Examining the Urban and Rural Healthcare Progress in Big Cities of China: Analysis of Monitoring Data in Dalian from 2008 to 2017

Abstract
:1. Introduction
2. Methods
2.1. Study Design and Data Collection
2.2. Procedure
2.3. Weighted TOPSIS Model
Standardization of Indicators
2.4. Analytic Hierarchy Process
2.5. Entropy Weight Method
2.6. Comprehensive Weight Model
2.7. TOPSIS Model
3. Results
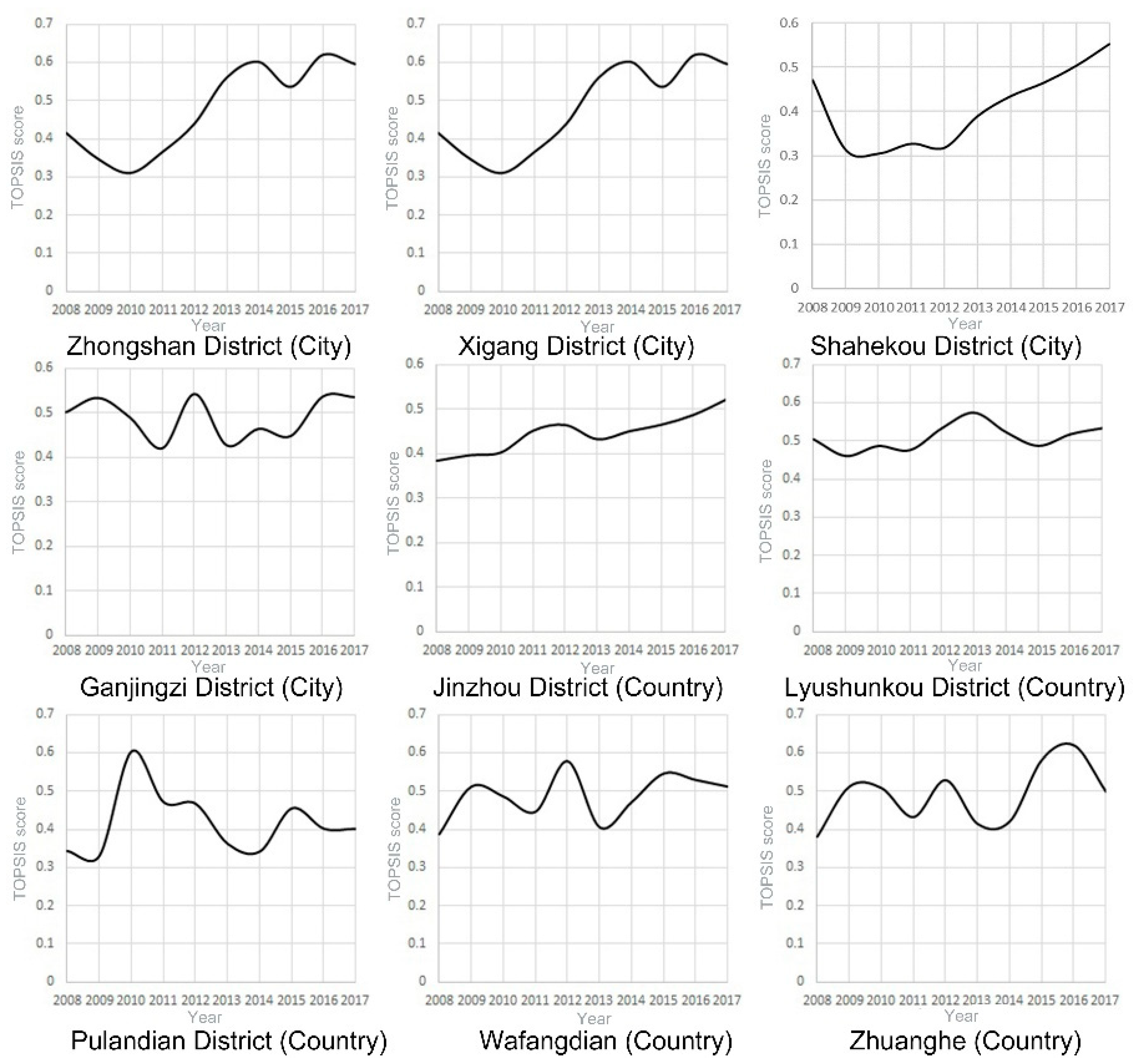
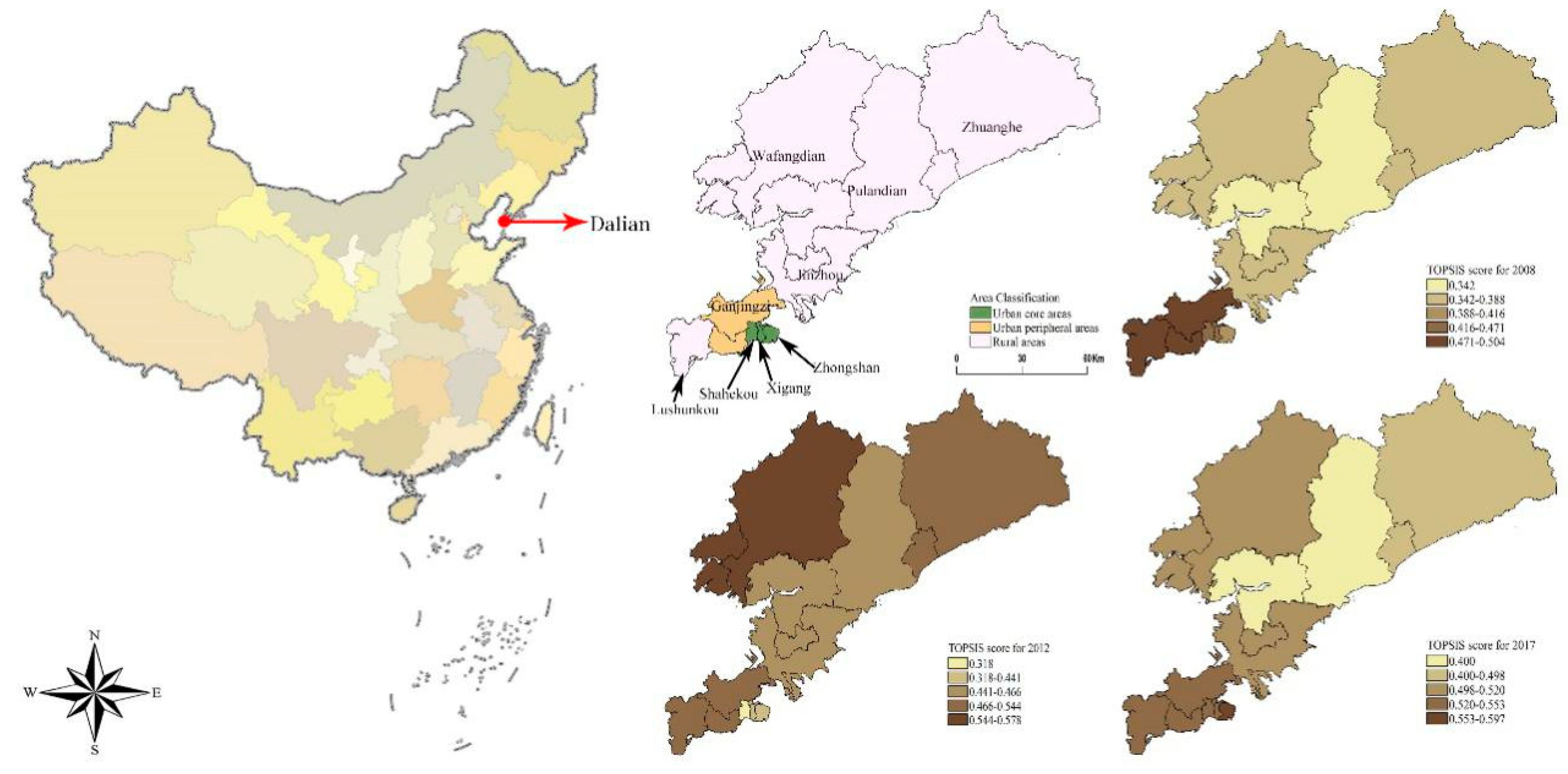
3.1. TOPSIS Scores of Urban and Rural Medical Care in Dalian
3.2. Indicator Contribution
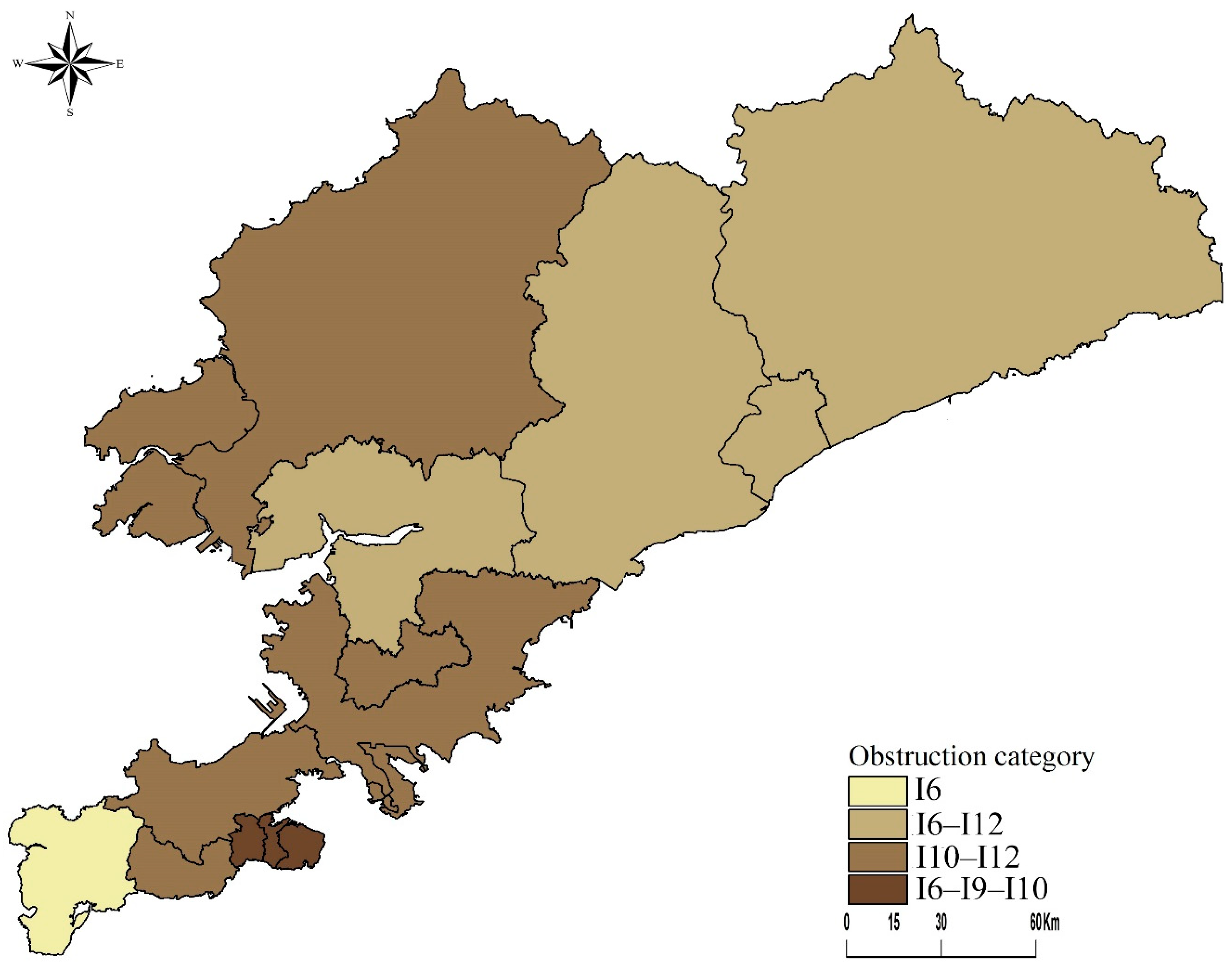
3.3. Obstructing Urban and Rural Medical Development Indicators
4. Discussion
4.1. Health Services in Urban vs. Rural Areas
4.2. Factors Promoting Healthcare Development
4.3. Obstacles to Healthcare Improvements
4.4. Application of this Research Model in Other Fields
4.5. Limitations of the Study
5. Conclusions
- Based on the results of the weighted TOPSIS model and the obstacle model, the healthcare services in Dalian’s urban areas have steadily increased, while those in the rural regions have been unstable and erratic. Although the urban–rural healthcare disparity has generally narrowed, continued progress is not assured.
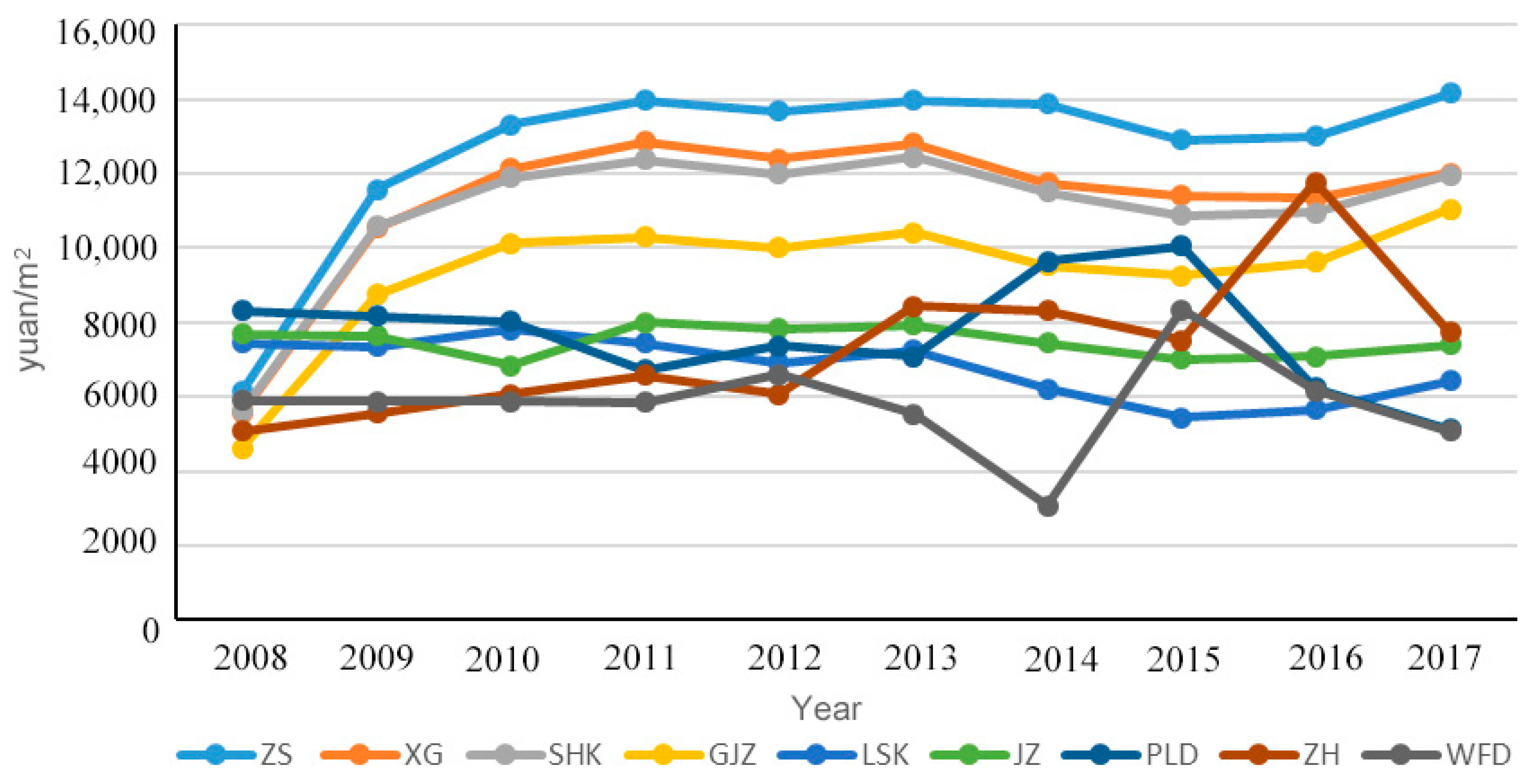
- Based on the location theory, residents in urban areas are more influenced by economic factors, while those in rural areas are more affected by time considerations. Therefore, when promoting the development of healthcare services in urban areas, policies and measures should consider the impact of land prices and per capita disposable income. For rural areas, constructing more medical institutions can effectively reduce the impact of time costs on the progress of health services.
