Urinary Arsenic Species are Detectable in Urban Underserved Hispanic/Latino Populations: A Pilot Study from the Study of Latinos: Nutrition & Physical Activity Assessment Study (SOLNAS)

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Laboratory Analyses
2.2. Statistical Analyses
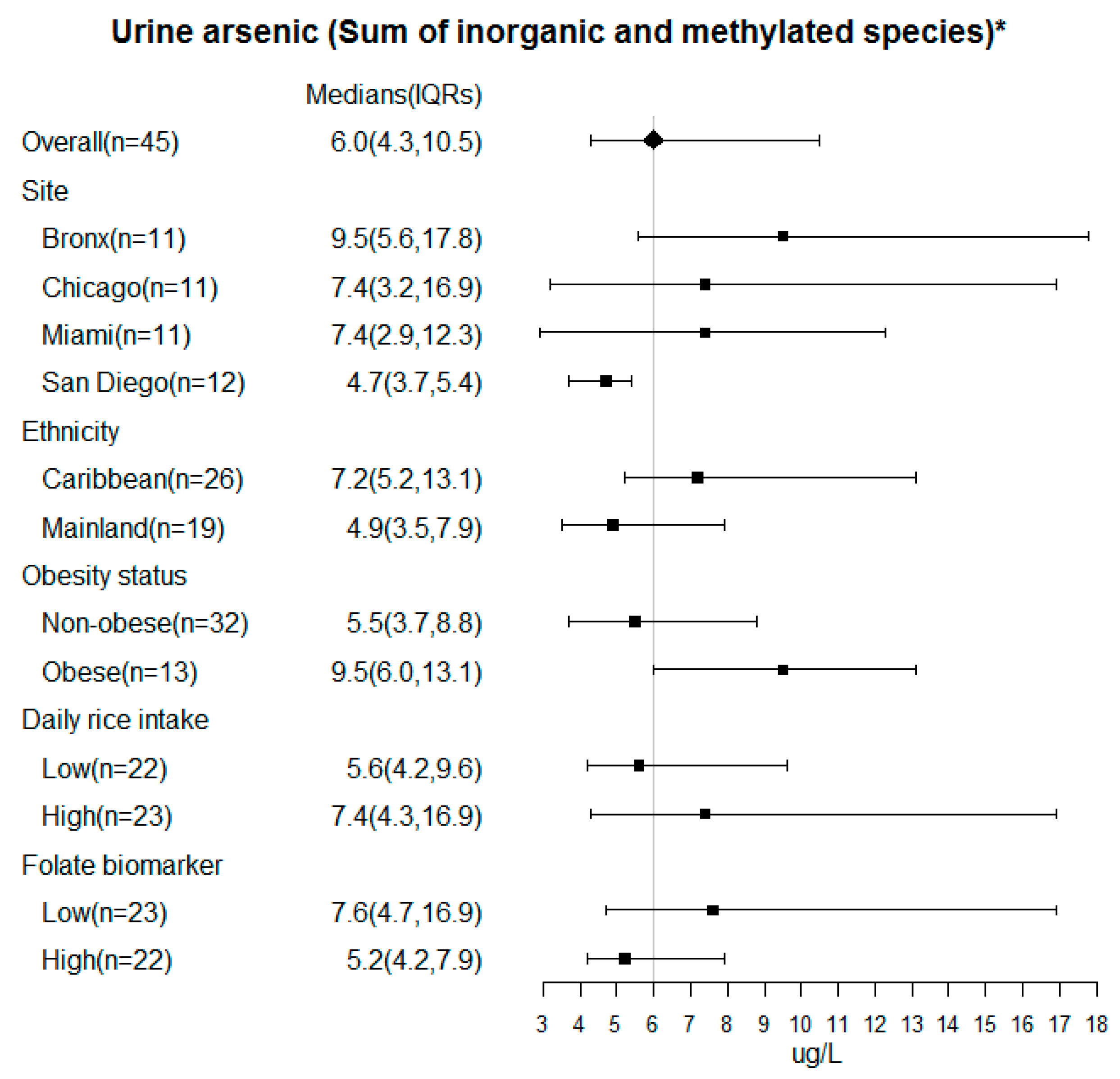
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Kuo, C.C.; Moon, K.A.; Wang, S.L.; Silbergeld, E.; Navas-Acien, A. The Association of Arsenic Metabolism with Cancer, Cardiovascular Disease, and Diabetes: A Systematic Review of the Epidemiological Evidence. Environ. Health Perspect. 2017, 125, 087001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Arsenic, metals, fibres, and dusts. IARC Monogr. Eval. Carcinog. Risks Hum. 2012, 100 Pt C, 11–465. [Google Scholar]
- Micha, R.; Penalvo, J.L.; Cudhea, F.; Imamura, F.; Rehm, C.D.; Mozaffarian, D. Association Between Dietary Factors and Mortality From Heart Disease, Stroke, and Type 2 Diabetes in the United States. JAMA 2017, 317, 912–924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corsino, L.; Sotres-Alvarez, D.; Butera, N.M.; Siega-Riz, A.M.; Palacios, C.; Perez, C.M.; Albrecht, S.S.; Espinoza Giacinto, R.A.; Perera, M.J.; Horn, L.V.; et al. Association of the DASH dietary pattern with insulin resistance and diabetes in US Hispanic/Latino adults: Results from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). BMJ Open Diabetes Res. Care 2017, 5, e000402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, E.M.; Acevedo, J.; López, F.G.; Cortés, S.; Ferreccio, C.; Smith, A.H.; Steinmaus, C.M. Hypertension among adults exposed to drinking water arsenic in Northern Chile. Environ. Res. 2017, 153, 99–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, Y.; Marshall, G.; Ferreccio, C.; Steinmaus, C.; Selvin, S.; Liaw, J.; Bates, M.N.; Smith, A.H. Acute myocardial infarction mortality in comparison with lung and bladder cancer mortality in arsenic-exposed region II of Chile from 1950 to 2000. Am. J. Epidemiol. 2007, 166, 1381–1391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; de Ferranti, S.; Despres, J.P.; Fullerton, H.J.; Howard, V.J.; et al. Heart disease and stroke statistics--2015 update: A report from the American Heart Association. Circulation 2015, 131, e29–e322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geiss, L.S.; Wang, J.; Cheng, Y.J.; Thompson, T.J.; Barker, L.; Li, Y.; Albright, A.L.; Gregg, E.W. Prevalence and incidence trends for diagnosed diabetes among adults aged 20 to 79 years, United States, 1980–2012. JAMA 2014, 312, 1218–1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Castro, B.R.; Caldwell, K.L.; Jones, R.L.; Blount, B.C.; Pan, Y.; Ward, C.; Mortensen, M.E. Dietary sources of methylated arsenic species in urine of the United States population, NHANES 2003–2010. PLoS ONE 2014, 9, e108098. [Google Scholar] [CrossRef] [PubMed]
