Contact Allergy—Emerging Allergens and Public Health Impact


Abstract
:1. Introduction
2. Methods
3. Results
3.1. Metals
3.2. Fragrances
3.3. Preservatives
3.4. Plastic Monomers and Rubber
3.5. Medicines (Active Principles and Excipients) and Cosmetics
3.6. Medical Devices
3.7. Clothing, Leather, and Dyes
3.8. Woods, Plants and Plant-Derived Materials
3.9. New Allergens
4. Discussion
4.1. Allergen-Specific Aspects
4.2. Pre-Marketing Screening: Alternative Methods
4.3. Post-Marketing Surveillance
4.4. Implications for Regulation
5. Conclusions
Funding
Conflicts of Interest
Abbreviations
| Shorthand | Explanation |
| ACD | Allergic contact dermatitis |
| CI | Confidence interval |
| EBS | European baseline series |
| ECHA | European Chemicals Agency (echa.europa.eu) |
| EECDRG | European Environmental and Contact Dermatitis Research Group (<www.eecdrg.org>) |
| ESCD | European Society of Contact Dermatitis (<www.escd.org>) |
| FM | Fragrance mix |
| GC-MS | Gas chromatography-mass spectrometry |
| HICC | Hydroxyisohexyl 3-cyclohexene carboxaldehyde |
| HPLC | High-performance liquid chromatography |
| ICPMS | Inductively coupled plasma mass spetrometry |
| IVDK | Information Network of Departments of Dermatology (<www.ivdk.org>) |
| LTT | Lymphocyte Transformation Test |
| M(C)I | Methyl(chloro)isothiazolinone |
| OOHs | Hydroperoxides |
| OR | Odds ratio |
| pet. | Petrolatum (as patch test vehicle) |
| QoL | Quality of life |
| ROAT | Repeated open application test |
References
- Diepgen, T.L.; Ofenloch, R.F.; Bruze, M.; Bertuccio, P.; Cazzaniga, S.; Coenraads, P.-J.; Elsner, P.; Gonçalo, M.; Svensson, Å.; Naldi, L. Prevalence of contact allergy in the general population in different European regions. Br. J. Derm. 2016, 174, 319–329. [Google Scholar] [CrossRef]
- Alinaghi, F.; Bennike, N.H.; Egeberg, A.; Thyssen, J.P.; Johansen, J.D. Prevalence of contact allergy in the general population: A systematic review and meta-analysis. Contact Derm. 2019, 80, 77–85. [Google Scholar] [CrossRef]
- Fischer, L.A.; Menné, T.; Voelund, A.; Johansen, J.D. Can exposure limitations for well-known contact allergens be simplified? An analysis of dose-response patch test data. Contact Derm. 2011, 64, 337–342. [Google Scholar] [CrossRef]
- Langen, U.; Schmitz, R.; Steppuhng, H. Häufigkeit allergischer erkrankungen in Deutschland ergebnisse der studie zur gesundheit erwachsener in Deutschland (DEGS1). Bundesgesundheitsblatt Gesundh. Gesundh. 2013, 56, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Uter, W.; Werfel, T.; White, I.R.; Johansen, J.D. Contact allergy: A review of current problems from a clinical perspective. Int. J. Env. Res. Public Health 2018, 15, 1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uter, W.; Schnuch, A.; Giménez-Arnau, A.; Orton, D. Databases and networks. The benefit for research and quality assurance in patch testing. In Contact Dermatitis; Duus Johansen, J., Mahler, V., Lepoittevin, J.-P., Frosch, P.J., Eds.; Springer: Heidelberg, Germany, 2019. [Google Scholar]
- Ahlström, M.G.; Thyssen, J.P.; Menné, T.; Johansen, J.D. Prevalence of nickel allergy in Europe following the EU Nickel Directive—A review. Contact Derm. 2017, 77, 193–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuttelaar, M.L.A.; Ofenloch, R.F.; Bruze, M.; Cazzaniga, S.; Elsner, P.; Gonçalo, M.; Naldi, L.; Svensson, Å.; Diepgen, T.L. Prevalence of contact allergy to metals in the European general population with a focus on nickel and piercings: The EDEN fragrance study. Contact Derm. 2018, 79, 1–9. [Google Scholar] [CrossRef]
