Experiences of the Built Environment, Falls and Fear of Falling Outdoors among Older Adults: An Exploratory Study and Future Directions


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Measures
2.3.1. Outcome Measures: Falls and Fear of Falling
2.3.2. Environmental Measures
2.3.3. Walking
2.3.4. Activities of Daily Living
2.3.5. Demographic
2.4. Data Collection
2.5. Ethical Approval
2.6. Study Area
2.7. Analyses
3. Results
3.1. Sample Characteristics
3.2. Falling
Location of Falls
- Fallen at home: 35%
- Fallen in the garden or driveway: 35%
- Fallen in the street: 30%
- Fallen elsewhere: 32%
3.3. Fear of Falling
4. Discussion
4.1. Limitations
4.2. Future Research Directions
- Is there a moderating effect of having experienced a fall on relationships between urban environments and fear of falling?
- What contribution do neighbourhood conditions to developing a fear of falling?
- How do neighbourhood conditions and individual risk factors interact to influence falling and fear of falling?
- How does the social and environmental context of falls influence outdoor falls?
- What is the relationship between the urban environment, outdoor mobility, falls and fear of falling in deprived areas, where neighbourhood conditions are likely to be poorer and rates of walking higher?
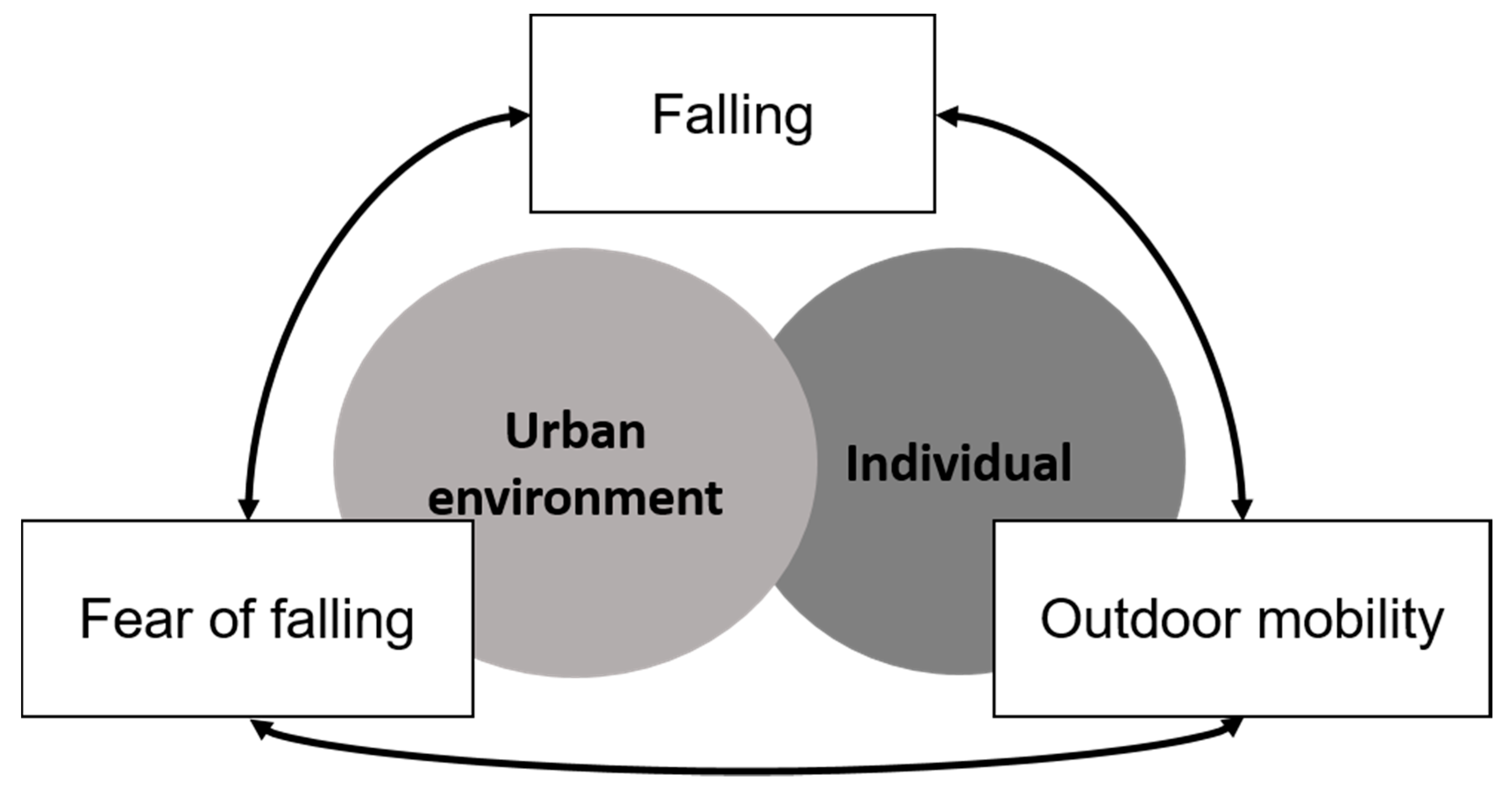
- Does new evidence support the conceptualisation of reciprocal and complex relationships between falling, fear of falling and outdoor mobility, and the contribution of urban environments and individual risk factors (Figure 1)
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Schwanen, T.; Ziegler, F. Wellbeing, independence and mobility: An introduction. Ageing Soc. 2011, 31, 719–733. [Google Scholar] [CrossRef] [Green Version]
- Gatrell, A.C. Therapeutic mobilities: Walking and ‘steps’ to wellbeing and health. Health Place 2013, 22, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Curl, A.; Clark, J. Health, Wellbeing and Quality of Life. In Transport Matters; Docherty, I., Shaw, J., Eds.; Policy Press: Bristol, UK, 2019. [Google Scholar]
- Lawton, M.P.; Nahemow, L. Ecology and the aging process. In The Psychology of Adult Development and Aging; Eisdorfer, C., Lawton, P.M., Eds.; American Psychological Association: Washington, DC, USA, 1973; pp. 619–674. [Google Scholar]
- Nordbakke, S.; Schwanen, T. Well-being and Mobility: A Theoretical Framework and Literature Review Focusing on Older People. Mobilities 2013, 9, 104–129. [Google Scholar] [CrossRef]
- Metz, D. Transport policy for an ageing population. Transp. Rev. 2003, 23, 375–386. [Google Scholar] [CrossRef]
- Bergland, A.; Thorsen, K.; Loland, N.W. The relationship between coping, self-esteem and health on outdoor walking ability among older adults in Norway. Ageing Soc. 2010, 30, 949–963. [Google Scholar] [CrossRef] [Green Version]
- Kerr, J.; Rosenberg, D.; Frank, L. The Role of the Built Environment in Healthy Aging: Community Design, Physical Activity, and Health among Older Adults. J. Plan. Lit. 2012, 27, 43–60. [Google Scholar] [CrossRef]
