Endurance Training vs. Circuit Resistance Training: Effects on Lipid Profile and Anthropometric/Body Composition Status in Healthy Young Adult Women

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Testing and Variables
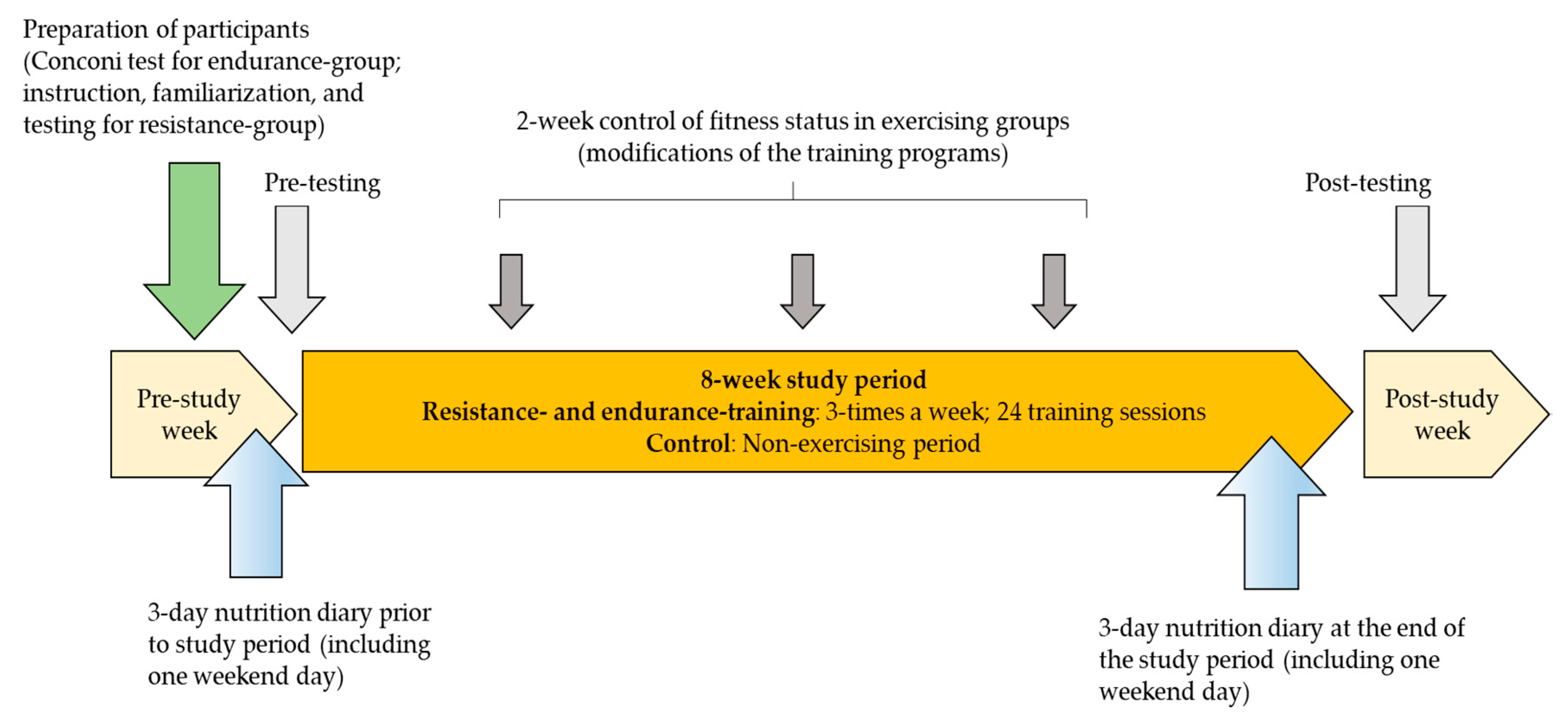
2.3. Physical Exercise Programs
2.4. Statistics
3. Results
4. Discussion
4.1. Positive Effects of Endurance and Resistance Training on Anthropometric/Body Composition Indices
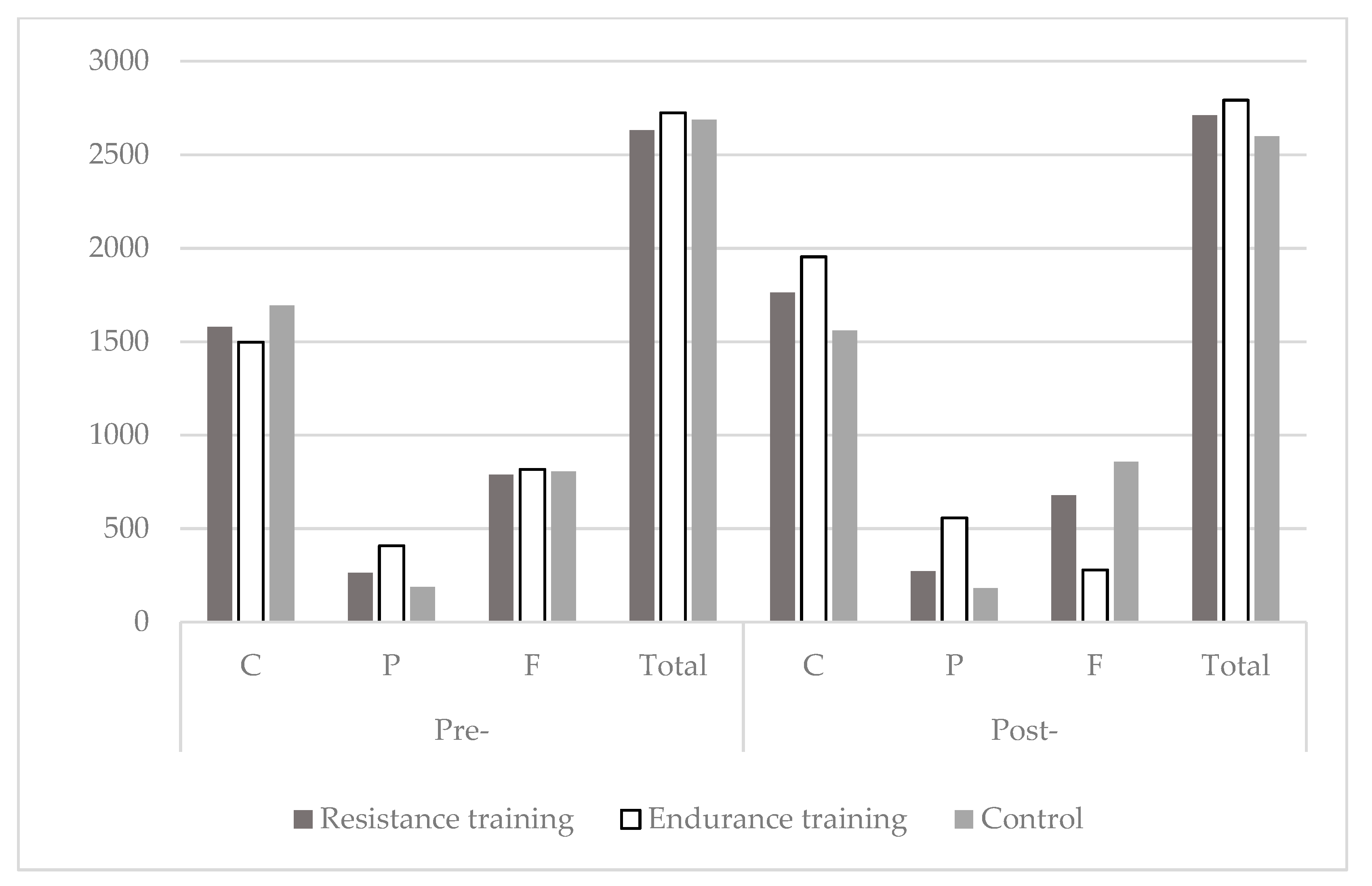
4.2. Positive Effects of Endurance and Resistance Training on Plasma Glucose and Lipid Profile
4.3. Study Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Crews, W.D., Jr.; Harrison, D.W.; Wright, J.W. A double-blind, placebo-controlled, randomized trial of the effects of dark chocolate and cocoa on variables associated with neuropsychological functioning and cardiovascular health: Clinical findings from a sample of healthy, cognitively intact older adults. Am. J. Clin. Nutr. 2008, 87, 872–880. [Google Scholar] [PubMed] [Green Version]
- Mann, S.; Beedie, C.; Jimenez, A. Differential effects of aerobic exercise, resistance training and combined exercise modalities on cholesterol and the lipid profile: Review, synthesis and recommendations. Sports Med. 2014, 44, 211–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marandi, S.M.; Abadi, N.G.; Esfarjani, F.; Mojtahedi, H.; Ghasemi, G. Effects of intensity of aerobics on body composition and blood lipid profile in obese/overweight females. Int. J. Prev. Med. 2013, 4, S118–S125. [Google Scholar] [PubMed]
- Saghafi-Asl, M.; Pirouzpanah, S.; Ebrahimi-Mameghani, M.; Asghari-Jafarabadi, M.; Aliashrafi, S.; Sadein, B. Lipid profile in relation to anthropometric indices and insulin resistance in overweight women with polycystic ovary syndrome. Health Promot. Perspect. 2013, 3, 206–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alnasir, F.A.; Masuadi, E.M. The effect of loss of body weight on lipid profile in overweight individuals. Saudi Med. J. 2006, 27, 687–692. [Google Scholar]
- Hwang, W.J.; Kim, J.A. Developing a Health-Promotion Program Based on the Action Research Paradigm to Reduce Cardiovascular Disease Risk Factors among Blue Collar Workers. Int. J. Environ. Res. Public Health 2019, 16, 4958. [Google Scholar] [CrossRef] [Green Version]
- Ratajczak, M.; Skrypnik, D.; Bogdanski, P.; Madry, E.; Walkowiak, J.; Szulinska, M.; Maciaszek, J.; Kregielska-Narozna, M.; Karolkiewicz, J. Effects of Endurance and Endurance-Strength Training on Endothelial Function in Women with Obesity: A Randomized Trial. Int. J. Environ. Res. Public Health 2019, 16, 4291. [Google Scholar] [CrossRef] [Green Version]
