Population Attributable Fraction of Early Age of Onset of Alcohol Use in Alcohol Abuse and Dependence: A 3-Year Follow-Up Study in University Students



Abstract
:1. Introduction
2. Materials and Methods
2.1. Design, Population and Sample
2.2. Data Collection Procedure
2.3. Definition of Variables
2.3.1. Dependent Variables
2.3.2. Independent Variables
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- World Health Organization. Global Status Report on Alcohol and Health; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Bryant, A.L.; Schulenberg, J.E.; O’Malley, P.M.; Bachman, J.G.; Johnston, L.D. How academic achievement, attitudes, and behaviors relate to the course substance use during adolescence:a 6-year, multiwave national longitudinal study. J. Res. Adolesc. 2003, 13, 361–397. [Google Scholar] [CrossRef]
- Staff, J.; Patrick, M.E.; Loken, E.; Maggs, J.L. Teenage alcohol use and educational attainment. J. Stud. Alcohol Drugs 2008, 69, 848–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caamaño-Isorna, F.; Mota, N.; Crego, A.; Corral, M.; Rodríguez, S.; Cadaveira, F. Consumption of medicines, alcohol, tobacco and cannabis among university students: A 2-year follow-up. Int. J. Public Health 2011, 56, 247–252. [Google Scholar] [CrossRef] [PubMed]
- McCabe, S.E.; Cranford, J.A.; Boyd, C.J. The relationship between past-year drinking behaviors and nonmedical use of prescription drugs: Prevalence of co-occurrence in a national sample. Drug Alcohol Depend. 2006, 84, 281–288. [Google Scholar] [CrossRef] [Green Version]
- McCabe, S.E.; Cranford, J.A.; Morales, M. Simultaneous and concurrent poly drug use of alcohol and prescription drugs: Prevalence, correlates, and consequences. J. Stud. Alcohol 2006, 67, 529–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caamaño-Isorna, F.; Moure-Rodríguez, L.; Doallo, S.; Corral, M.; Rodriguez, S.; Cadaveira, F. Heavy episodic drinking and alcohol-related injuries: An open cohort study among college students. Accid. Anal. Prev. 2017, 100, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Caamaño-Isorna, F.; Moure-Rodriguez, L.; Corral, M.; Cadaveira, F. Traffic accidents and heavy episodic drinking among university students. Traffic Inj. Prev. 2017, 18, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Carbia, C.; Cadaveira, F.; López-Caneda, E.; Caamano-Isorna, F.; Rodríguez, S.; Corral, M. Working memory over a six-year period in young binge drinkers. Alcohol 2017, 61, 17–23. [Google Scholar] [CrossRef] [Green Version]
- López-Caneda, E.; Rodríguez, S.; Corral, M.; Doallo, S.; Cadaveira, F. Evolution of the binge drinking pattern in college students: Neurophysiological correlates. Alcohol 2014, 48, 407–418. [Google Scholar] [CrossRef]
- López-Caneda, E.; Cadaveira, F.; Crego, A.; Doallo, S.; Corral, M.; Gómez-Suárez, A.; Rodríguez Holguín, S. Effects of a persistent binge drinking pattern of alcohol consumption in young people: A follow-up study using event-related potentials. Alcohol Alcohol. 2013, 48, 464–471. [Google Scholar] [CrossRef] [Green Version]
- Pickett, W.; Schmid, H.; Boyce, W.F.; Simpson, K.; Scheidt, P.C.; Mazur, J.; Molcho, M.; King, M.A.; Godeau, E.; Overpeck, M.; et al. Multiple risk behavior and injury: An international analysis of young people. Arch. Pediatr. Adolesc. Med. 2002, 156, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Karam, E.; Kypri, K.; Salamoun, M. Alcohol use among college students: An international perspective. Curr. Opin. Psychiatry 2007, 20, 213–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wicki, M.; Kuntsche, E.; Gmel, G. Drinking at European universities? A review of students’ alcohol use. Addict. Behav. 2010, 35, 913–924. [Google Scholar] [CrossRef] [PubMed]
- Kypri, K.; Cronin, M.; Wright, C.S. Do University students drink more hazardously than their non-student peers? Addiction 2005, 100, 713–714. [Google Scholar] [CrossRef] [PubMed]
- Bewick, B.M.; Mulhern, B.; Barkham, M.; Trusler, K.; Hill, A.J.; Stiles, W.B. Changes in undergraduate student alcohol consumption as they progress through university. BMC Public Health 2008, 8, 163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, A.C.; Brandon, K.O.; Goldman, M.S. The college and noncollege experience: A review of the factors that influence drinking behavior in young adulthood. J. Stud. Alcohol Drugs 2010, 71, 742–750. [Google Scholar] [CrossRef]
- Degenhardt, L.; O’Loughlin, C.; Swift, W.; Romaniuk, H.; Carlin, J.; Coffey, C.; Hall, W.; Patton, G. The persistence of adolescent binge drinking into adulthood: Findings from a 15-year prospective cohort study. BMJ Open 2013, 3, e003015. [Google Scholar] [CrossRef] [Green Version]
- Kramer, J.R.; Chan, G.; Dick, D.M.; Kuperman, S.; Bucholz, K.K.; Edenberg, H.J.; Polgreen, L.A.; Hesselbrock, V.M.; Schuckit, M.A.; Nurnberger, J.I.; et al. Multiple-domain predictors of problematic alcohol use in young adulthood. J. Stud. Alcohol Drugs 2008, 69, 649–659. [Google Scholar] [CrossRef] [Green Version]