- Lee, S.; Lee, C.; Ory, G.M. Association between Recent Falls and Changes in Outdoor Environments near Community-Dwelling Older Adults’ Homes over Time: Findings from the NHATS Study. Int. J. Environ. Res. Public Health 2019, 16, 3230. [Google Scholar] [CrossRef] [Green Version]
- Skelton, D.; Todd, C. What Are the Main Risk Factors for Falls Amongst Older People and What Are the Most Effective Interventions to Prevent These Falls? WHO Regional Office for Europe Copenhagen: Copenhagen, Denmark, 2004. [Google Scholar]
- Kelsey, J.L.; Procter-Gray, E.; Hannan, M.T.; Li, W. Heterogeneity of falls among older adults: Implications for public health prevention. Am. J. Public Health 2012, 102, 2149–2156. [Google Scholar] [CrossRef]
- Li, W.; Procter-Gray, E.; Lipsitz, L.A.; Leveille, S.G.; Hackman, H.; Biondolillo, M.; Hannan, M.T. Utilitarian Walking, Neighborhood Environment, and Risk of Outdoor Falls Among Older Adults. Am. J. Public Health 2014, 104, e30–e37. [Google Scholar] [CrossRef]
- Li, W.; Keegan, T.H.; Sternfeld, B.; Sidney, S.; Quesenberry, C.P., Jr.; Kelsey, J.L. Outdoor falls among middle-aged and older adults: A neglected public health problem. Am. J. Public Health 2006, 96, 1192–1200. [Google Scholar] [CrossRef]
- Chippendale, T.; Boltz, M. Outdoor Fall Experiences: An Exploratory Study of Urban and Suburban Dwelling Older Adults. Phys. Occup. Ther. Geriatr. 2018, 36, 234–244. [Google Scholar] [CrossRef]
- Curl, A.; Thompson, C.W.; Aspinall, P.; Ormerod, M. Developing an audit checklist to assess outdoor falls risk. Proc. Inst. Civ. Eng. Urban Des. Plan. 2016, 169, 138–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chippendale, T.; Boltz, M. The neighborhood environment: Perceived fall risk, resources, and strategies for fall prevention. Gerontologist 2015, 55, 575–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyman, S.R.; Ballinger, C.; Phillips, J.E.; Newton, R. Characteristics of outdoor falls among older people: A qualitative study. BMC Geriatr. 2013, 13, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satariano, W.A.; Wang, C.; Kealey, M.E.; Kurtovich, E.; Phelan, E.A. Risk Profiles for Falls among Older Adults: New Directions for Prevention. Front. Public Health 2017, 5, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijlhuizen, G.J.; de Jong, R.; Hopman-Rock, M. Older persons afraid of falling reduce physical activity to prevent outdoor falls. Prev. Med. 2007, 44, 260–264. [Google Scholar] [CrossRef]
- Bath, P.A.; Morgan, K. Differential risk factor profiles for indoor and outdoor falls in older people living at home in Nottingham, UK. Eur. J. Epidemiol. 1999, 15, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Tinetti, M.E.; Powell, L. Fear of Falling and Low Self-efficacy: A Cause of Dependence in Elderly Persons. J. Gerontol. 1993, 48, 35–38. [Google Scholar] [CrossRef]
- Chippendale, T.; Lee, C.D. Characteristics and fall experiences of older adults with and without fear of falling outdoors. Aging Ment. Health 2018, 22, 849–855. [Google Scholar] [CrossRef]