- Simonsen, A.B.; Foss-Skiftesvik, M.H.; Thyssen, J.P.; Deleuran, M.; Mortz, C.G.; Zachariae, C.; Skov, L.; Osterballe, M.; Funding, A.; Avnstorp, C.; et al. Contact allergy in Danish children: Current trends. Contact Derm. 2018, 79, 295–302. [Google Scholar] [CrossRef]
- Ahlström, M.G.; Thyssen, J.P.; Wennervaldt, M.; Menné, T.; Johansen, J.D. Nickel allergy and allergic contact dermatitis: A clinical review of immunology, epidemiology, exposure, and treatment. Contact Derm. 2019, 81, 227–241. [Google Scholar] [CrossRef] [Green Version]
- Uter, W.; Wolter, J. Nickel and cobalt release from earrings and piercing jewellery-analytical results of a German survey in 2014. Contact Derm. 2018, 78, 321–328. [Google Scholar] [CrossRef]
- Ahlström, M.G.; Thyssen, J.P.; Menné, T.; Jellesen, M.S.; Westermann, P.J.S.; Johansen, J.D. Nickel and cobalt release from fidget spinners on the Danish market. Contact Derm. 2018, 78, 357–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lian, B.S.Y.; McFadden, J.P.; Lee, S.X. Nickel by proxy. Contact Derm. 2019, 81, 69. [Google Scholar] [CrossRef] [PubMed]
- White, J.M.L.; du Vivier, A.W.P. Occupational allergic contact dermatitis caused by nickel in embroidery needles. Contact Derm. 2018, 79, 181–182. [Google Scholar] [CrossRef] [PubMed]
- Symanzik, C.; John, S.M.; Strunk, M. Nickel release from metal tools in the German hairdressing trade—A current analysis. Contact Derm. 2019, 80, 382–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warshaw, E.M.; Schlarbaum, J.P.; DeKoven, J.G.; Silverberg, J.I.; Zug, K.A.; Marks, J.G.; Belsito, D.V.; Mathias, T.; Reeder, M.J.; Atwater, A.R.; et al. Occupationally related nickel reactions: A retrospective analysis of the north american contact dermatitis group data 1998–2016. Dermatitis 2019, 30, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Wennervaldt, M.; Ahlström, M.G.; Menné, T.; Thyssen, J.P.; Johansen, J.D. Diagnostic workup of occupational allergic nickel dermatitis in a nurse with multiple nickel exposures. Contact Derm. 2019, 81, 311–313. [Google Scholar] [CrossRef] [PubMed]
- Jellesen, M.S.; Olsen, C.B.; Ruff, S.; Spiewak, R.; Hamann, D.; Hamann, C.R.; White, I.R.; Johansen, J.D.; Thyssen, J.P. Electrochemical screening spot test method for detection of nickel and cobalt ion release from metal surfaces. Dermatitis 2018, 29, 187–192. [Google Scholar] [CrossRef] [Green Version]
- Goldminz, A.M.; Scheinman, P.L. Comparison of nickel sulfate 2.5% and nickel sulfate 5% for detecting nickel contact allergy. Dermatitis 2018, 29, 321–323. [Google Scholar] [CrossRef]
- Bruze, M.; Hindsén, M.; Mowitz, M. A retrospective study of aimed patch testing with aqueous nickel sulfate hexahydrate at 30% and 15% in patients with dermatitis. Dermatitis 2018, 29, 193–195. [Google Scholar] [CrossRef]
- Prasithirun, P.; Kasemsarn, P.; Boonchai, W. Allergic contact dermatitis caused by nickel in an eyebrow pencil. Contact Derm. 2019, 80, 125–126. [Google Scholar] [CrossRef]