- Gómez, P.; Moure-Rodríguez, L.; López-Caneda, E.; Rial, A.; Cadaveira, F.; Caamaño-Isorna, F. Patterns of Alcohol Consumption in Spanish University Alumni: Nine Years of Follow-Up. Front. Psychol. 2017, 15, 756. [Google Scholar] [CrossRef] [Green Version]
- Moure-Rodríguez, L.; Piñeiro, M.; Corral, M.; Rodríguez-Holguín, S.; Cadaveira, F.; Caamaño-Isorna, F. Identifying Predictors and Prevalence of Alcohol Consumption among University Students: Nine Years of Follow-Up. PLoS ONE 2016, 11, e0165514. [Google Scholar] [CrossRef]
- Merrill, J.E.; Carey, K.B. Drinking Over the Lifespan: Focus on College Ages. Alcohol Res. Curr. Rev. 2016, 38, 103–114. [Google Scholar]
- Chen, K.; Kandel, D.B. The natural history of drug use from adolescence to the mid-thirties in a general population sample. Am. J. Public Health 1995, 85, 41–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dantzer, C.; Wardle, J.; Fuller, R.; Pampalone, S.Z.; Steptoe, A. International Study of Heavy Drinking: Attitudes and Sociodemographic Factors in University Students. J. Am. Coll. Health 2006, 55, 83–89. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. The Surgeon General’s Call to Action To Prevent and Reduce Underage Drinking; U.S. Department of Health and Human Services, Office of the Surgeon General: Rockville, MD, USA, 2007.
- Knight, J.R.; Wechsler, H.; Kuo, M.; Seibrin, M.; Weitzman, E.R.; Schuckit, M.A. Alcohol abuse and dependence among U.S. college students. J. Stud. Alcohol 2002, 63, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Heather, N.; Partington, S.; Partington, E.; Longstaff, F.; Allsop, S.; Jankowski, M.; Wareham, H.; St Clair Gibson, A. Alcohol use disorders and hazardous drinking among undergraduates at English universities. Alcohol Alcohol. 2011, 46, 270–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caetano, R.; Babor, T.F. Diagnosis of alcohol dependence in epidemiological surveys: An epidemic of youthful alcohol dependence or a case of measurement error? Addiction 2006, 101, 111–114. [Google Scholar] [CrossRef]
- Dick, D.M.; Nasim, A.; Edwards, A.C.; Salvatore, J.E.; Cho, S.B.; Adkins, A.; Meyers, J.; Yan, J.; Cooke, M.; Clifford, J.; et al. Spit for Science: Launching a longitudinal study of genetic and environmental influences on substance use and emotional health at a large US university. Front. Genet. 2014, 5, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)-a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Bucholz, K.K.; Cadoret, R.; Cloninger, C.R.; Dinwiddie, S.H.; Hesselbrock, V.M.; Nurnberger, J.I., Jr.; Reich, T.; Schmidt, I.; Schuckit, M.A. A new, semi-structured psychiatric interview for use in genetic linkage studies: A report on the reliability of the SSAGA. J. Stud. Alcohol 1994, 55, 149–158. [Google Scholar] [CrossRef]
- Substance Abuse and Mental Health Services Administration. Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2013.
- Kendler, K.S.; Gardner, C.O.; Prescott, C.A. Religion, psychopathology, and substance use and abuse; a multimeasure, genetic-epidemiologic study. Am. J. Psychiatry 1997, 154, 322–329. [Google Scholar] [CrossRef]
- Dai, H. Trends in Single, Dual, and Poly Use of Alcohol, Cigarettes, and Marijuana Among US High-School Students: 1991–2017. Am. J. Public Health 2019, 109, 1138–1140. [Google Scholar] [CrossRef] [PubMed]
- Morgenstern, H.; Bursic, E.S. A method for using epidemiologic data to estimate the potential impact of an intervention on the health status of a target population. J. Community Health 1982, 7, 292–309. [Google Scholar] [CrossRef] [PubMed]
- Department of Mental Health and Substance Abuse. Alcohol, Gender and Drinking Problems: Perspectives from Low and Middle Income Countries; WHO: Geneva, Switzerland, 2005. [Google Scholar]
- Grant, B.F. Prevalence and correlates of alcohol use and DSM-IV alcohol dependence in the United States: Results of the National Longitudinal Alcohol Epidemiologic Survey. J. Stud. Alcohol 1997, 58, 464–473. [Google Scholar] [CrossRef] [PubMed]
- Davoren, M.P.; Demant, J.; Shiely, F.; Perry, I.J. Alcohol consumption among university students in Ireland and the United Kingdom from 2002 to 2014: A systematic review. BMC Public Health 2016, 16, 173. [Google Scholar] [CrossRef] [Green Version]
- Simons-Morton, B.G.; Farhat, T.; ter Bogt, T.F.; Hublet, A.; Kuntsche, E.; Nic Gabhainn, S.; Godeau, E.; Kokkevi, A. Gender specific trends in alcohol use: Cross-cultural comparisons from 1998 to 2006 in 24 countries and regions. Int. J. Public Healt 2009, 54, 199–208. [Google Scholar] [CrossRef] [Green Version]
- Piazza, N.J.; Vrbka, J.L.; Yeager, R.D. Telescoping of alcoholism in women alcoholics. Int. J. Addict. 1989, 24, 19–28. [Google Scholar] [CrossRef]