- Lee, S.; Lee, C.; Rodiek, S. Outdoor exposure and perceived outdoor environments correlated to fear of outdoor falling among assisted living residents. Aging Ment. Health 2019. [Google Scholar] [CrossRef]
- Kempen, G.I.J.M.; van Haastregt, J.C.M.; McKee, K.J.; Delbaere, K.; Zijlstra, G.A.R. Socio-demographic, health-related and psychosocial correlates of fear of falling and avoidance of activity in community-living older persons who avoid activity due to fear of falling. BMC Public Health 2009, 9, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez-Jara, J.; Walker, D.; Heslop, P.; Robinson, S. Measuring fear of falling and its effect on quality of life and activity. Rev. Clin. Gerontol. 2010, 20, 277–287. [Google Scholar] [CrossRef]
- Smith, A.R.; Chen, C.; Clarke, P.; Gallagher, N.A. Trajectories of Outdoor Mobility in Vulnerable Community-Dwelling Elderly: The Role of Individual and Environmental Factors. J. Aging Health 2015, 28, 796–811. [Google Scholar] [CrossRef] [PubMed]
- Scheffer, A.C.; Schuurmans, M.J.; van Dijk, N.; van der Hooft, T.; de Rooij, S.E. Fear of falling: Measurement strategy, prevalence, risk factors and consequences among older persons. Age Ageing 2008, 37, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, M.; Ohyama, N.; Yamada, K.; Kanamori, M. The relationship between fear of falling, activities of daily living and quality of life among elderly individuals. Nurs. Health Sci. 2002, 4, 155–161. [Google Scholar] [CrossRef]
- Zijlstra, G.A.; van Haastregt, J.C.; van Eijk, J.T.; van Rossum, E.; Stalenhoef, P.A.; Kempen, G.I. Prevalence and correlates of fear of falling, and associated avoidance of activity in the general population of community-living older people. Age Ageing 2007, 36, 304–309. [Google Scholar] [CrossRef] [Green Version]
- Friedman, S.M.; Munoz, B.; West, S.K.; Rubin, G.S.; Fried, L.P. Falls and Fear of Falling: Which Comes First? A Longitudinal Prediction Model Suggests Strategies for Primary and Secondary Prevention. J. Am. Geriatr. Soc. 2002, 50, 1329–1335. [Google Scholar] [CrossRef]
- Koohsari, M.J.; Badland, H.; Giles-Corti, B. (Re)Designing the built environment to support physical activity: Bringing public health back into urban design and planning. Cities 2013, 35, 294–298. [Google Scholar] [CrossRef]
- Musselwhite, C.; Scott, T. Developing A Model of Mobility Capital for An Ageing Population. Int. J. Environ. Res. Public Health 2019, 16, 3327. [Google Scholar] [CrossRef] [Green Version]
- Franke, T.; Tong, C.; Ashe, M.C.; McKay, H.; Sims-Gould, J.; Team, T.W.T.T. The secrets of highly active older adults. J. Aging Stud. 2013, 27, 398–409. [Google Scholar] [CrossRef]
- Lee, S.; Lee, C.; Ory, M.G.; Won, J.; Towne, S.D.; Wang, S.; Forjuoh, S.N. Fear of Outdoor Falling among Community-Dwelling Middle-Aged and Older Adults: The Role of Neighborhood Environments. Gerontologist 2018, 58, 1065–1074. [Google Scholar] [CrossRef] [Green Version]