- Different factors may hinder the development of healthcare systems in urban and rural areas. Urban areas should focus on coordinated development to address impediments in healthcare progress, while rural areas should address healthcare concerns based on local needs and conditions.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World bank. China’s Medical System Reform Policy Recommendations; World bank: Washington, DC, USA, 2010. [Google Scholar]
- Security, World Bank; World Health Organization; China Ministry of Finance; National Health and Family Planning Commission; Ministry of Human Resources and Social Security. Deepen the Reform of China’s Medical and Health System—Building a Quality-based Service Delivery System based on Value; Chinese Government Gazette: Beijing, China, 2018. [Google Scholar]
- World bank. World Bank Open Data; World bank: Washington, DC, USA, 2018. [Google Scholar]
- National Healthcare Security Administration. Notice on Doing a Good Job of Basic Medical Insurance for Urban and Rural Residents in 2019; National Healthcare Security Administration: Beijing, China, 2019.
- China State Council. China’s State Council Views on the Integration of Basic Medical Insurance System for Urban and Rural Residents; China State Council: Beijing, China, 2016.
- National Development and Reform Commission. Notice on Printing and Issuing Advice on Drug Price Reform; National Development and Reform Commission: Beijing, China, 2015.
- National Healthcare Security Administration. Notice of the National Health Insurance Administration on the Inclusion of 17 Kinds of Anticancer Drugs in the Category B of the National Basic Medical Insurance, Work Injury Insurance and Maternity Insurance Drug List; National Healthcare Security Administration: Beijing, China, 2018.
- World Health Organization. Who Collaborating Centres Database; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- United Nations. Un Databases; United Nations: New York, NY, USA, 2018. [Google Scholar]