- Tran, B.X.; Dang, K.A.; Le, H.T.; Ha, G.H.; Nguyen, L.H.; Nguyen, T.H.; Tran, T.H.; Latkin, C.A.; Ho, C.S.H.; Ho, R.C.M. Global Evolution of Obesity Research in Children and Youths: Setting Priorities for Interventions and Policies. Obes. Facts 2019, 12, 137–149. [Google Scholar] [CrossRef]
- Swift, D.L.; Johannsen, N.M.; Lavie, C.J.; Earnest, C.P.; Church, T.S. The role of exercise and physical activity in weight loss and maintenance. Prog. Cardiovasc. Dis. 2014, 56, 441–447. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Kyrolainen, H.; Hackney, A.C.; Salminen, R.; Repola, J.; Hakkinen, K.; Haimi, J. Effects of Combined Strength and Endurance Training on Physical Performance and Biomarkers of Healthy Young Women. J. Strength Cond. Res. 2018, 32, 1554–1561. [Google Scholar] [CrossRef]
- Alberga, A.S.; Farnesi, B.C.; Lafleche, A.; Legault, L.; Komorowski, J. The effects of resistance exercise training on body composition and strength in obese prepubertal children. Phys. Sportsmed. 2013, 41, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Stangier, C.; Abel, T.; Mierau, J.; Hollmann, W.; Struder, H.K. Effects of Cycling Versus Running Training on Sprint and Endurance Capacity in Inline Speed Skating. J. Sports Sci. Med. 2016, 15, 41–49. [Google Scholar] [PubMed]
- Hottenrott, K.; Ludyga, S.; Schulze, S. Effects of high intensity training and continuous endurance training on aerobic capacity and body composition in recreationally active runners. J. Sports Sci. Med. 2012, 11, 483–488. [Google Scholar]
- Delgado-Floody, P.; Latorre-Roman, P.; Jerez-Mayorga, D.; Caamano-Navarrete, F.; Garcia-Pinillos, F. Feasibility of incorporating high-intensity interval training into physical education programs to improve body composition and cardiorespiratory capacity of overweight and obese children: A systematic review. J. Exerc. Sci. Fit. 2019, 17, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Paoli, A.; Pacelli, Q.F.; Moro, T.; Marcolin, G.; Neri, M.; Battaglia, G.; Sergi, G.; Bolzetta, F.; Bianco, A. Effects of high-intensity circuit training, low-intensity circuit training and endurance training on blood pressure and lipoproteins in middle-aged overweight men. Lipids Health Dis. 2013, 12, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagstrom, A.D.; Marshall, P.W.; Halaki, M.; Hackett, D.A. The Effect of Resistance Training in Women on Dynamic Strength and Muscular Hypertrophy: A Systematic Review with Meta-analysis. Sports Med. 2019. [Google Scholar] [CrossRef]