- Yardley, L.; Beyer, N.; Hauer, K.; Kempen, G.; Piot-Ziegler, C.; Todd, C. Development and initial validation of the Falls Efficacy Scale-International (FES-I). Age Ageing 2005, 34, 614–619. [Google Scholar] [CrossRef] [Green Version]
- Hill, K.D.; Schwarz, J.A.; Kalogeropoulos, A.J.; Gibson, S.J. Fear of falling revisited. Arch. Phys. Med. Rehabil. 1996, 77, 1025–1029. [Google Scholar] [CrossRef]
- Shrive, F.M.; Stuart, H.; Quan, H.; Ghali, W.A. Dealing with missing data in a multi-question depression scale: A comparison of imputation methods. BMC Med. Res. Methodol. 2006, 6, 57. [Google Scholar] [CrossRef] [Green Version]
- Lättman, K.; Olsson, L.E.; Friman, M. A new approach to accessibility—Examining perceived accessibility in contrast to objectively measured accessibility in daily travel. Res. Transp. Econ. 2018, 69, 501–511. [Google Scholar] [CrossRef]
- Hurtig-Wennlöf, A.; Hagströmer, M.; Olsson, L.A. The International Physical Activity Questionnaire modified for the elderly: Aspects of validity and feasibility. Public Health Nutr. 2010, 13, 1847–1854. [Google Scholar] [CrossRef]
- Curl, A.; Thompson, C.W.; Alves, S.; Aspinall, P. Outdoor Environmental Supportiveness and Older People’s Quality of Life: A Personal Projects Approach. J. Hous. Elder. 2016, 30, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Sugiyama, T.; Thompson, C.W. Older people’s health, outdoor activity and supportiveness of neighbourhood environments. Landsc. Urban Plan. 2007, 83, 168–175. [Google Scholar] [CrossRef]
- Statistics New Zealand. Census 2018. In Stats NZ and licensed by Stats NZ for re-use under the Creative Commons Attribution 4.0 International licence; Statistics New Zealand: Wellington, New Zealand, 2018. [Google Scholar]
- Annear, M.; Keeling, S.; Wilkinson, T. Participatory and evidence-based recommendations for urban redevelopment following natural disasters: Older adults as policy advisers. Australas. J. Ageing 2014, 33, 43–49. [Google Scholar] [CrossRef]
- Curl, A.; Mason, P. Neighbourhood perceptions and older adults’ wellbeing: Does walking explain the relationship in deprived urban communities? Transp. Res. Part A Policy Pract. 2019, 123, 119–129. [Google Scholar] [CrossRef] [Green Version]
- Rantakokko, M.; Manty, M.; Iwarsson, S.; Tormakangas, T.; Leinonen, R.; Heikkinen, E.; Rantanen, T. Fear of moving outdoors and development of outdoor walking difficulty in older people. J. Am. Geriatr. Soc. 2009, 57, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Duckham, R.L.; Procter-Gray, E.; Hannan, M.T.; Leveille, S.G.; Lipsitz, L.A.; Li, W. Sex differences in circumstances and consequences of outdoor and indoor falls in older adults in the MOBILIZE Boston cohort study. BMC Geriatr. 2013, 13, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NZ Injury Query System (NIQS). Injury Prevention Research Unit, Department of Preventive and Social Medicine, University of Otago, New Zealand. Available online: https://psm-dm.otago.ac.nz/niqs (accessed on 30 October 2019).