- Yaya, S.; Uthman, O.A.; Okonofua, F.; Bishwajit, G. Decomposing the rural-urban gap in the factors of under-five mortality in sub-saharan africa? Evidence from 35 countries. BMC Public Health 2019, 19, 616. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Peterson, S.; Lavergne, R.; Ahuja, M.; McGrail, K. Predicting the cost of health care services: A comparison of case-mix systems and comorbidity indices that use administrative data. Med. Care 2019, 58, 114–119. [Google Scholar] [CrossRef]
- Yiengprugsawan, V.; Carmichael, G.A.; Lim, L.L.; Seubsman, S.A.; Sleigh, A.C. Has universal health insurance reduced socioeconomic inequalities in urban and rural health service use in thailand? Health Place 2010, 16, 1030–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.A.; Park, J.H.; Kim, M. Social and physical environments and self-rated health in urban and rural communities in korea. Int. J. Environ. Res. Public Health 2015, 12, 14329–14341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.L.A. Analysis on the integration of urban and rural medical insurance system. In Proceedings of the 2018 International Conference on Advanced Electronic Materials, Computers and Materials Engineering, Singapore, 14–16 September 2018; Volume 439, p. 032034. [Google Scholar]
- Today, C.P. China is integrating basic medical insurance system for urban and rural residents. China Popul. Today 2016, 1, 47. [Google Scholar]
- Wang, H.H.; Huang, S.M.; Zhang, L.X.; Rozelle, S.; Yan, Y.Y. A comparison of rural and urban healthcare consumption and health insurance. China Agric. Econ. Rev. 2010, 2, 212–227. [Google Scholar] [CrossRef] [Green Version]
- Alghnam, S.; Thorpe, R.; Gaskin, D. 27 The impact of traumatic injuries on medical expenditures in the United States: A population-based study. Inj. Prev. 2015, 21, 10. [Google Scholar] [CrossRef]
- Xu, J.; Wang, J.; King, M.; Liu, R.Y.; Yu, F.H.; Xing, J.S.; Su, L.; Lu, M.S. Rural-urban disparities in the utilization of mental health inpatient services in China: The role of health insurance. Int. J. Health Econ. Manag. 2018, 18, 377–393. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Sun, Y.; Zhang, Y.; Yi, D.; Ma, C.; Ma, S. Rural-urban disparity in health care: Observations from Suzhou, China. Public Health 2016, 138, 164–167. [Google Scholar] [CrossRef]