- Evans, J.W. Periodized Resistance Training for Enhancing Skeletal Muscle Hypertrophy and Strength: A Mini-Review. Front. Physiol. 2019, 10, 13. [Google Scholar] [CrossRef]
- Schoenfeld, B.J.; Grgic, J.; Ogborn, D.; Krieger, J.W. Strength and Hypertrophy Adaptations Between Low- vs. High-Load Resistance Training: A Systematic Review and Meta-analysis. J. Strength Cond. Res. 2017, 31, 3508–3523. [Google Scholar] [CrossRef]
- Duxbury, L. Work-life conflict in Canada in the new millennium-A status report. Sydney Papers 2003, 15, 78. [Google Scholar]
- American Psychiatric Association. Annual Convention Report; American Psychiatric Association: Arlongton, VA, USA, 2013; No. 8. [Google Scholar]
- Aleksovska, K.; Puggina, A.; Giraldi, L.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Chantal, S.; Ciarapica, D.; Colotto, M.; et al. Biological determinants of physical activity across the life course: A “Determinants of Diet and Physical Activity” (DEDIPAC) umbrella systematic literature review. Sports Med. Open 2019, 5, 2. [Google Scholar] [CrossRef]
- EU Special Eurobarometer 412 on“Sport and Physical Activity” Special Eurobarometer. Available online: https://ec.europa.eu/commfrontoffice/publicopinion/archives/ebs/ebs_412_en.pdf (accessed on 11 February 2020).
- Strachan, S.M.; Perras, M.G.; Brawley, L.R.; Spink, K.S. Exercise in challenging times: The predictive utility of identity, self-efficacy, and past exercise. Sport Exerc. Perform. Psychol. 2016, 5, 247. [Google Scholar] [CrossRef]
- Locke, S.R.; Brawley, L.R. Perceptions of exercise consistency: Relation to exercise-related cognitive errors and cognitions. J. Health Psychol. 2017, 22, 684–694. [Google Scholar] [CrossRef] [PubMed]
- Fett, C.A.; Fett, W.C.; Marchini, J.S. Circuit weight training vs jogging in metabolic risk factors of overweight/obese women. Arq. Bras. Cardiol. 2009, 93, 519–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barranco-Ruiz, Y.; Ramirez-Velez, R.; Martinez-Amat, A.; Villa-Gonzalez, E. Effect of Two Choreographed Fitness Group-Workouts on the Body Composition, Cardiovascular and Metabolic Health of Sedentary Female Workers. Int. J. Environ. Res. Public Health 2019, 16, 4986. [Google Scholar] [CrossRef] [Green Version]
- Zenic, N.; Rausavljevic, N.; Bercic, H. Leisure-time physical activities: The anthropological benefits and health risks. Kinesiol. Slov. 2006, 12, 75–83. [Google Scholar]
- Condello, G.; Puggina, A.; Aleksovska, K.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Simon, C.; Ciarapica, D.; Coppinger, T.; et al. Behavioral determinants of physical activity across the life course: A “DEterminants of DIet and Physical ACtivity” (DEDIPAC) umbrella systematic literature review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 58. [Google Scholar] [CrossRef] [Green Version]
