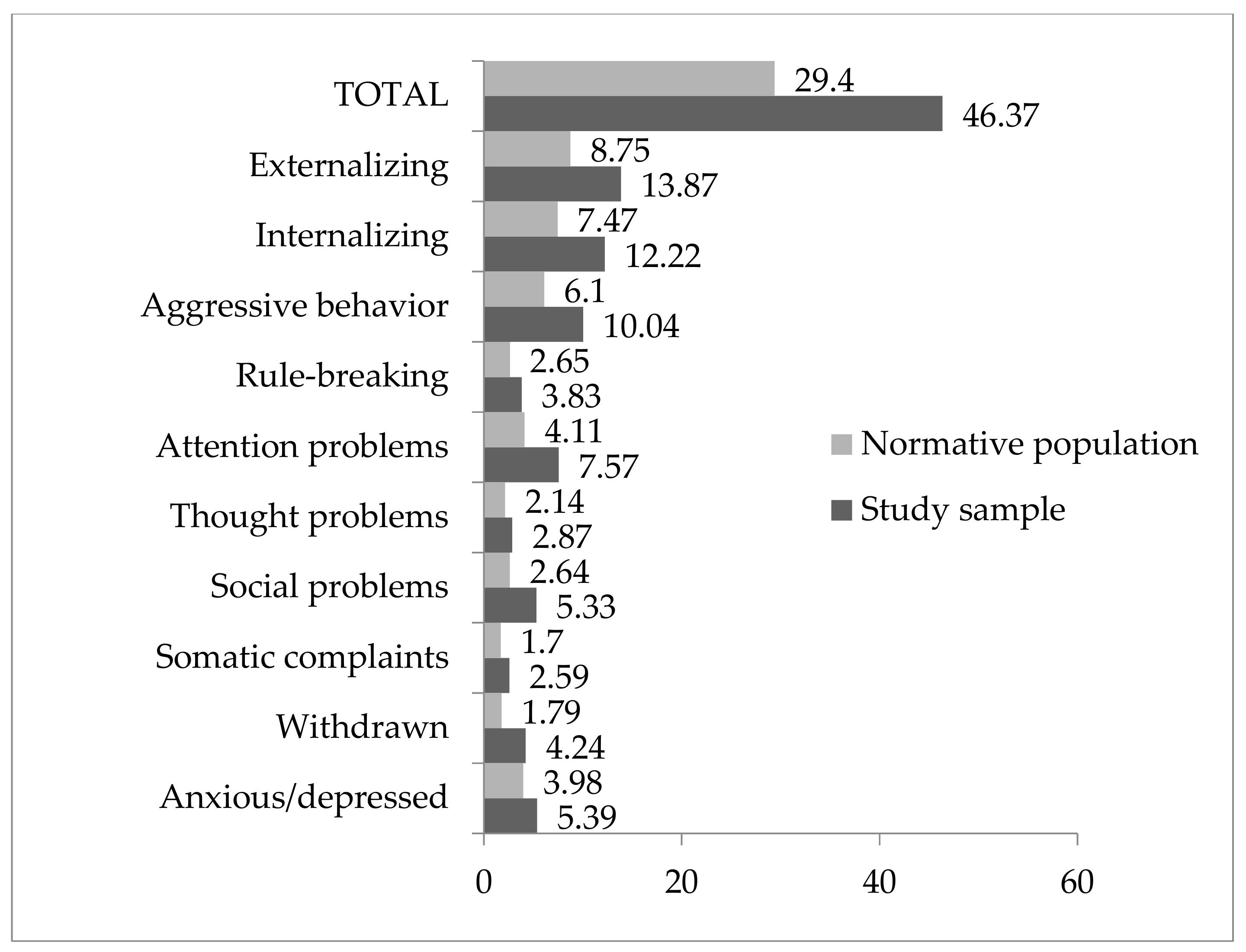
- To explore the existence of differences between children exposed to IPV and their peers in the general population in terms of behavioral problems;
- To describe the parenting competences of mother–child interactions in the context of social care for women who are victims of gender-based violence;
- To explore whether there is an association between behavioral problems in children and parenting competences in mother–child interactions in the shelters.