- Helt, E.H. Economic determinism—Model of political economy of medical care. Int. J. Health Serv. 1973, 3, 475–485. [Google Scholar] [CrossRef]
- Hibbard, J.H.G.M.; Jimison, H.; Capizzi, J.; Kunkel, L. The impact of a community-wide self-care information project on self-care and medical care utilization. Eval. Health Prof. 2001, 24, 404–423. [Google Scholar] [CrossRef] [PubMed]
- Fairchild, A.L. The rise and fall of the medical gaze: The political economy of immigrant medical inspection in modern america. Sci. Context 2006, 19, 337–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linde, A. The impact of improvements in medical care resources on homicide trends: The case of Germany (1977–2011). Eur. J. Crim. Policy Res. 2018, 24, 99–119. [Google Scholar] [CrossRef]
- Mandic, K.; Delibasic, B.; Knezevic, S.; Benkovic, S. Analysis of the financial parameters of Serbian banks through the application of the fuzzy ahp and topsis methods. Econ. Model. 2014, 43, 30–37. [Google Scholar] [CrossRef]
- Rakhshan, S.A. Efficiency ranking of decision making units in data envelopment analysis by using topsis-dea method. J. Oper. Res. Soc. 2017, 68, 906–918. [Google Scholar] [CrossRef]
- Bureau of Diplomatic Security. Dalian Statistical Yearbook; Dalian Bureau of Statistics: Dalian, China, 2008–2017.
- Dalian health bureau. Data from Dalian Health Monitoring Station; Dalian health bureau: Dalian, China, 2008–2017.
- Saaty, T.L. Decision-making with the AHP: Why is the principal eigenvector necessary. Eur. J. Oper. Res. 2003, 145, 85–91. [Google Scholar] [CrossRef]
- Ayağ, Z. A fuzzy AHP-based simulation approach to concept evaluation in a NPD environment. IIE Trans. 2005, 37, 827–842. [Google Scholar] [CrossRef]
- Ma, J.; Fan, Z.P.; Huang, L.H. A subjective and objective integrated approach to determine attribute weights. Eur. J. Oper. Res. 1999, 112, 397–404. [Google Scholar] [CrossRef]