- Cortis, C.; Puggina, A.; Pesce, C.; Aleksovska, K.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Simon, C.; Ciarapica, D.; et al. Psychological determinants of physical activity across the life course: A “DEterminants of DIet and Physical ACtivity” (DEDIPAC) umbrella systematic literature review. PLoS ONE 2017, 12, e0182709. [Google Scholar] [CrossRef]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Merz, C.N.B.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2889–2934. [Google Scholar] [CrossRef] [Green Version]
- Heyward, V.H.; Stolarczyk, L.M. Applied Body Composition Assessment; Human Kinetics: Padsey, UK, 1996. [Google Scholar]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Kulier, I. Prehrambene Tablice (Kemijski Sastav Namirnica); Hrvatski Farmer: Zagreb, Croatia, 1996. [Google Scholar]
- Conconi, F.; Grazzi, G.; Casoni, I.; Guglielmini, C.; Borsetto, C.; Ballarin, E.; Mazzoni, G.; Patracchini, M.; Manfredini, F. The Conconi test: Methodology after 12 years of application. Int. J. Sports Med. 1996, 17, 509–519. [Google Scholar] [CrossRef]
- Nikolaizik, W.H.; Knopfli, B.; Leister, E.; de Boer, P.; Sievers, B.; Schoni, M.H. The anaerobic threshold in cystic fibrosis: Comparison of V-slope method, lactate turn points, and Conconi test. Pediatr. Pulmonol. 1998, 25, 147–153. [Google Scholar] [CrossRef]
- Ferguson, C.J. An effect size primer: A guide for clinicians and researchers. Prof. Psychol. Res. Pract. 2009, 40, 532. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Assosiates: New York, NY, USA, 1988. [Google Scholar]
- Stasiulis, A.; Mockiene, A.; Vizbaraite, D.; Mockus, P. Aerobic exercise-induced changes in body composition and blood lipids in young women. Medicina (Kaunas) 2010, 46, 129–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LeMura, L.M.; von Duvillard, S.P.; Andreacci, J.; Klebez, J.M.; Chelland, S.A.; Russo, J. Lipid and lipoprotein profiles, cardiovascular fitness, body composition, and diet during and after resistance, aerobic and combination training in young women. Eur. J. Appl. Physiol. 2000, 82, 451–458. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K.; American College of Sports Medicine. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]
- Williams, C.B.; Zelt, J.G.; Castellani, L.N.; Little, J.P.; Jung, M.E.; Wright, D.C.; Tschakovsky, M.E.; Gurd, B.J. Changes in mechanisms proposed to mediate fat loss following an acute bout of high-intensity interval and endurance exercise. Appl. Physiol. Nutr. Metab. 2013, 38, 1236–1244. [Google Scholar] [CrossRef]