- Greenfield, S.F.; Back, S.E.; Lawson, K.; Brady, K.T. Substance Abuse in Women. Psychiatr. Clin. N. Am. 2010, 33, 339–355. [Google Scholar] [CrossRef]
- Seedat, S.; Scott, K.M.; Angermeyer, M.C.; Berglund, P.; Bromet, E.J.; Brugha, T.S.; Demyttenaere, K.; de Girolamo, G.; Haro, J.M.; Jin, R.; et al. Cross-national associations between gender and mental disorders in the World Health Organization World Mental Health Surveys. Arch. Gen. Psychiatry 2009, 66, 785–795. [Google Scholar] [CrossRef]
- Andersson, C.; Johnsson, K.O.; Berglund, M.; Ojehagen, A. Alcohol involvement in Swedish University freshmen related to gender, age, serious relationship and family history of alcohol problems. Alcohol Alcohol. 2007, 42, 448–455. [Google Scholar] [CrossRef] [Green Version]
- Dawson, D.A.; Grant, B.F.; Stinson, F.S.; Chou, P.S. Another look at heavy episodic drinking and alcohol use disorders among college and non college youth. J. Stud. Alcohol 2004, 65, 477–488. [Google Scholar] [CrossRef]
- Esser, M.B.; Hedden, S.L.; Kanny, D.; Brewer, R.D.; Gfroerer, J.C.; Naimi, T.S. Prevalence of alcohol dependence among US adult drinkers, 2009–2011. Prev. Chronic. Dis. 2014, 11, E206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harford, T.C.; Grant, B.F.; Yi, H.Y.; Chen, C.M. Patterns of DSM-IV alcohol abuse and dependence criteria among adolescents and adults: Results from the 2001 National Household Survey on Drug Abuse. Alcohol Clin. Exp. Res. 2005, 29, 810–828. [Google Scholar] [CrossRef] [PubMed]
- Babor, T.F. We shape our tools, and thereafter our tools shape us: Psychiatric epidemiology and the alcohol dependence syndrome concept. Addiction 2007, 102, 1534–1535. [Google Scholar] [CrossRef] [PubMed]
- Atwell, K.; Abraham, C.; Duka, T. A parsimonious, integrative model of key psychological correlates of UK university students’ alcohol consumption. Alcohol Alcohol. 2011, 46, 253–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawson, D.A.; Goldstein, R.B.; Chou, S.P.; Ruan, W.J.; Grant, B.F. Age at First Drink and the First Incidence of Adult-Onset DSM-IV Alcohol Use Disorders. Alcohol Clin. Exp. Res. 2008, 32, 2149–2160. [Google Scholar] [CrossRef]
- Grant, B.F.; Dawson, D.A. Age at onset of alcohol use and its association with DSM-IV alcohol abuse and dependence: Results from the National Longitudinal Alcohol Epidemiologic Survey. J. Subst. Abuse 1997, 9, 103–110. [Google Scholar] [CrossRef]
- Donovan, J.E. Adolescent alcohol initiation: A review of psychosocial risk factors. J. Adolesc Health 2004, 35, 529-e7. [Google Scholar] [CrossRef]
- Fergusson, D.M.; Lynskey, M.T.; Horwood, L.J. Childhood exposure to alcohol and adolescent drinking patterns. Addiction 1994, 89, 1007–1016. [Google Scholar] [CrossRef]
- National Institute on Alcohol Abuse and Alcoholism. High-Risk Drinking in k Drinking in k Drinking in College: What We Know and What We Need To Learn. Final Report of the Panel on Contexts and Consequences; National Institute on Alcohol Abuse and Alcoholism: Rockville, MD, USA, 2002.
- Skidmore, J.R.; Murphy, J.G.; Martens, M.; Dennhardt, A.A. Alcohol-related consequences in African American and European American college students. J. Ethn. Subst. Abuse 2012, 11, 174–191. [Google Scholar] [CrossRef]
- Delva, J.; Smith, M.; Howell, R.; Harrison, D.; Wilke, D.; Jackson, D. A study of the relationship between protective behaviors and drinking consequences among undergraduate college students. J. Am. Coll. Health 2004, 53, 19–26. [Google Scholar] [CrossRef]
- Clarke, N.; Kim, S.Y.; White, H.R.; Jiao, Y.; Mun, E.Y. Associations Between Alcohol Use and Alcohol-Related Negative Consequences Among Black and White College Men and Women. J. Stud. Alcohol Drugs 2013, 74, 521–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wechsler, H.; Lee, J.E.; Nelson, T.F.; Kuo, M. Underage college students drinking behavior, access to alcohol and the influence of deterrence policies. Findings from the Harvard School of Public HealthCollege Alcohol Study. J. Am. Coll. Health 2002, 50, 223–236. [Google Scholar] [CrossRef] [PubMed]
- Weitzman, E.R.; Chen, Y.Y.; Subramanian, S.V. Youth smoking risk and community patterns of alcohol availability and control: A national multilevel study. J. Epidemiol. Community Health 2005, 59, 1065–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter, M.; Leppin, A.; Gabhainn, S.N. The relationship between parental socio-economic status and episodes of drunkenness among adolescents: Findings from a cross-national survey. BMC Public Health 2006, 6, 289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LGBT Foundation. The Lesbian, Gay, Bisexual and Trans Public Health Outcomes Framework Companion Document. 2016. Available online: https://www.london.gov.uk/sites/default/files/LGBT%20Public%20Health%20Outcomes%20Framework%20Companion%20Doc.pdf (accessed on 12 July 2019).