- Zhang, H.; Gu, C.L.; Gu, L.W.; Zhang, Y. The evaluation of tourism destination competitiveness by TOPSIS & information entropy—A case in the Yangtze River Delta of China. Tour. Manag. 2011, 32, 443–451. [Google Scholar]
- Arlak, I.B.; Tolga, A.C. Evaluation of medical devices using fuzzy topsis with type-2 fuzzy numbers. In Proceedings of the 11th International FLINS Conference on Decision Making and Soft Computing, João Pessoa, Brazil, 18 August 2014. [Google Scholar]
- Lin, C.-T.; Tsai, M.-C. Development of an expert selection system to choose ideal cities for medical service ventures. Expert Syst. Appl. 2009, 36 Pt 1, 2266–2274. [Google Scholar] [CrossRef]
- Loprest, P.; Davidoff, A. How children with special health care needs affect the employment decisions of low-income parents. Matern. Child Health J. 2004, 8, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Pastor, C.J.M.; Escudero, M.A.G.; Martinez, A.M.; Ivanez, F.F.; Lloret, J.Q.; Roman, V.R. Impact of a social and employment crisis on the demand for mental health care (footwear crisis, elche 2004). Rev. De Psiquiatr. Y Salud Ment. 2011, 4, 75–80. [Google Scholar] [CrossRef] [PubMed]
- General Office of the STATE COUNCIL. Circular of the General Office of the STATE COUNCIL on the Pilot Work of New Rural Cooperative Medical System in the Second Half of 2004; General Office of the State Council: Beijing, China, 2004.
- General Office of the STATE COUNCIL. The General Office of the State Council Forwarded to the Ministry of Health and Other Departments on the Establishment of Notice on New Rural Cooperative Medical System; General Office of the State Council: Beijing, China, 2008.
- General Office of the STATE COUNCIL. Circular of the State Council on the Approval and Transmission of Several Opinions of the Ministry of Health and Other Departments on the Development and Improvement of Rural Cooperative Medical Care; General Office of the State Council: Beijing, China, 2016.