- Lee, M.G.; Park, K.S.; Kim, D.U.; Choi, S.M.; Kim, H.J. Effects of high-intensity exercise training on body composition, abdominal fat loss, and cardiorespiratory fitness in middle-aged Korean females. Appl. Physiol. Nutr. Metab. 2012, 37, 1019–1027. [Google Scholar] [CrossRef]
- Millet, G.; Perrey, S.; Divert, C.; Foissac, M. The role of engineering in fatigue reduction during human locomotion—A review. Sports Eng. 2006, 9, 209–220. [Google Scholar] [CrossRef]
- Grampp, J.; Willson, J.; Kernozek, T. The plantar loading variations to uphill and downhill gradients during treadmill walking. Foot Ankle Int. 2000, 21, 227–231. [Google Scholar] [CrossRef]
- Cunha, P.M.; Tomeleri, C.M.; Nascimento, M.A.; Mayhew, J.L.; Fungari, E.; Trindade, L.; Barbosa, D.S.; Venturini, D.; Cyrino, E.S. Comparision of Low and High Volume of Resistance Training on Body Fat and Blood Biomarkers in Untrained Older Women: A Randomized Clinical Trial. J. Strength Cond. Res. 2019. [Google Scholar] [CrossRef]
- Franco, C.M.C.; Carneiro, M.; Alves, L.T.H.; Junior, G.N.O.; de Sousa, J.F.R.; Orsatti, F.L. Lower-Load is More Effective Than Higher-Load Resistance Training in Increasing Muscle Mass in Young Women. J. Strength Cond. Res. 2019, 33 (Suppl. S1), S152–S158. [Google Scholar] [CrossRef]
- Gettman, L.R.; Pollock, M.L. Circuit Weight Training: A Critical Review of Its Physiological Benefits. Phys. Sportsmed. 1981, 9, 44–60. [Google Scholar] [CrossRef] [PubMed]
- Gettman, L.R.; Ayres, J.J.; Pollock, M.L.; Jackson, A. The effect of circuit weight training on strength, cardiorespiratory function, and body composition of adult men. Med. Sci. Sports 1978, 10, 171–176. [Google Scholar] [PubMed]
- Dinyer, T.K.; Byrd, M.T.; Garver, M.J.; Rickard, A.J.; Miller, W.M.; Burns, S.; Clasey, J.L.; Bergstrom, H.C. Low-Load vs. High-Load Resistance Training to Failure on One Repetition Maximum Strength and Body Composition in Untrained Women. J. Strength Cond. Res. 2019, 33, 1737–1744. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, F.C.; de Medeiros, A.I.; Nicioli, C.; Nunes, J.E.; Shiguemoto, G.E.; Prestes, J.; Verzola, R.M.; Baldissera, V.; Perez, S.E. Circuit resistance training in sedentary women: Body composition and serum cytokine levels. Appl. Physiol. Nutr. Metab. 2010, 35, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Franklin, N.C.; Robinson, A.T.; Bian, J.T.; Ali, M.M.; Norkeviciute, E.; McGinty, P.; Phillips, S.A. Circuit resistance training attenuates acute exertion-induced reductions in arterial function but not inflammation in obese women. Metab. Syndr. Relat. Disord. 2015, 13, 227–234. [Google Scholar] [CrossRef] [Green Version]