- Borak, J.; Hosgood, H.D. Seafood arsenic: Implications for human risk assessment. Regul. Toxicol. Pharmacol. 2007, 47, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Sams, R., 2nd; Wolf, D.C.; Ramasamy, S.; Ohanian, E.; Chen, J.; Lowit, A. Workshop overview: Arsenic research and risk assessment. Toxicol. Appl. Pharmacol. 2007, 222, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Taylor, V.; Goodale, B.; Raab, A.; Schwerdtle, T.; Reimer, K.; Conklin, S.; Karagas, M.R.; Francesconi, K.A. Human exposure to organic arsenic species from seafood. Sci. Total Environ. 2017, 580, 266–282. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.R.; Tellez-Plaza, M.; Vaidya, D.; Grau, M.; Francesconi, K.A.; Goessler, W.; Guallar, E.; Post, W.S.; Kaufman, J.D.; Navas-Acien, A. Estimation of Inorganic Arsenic Exposure in Populations With Frequent Seafood Intake: Evidence From MESA and NHANES. Am. J. Epidemiol. 2016, 184, 590–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, M.R.; Tellez-Plaza, M.; Vaidya, D.; Grau-Perez, M.; Post, W.S.; Kaufman, J.D.; Guallar, E.; Francesconi, K.A.; Goessler, W.; Nachman, K.E.; et al. Ethnic, geographic and dietary differences in arsenic exposure in the multi-Ethnic study of atherosclerosis (MESA). J. Expo. Sci. Environ. Epidemiol. 2018. [Google Scholar] [CrossRef]
- Lavange, L.M.; Kalsbeek, W.D.; Sorlie, P.D.; Aviles-Santa, L.M.; Kaplan, R.C.; Barnhart, J.; Liu, K.; Giachello, A.; Lee, D.J.; Ryan, J.; et al. Sample design and cohort selection in the Hispanic Community Health Study/Study of Latinos. Ann. Epidemiol. 2010, 20, 642–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mossavar-Rahmani, Y.; Shaw, P.A.; Wong, W.W.; Sotres-Alvarez, D.; Gellman, M.D.; Van Horn, L.; Stoutenberg, M.; Daviglus, M.L.; Wylie-Rosett, J.; Siega-Riz, A.M.; et al. Applying Recovery Biomarkers to Calibrate Self-Report Measures of Energy and Protein in the Hispanic Community Health Study/Study of Latinos. Am. J. Epidemiol. 2015, 181, 996–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheer, J.; Findenig, S.; Goessler, W.; Francesconi, K.A.; Howard, B.; Umans, J.G.; Pollak, J.; Tellez-Plaza, M.; Silbergeld, E.K.; Guallar, E.; et al. Arsenic species and selected metals in human urine: Validation of HPLC/ICPMS and ICPMS procedures for a long-Term population-Based epidemiological study. Anal. Methods 2012, 4, 