- Gonzales, G.; Przedworski, J.; Henning-Smith, C. Comparison of Health and Health Risk Factors Between Lesbian, Gay, and Bisexual Adults and Heterosexual Adults in the United States: Results From the National Health Interview Survey. JAMA Intern. Med. 2016, 176, 1344–1351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drabble, L.A.; Trocki, K.F.; Korcha, R.A.; Klinger, J.L.; Veldhuis, C.B.; Hughes, T.L. Comparing substance use and mental health outcomes among sexual minority and heterosexual women in probability and non-probability samples. Drug Alcohol Depend. 2018, 185, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Drabble, L.; Trocki, K. Alcohol Consumption, Alcohol-Related Problems, and Other Substance Use Among Lesbian and Bisexual Women. J. Lesbian Stud. 2005, 9, 19–30. [Google Scholar] [CrossRef]
- Lyons, A. Resilience in lesbians and gay men: A review and key findings from a nationwide Australian survey. Int. Rev. Psychiatry 2015, 27, 435–443. [Google Scholar] [CrossRef]
- Snipes, D.J.; Jeffers, A.J.; Benotsch, E.G.; McCauley, J.; Bannerman, D.; Granger, C.; Martin, A.M. Religiosity in the non-medical use of prescription medication in college students. Am. J. Drug Alcohol Abuse 2015, 41, 93–99. [Google Scholar] [CrossRef]
- Suerken, C.K.; Reboussin, B.A.; Sutfin, E.L.; Wagoner, K.G.; Spangler, J.; Wolfson, M. Prevalence of marijuana use at college entry and risk factors for initiation during freshman year. Addict. Behav. 2014, 39, 302–307. [Google Scholar] [CrossRef] [Green Version]
- Thompson, W.E. Social Support, Religious Involvement and Alcohol Use among Students at a Conservative Religious University. Behav. Sci. 2017, 7, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothman, K.J.; Greenland, S. Types of epidemiology study. In Modern Epidemiology, 2nd Ed.; Rothman, K.J., Greenland, S., Eds.; Lippincott and Raven: Philadelphia, PA, USA, 1988; pp. 74–75. [Google Scholar]
- Drabble, L.; Trocki, K.; Salcedo, B.; Morales, B.R.; Korcha, R.A. Strengths and coping strategies in the life narratives of sexual minority women. J. Gay Lesbian Soc. Serv. 2018, 30, 409–429. [Google Scholar] [CrossRef] [PubMed]
- De Lira, A.N.; de Morais, N.A. Resilience in Lesbian, Gay, and Bisexual (LGB) populations: An integrative literature review. Sex. Res. Soc. Policy 2018, 15, 272–282. [Google Scholar] [CrossRef]


{kind=link}
| Proportion of Subjects (%) | |||||
|---|---|---|---|---|---|
| Characteristics | Initial n = 3113 | 1-Year Follow-up n = 1667 | 2-Year Follow-up n = 1315 | 3-Year Follow-up n = 1112 | p-Value |
| Diagnostic and Statistical Manual of Mental Disorders, 4th Edition | |||||
| Non- abuse and non-dependence | 78.8 | 81.8 | 80.6 | 81.2 | |
| Abuse | 14.1 | 12.5 | 13.9 | 12.8 | |
| Dependence | 7.1 | 5.7 | 5.5 | 6.0 | 0.394 |