- Nixon, R.L.; Higgins, C.L.; Maor, D.; Rajgopal Bala, H.; Lalji, A.; Heim, K.E. Does clinical testing support the current guidance definition of prolonged contact for nickel allergy? Contact Derm. 2018, 79, 356–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahlström, M.G.; Thyssen, J.P.; Menné, T.; Lidén, C. Short contact with nickel is not harmless. Contact Derm. 2019, 80, 259–260. [Google Scholar] [CrossRef] [PubMed]
- Ahlström, M.G.; Midander, K.; Menné, T.; Lidén, C.; Johansen, J.D.; Julander, A.; Thyssen, J.P. Nickel deposition and penetration into the stratum corneum after short metallic nickel contact: An experimental study. Contact Derm. 2019, 80, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Shutty, B.G.; Scheinman, P.L. Allergic contact mucositis caused by metal: A covertly located permanent dental retainer. Contact Derm. 2018, 78, 88–90. [Google Scholar] [CrossRef]
- Malinauskiene, L. Contact allergy to a meteorite: An interesting consequence of nickel allergy. Contact Derm. 2018, 79, 36–37. [Google Scholar] [CrossRef]
- Limone, B.A.; Jacob, S.E. Military Decorative pin dermatitis: prevention for nickel allergy among service members. Dermatitis 2018, 29, 46–47. [Google Scholar] [CrossRef]
- Malmberg, P.; Guttenberg, T.; Ericson, M.B.; Hagvall, L. Imaging mass spectrometry for novel insights into contact allergy—a proof-of-concept study on nickel. Contact Derm. 2018, 78, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Alinaghi, F.; Zachariae, C.; Thyssen, J.P.; Johansen, J.D. Causative exposures and temporal development of cobalt allergy in Denmark between 2002 and 2017. Contact Derm. 2019, 81, 242–248. [Google Scholar] [CrossRef] [Green Version]
- Dittmar, D.; Ofenloch, R.F.; Schuttelaar, M.L.A. Persistence of contact allergy: A retrospective analysis. Contact Derm. 2018, 78, 143–150. [Google Scholar] [CrossRef] [Green Version]
- Hamann, D.; Hamann, C.R.; Kishi, P.; Menné, T.; Thyssen, J.P. Cobalt not detected in contemporary US consumer paint colorants by cobalt indicator solution or X-ray fluorescence spectroscopy. Contact Derm. 2018, 78, 355–356. [Google Scholar] [CrossRef]
- Kettelarij, J.; Midander, K.; Lidén, C.; Julander, A. Contamination of skin and surfaces by cobalt in the hard metal industry. Contact Derm. 2018, 79, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Hamann, C.R.; Hamann, D.; Simonsen, A.B.; Zachariae, C.; Johansen, J.D.; Thyssen, J.P. Cobalt content of a convenience sample of leather shoes and gloves in Denmark. Contact Derm. 2019, 80, 248–249. [Google Scholar] [CrossRef] [PubMed]
- Simonsen, A.B.; Friis, U.F.; Johansen, J.D.; Zachariae, C.; Sloth, J.J.; Thyssen, J.P. Occupational allergic contact dermatitis caused by cobalt in machine oil. Contact Derm. 2019, 80, 59–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verma, K.K.; Zimerson, E.; Bruze, M.; Engfeldt, M.; Svedman, C.; Isaksson, M. Is a high concentration of hexavalent chromium in Indian cement causing an increase in the frequency of cement dermatitis in India? Contact Derm. 2018, 79, 49–51. [Google Scholar] [CrossRef] [PubMed]
- Alinaghi, F.; Zachariae, C.; Thyssen, J.P.; Johansen, J.D. Temporal changes in chromium allergy in Denmark between 2002 and 2017. Contact Derm. 2019, 80, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Lejding, T.; Mowitz, M.; Isaksson, M.; Bruze, M.; Pontén, A.; Svedman, C.; Zimerson, E.; Engfeldt, M. A retrospective investigation of hexavalent chromium allergy in southern Sweden. Contact Derm. 2018, 78, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Bocca, B.; Senofonte, O.; Petrucci, F. Hexavalent chromium in tattoo inks: Dermal exposure and systemic risk. Contact Derm. 2018, 79, 218–225. [Google Scholar] [CrossRef]