- Children who have experienced gender-based violence against their mothers have a higher rate of behavioral problems;
- Women who are victims of gender-based violence may have reduced parenting competences;
- There is an association between the quality of parenting competences demonstrated by mothers while living with their children in shelters and the rate of child behavioral problems.
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Demographic Data Collection Sheet
2.2.2. Child Behavior Checklist (CBCL)
2.2.3. Scale of Competent Parenting Behavior
“The group of capabilities that allows parents to address the work of being parents in a flexible and adaptable way, according to the evolutionary and educational needs of their children, by standards considered acceptable to society, and taking advantage of all opportunities and support provided by systems influencing the family in order develop these skills.”(p. 115)
2.3. Procedure
2.4. Statistical Analyses
2.4.1. Child Behavior Check List (CBCL)
2.4.2. Scale of Competent Parenting Behavior
3. Results
3.1. Sociodemographic Characteristics of the Children and Their Mothers
3.2. Child Behavioral Problems
3.3. Competent Parenting Behavior
3.4. Association between Behavioral Problems in Children (CBCL) and Mothers’ Parenting Competences
4. Discussion
5. Conclusions and Proposals for Social Intervention
Limitations of the Study
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- European Union Agency for Fundamental Rights. Violence against Women: An EU-Wide Survey. Main Results Report; Publications Office of the European Union: Brussels, Belgium, 2014. [Google Scholar]
- Överlien, C.; Hyden, M. Children’s actions when experiencing domestic violence. Childhood 2009, 16, 479–496. [Google Scholar] [CrossRef] [Green Version]
- Holden, G.W.; Ritchie, K.L. Linking extreme marital discord, child rearing, and child behavior problems: Evidence from battered women. Child Dev. 2003, 62, 311–327. [Google Scholar] [CrossRef]
- Devaney, J. Research Review: The Impact of Domestic Violence on Children. Ir. Probat. J. 2015, 12, 79–94. [Google Scholar]
- Bancroft, L.R.; Silverman, J.G. The Batterer as Parent: Addressing the Impact of Domestic Violence on Family Dynamics; Sage: Thousand Oaks, CA, USA, 2002; Available online: http://www.lundybancroft.com/pages/b_as_parent.html (accessed on 7 February 2020).
- Beeble, M.L.; Bybee, D.I.; Sullivan, C.M. Abusive men’s use of children to control their partners and ex-partners. Eur. Psychol. 2007, 12, 54–61. [Google Scholar] [CrossRef]
- Unicef. The Body Shop International and the Secretariat for the United Nations Secretary-General’s Study on Violence against Children. Behind Closed Doors. The Impact of Domestic Violence on Children. Littlehampton, 2006. Available online: http://www.unicef.org/protection/files/BehindClosedDoors.pdf (accessed on 13 February 2018).
- Ministerio de Sanidad, Servicios Sociales e Igualdad. Macroencuesta de Violencia de Género 2015. Avance de resultados. Available online: http://www.msssi.gob.es/ssi/violenciaGenero/laDelegacionInforma/pdfs/DGVG_Informa_Macroencuesta.pdf (accessed on 25 May 2018).