- Nickel, S. Location Theory; Springer: Berlin, Germany, 2005. [Google Scholar]
- Kelly, T. Back to the land: Arthurdale, fdr’s new deal, and the costs of economic planning. J. Soc. Hist. 2013, 46, 1106–1107. [Google Scholar] [CrossRef]
- Wan, F.; Xin, Z.; Zhou, L.; Bai, L.; Wang, Y.M.; Gu, S.H.; Liu, S.Q.; Li, M.M.; Sang, S.W.; Zhang, J.; et al. Heat vulnerability assessment in jinan city: A comparison between residents living in urban centers and urban-fringe areas. Zhonghua Liuxingbingxue Zazhi 2014, 35, 669–674. [Google Scholar] [PubMed]
- Liu, R.; Yan, B.-J.; Huang, Z.-P. Complexity analysis of urban public transit network. J. Transp. Syst. Eng. Inf. Technol. 2009, 9, 17–22. [Google Scholar]
- Pandit, A.; Lu, Z.; Crittenden, J.C. Managing the complexity of urban systems. J. Ind. Ecol. 2015, 19, 201–204. [Google Scholar] [CrossRef]
- Fleury, D. Urban safety management: How to deal with complexity. Adv. Complex Syst. 2007, 10, 327–338. [Google Scholar] [CrossRef]
- Harper, R.G.; Chacko, R.C.; Kotik-Harper, D.; Young, J.; Gotto, J. Self-report evaluation of health behavior, stress vulnerability, and medical outcome of heart transplant recipients. Psychosom. Med. 1998, 60, 563–569. [Google Scholar] [CrossRef]
- Bieler, G.; Paroz, S.; Faouzi, M.; Trueb, L.; Vaucher, P.; Althaus, F.; Daeppen, J.B.; Bodenmann, P. Social and medical vulnerability factors of emergency department frequent users in a universal health insurance system. Acad. Emerg. Med. 2012, 19, 63–68. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primary Index | Secondary Index | Tertiary Index | Average Value | Standardized Mean |
|---|---|---|---|---|
| social life system (A1) | population pressure (B1) (We defined population pressure as a variety of population data that can affect urban development within the city.) | population size (C1) | 5,831,091 people | 0.3162 |
| population density (C2) | 498,412.1 people/km2 | 0.3162 | ||
| population mechanical change rate (C3) | 3.09% | 0.2475 | ||
| population over 60 (C4) | 498,412 people | 0.3052 | ||
| rural population (C5) | 2.276 million people | 0.3129 | ||
| the cost of living (B2) (We defined the cost of living as income and expenditure necessary for urban living.) | per-capita disposable income (C6) | 37,282.2 yuan | 0.3103 | |
| housing prices (C7) | 8823.21 yuan/m2 | 0.3146 | ||
| health care consumption (C8) | 35,552.15 yuan | 0.2957 | ||
| economic system (A2) | regional economy (B3) (We used regional GDP as an indicator of the regional economy.) | regional GDP (C9) | 16.197 billion yuan | 0.3100 |
| government medical input (B4) (We used government expenditure on health as an indicator of medical construction.) | government health care expenditure (C10) | 437.9973 million yuan | 0.3005 | |
| medical system (A3). | primary medical facility (B5) (We used primary medical facility. The institution was defined as various types of hospitals that can meet the medical needs of urban residents, and the total size was represented by the number of medical beds.) | medical bed count (C11) | 35,552.15 beds | 0.3126 |
| the number of medical institutions (C12) | 1619.37 institutions | 0.3077 | ||
| medical staffing (B6) (To fully display the scale of medical personnel in Dalian, we have counted the number of doctors and in-service doctors in all medical institutions’ number of nurses.) | the number of doctors and nurses (C13) | 37282 people | 0.3071 | |
| the number of practicing and assistant doctors (C14) | 8800.28 people | 0.2470 | ||