| Age of onset of alcohol use | |||||
| Older than 18 years | 19.9 | 27.1 | 31.5 | 32.2 | |
| 18 years | 29.3 | 30.6 | 27.5 | 27.6 | |
| 17 years | 21.1 | 18.2 | 17.2 | 16.1 | |
| 16 years | 16.2 | 14.2 | 13.5 | 13.0 | |
| Younger than 16 years | 13.5 | 9.9 | 10.4 | 11.1 | <0.001 |
| Cannabis consumption | |||||
| No | 66.0 | 67.5 | 69.1 | 69.6 | |
| Yes | 34.0 | 32.5 | 30.9 | 30.4 | 0.105/0.010 (lineal association) |
| Sexual orientation | |||||
| Heterosexual | 89.7 | 90.2 | 90.6 | 90.3 | |
| Homosexual | 2.1 | 2.1 | 1.9 | 1.6 | |
| Bisexual | 8.2 | 7.6 | 7.6 | 8.1 | 0.915 |
| Ethnicity | |||||
| White | 48.9 | 43.7 | 42.7 | 42.5 | |
| Asian | 15.2 | 18.5 | 20.2 | 20.6 | |
| Black | 22.8 | 25.2 | 25.2 | 25.0 | |
| Hispanic | 5.9 | 5.1 | 5.6 | 5.9 | |
| More than one race | 6.7 | 7.0 | 6.7 | 6.0 | <0.001 |
| Residence | |||||
| Parental home | 6.3 | 6.1 | 6.5 | 7.0 | |
| Residence hall | 88.6 | 89.7 | 88.9 | 88.6 | |
| Off-campus housing | 5.2 | 4.2 | 3.9 | 4.4 | 0.580 |
| Work status | |||||
| Currently not working | 72.9 | 73.8 | 74.7 | 74.1 | |
| Part-time | 24.4 | 23.1 | 22.0 | 22.4 | |
| Full-time | 2.7 | 3.1 | 3.3 | 3.5 | 0.628 |
| Percentage of Subjects (%) | |||||
|---|---|---|---|---|---|
| Characteristics | Initial n = 2057 | 1-Year Follow-up n = 883 | 2-Year Follow-up n = 644 | 3-Year Follow-up n = 540 | p-Value |
| Diagnosis of alcohol disorder according to DSM-IV | |||||
| Non- abuse and non- dependence | 74.6 | 75.5 | 76.9 | 73.3 | |
| Abuse | 17.7 | 16.6 | 15.8 | 19.1 | |
| Dependence | 7.8 | 7.6 | 7.3 | 7.6 | 0.913 |
| Age of onset of alcohol use | |||||
| Older than 18 years | 16.5 | 23.0 | 26.5 | 27.1 | |
| 18 years | 32.8 | 32.4 | 30.4 | 32.6 | |
| 17 years | 22.2 | 20.5 | 19.9 | 19.1 | |
| 16 years | 14.6 | 11.4 | 11.3 | 11.0 | |
| Younger than 16 years | 14.0 | 12.7 | 11.9 | 10.2 | <0.001 |
| Cannabis consumption | |||||
| No | 56.9 | 57.7 | 60.7 | 62.9 | |
| Yes | 43.1 | 42.3 | 39.3 | 37.1 | 0.087/0.012 (linear association) |
| Sexual orientation | |||||
| Heterosexual | 89.8 | 90.5 | 88.8 | 90.2 | |
| Homosexual | 7.1 | 6.7 | 7.8 | 6.2 | |
| Bisexual | 3.0 | 2.8 | 3.3 | 3.6 | 0.902 |
| Ethnicity | |||||
| White | 55.7 | 54.7 | 53.0 | 52.0 | |
| Asian | 17.7 | 20.9 | 21.8 | 21.8 | |
| Black | 14.9 | 14.6 | 16.7 | 16.3 | |
| Hispanic | 6.8 | 6.2 | 5.6 | 6.3 | |
| More than one race | 5.0 | 3.5 | 2.9 | 3.6 | 0.110 |
| Residence | |||||
| Parental home | 7.1 | 7.1 | 5.7 | 6.4 | |
| Residence hall | 85.8 | 88.4 | 89.2 | 88.1 | |
| Off-campus housing | 7.1 | 4.6 | 5.1 | 5.5 | 0.171 |
| Work status | |||||
| Currently not working | 76.7 | 75.6 | 76.5 | 74.9 | |
| Part-time | 21.3 | 22.7 | 22.6 | 24.2 | |
| Full-time | 2.0 | 1.7 | 1.0 | 0.9 | 0.418 |
| Proportion of Subjects (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Alcohol Abuse (DSM-IV) | Alcohol Dependence (DSM-IV) | |||||||||