- Sindic de Greuges de la Comunidad Valenciana. Informe del Síndic de Greuges Sobre La atención y Protección a Las Mujeres Víctimas de Violencia de Género en la Comunitat Valenciana; Sindic de greuges: Alicante, Spain, 2017. [Google Scholar]
- Kitzmann, K.M.; Gaylord, N.K.; Holt, A.R.; Kenny, E.D. Child witnesses to domestic violence: A meta-analytic review. J. Consult. Clin. Psychol. 2003, 71, 339–352. [Google Scholar] [CrossRef]
- Wolfe, D.A.; Crooks, C.V.; Lee, V.; McIntyre-Smith, A.; Jaffe, P.G. The effects of children’s exposure to domestic violence: A meta-analysis and critique. Clin. Child. Fam. Psychol. Rev. 2003, 6, 171–187. [Google Scholar] [CrossRef]
- Evans, S.E.; Davies, C.; DiLillo, D. Exposure to domestic violence: A meta-analysis of child and adolescent outcomes. Aggress. Violent. Behav. 2008, 13, 131–140. [Google Scholar] [CrossRef] [Green Version]
- Holt, S.; Buckley, H.; Whelan, S. The impact of exposure to domestic violence on children and young people: A review of the literature. Child. Abus. Negl. 2008, 32, 797–810. [Google Scholar] [CrossRef] [PubMed]
- Lourenço, L.M.; Baptista, M.N.; Senra, L.X.; Adriana, A.A.; Basılio, C.; Bhona, F.M.D.C. Consequences of exposure to domestic violence for children: A systematic review of the literature. Paideıa 2013, 23, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Jouriles, E.N.; Rosenfield, D.; McDonald, R.; Mueller, V. Child involvement in interparental conflict and child adjustment problems: A longitudinal study of violent families. J. Abnorm. Child. Psychol. 2014, 42, 693–704. [Google Scholar] [CrossRef] [Green Version]
- Pingley, T. The Impact of Witnessing Domestic Violence on Children: A Systematic Review. Master Soc. Work Clin. Res. Pap. 2017. Available online: https://sophia.stkate.edu/msw_papers/776 (accessed on 7 February 2020).
- McTavish, J.R.; MacGregor, J.C.D.; Wathen, C.N.; MacMillan, H.L. Children exposure to intimate partner violence: An overview. Int. Rev. Psychiatry 2016, 28, 504–518. [Google Scholar] [CrossRef] [PubMed]
- Stanley, N. Children Experiencing Domestic Violence: A Research Review; Research in Practice: Dartington, UK, 2011. [Google Scholar]
- Emery, C.R. Controlling for selection effects in the relationship between child behavior problems and exposure to intimate partner violence. J. Interpers. Violence 2011, 26, 1541–1558. [Google Scholar] [CrossRef] [PubMed]
- Vu, N.L.; Jouriles, E.N.; McDonald, R.; Rosenfield, D. Children’s exposure to intimate partner violence: A meta-analysis of longitudinal associations with child adjustment problems. Clin. Psychol. Rev. 2016, 46, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, K.J.; Baradaran, L.P.; Abbot, C.B.; Lamb, M.E.; Guterman, E. Type of violence, age, and gender differences in the effects of family violence on children’s behavior problems: A mega-analysis. Dev. Rev. 2006, 26, 89–112. [Google Scholar] [CrossRef]
- Mohand, L.; Carracedo, S.; Herrera, L. Impacto de la violencia de género en el estado de salud física y psicoemocional de los hijos. Dedica. Rev. De Educ. E Hum. 2014, 6, 73–84. [Google Scholar]
- Alcántara, M.V.; López-Soler, C.; Castro, M.; López, J.J. Alteraciones psicológicas en menores expuestos a violencia de género: Prevalencia y diferencias de género y edad. An. De Psicol. 2013, 29, 741–747. [Google Scholar] [CrossRef] [Green Version]