406–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gamble, M.V.; Liu, X.; Slavkovich, V.; Pilsner, J.R.; Ilievski, V.; Factor-Litvak, P.; Levy, D.; Alam, S.; Islam, M.; Parvez, F.; et al. Folic acid supplementation lowers blood arsenic. Am. J. Clin. Nutr. 2007, 86, 1202–1209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, B.A.; Hall, M.N.; Liu, X.; Parvez, F.; Sanchez, T.R.; van Geen, A.; Mey, J.L.; Siddique, A.B.; Shahriar, H.; Uddin, M.N.; et al. Folic Acid and Creatine as Therapeutic Approaches to Lower Blood Arsenic: A Randomized Controlled Trial. Environ. Health Perspect. 2015, 123, 1294–1301. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristic | Women | Men | All |
|---|---|---|---|
| n = 22 | n = 23 | n = 45 | |
| Age (years), Median (IQR) | 45.0 (36.0, 57.5) | 45.0 (37.5, 50.0) | 45.0 (36.0, 51.0) |
| BMI (kg/m2), Median (IQR) | 28.6 (25.8, 29.8) | 27.4 (24.8, 30.8) | 28.3 (25.0, 30.4) |
| Center, n (%) | |||
| Bronx | 4 (18.2) | 7 (30.4) | 11 (24.4) |
| Chicago | 6 (27.3) | 5 (21.7) | 11 (24.4) |
| Miami | 4 (18.2) | 7 (30.4) | 11 (24.4) |
| San Diego | 8 (36.4) | 4 (17.4) | 12 (26.7) |
| Hispanic/Latino Background, n (%) | |||
| Central American | 2 (9.1) | 1 (4.3) | 3 (6.7) |
| Cuban | 4 (18.2) | 6 (26.1) | 10 (22.2) |
| Dominican | 2 (9.1) | 2 (8.7) | 4 (8.9) |
| Mexican | 8 (36.4) | 6 (26.1) | 14 (31.1) |
| Puerto Rican | 5 (22.7) | 7 (30.4) | 12 (26.7) |
| South American | 1 (4.5) | 1 (4.3) | 2 (4.4) |
| Nativity, n (%) | |||
| Not born in 50 US States | 17 (77.3) | 16 (69.6) | 33 (73.3) |
| Born in 50 US States | 5 (22.7) | 7 (30.4) | 12 (26.7) |
| Arsenic | SOLNAS Visit | Mean (SD) | Median (IQR) | Minimum | Max | # Below LOD |
|---|---|---|---|---|---|---|
| u∑As †, µg/L | 1 | 28.46 (47.42) | 16.20 (7.20, 24.40) | 2.20 | 227.20 | 0 |
| 2 | 11.71 (8.00) | 11.90 (4.38, 17.28) | 1.30 | 26.20 | 0 | |
| 3 | 20.50 (18.71) | 12.65 (10.00, 26.32) | 2.10 | 78.90 | 0 | |
| ∑As ¥, µg/L | 1 | 9.58 (10.75) | 6.04 (4.30, 10.46) | 1.99 | 69.30 | N/A |
| 2 | 7.34 (5.94) | 5.43 (2.77, 12.77) | 1.03 | 19.18 | N/A | |
| 3 | 9.80 (5.94) | 8.54 (5.75, 11.99) | 2.70 | 24.84 | N/A | |
| Inorganic As (iAs), µg/L | 1 | 0.91 (0.83) | 0.60 (0.40, 0.97) | <LOD | 3.37 | 1 |
| 2 | 0.71 (0.64) | 0.58 (0.18, 0.87) | <LOD | 2.19 | 2 | |
| 3 | 1.11 (0.94) | 0.74 (0.58, 1.31) | 0.19 | 4.11 | 0 | |
| Monomethylated As (MMA), µg/L | 1 | 2.08 (5.32) | 1.16 (0.69, 1.86) | 0.19 | 36.41 | 0 |
| 2 | 1.09 (0.98) | 0.86 (0.44, 1.45) | 0.13 | 4.11 | 0 | |
| 3 | 1.75 (1.21) | 1.38 (0.92, 2.13) | 0.39 | 4.83 | 0 | |
| Dimethylated As (DMA), µg/L | 1 | 13.26 (22.01) | 7.18 (4.29, 15.27) | 1.25 | 148.86 | 0 |