- Sasidharan, V.; Payne, L.; Orsega-Smith, E.; Godbey, G. Older adults’ physical activity participation and perceptions of wellbeing: Examining the role of social support for leisure. Manag. Leis. 2007, 11, 164–185. [Google Scholar] [CrossRef]
- Chippendale, T.; Raveis, V. Knowledge, behavioral practices, and experiences of outdoor fallers: Implications for prevention programs. Arch. Gerontol. Geriatr. 2017, 72, 19–24. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Total Sample n = 129 * (%) | Fallen n = 44 (%) | Fear of Falling n = 55 (%) |
|---|---|---|---|
| Gender: Female | 99 (81) | 77 | 93 |
| Age 50–59 | 17 (13) | 16 | 15 |
| Age 60–69 | 34 (26) | 34 | 26 |
| Age 70–79 | 62 (48) | 39 | 46 |
| Age 80+ | 16 (12) | 11 | 15 |
| Driver licence | 121 (95) | 96 | 93 |
| Lives alone | 38 (30) | 34 | 32 |
| Live with spouse/family | 88 (68) | 66 | 69 |
| Walking related PA: Low | 58 (50) | 55 | 54 |
| Walking related PA: Medium | 53 (46) | 38 | 42 |
| Walking related PA: High | 5 (4) | 7 | 4 |
| Sample: Mean (sd) | Fallen: Mean (sd) | Fear of Falling: Mean (sd) | |
| Age | 70.5 (7.9) | 70.1 (8.1) | 70.6 (8.1) |
| Activities of daily diving (scale) | 6.3 (3.5) | 8.1 (4.1) | 8.1 (3.9) |
| Perceived accessibility | 17.3 (3.5) | 16.1 (3.8) | 15.8 (3.9) |
| Minutes walked per week | 315 (295) | 336 (359) | 276 (295) |
| Neighbourhood conditions | 2.3 (1.1) | 2.6 (1.1) | 2.5 (1.2) |
| Fear of falling (scale) | 13.2 (61) | 15.0 (7.4) | - |
| Covariate | Fallen at Least Once (Unadjusted) OR (CI) | Fallen at Least Once (Adjusted for ADL and Gender) OR (CI) |
|---|---|---|
| Neighbourhood conditions | NR2 0.06 1.51 (1.06, 2.16) * | NR2 0.11 0.35 (0.98, 2.04) |
| Perceived accessibility | NR2 0.07 0.87 (0.78, 0.97)* | NR2 0.07 0.94 (0.80, 1.04) |
| Walking related PA (ref: Low) | NR2 0.03 | |
| Walking related PA: Medium | 0.66 (0.30, 1.15) | |
| Walking related PA: High | 2.28 (0.35, 14.74) | |
| Mins per week walking | NR2 0.004 1.00 (0.99, 1.002) | |
| Fear falling (ref: no fear) | NR2 0.03 1.81 (0.87, 3.79) | |
| Fear of falling scale | NR2 0.06 1.07 (1.01, 1.14) | |
| Age | NR2 0.02 0.99 (0.95, 1.04) | |
| Male (ref: female) | NR2 0.06 1.43 (0.57, 3.56) | |
| Live alone (ref: living with others) | NR2 0.01 1.37 (0.63, 3.01) | |
| Driver licence (ref: no licence) | NR2 0.001 1.33 (0.25, 7.15) | |
| Activities of daily living | NR2 0.07 1.15 (1.03, 1.29) * |
| Covariate | Fear of Falling (Unadjusted) OR (CI) | Fear of Falling (Adjusted for Falling, ADL and Gender) OR (CI) |
|---|---|---|
| Neighbourhood conditions | NR2 0.06 1.50 (1.06, 2.12) * | NR2 0.27 1.27 (0.87, 1.86) |
| Perceived accessibility (PAC) | NR2 0.18 0.79 (0.70, 0.89) ** | NR2 0.33 0.78 (0.66, 0.93) ** |
| Walking related PA (ref: Low) | NR2 0.07 | |
| Walking related PA: Medium | 0.75 (0.35, 1.59) | |