- Bayarri, E.; Ezpeleta, L.; Granero, R. Exposure to Intimate Partner Violence, Psychopathology, and Functional Impairment in Children and Adolescents: Moderator Effect of Sex and Age. J. Fam. Violence 2011, 26, 535–543. [Google Scholar] [CrossRef]
- Graham-Bermann, S.A.; Gruber, G.; Howell, K.H.; Girz, L. Factors discriminating among profiles of resilience and psychopathology in children exposed to intimate partner violence (IPV). Child. Abus. Negl. 2009, 33, 648–660. [Google Scholar] [CrossRef]
- Huth-Bocks, A.; Levendosky, A.; Semel, M. The direct and indirect effects of domestic violence on young children’s intellectual functioning. J. Fam. Violence 2001, 16, 269–290. [Google Scholar] [CrossRef]
- Rosser, A.; Suriá, R.; Villegas, E. La exposición a violencia de género y su repercusión en la adaptación escolar de los menores. Bordón 2013, 67, 117–129. [Google Scholar]
- Suzuki, S.L.; Geffner, R.; Bucky, S. The Experiences of Adults Exposed to Intimate Partner Violence as Children: An Exploratory Qualitative Study of Resilience and Protective Factors. J. Emot. Abus. 2008, 8. [Google Scholar] [CrossRef]
- DeBoard-Lucas, R.L.; Fosco, G.M.; Raynor, S.R.; Grych, J.H. Interparental conflict in context: Exploring relations between parenting processes and children’s conflict appraisals. Clin. Child. Fam. Psychol. Rev. 2010, 39, 163–175. [Google Scholar] [CrossRef] [PubMed]
- López-Soler, C.; Alcántara-López, M.; Castro, M.; Sánchez-Meca, J.; Fernández, V. The association between maternal exposure to intimate partner violence and emotional and behavioral problems in Spanish children and adolescents. J. Fam. Violence 2017, 2, 135–144. [Google Scholar] [CrossRef]
- González, F.; Gimeno, A. Violencia de género. Perfil de mujeres con ayuda social. Interv. Psicosoc. 2009, 18, 165–175. [Google Scholar] [CrossRef]
- Ramos, E.; de la Peña, E.M.; Luzón, J.M.; Recio, P. Andalucía Detecta-Andalucía Interviene. Impacto de la Exposición a Violencia de Género en Menores. Resultados y Recomendaciones; Instituto andaluz de la mujer: Sevilla, Spain, 2011. [Google Scholar]
- Huth-Bocks, A.C.; Hughes, H.M. Parenting stress, parenting behavior, and children’s adjustment in families experiencing intimate partner violence. J. Fam. Violence 2008, 23, 243–251. [Google Scholar] [CrossRef]
- Matud, M.P. Impacto de la violencia doméstica en la salud de la mujer maltratada. Psicothema 2004, 16, 397–401. [Google Scholar]
- Levendosky, A.A.; Graham-Bermann, S.A. Parenting in battered women: The effects of domestic violence on women and their children. J. Fam. Violence 2001, 16, 171–192. [Google Scholar] [CrossRef]
- Timmer, S.G.; Thompson, D.; Culver, M.; Urquiza, A.J.; Altenhofen, S. Mothers’ physical abusiveness in a context of violence: Effects on the mother-child relationship. Dev. Psychopathol. 2012, 24, 79–92. [Google Scholar] [CrossRef]
- Letourneau, N.L.; Fedick, C.B.; Willms, J.D. Mothering and domestic violence: A longitudinal analysis. J. Fam. Violence 2007, 22, 649–659. [Google Scholar] [CrossRef]