| 2 | 7.05 (5.17) | 5.69 (3.13, 11.32) | 0.78 | 18.95 | 0 | |
| 3 | 10.26 (6.24) | 9.02 (6.36, 10.71) | 1.73 | 26.76 | 0 | |
| iAs % | 1 | 8.78 (3.73) | 8.28 (6.51, 11.03) | 0.22 | 20.09 | N/A |
| 2 | 8.67 (4.07) | 8.98 (6.28, 10.00) | 0.50 | 20.86 | N/A | |
| 3 | 9.58 (3.84) | 8.26 (7.37, 11.24) | 5.36 | 21.30 | N/A | |
| MMA% | 1 | 12.26 (4.96) | 12.25 (9.12, 14.69) | 2.49 | 26.32 | N/A |
| 2 | 12.69 (4.28) | 11.59 (9.75, 13.71) | 7.47 | 21.85 | N/A | |
| 3 | 13.60 (5.22) | 13.21 (10.51, 17.23) | 5.84 | 23.12 | N/A | |
| DMA% | 1 | 80.31 (7.66) | 79.56 (76.22, 83.93) | 59.81 | 96.09 | N/A |
| 2 | 79.69 (5.95) | 80.13 (77.34, 83.21) | 68.20 | 89.79 | N/A | |
| 3 | 78.12 (7.89) | 78.59 (73.14, 83.75) | 64.36 | 89.78 | N/A |
| As Species | All Visits † (n = 85) | Second vs. First (n = 65) | Third vs. First (n = 65) |
|---|---|---|---|
| Log-∑As * | 0.48 (0.27–0.70) | 0.62 (0.37–0.82) | 0.42 (0.15–0.76) |
| Inorganic As (iAs) % | 0.36 (0.15–0.63) | 0.20 (0.02–0.75) | 0.65 (0.41–0.84) |
| Monomethylarsonic acid (MMA) % | 0.74 (0.57–0.85) | 0.71 (0.48–0.86) | 0.72 (0.50–0.87) |
| Dimethylarsinic acid (DMA) % | 0.67 (0.49–0.81) | 0.57 (0.31–0.8) | 0.71 (0.49–0.86) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hosgood, H.D.; Slavkovich, V.; Hua, S.; Klugman, M.; Grau-Perez, M.; Thyagarajan, B.; Graziano, J.; Cai, J.; Shaw, P.A.; Kaplan, R.; et al. Urinary Arsenic Species are Detectable in Urban Underserved Hispanic/Latino Populations: A Pilot Study from the Study of Latinos: Nutrition & Physical Activity Assessment Study (SOLNAS). Int. J. Environ. Res. Public Health 2020, 17, 2247. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072247
Hosgood HD, Slavkovich V, Hua S, Klugman M, Grau-Perez M, Thyagarajan B, Graziano J, Cai J, Shaw PA, Kaplan R, et al. Urinary Arsenic Species are Detectable in Urban Underserved Hispanic/Latino Populations: A Pilot Study from the Study of Latinos: Nutrition & Physical Activity Assessment Study (SOLNAS). International Journal of Environmental Research and Public Health. 2020; 17(7):2247. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072247
Chicago/Turabian StyleHosgood, H. Dean, Vesna Slavkovich, Simin Hua, Madelyn Klugman, Maria Grau-Perez, Bharat Thyagarajan, Joseph Graziano, Jianwen Cai, Pamela A Shaw, Robert Kaplan, and et al. 2020. "Urinary Arsenic Species are Detectable in Urban Underserved Hispanic/Latino Populations: A Pilot Study from the Study of Latinos: Nutrition & Physical Activity Assessment Study (SOLNAS)" International Journal of Environmental Research and Public Health 17, no. 7: 2247. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072247