| Period | Period | |||||||||
| Participants Characteristics | First Year, Fall | First Year, Spring | Second Year, Spring | Third Year, Spring | Fourth Year, Spring | First Year, Fall | First Year, Spring | Second year, SPRING | Third Year, Spring | Fourth Year, Spring |
| Age of onset of alcohol use | ||||||||||
| Older than 18 years | 3.3 | 3.9 | 3.1 | 4.9 | 5.0 | 1.1 | 0.6 | 1.5 | 1.0 | 1.3 |
| 18 years | 7.2 | 7.1 | 11.0 | 10.2 | 16.0 | 2.5 | 2.5 | 3.3 | 3.3 | 4.9 |
| 17 years | 13.5 | 14.9 | 18.0 | 19.8 | 21.8 | 5.6 | 5.5 | 5.7 | 8.3 | 5.8 |
| 16 years | 29.5 | 28.4 | 28.6 | 31.4 | 22.6 | 11.8 | 6.7 | 9.7 | 7.2 | 6.5 |
| Younger than 16 years | 46.4* | 36.6* | 31.5* | 35.1* | 46.7* | 18.7* | 11.0* | 13.8* | 8.8* | 17.1* |
| Ethnicity | ||||||||||
| White | 29.9 | 18.6 | 19.0 | 19.6 | 23.0 | 9.2 | 4.7 | 6.6 | 4.9 | 7.5 |
| Asian | 12.7 | 10.9 | 11.7 | 11.3 | 9.1 | 8.1 | 5.2 | 6.7 | 4.3 | 3.4 |
| Black | 8.3 | 11.1 | 7.5 | 11.5 | 12.5 | 6.1 | 5.0 | 3.1 | 2.6 | 2.9 |
| Hispanic | 11.4 | 15.3 | 20.8 | 13.6 | 18.6 | 5.5 | 3.5 | 3.9 | 6.8 | 3.4 |
| More than one race | 19.8* | 20.9* | 17.3* | 14.5^ | 13.3* | 4.1 | 5.5 | 5.4 | 9.2 | 5.0 |
| Sexual orientation | ||||||||||
| Heterosexual | 17.5 | 13.6 | 14.1 | 14.7 | 15.8 | 6.9 | 4.2 | 4.8 | 4.2 | 4.9 |
| Homosexual | 16.7 | 12.0 | 35.5 | 35.0 | 23.5 | 5.3 | 0 | 9.7 | 5.0 | 5.9 |
| Bisexual | 20.6 | 18.9 | 17.9* | 18.5^ | 26.8 | 9.7 | 5.3 | 8.5 | 6.5 | 8.5 |
| Residence | ||||||||||
| Parental home | 17.5 | 11.6 | 7.4 | 5.9 | 18.9 | 0.0 | 1.4 | 2.1 | 2.0 | 4.2 |
| Residence hall | 17.9 | 15.9 | 9.6 | 8.5 | 9.8 | 9.4 | 4.9 | 2.9 | 2.4 | 2.8 |
| Off-campus housing | 28.9 | 20.7 | 20.5* | 20.2* | 19.1^ | 16.7^ | 5.2 | 7.7 | 5.9^ | 6.2 |
| Work status | ||||||||||
| Currently not working | 17.7 | 15.6 | 14.1 | 17.6 | 17.8 | 8.7 | 4.8 | 4.8 | 6.4 | 8.0 |
| Part-time | 21.6 | 15.4 | 14.5 | 13.4 | 15.6 | 10.4 | 4.6 | 5.3 | 2.9 | 3.9 |
| Full-time | 9.5 | 31.8 | 37.8* | 26.4^ | 26.9 | 13.0 | 4.5 | 16.2^ | 11.3^ | 7.5 |
| Total | 18.4 | 15.8 | 15.0 | 15.4 | 17.0 | 7.8 | 4.7 | 5.3 | 4.5 | 5.3 |
| Proportion of Subjects (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Alcohol Abuse (DSM-IV) | Alcohol Dependence (DSM-IV) | |||||||||
| Period | Period | |||||||||
| Participants Characteristics | First Year, Fall | First Year, Spring | Second Year, Spring | Third Year, Spring | Fourth Year, Spring | First Year, Fall | First Year, Spring | Second Year, Spring | Third Year, Spring | Fourth Year, Spring |
| Age of onset of alcohol use | ||||||||||
| Older than 18 years | 9.7 | 8.3 | 7.1 | 5.1 | 8.1 | 6.3 | 2.1 | 2.4 | 4.3 | 3.3 |
| 18 years | 7.1 | 16.5 | 14.1 | 20.2 | 22.5 | 3.3 | 4.5 | 6.2 | 7.5 | 11.9 |
| 17 years | 23.8 | 22.8 | 27.2 | 29.7 | 34.1 | 3.3 | 6.1 | 9.5 | 8.1 | 15.9 |