- Gustafsson, H.C.; Cox, M.J.; Blair, C. Maternal parenting as a mediator of the relationship between intimate partner violence and effortful control. J. Fam. Psychol. 2012, 26, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorence, B.; Hidalgo, V.; Pérez-Padilla, J.; Menéndez, S. The Role of Parenting Styles on Behavior Problem Profiles of Adolescents. Int. J. Environ. Res. Public Health 2019, 16, 2767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, F.; Serra, E.; Garcia, O.F.; Martinez, I.; Cruise, E. A third emerging stage for the current digital society? Optimal parenting styles in Spain, the United States, Germany, and Brazil. Int. J. Environ. Res. Public Health 2019, 16, 2333. [Google Scholar] [CrossRef] [Green Version]
- Martínez, I.; Murgui, S.; García, O.F.; García, F. Parenting in the digital era: Protective and risk parenting styles for traditional bullying and cyberbullying victimization. Comput. Hum. Behav. 2019, 90, 84–92. [Google Scholar] [CrossRef]
- Ehrensaft, M.K.; Cohen, P.; Brown, J.; Smailes, E.; Chen, H.; Johnson, J.G. Intergenerational transmission of partner violence: A 20-year prospective study. J. Consult. Clin. Psychol. 2003, 71, 741–753. [Google Scholar] [CrossRef]
- Nikulina, V.; Gellin, M.; Zwilling, A. Is There a Cumulative Association Between Adverse Childhood Experiences and Intimate Partner Violence in Emerging Adulthood? J. Interpers. Violence 2017. [Google Scholar] [CrossRef]
- Kimber, M.; Adham, S.; Gill, S.; McTavish, J.; MacMillan, H.L. The association between child exposure to intimate partner violence (IPV) and perpetration of IPV in adulthood—A systematic review. Child. Abus. Negl. 2018, 76, 273–286. [Google Scholar] [CrossRef]
- Lieberman, A.F.; Van Horn, P.; Ippen, C.G. Toward evidence-based treatment: Child-parent psychotherapy with preschoolers exposed to marital violence. J. Am. Acad. Child. Adolesc. Psychiatry 2005, 44, 1241–1248. [Google Scholar] [CrossRef]
- Achenbach, T.M. Manual for the Child Behavior Checklist 4/18 and 1991 Profile; University of Vermont: Burlington, VT, USA, 1991. [Google Scholar]
- Achenbach, T.M.; Rescorla, L.A. Manual of the ASEBA Ages Form and Profile; University of Vermont, Research Center for Children, Youth and Families: Burlington, VT, USA, 2001. [Google Scholar]
- Mohr, W.K.; Lutz, M.J.N.; Fantuzzo, J.W.; Perry, M.A. Children Exposed to Family Violence A Review of Empirical Research from a Developmental- Ecological Perspective. Trauma Violence Abus. 2000, 1, 264–283. [Google Scholar] [CrossRef]
- Baremos para CBCL 6-18. UAB-y Servicio de Psicología Aplicada–UNED; Unitat d’Epidemiologia i de Diagnòstic en Psicopatologia del Desenvolupament: Barcelona, Spain, 2013.
- Rodrigo, M.J.; Martín, J.C.; Cabrera, E.; Máiquez, M.L. Las Competencias Parentales en Contextos de Riesgo Psicosocial. Interv. Psicosoc. 2009, 18, 113–120. [Google Scholar] [CrossRef]
- Barudy, J.; Dantagnan, M. Los Desafíos Invisibles de ser Madre o padre. Manual de Evaluación de las Competencias y la Resiliencia Parental; Gedisa: Barcelona, Spain, 2010. [Google Scholar]
- Osterlind, S.J. Constructing Tests Items; Kluwer Academic Publishers: Boston, MA, USA, 1989. [Google Scholar]
- Losada, J.L.; López-Feal, R. Métodos de Investigación en Conductas Humanas y Sociales; Thompson: Madrid, Spain, 2003. [Google Scholar]
- Kernick, M.; Wolf, M.; Holt, V.; Mcknight, B.; Huebner, C.; Rivara, F. Behavioral problems among children whose mothers are abused by an intimate partner. Child. Abus. Negl. 2003, 27, 1231–1246. [Google Scholar] [CrossRef] [PubMed]
- Masten, A.S.; Curtis, W.J. Integrating competence and psychopathology: Pathways toward a comprehensive science of adaption in development. Dev. Psychopathol. 2000, 12, 529–550. [Google Scholar] [CrossRef]