- Ghanbari-Niaki, A.; Saeidi, A.; Ahmadian, M.; Gharahcholo, L.; Naghavi, N.; Fazelzadeh, M.; Mahjoub, S.; Myers, S.; Williams, A. The combination of exercise training and Zataria multiflora supplementation increase serum irisin levels in postmenopausal women. Integr. Med. Res. 2018, 7, 44–52. [Google Scholar] [CrossRef]
- Holloszy, J.O.; Kohrt, W.M. Regulation of carbohydrate and fat metabolism during and after exercise. Annu. Rev. Nutr. 1996, 16, 121–138. [Google Scholar] [CrossRef]
- Borghouts, L.B.; Keizer, H.A. Exercise and insulin sensitivity: A review. Int. J. Sports Med. 2000, 21, 1–12. [Google Scholar] [CrossRef]
- Conn, V.S.; Koopman, R.J.; Ruppar, T.M.; Phillips, L.J.; Mehr, D.R.; Hafdahl, A.R. Insulin Sensitivity Following Exercise Interventions: Systematic Review and Meta-Analysis of Outcomes Among Healthy Adults. J. Prim. Care Community Health 2014, 5, 211–222. [Google Scholar] [CrossRef] [Green Version]
- Coggan, A.R. Plasma glucose metabolism during exercise in humans. Sports Med. 1991, 11, 102–124. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Lauer, J.A.; Hutubessy, R.C.; Niessen, L.; Tomijima, N.; Rodgers, A.; Lawes, C.M.; Evans, D.B. Effectiveness and costs of interventions to lower systolic blood pressure and cholesterol: A global and regional analysis on reduction of cardiovascular-disease risk. Lancet 2003, 361, 717–725. [Google Scholar] [CrossRef]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Blaha, M.J.; Dai, S.; Ford, E.S.; Fox, C.S.; Franco, S.; et al. Executive summary: Heart disease and stroke statistics—2014 update: A report from the American Heart Association. Circulation 2014, 129, 399–410. [Google Scholar] [CrossRef] [PubMed]
- Dunn, A.L.; Marcus, B.H.; Kampert, J.B.; Garcia, M.E.; Kohl, H.W., 3rd; Blair, S.N. Reduction in cardiovascular disease risk factors: 6-month results from Project Active. Prev. Med. 1997, 26, 883–892. [Google Scholar] [CrossRef]
- Millet, G.P.; Vleck, V.E.; Bentley, D.J. Physiological differences between cycling and running. Sports Med. 2009, 39, 179–206. [Google Scholar] [CrossRef]
- Prabhakaran, B.; Dowling, E.A.; Branch, J.D.; Swain, D.P.; Leutholtz, B.C. Effect of 14 weeks of resistance training on lipid profile and body fat percentage in premenopausal women. Br. J. Sports Med. 1999, 33, 190–195. [Google Scholar] [CrossRef]
- Sheikholeslami Vatani, D.; Ahmadi, S.; Ahmadi Dehrashid, K.; Gharibi, F. Changes in cardiovascular risk factors and inflammatory markers of young, healthy, men after six weeks of moderate or high intensity resistance training. J. Sports Med. Phys. Fit. 2011, 51, 695–700. [Google Scholar]