| 16 years | 35.4 | 33.0 | 34.6 | 34.9 | 34.6 | 11.2 | 12.2 | 16.0 | 17.5 | 23.1 |
| Younger than 16 years | 44.5* | 39.2* | 41.7* | 28.6* | 21.7* | 19.2* | 13.7* | 11.9* | 18.8* | 10.9* |
| Ethnicity | ||||||||||
| White | 24.6 | 24.1 | 24.9 | 26.5 | 25.3 | 7.5 | 7.2 | 9.0 | 10.8 | 12.3 |
| Asian | 12.3 | 12.1 | 15.7 | 10.7 | 14.3 | 4.3 | 5.6 | 6.1 | 5.4 | 4.8 |
| Black | 12.3 | 20.0 | 10.5 | 10.2 | 20.8 | 7.7 | 2.7 | 6.3 | 5.7 | 16.7 |
| Hispanic | 16.2 | 19.6 | 19.0 | 10.0 | 17.2 | 7.1 | 12.5 | 7.1 | 12.9 | 13.8 |
| More than one race | 10.5 * | 25.7 | 11.5* | 50.0* | 22.2 | 9.4 | 2.9 | 7.7 | 18.8 | 11.1 |
| Sexual orientation | ||||||||||
| Heterosexual | 19.3 | 19.3 | 19.8 | 19.1 | 22.5 | 5.7 | 6.5 | 8.2 | 9.4 | 11.5 |
| Homosexual | 17.6 | 7.9 | 24.0 | 27.7 | 13.3 | 2.9 | 0.0 | 6.0 | 6.4 | 6.7 |
| Bisexual | 14.3 | 27.8 | 23.8 | 25.0 | 23.5 | 0.0 | 16.7 | 0.0 | 10.0 | 11.8 |
| Residence | ||||||||||
| Parental home | 15.4 | 18.4 | 13.5 | 5.1 | 11.8 | 11.1 | 2.6 | 7.7 | 7.7 | 8.8 |
| Residence hall | 21.2 | 20.7 | 12.7 | 9.6 | 15.4 | 7.6 | 6.4 | 4.4 | 5.2 | 5.8 |
| Off-campus housing | 36.7^ | 31.2 | 24.7* | 24.6* | 23.7^ | 20.6^ | 10.4 | 9.4 | 10.2 | 12.4 |
| Work status | ||||||||||
| Currently not working | 22.9 | 21.9 | 19.0 | 19.1 | 23.2 | 8.9 | 6.6 | 7.4 | 7.6 | 11.6 |
| Part-time | 19.6 | 20.0 | 23.7 | 21.3 | 19.8 | 7.1 | 5.7 | 7.8 | 11.0 | 11.5 |
| Full-time | 21.4 | 40.0 | 23.5 | 26.3 | 31.8 | 0.0 | 30.0^ | 11.8 | 10.5 | 9.1 |
| Total | 20.6 | 21.5 | 20.5 | 20.2 | 21.9 | 7.1 | 6.6 | 7.7 | 9.1 | 11.3 |
| Odds Ratio (95% Confidence Interval) | ||||
|---|---|---|---|---|
| Females | Males | |||
| Predictors | Alcohol Abuse | Alcohol Dependence | Alcohol Abuse | Alcohol Dependence |
| Age of onset of alcohol use | ||||
| Older than 18 years | 1 | 1 | 1 | 1 |
| 18 years | 3.01 (2.00–4.06) | 2.83 (1.39–5.76) | 2.24 (1.53–3.27) | 1.83 (1.07–3.14) |
| 17 years | 5.33 (3.44–7.05) | 5.66 (2.80–11.43) | 4.15 (2.84–6.06) | 2.40 (1.38–4.19) |
| 16 years | 10.19 (6.85–13.92) | 7.95 (3.96–15.99) | 6.62 (4.46–9.84) | 5.57 (3.21–9.66) |
| Younger than 16 years | 14.98 (9.53–19.92) | 11.83 (5.89–23.78) | 7.41 (4.95–11.10) | 6.24 (3.58–10.88) |
| Residence | ||||
| Parental home | 1 | 1 | ||
| Residence hall | 0.96 (0.64– 1.44) | 1.56 (0.67– 3.65) | ||
| Off-campus housing | 1.73 (1.16–2.56) | 2.76 (1.19–6.40) | ||
| Ethnicity | ||||
| Black/African American | 1 | 1 | 1 | 1 |
| Asian | 1.18 (0.85–1.65) | 1.24 (0.91–1.70) | 0.84 (0.57–1.24) | 0.68 (0.40–1.15) |
| Hispanic | 1.22(0.81–1.84) | 1.16 (0.78–1.72) | 0.90 (0.57–1.42) | 1.30 (0.73–2.29) |
| White | 1.58 (1.23–2.02) | 1.51 (1.19–2.91) | 1.50 (1.11–2.03) | 1.02 (0.68–1.52) |
| More than one race | 1.73 (1.19–2.51) | 1.73 (1.21–2.48) | 1.35 (0.81–2.24) | 1.19 (0.61–2.34) |