- Graham-Bermann, SA.; Howell, KH.; Lilly, MM.; Devoe, E. Mediators and moderators of change in adjustment following intervention for children exposed to intimate partner violence (IPV). J. Interpers. Violence 2011, 26, 1815–1833. [Google Scholar] [CrossRef] [PubMed]
- Gaxiola, J.C.; Millanes, R.M.; Aranda, C.L. Estilos de crianza en madres con experiencias de violencia de pareja. Psicumex 2017, 7, 22–39. [Google Scholar] [CrossRef]
- Manning, L.G.; Davies, P.T.; Cicchetti, D. Interparental violence and childhood adjustment: How and why maternal sensitivity is a protective factor. Child. Dev. 2014, 85, 2263–2278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amor, P.J.; Echeburúa, E.; Corral, P.; Zubizarreta, I.; Sarasúa, B. Repercusiones psicopatológicas de la violencia doméstica en la mujer en función de las circunstancias del maltrato. Rev. Int. De Psicol. Clínica Y De La Salud 2002, 2, 227–246. [Google Scholar]
- Gámez-Guadix, M.; Almendros, C. Exposición a la violencia entre los padres, prácticas de crianza y malestar psicológico a largo plazo en los hijos. Psychosoc. Interv. 2011, 20, 121–130. [Google Scholar] [CrossRef] [Green Version]
- Humphreys, C.; Mullender, A.; Thiara, R. Talking to My Mum’. Developing Communication Between Mothers and Children in the Aftermath of Domestic Violence. J. Soc. Work 2006, 6, 53–63. [Google Scholar] [CrossRef]
- Katz, E. Domestic Violence, Children’s Agency and Mother-Child Relationships: Towards a More Advanced Model. Child. Soc. 2015, 29, 69–79. [Google Scholar] [CrossRef]
- Katz, E. Recovery-Promoters:Ways in which Children and Mothers Support One Another’s Recoveries from Domestic Violence. Br. J. Soc. Work 2015, 45, 153–169. [Google Scholar] [CrossRef]
- Carracedo, S.; Fariña, F.; Seijo, D. Children exposed to intimate partner violence: Impact assessment and guidelines for intervention. Rev. De Psicol. Clínica Con Niños Y Con Adolesc. 2017, 5, 16–22. [Google Scholar] [CrossRef]
- Whaten, C.N.; MacMillan, H.L. Children’s exposure to intimate partner violence: Impacts and interventions. Paediatr. Child. Health 2013, 18, 419–422. [Google Scholar] [CrossRef] [Green Version]
- Olaya, B.; Tarragona, M.J.; de la Osa, N.; Ezpeleta, L. Protocolo de evaluación de niños y adolescentes víctimas de la violencia doméstica. Pap. Del Psicólogo 2008, 29, 123–135. [Google Scholar]
- Edleson, J.L.; Mbilinyi, L.F.; Beeman, S.K.; Hagemeister, A.K. How children are involved in adult domestic violence: Results from a four city telephone survey. J. Interpers. Violence 2003, 18, 18–32. [Google Scholar] [CrossRef]
- Howarth, E.; Moore, T.H.M.; Welton, N.J.; Lewis, N.; Stanley, N.; MacMillan, H.; Shaw, A.; Hester, M.; Bryden, P.; Feder, G. IMPRoving Outcomes for children exposed to domestic ViolencE (IMPROVE): An evidence synthesis. Public Health Res. 2016, 4, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, K.; Van Ee, E. Mothers and Children Exposed to Intimate Partner Violence: A Review of Treatment Interventions. Int. J. Environ. Res. Public Health 2018, 15, 1–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Austin, A.; Shanahan, M.; Barrios, Y.; Macy, R. A Systematic Review of Interventions for Women Parenting in the Context of Intimate Partner Violence. Trauma Violence Abus. 2017, 1, 1–11. [Google Scholar] [CrossRef]