- Hedberg, Y.S.; Erfani, B.; Matura, M.; Lidén, C. Chromium (III) release from chromium-tanned leather elicits allergic contact dermatitis: A use test study. Contact Derm. 2018, 78, 307–314. [Google Scholar] [CrossRef] [Green Version]
- Hedberg, Y.S.; Wei, Z.; Moncada Chévez, F. Chromium (III), chromium (VI) and cobalt release from leathers produced in Nicaragua. Contact Derm. 2019, 80, 149–155. [Google Scholar] [CrossRef] [Green Version]
- Jiang, A.; Harrison, J.C.; Siegel, P.D.; Maibach, H. Possible role of regional variation in allergic contact dermatitis: Case report. Contact Derm. 2018, 78, 228–229. [Google Scholar] [CrossRef]
- Van Delft, L.C.J.; Ramakers, N.A.M.; Verstraeten, V.L.R.M. Peculiar contact dermatitis in a construction worker. Contact Derm. 2019, 80, 166–167. [Google Scholar] [CrossRef] [PubMed]
- Tewari, A.; Khan, I.; Ostlere, L. Steering wheel and gearstick dermatitis caused by chromate. Contact Derm. 2019, 81, 322–323. [Google Scholar] [CrossRef] [PubMed]
- Reveko, V.; Lampert, F.; Din, R.U.; Thyssen, J.P.; Møller, P. False-positive result when a diphenylcarbazide spot test is used on trivalent chromium-passivated zinc surfaces. Contact Derm. 2018, 78, 315–320. [Google Scholar] [CrossRef]
- Marsidi, N.; Beijnen, J.H.; van Zuuren, E.J. Palladium-induced granulomas analysed with inductively coupled plasma mass spectrometry. Contact Derm. 2018, 79, 41–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Ruiz, L.; Vergara De Caso, E.; Peña-Sánchez, R.; Silvestre-Salvador, J.F. Delayed hypersensitivity to palladium dichloride: 15-year retrospective study in a skin allergy unit. Contact Derm. 2019, 81, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Rosholm Comstedt, L.; Engfeldt, M.; Svedman, C.; Åkesson, A.; Hindsén, M.; Bruze, M. Variation and covariation in patch test reactivity to palladium and nickel salts. Eur. J. Derm. 2018, 28, 668–676. [Google Scholar]
- Garcia-Nunez, I.; Algaba-Marmol, M.-A.; Suarez-Vergara, M.; Fuentes-Soltero, J.; Fernandez-Barrera, C.; Bartolome, B.; Grau-Bonete, A.; Ignacio-Garcia, J.-M. Vanadium contact dermatitis: Case report and studies performed. Contact Derm. 2019, 80, 127–128. [Google Scholar] [CrossRef]
- Gil, F.; Rato, M.; Monteiro, A.; Parente, J.; Aranha, J. Occupational lichenoid allergic contact dermatitis caused by tin. Contact Derm. 2019, 81, 71–73. [Google Scholar] [CrossRef]
- Matsudate, Y.; Yamashita, M.; Fujii, Y.; Urano, Y. Contact granulomatous hypersensitivity to indium in a patient with orofacial granulomatosis. Contact Derm. 2019, 81, 293–294. [Google Scholar] [CrossRef]
- Deleuran, M.G.; Ahlström, M.G.; Zachariae, C.; Johansen, J.D.; Thyssen, J.P. Patch test reactivity to aluminium chambers. Contact Derm. 2019, 81, 318–319. [Google Scholar] [CrossRef]
- King, N.; Moffitt, D. Allergic contact dermatitis secondary to the use of aluminium Finn Chambers®. Contact Derm. 2018, 78, 365–366. [Google Scholar] [CrossRef] [PubMed]