| resident medical insurance (B7) (We took the number of people covered by medical insurance as one of the indicators reflecting residents medical security, but there were still residents who did not participate in medical insurance. To balance the supply and demand relationship, we added the number of doctors per 1000 people. with the number of nurses per thousand people to avoid research errors.) | the number of residents insured (C15) | 342,313 people | 0.2822 | |
| the number of doctors per thousand (C16) | 3.56 people | 0.31401 | ||
| the number of nurses per thousand (C17) | 7.14 people | 0.3118 |
| Index | EWM | AHP | Comprehensive Weight |
|---|---|---|---|
| C1 | 0.047 | 0.069 | 0.058 |
| C2 | 0.049 | 0.042 | 0.0455 |
| C3 | 0.029 | 0.042 | 0.0355 |
| C4 | 0.056 | 0.069 | 0.0625 |
| C5 | 0.086 | 0.026 | 0.056 |
| C6 | 0.025 | 0.059 | 0.042 |
| C7 | 0.108 | 0.034 | 0.071 |
| C8 | 0.044 | 0.041 | 0.0425 |
| C9 | 0.043 | 0.039 | 0.041 |
| C10 | 0.075 | 0.039 | 0.057 |
| C11 | 0.049 | 0.135 | 0.092 |
| C12 | 0.035 | 0.112 | 0.0735 |
| C13 | 0.071 | 0.138 | 0.1045 |
| C14 | 0.121 | 0.049 | 0.085 |
| C15 | 0.057 | 0.019 | 0.038 |
| C16 | 0.053 | 0.039 | 0.046 |
| C17 | 0.052 | 0.048 | 0.05 |
| Year | Urban | Rural | |||||||
|---|---|---|---|---|---|---|---|---|---|
| ZS | XG | SHK | GJZ | JZ | LSK | PLD | WFD | ZH | |
| 2008 | 0.4164 | 0.4662 | 0.4712 | 0.5023 | 0.3850 | 0.5037 | 0.3419 | 0.3876 | 0.3808 |
| 2009 | 0.3480 | 0.3127 | 0.3137 | 0.5346 | 0.3970 | 0.4591 | 0.3291 | 0.5118 | 0.5120 |
| 2010 | 0.3116 | 0.3146 | 0.3048 | 0.4897 | 0.4035 | 0.4856 | 0.6021 | 0.4859 | 0.5081 |
| 2011 | 0.3665 | 0.3485 | 0.3272 | 0.4208 | 0.4514 | 0.4747 | 0.4701 | 0.4465 | 0.4323 |
| 2012 | 0.4407 | 0.4235 | 0.3181 | 0.5436 | 0.4641 | 0.5337 | 0.4657 | 0.5778 | 0.5287 |
| 2013 | 0.5608 | 0.5107 | 0.3894 | 0.4275 | 0.4326 | 0.5752 | 0.3605 | 0.4056 | 0.4141 |
| 2014 | 0.6022 | 0.5725 | 0.4344 | 0.4646 | 0.4503 | 0.5225 | 0.3404 | 0.4719 | 0.421 |
| 2015 | 0.5368 | 0.4678 | 0.4646 | 0.4484 | 0.4647 | 0.4862 | 0.4538 | 0.546 | 0.582 |
| 2016 | 0.6208 | 0.5611 | 0.5037 | 0.5378 | 0.4865 | 0.5173 | 0.4003 | 0.5289 | 0.619 |
| 2017 | 0.5967 | 0.5466 | 0.5525 | 0.5365 | 0.5198 | 0.5337 | 0.4002 | 0.5116 | 0.4982 |
| Indicator | ZS | XG | SHK | GJZ | LSK | JZ | PLD | WFD | ZH |
|---|---|---|---|---|---|---|---|---|---|
| C1 | 6.04% | 5.70% | 5.57% | 5.91% | 5.56% | 5.98% | 5.73% | 8.53% | 5.20% |
| 5th | 6th | 7th | 6th | 8th | 6th | 6th | 4th | 9th | |
| C2 | 5.83% | 5.69% | 5.85% | 5.91% | 3.87% | 5.95% | 10.39% | 4.83% | 5.29% |
| 6th | 7th | 6th | 7th | 16th | 7th | 3rd | 10th | 7th | |
| C3 | 4.37% | 4.27% | 4.23% | 5.07% | 5.66% | 5.16% | 4.66% | 5.60% | 5.91% |
| 10th | 12th | 12th | 10th | 6th | 9th | 11th | 7th | 6th | |
| C4 | 5.18% | 6.20% | 7.36% | 3.94% | 4.63% | 3.08% | 3.38% | 6.33% | 4.95% |
| 7th | 4th | 4th | 15th | 12th | 16th | 15th | 6th | 12th | |
| C5 | - | - | - | 5.52% | 5.11% | 3.82% | 4.66% | 4.79% | 5.04% |
| 8th | 9th | 15th | 12th | 11th | 10th | ||||
| C6 | 8.57% | 8.63% | 8.56% | 9.83% | 10.35% | 10.37% | 10.52% | 10.85% | 10.50% |
| 1st | 1st | 1st | 2nd | 2nd | 2nd | 2nd | 2nd | 2nd | |
| C7 | 7.04% | 5.91% | 5.97% | 5.19% | 4.84% | 4.32% | 3.82% | 2.99% | 2.92% |
| 4th | 5th | 5th | 9th | 11th | 14th | 13th | 17th | 17th | |
| C8 | 4.11% | 4.17% | 4.75% | 3.81% | 4.50% | 4.80% | 4.67% | 4.11% | 3.78% |
| 13th | 13th | 9th | 16th | 13th | 10th | 10th | 13th | 16th | |
| C9 | 8.54% | 8.22% | 7.77% | 8.71% | 8.11% | 8.60% | 8.06% | 8.46% | 8.47% |
| 2nd | 2nd | 2nd | 4th | 4th | 4th | 5th | 5th | 4th | |
| C10 | 8.20% | 7.12% | 7.64% | 9.09% | 9.34% | 9.67% | 9.38% | 9.22% | 9.01% |
| 3rd | 3rd | 3rd | 3rd | 3rd | 3rd | 4th | 3rd | 3rd | |
| C11 | 3.16% | 2.75% | 2.47% | 2.39% | 5.66% | 2.66% | 2.92% | 3.09% | 4.26% |
| 16th | 16th | 16th | 17th | 7th | 17th | 17th | 16th | 15th | |