- Cater, A.; Överlien, C. Children exposed to domestic violence: A discussion about research ethics and researchers’ responsibilities. Nord. Soc. Work Res. 2014, 4, 67–79. [Google Scholar] [CrossRef]


{kind=link}
| Children | Age | Range | Average; SD | |
| 6–17 | 10.96; 2.80 | |||
| Sex | n | % | ||
| - Boy | 22 | 47.80; 52.20 | ||
| - Girl | 24 | |||
| Women (n = 29) | Age | Range | Average; SD | |
| 27–48 | 36; 5.70 | |||
| Education | n | % | ||
| - Elementary | 19 | 65.5 | ||
| - Secondary/professional training | 9 | 31 | ||
| - Higher | 1 | 3.4 | ||
| Violence suffered | n | % | ||
| - Physical | 28 | 96.60 | ||
| - Psychological | 27 | 93.10 | ||
| - Sexual | 12 (*) | 41.40 | ||
| Nº children in the shelter | n | % | ||
| - 1 | 16 | 55.17 | ||
| - 2 | 9 | 31.03 | ||
| - 3 | 4 | 13.79 |
| Items of the Scale related to Quality of Mother Parenting Competences | No | Yes | ||
|---|---|---|---|---|
| n | % | n | % | |
| 1. Mother plays with him/her in the center—they spend time together | 37 | 84.1 | 7 | 15.9 |
| 2. Mother is affectionate with child’s demands | 34 | 75.6 | 11 | 24.4 |
| 3. Mother establishes rules and limits | 36 | 80.0 | 9 | 20.0 |
| 4. The mother stimulates the autonomy of the child | 24 | 54.5 | 20 | 45.5 |
| 5. The mother enjoys the time she spends with her son/daughter | 22 | 48.9 | 23 | 51.1 |
| Mother Plays with Him in the Center, They Spend Time Together | Mother is Affectionate with Child’s Demands | Mother Sets Appropriate Rules and Limits | Mother Enjoys Sharing Her Time with Her Child | Mother Stimulates the Child’s Personal Autonomy | |
|---|---|---|---|---|---|
| Anxiety/depression | −0,247 | −0,025 | −0,001 | −0,243 | −0,330 * |
| Withdrawn | −0,243 | 0,057 | 0,032 | −0,087 | 0,117 |
| Somatic complaints | −0,086 | −0,077 | −0,095 | −0,148 | −0,167 |
| Social problems | −0,431 ** | 0,032 | 0,090 | −0,271 | −0,250 |
| Thought problems | −0,102 | 0,039 | 0,054 | −0,109 | −0,175 |
| Attention problems | −0,296 | −0,062 | −0,139 | −0,413 ** | −0,380 * |
| Rule-breaking behaviors | −0,190 | −0,311 * | −0,315 * | −0,406 ** | −0,386 * |
| Aggressiveness | −0,238 | −0,289 | −0,269 | −0,394 * | −0,381* |
| Internalizing behaviors | −0,228 | −0,018 | −0,022 | −0,192 | −0,165 |
| Externalizing behaviors | −0,240 | −0,315 * | −0,301 | −0,425 ** | −0,408 ** |
| Total | −0,283 | −0,128 | −0,123 | −0,329 | −0,379 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosser-Limiñana, A.; Suriá-Martínez, R.; Mateo Pérez, M.Á. Children Exposed to Intimate Partner Violence: Association Among Battered Mothers’ Parenting Competences and Children’s Behavior. Int. J. Environ. Res. Public Health 2020, 17, 1134. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041134
Rosser-Limiñana A, Suriá-Martínez R, Mateo Pérez MÁ. Children Exposed to Intimate Partner Violence: Association Among Battered Mothers’ Parenting Competences and Children’s Behavior. International Journal of Environmental Research and Public Health. 2020; 17(4):1134. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041134
Chicago/Turabian StyleRosser-Limiñana, Ana, Raquel Suriá-Martínez, and Miguel Ángel Mateo Pérez. 2020. "Children Exposed to Intimate Partner Violence: Association Among Battered Mothers’ Parenting Competences and Children’s Behavior" International Journal of Environmental Research and Public Health 17, no. 4: 1134. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041134