{kind=link}
{kind=link}
| Exercise | Equipment used | Week 1 | Week 2 | Week 3 | Week 4 | Week 5 | Week 6 | Week 7 | Week 8 |
|---|---|---|---|---|---|---|---|---|---|
| Abdominal curls | OBW | x | x | x | x | ||||
| Abdominal curls (added weights) | OBW + FW | xx | xx | xx | xx | ||||
| Leg raises | OBW | x | |||||||
| Hyperextension bench | OBW | x | x | x | xx | xx | xx | x | x |
| Knee extension | WM | x | x | ||||||
| Hamstring curl | WM | x | x | x | x | x | x | x | |
| Lunges | OBW | x | x | x | |||||
| Lunges (added weights) | OBW + FW | x | x | ||||||
| Squats | OBW | x | x | x | |||||
| Squats (added weights) | OBW + FW | x | x | ||||||
| Legg adductions | WM | x | x | x | x | x | |||
| Legg abductions | WM | x | x | x | x | x | |||
| Latt pulldowns | WM | x | x | x | x | ||||
| Rowing torso | WM | x | x | x | x | ||||
| Biceps curls | x | x | x | x | x | ||||
| Triceps extension | WM | x | x | x | |||||
| Butterfly bench | WM | x | x | x | |||||
| Bench press | WM & FW | x | x | x | x | x | |||
| Inclined bench press | WM & FW | ||||||||
| Overhead press | WM & FW | x | x | x | |||||
| Number of circuits per training session | 2 | 2 | 3 | 3 | 2 | 3 | 3 | 2 | |
| Time of work per set (in seconds) | 30 | 30 | 25 | 30 | 30 | 30 | 30 | 30 | |
| Rest between sets (in seconds) | 30 | 30 | 35 | 30 | 30 | 30 | 30 | 30 | |
| Rest between circuits (in minutes) | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | |
| Warm-up (in minutes) | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | |
| Cool-down (in minutes) | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | |
| Variables | Resistance-Training (n = 19) | Endurance-Training (n = 20) | Control (n = 18) | |||
|---|---|---|---|---|---|---|
| Pre- | Post- | Pre- | Post- | Pre- | Post- | |
| BM (kg) | 66.53 ± 6.51 | 62.4 ± 6.58 * | 67.35 ± 8.39 | 62.38 ± 8.56 * | 64.89 ± 7.05 | 64.06 ± 7.78 |
| BMI (kg/m2) | 24.02 ± 2.39 | 22.82 ± 2.39 * | 25.11 ± 2.69 | 23.09 ± 2.79 * | 23.55 ± 2.32 | 23.99 ± 2.32 |
| Tr_SF (mm) | 24.71 ± 6.3 | 20.56 ± 3.56 * | 26.78 ± 6.58 | 21.39 ± 4.03 * | 23.09 ± 9.84 | 23.47 ± 9.56 |
| Th_SF (mm) | 23.68 ± 9.99 | 21.06 ± 4.88 * | 25.74 ± 7.52 | 23.87 ± 5.46 * | 22.56 ± 5.2 | 22.58 ± 8.83 |
| SI_SF (mm) | 18.27 ± 7.04 | 15.24 ± 3.02 * | 20.57 ± 4.41 | 17.7 ± 3.7 * | 17.76 ± 5.68 | 17.56 ± 6.4 |
| BF (%) | 34.92 ± 5.79 | 29.89 ± 4.41 * | 36.43 ± 5.43 | 30.14 ± 4.04 * | 33.99 ± 5.92 | 34.05 ± 6.11 |
| TC (mmol/L) | 4.57 ± 0.6 | 3.98 ± 0.55 * | 4.94 ± 0.56 | 3.77 ± 0.47 * | 4.63 ± 0.59 | 4.51 ± 0.57 |