| C12 | 4.48% | 5.69% | 5.40% | 10.29% | 11.65% | 12.01% | 11.63% | 12.08% | 10.68% |
| 8th | 8th | 8th | 1st | 1st | 1st | 1st | 1st | 1st | |
| C13 | 4.47% | 4.49% | 4.56% | 4.87% | 4.04% | 4.64% | 5.09% | 4.35% | 5.21% |
| 9th | 10th | 11th | 12th | 15th | 12th | 9th | 12th | 8th | |
| C14 | 3.19% | 3.62% | 3.66% | 4.13% | 3.66% | 4.43% | 5.17% | 3.40% | 6.93% |
| 15th | 14th | 13th | 14th | 17th | 13th | 8th | 15th | 5th | |
| C15 | 4.25% | 4.36% | 4.75% | 4.97% | 4.97% | 4.66% | 5.33% | 4.90% | 4.79% |
| 11th | 11th | 10th | 11th | 10th | 11th | 7th | 9th | 13th | |
| C16 | 4.18% | 4.55% | 3.60% | 8.15% | 6.08% | 5.51% | 3.72% | 5.26% | 4.98% |
| 12th | 9th | 14th | 5th | 5th | 8th | 14th | 8th | 11th | |
| C17 | 3.34% | 3.11% | 2.91% | 4.64% | 4.37% | 6.74% | 3.27% | 3.61% | 4.48% |
| 14th | 15th | 15th | 13th | 14th | 5th | 16th | 14th | 14th |
| Obstacle Factor | Summary of Indicator Information | ZS | XG | SHK | GJZ | LSK | JZ | PLD | WFD | ZH |
|---|---|---|---|---|---|---|---|---|---|---|
| I1 | population size | 5.38 | 5.07 | 4.94 | 5.56 | 8.28 | 5.62 | 5.28 | 7.74 | 4.73 |
| I2 | population density | 5.98 | 5.06 | 5.19 | 5.55 | 8.15 | 5.59 | 9.58 | 4.42 | 4.81 |
| I3 | population mechanical change rate | 5.15 | 5.16 | 5.44 | 5.16 | 5.98 | 5.28 | 6.85 | 9.25 | 9.76 |
| I4 | population over 60 | 5.71 | 5.67 | 5.61 | 3.74 | 4.48 | 2.94 | 3.17 | 5.79 | 4.56 |
| I5 | rural population | - | - | - | 5.88 | 5.24 | 3.64 | 4.33 | 4.35 | 4.59 |
| I6 | per capita disposable income | 10.83 | 11.22 | 11.25 | 8.66 | 10.20 | 9.38 | 11.35 | 8.49 | 10.12 |
| I7 | housing prices | 6.33 | 6.30 | 6.32 | 4.90 | 4.64 | 4.06 | 3.55 | 2.74 | 2.70 |
| I8 | health care consumption | 4.80 | 4.81 | 4.53 | 3.67 | 4.38 | 4.74 | 4.53 | 3.90 | 3.53 |
| I9 | regional GDP | 10.75 | 10.44 | 10.99 | 7.76 | 9.05 | 8.31 | 8.83 | 7.79 | 7.81 |
| I10 | government health care expenditure | 10.38 | 10.37 | 10.88 | 10.26 | 7.76 | 10.10 | 7.60 | 10.32 | 7.40 |
| I11 | medical bed count | 4.85 | 4.45 | 4.21 | 2.24 | 5.54 | 2.52 | 2.72 | 2.86 | 3.89 |
| I12 | the number of medical institutions | 5.12 | 5.15 | 5.86 | 10.48 | 3.77 | 12.96 | 11.00 | 12.45 | 11.94 |
| I13 | the number of doctors and nurses | 5.11 | 5.12 | 5.17 | 4.65 | 3.94 | 4.45 | 4.82 | 4.05 | 4.74 |
| I14 | the number of practicing and assistant doctors | 4.86 | 5.24 | 5.25 | 3.95 | 3.53 | 4.21 | 4.78 | 3.10 | 6.31 |
| I15 | the number of residents insured | 5.00 | 5.12 | 4.53 | 4.94 | 4.91 | 4.54 | 5.15 | 4.60 | 4.48 |
| I16 | the number of doctors per thousand | 4.73 | 5.05 | 4.22 | 8.22 | 5.88 | 5.24 | 3.43 | 4.79 | 4.53 |
| I17 | the number of nurses per thousand | 5.01 | 5.77 | 5.60 | 4.36 | 4.25 | 6.42 | 3.02 | 3.34 | 4.11 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qiu, Y.; Lu, W.; Guo, J.; Sun, C.; Liu, X. Examining the Urban and Rural Healthcare Progress in Big Cities of China: Analysis of Monitoring Data in Dalian from 2008 to 2017. Int. J. Environ. Res. Public Health 2020, 17, 1148. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041148
Qiu Y, Lu W, Guo J, Sun C, Liu X. Examining the Urban and Rural Healthcare Progress in Big Cities of China: Analysis of Monitoring Data in Dalian from 2008 to 2017. International Journal of Environmental Research and Public Health. 2020; 17(4):1148. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041148
Chicago/Turabian StyleQiu, Yukun, Wei Lu, Jianke Guo, Caizhi Sun, and Xinyu Liu. 2020. "Examining the Urban and Rural Healthcare Progress in Big Cities of China: Analysis of Monitoring Data in Dalian from 2008 to 2017" International Journal of Environmental Research and Public Health 17, no. 4: 1148. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041148