| Walking related PA: High | 0.82 (0.13, 5.28) | |
| Mins per week walking | NR2 0.02 0.99 (0.99, 1.00) | |
| Frequency of falling (ref: not fallen) | NR2 0.06 | |
| Fallen once | 1.1 (0.44, 2.75) | |
| Fallen more than once | 2.59 (1.24, 10.38) * | |
| Age | NR2 0.00 1.00 (0.96,1.05) | |
| Male (ref: female) | NR2 0.10 0.20 (0.06, 0.62) * | |
| Live alone (ref: living with others) | NR2 0.02 1.16 (0.54, 2.49) | |
| Driver licence (ref: no licence) | NR2 0.07 0.53 (0.11, 2.46) | |
| Activities of daily living (ADL) | NR2 0.11 1.21 (1.06, 1.38) * |
| Covariate | Fear of Falling Scale (Unadjusted) | Fear of Falling Scale (Adjusted for ADL, Falling and Gender) |
|---|---|---|
| Neighbourhood conditions | 2.10 (1.56, 3.05) ** R2 0.14 | 1.38 (0.54, 2.22) ** R2 0.41 |
| Perceived accessibility (PAC) | −0.81 (−1.08, −0.55) ** R2 0.23 | −0.55 (−0.85, −0.47) ** R2 0.41 |
| Walking related PA (ref: Low) | R2 0.03 | |
| Walking related PA: Medium | −1.96 (−4.42, 0.33) | |
| Walking related PA: High | −2.97 (−8.57, 2.63) | |
| Mins per week walking | −0.004 (−0.008, −0.001) R2 0.05 | |
| Fallen once | 0.51 (−2.10, 3.11) | |
| Fallen more than once | 5.53 (2.63, 8.43) ** R2 0.10 | |
| Age | 0.08 (−0.05, 0.21) R2 0.01 | |
| Male | −3.92 (−657, −1.26) ** R2 0.07 | |
| Live alone | 2.11 (−0.18, 4.41) R2 0.03 | |
| Driver licence | −1.78 (−6.46, 2.90) R2 0.04 | |
| Activities of daily living (ADL) | 0.81 (0.54, 1.09) ** R2 0.21 |
| Covariate | Fear of Falling Scale |
|---|---|
| Neighbourhood conditions | 1.15 (0.32, 1.99) ** |
| Perceived accessibility (PAC) | −0.47 (−0.78, −0.16) ** |
| Fallen once | −0.13 (−2.42, 2.15) |
| Fallen more than once | 2.98 (0.41, 5.55) * |
| Male | −4.12 (−6.44, −1.80) ** |
| Activities of daily living (ADL) | 0.51 (0.19, 0.83) ** |
| R2 0.42 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Curl, A.; Fitt, H.; Tomintz, M. Experiences of the Built Environment, Falls and Fear of Falling Outdoors among Older Adults: An Exploratory Study and Future Directions. Int. J. Environ. Res. Public Health 2020, 17, 1224. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041224
Curl A, Fitt H, Tomintz M. Experiences of the Built Environment, Falls and Fear of Falling Outdoors among Older Adults: An Exploratory Study and Future Directions. International Journal of Environmental Research and Public Health. 2020; 17(4):1224. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041224
Chicago/Turabian StyleCurl, Angela, Helen Fitt, and Melanie Tomintz. 2020. "Experiences of the Built Environment, Falls and Fear of Falling Outdoors among Older Adults: An Exploratory Study and Future Directions" International Journal of Environmental Research and Public Health 17, no. 4: 1224. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041224