| HDL (mmol/L) | 1.63 ± 0.25 | 1.09 ± 0.16 * | 1.74 ± 0.27 | 1.25 ± 0.18* | 1.57 ± 0.21 | 1.59 ± 0.26 |
| LDL (mmol/L) | 3.42 ± 0.48 | 2.5 8± 0.47 * | 3.36 ± 0.43 | 2.21 ± 0.46 * | 3.14 ± 0.62 | 2.96 ± 0.51 |
| TG (mmol/L) | 1.15 ± 0.15 | 0.6 ± 0.13 * | 1.18 ± 0.23 | 0.72 ± 0.16 * | 1.19 ± 0.22 | 1.01 ± 0.23 * |
| PG (mmol/L) | 5.19 ± 0.55 | 4.06 ± 0.42 * | 4.89 ± 0.54 | 4.25 ± 0.6 * | 5.04 ± 0.51 | 4.92 ± 0.36 |
| Variables | Main Effects | Interaction | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Group | Measurement | Group × Measurement | |||||||
| F-Test | p | η2 | F-Test | p | η2 | F-Test | p | η2 | |
| BM (kg) | 0.1 | 0.88 | 0.01 | 327.1 | 0.001 | 0.87 | 128 | 0.001 | 0.72 |
| BMI (kg/m2) | 0.63 | 0.53 | 0.02 | 143.97 | 0.001 | 0.73 | 60.77 | 0.001 | 0.69 |
| Tr_SF (mm) | 0.93 | 0.39 | 0.03 | 73.73 | 0.001 | 0.58 | 21.36 | 0.001 | 0.44 |
| Th_SF (mm) | 6.31 | 0.01 | 0.19 | 146.63 | 0.001 | 0.73 | 36.25 | 0.001 | 0.57 |
| SI_SF (mm) | 1.75 | 0.18 | 0.06 | 39.1 | 0.001 | 0.42 | 8.73 | 0.001 | 0.25 |
| BF (%) | 3.98 | 0.03 | 0.13 | 183.91 | 0.001 | 0.77 | 46.45 | 0.001 | 0.63 |
| TC (mmol/L) | 1.75 | 0.18 | 0.06 | 84.62 | 0.001 | 0.61 | 19.45 | 0.001 | 0.42 |
| HDL (mmol/L) | 5.63 | 0.01 | 0.17 | 139.33 | 0.001 | 0.72 | 38.17 | 0.001 | 0.59 |
| LDL (mmol/L) | 1.97 | 0.15 | 0.07 | 173.77 | 0.001 | 0.77 | 26.66 | 0.001 | 0.49 |
| TG (mmol/L) | 7.37 | 0.01 | 0.21 | 464.25 | 0.001 | 0.89 | 35.41 | 0.001 | 0.57 |
| PG (mmol/L) | 4.54 | 0.02 | 0.14 | 98.08 | 0.001 | 0.65 | 20.65 | 0.001 | 0.43 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beqa Ahmeti, G.; Idrizovic, K.; Elezi, A.; Zenic, N.; Ostojic, L. Endurance Training vs. Circuit Resistance Training: Effects on Lipid Profile and Anthropometric/Body Composition Status in Healthy Young Adult Women. Int. J. Environ. Res. Public Health 2020, 17, 1222. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041222
Beqa Ahmeti G, Idrizovic K, Elezi A, Zenic N, Ostojic L. Endurance Training vs. Circuit Resistance Training: Effects on Lipid Profile and Anthropometric/Body Composition Status in Healthy Young Adult Women. International Journal of Environmental Research and Public Health. 2020; 17(4):1222. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041222
Chicago/Turabian StyleBeqa Ahmeti, Gentiana, Kemal Idrizovic, Abdulla Elezi, Natasa Zenic, and Ljerka Ostojic. 2020. "Endurance Training vs. Circuit Resistance Training: Effects on Lipid Profile and Anthropometric/Body Composition Status in Healthy Young Adult Women" International Journal of Environmental Research and Public Health 17, no. 4: 1222. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041222