| Sexual orientation | ||||
| Heterosexual | 1 | |||
| Homosexual | 2.09 (1.21–3.58) | |||
| Bisexual | 1.28 (0.97–1.69) | |||
| Religiosity | ||||
| Tercile 1 (Low) | 1 | 1 | ||
| Tercile 2 (Medium) | 0.80 (0.65–0.96) | 0.90 (0.68–1.19) | ||
| Tercile 3 (High) | 0.58 (0.43–0.78) | 0.76 (0.50–1.14) | ||
| Work status | ||||
| Currently not working | 1 | 1 | ||
| Part-time | 0.87 (0.72–1.04) | 0.68 (0.50–0.92) | ||
| Full-time | 1.69 (1.14–2.52) | 1.78 (1.00–3.16) | ||
| Period | ||||
| First year, fall | 1 | 1 | 1 | 1 |
| First year, spring | 0.92 (0.68–1.24) | 0.44 (0.28–0.70) | 1.22 (0.95–1.54) | 0.89 (0.71–1.31) |
| Second year, spring | 0.80 (0.58–1.10) | 0.44 (0.27–0.74) | 1.24 (0.95–1.62) | 1.16 (0.78–1.72) |
| Third year, spring | 0.85 (0.60–1.20) | 0.39 (0.23–0.67) | 1.36 (1.02–1.80) | 1.43 (0.95–2.16) |
| Fourth year, spring | 0.96 (0.67–1.39) | 0.46 (0.26–0.82) | 1.54 (1.13–2.11) | 1.98 (1.33– 2.95) |
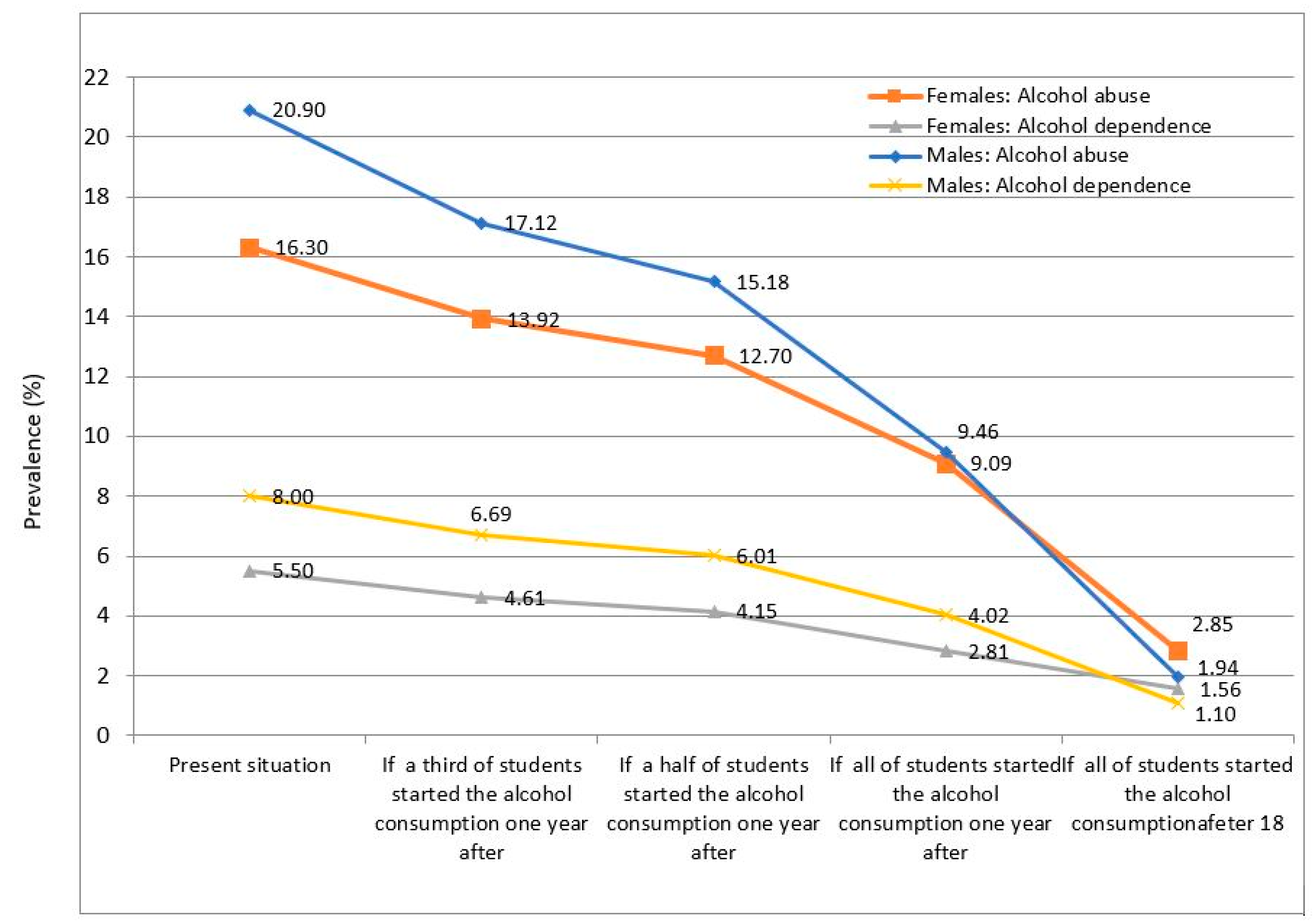
| Proportion (%) of alcohol abuse removed if… | Proportion (%) of alcohol dependence removed if… | |||||||
| …one third started alcohol use one year later | …one half started alcohol use one year later | …all students started alcohol use one year later | …all students started e alcohol use after age 18 years | …one third started alcohol use one year later | …one half started alcohol use one year later | …all students started alcohol use one year later | …all students started alcohol use after age 18 years | |
| Females | 14.59 | 22.11 | 44.21 | 80.9 | 16.15 | 24.46 | 48.93 | 71.7 |
| Males | 18.06 | 27.37 | 54.74 | 71.0 | 16.40 | 24.85 | 49.69 | 63.5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caamano-Isorna, F.; Adkins, A.; Aliev, F.; Moure-Rodríguez, L.; Dick, D.M. Population Attributable Fraction of Early Age of Onset of Alcohol Use in Alcohol Abuse and Dependence: A 3-Year Follow-Up Study in University Students. Int. J. Environ. Res. Public Health 2020, 17, 2159. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062159
Caamano-Isorna F, Adkins A, Aliev F, Moure-Rodríguez L, Dick DM. Population Attributable Fraction of Early Age of Onset of Alcohol Use in Alcohol Abuse and Dependence: A 3-Year Follow-Up Study in University Students. International Journal of Environmental Research and Public Health. 2020; 17(6):2159. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062159
Chicago/Turabian StyleCaamano-Isorna, Francisco, Amy Adkins, Fazil Aliev, Lucía Moure-Rodríguez, and Danielle M. Dick. 2020. "Population Attributable Fraction of Early Age of Onset of Alcohol Use in Alcohol Abuse and Dependence: A 3-Year Follow-Up Study in University Students" International Journal of Environmental Research and Public Health 17, no. 6: 2159. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062159