- Gente Lidholm, A.; Inerot, A.; Gillstedt, M.; Bergfors, E.; Trollfors, B. Comparison of reactivity to a metallic disc and 2% aluminium salt in 366 children, and reproducibility over time for 241 young adults with childhood vaccine-related aluminium contact allergy. Contact Derm. 2018, 79, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Bergfors, E.; Inerot, A.; Falk, L.; Nyström, U.; Trollfors, B. Patch testing children with aluminium chloride hexahydrate in petrolatum: A review and a recommendation. Contact Derm. 2019, 81, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goiset, A.; Darrigade, A.-S.; Labrèze, C.; Boralevi, F.; Milpied, B. Aluminium sensitization in a French paediatric patch test population. Contact Derm. 2018, 79, 382–383. [Google Scholar] [CrossRef] [PubMed]
- Poziomkowska-Gęsicka, I.; Summer, B.; Sokołowska, M.; Thomas, P.; Kurek, M. Allergic contact dermatitis caused by hypersensitivity to gold-description of a clinical case. Contact Derm. 2018, 78, 363–365. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Villa Lario, A.; Medina-Montalvo, S.; Gómez-Zubiaur, A.; Montes-Mollón, M.Á.; Álvarez-Castro, Y.; Piteiro-Bermejo, A.B.; Trasobares-Marugán, L. Late cutaneous B-cell pseudolymphoma after an upper-eyelid gold weight implant. Contact Derm. 2019, 80, 256–258. [Google Scholar] [CrossRef]
- Pita da Veiga, G.; Sainz-Gaspar, L.; Suárez-Peñaranda, J.M.; Sánchez-Aguilar, D.; Vázquez-Veiga, H.; Fernández-Redondo, V. Late cutaneous reaction after gold patch testing with features of Langerhans cell histiocytosis. Contact Derm. 2019, 81, 291–292. [Google Scholar] [CrossRef]
- Hamann, D.; Bruze, M.; Fowler, J.F.; Hamann, C.R.; Andersen, K.E.; Hamann, C.P. Excipient and dose per unit area affect sensitivity when patch testing with gold sodium thiosulfate. Dermatitis 2018, 29, 258–263. [Google Scholar] [CrossRef]
- Suzuki, K.; Yagami, A.; Ito, A.; Kato, A.; Miyazawa, H.; Kanto, H.; Matsunaga, K. Positive reactions to gold sodium thiosulfate in patch test panels (TRUE Test) in Japan: A multicentre study. Contact Derm. 2019, 80, 114–117. [Google Scholar] [CrossRef]
- Hamann, D.; Hamann, C.; Fowler, J.F.; Andersen, K.E.; Bruze, M. Response to: Positive reactions to gold sodium thiosulfate in patch test panels (TRUE Test) in Japan: A multicentre study. Contact Derm. 2019, 81, 156. [Google Scholar] [CrossRef] [Green Version]
- Lyapina, M.; Dencheva, M.; Krasteva, A.; Cekova, M.; Deliverska, M.; Vodenicharov, V.; Markov, D.; Mitova, Y.; Kisselova, A. Contact sensitization to metals in dental exposures in Bulgaria. Biotechnol. Biotechnol. Equip. 2018, 32, 707–713. [Google Scholar] [CrossRef] [Green Version]
- De Graaf, N.P.J.; Feilzer, A.J.; Kleverlaan, C.J.; Bontkes, H.; Gibbs, S.; Rustemeyer, T. A retrospective study on titanium sensitivity: Patch test materials and manifestations. Contact Derm. 2018, 79, 85–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furrer, S.; Scherer Hofmeier, K.; Grize, L.; Bircher, A.J. Metal hypersensitivity in patients with orthopaedic implant complications-A retrospective clinical study. Contact Derm. 2018, 79, 91–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Groot, A.C. Myroxylon pereirae resin (balsam of Peru)-A critical review of the literature and assessment of the significance of positive patch test reactions and the usefulness of restrictive diets. Contact Derm. 2019, 80, 335–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ung, C.Y.; White, J.M.L.; White, I.R.; Banerjee, P.; McFadden, J.P. Patch testing with the European baseline series fragrance markers: A 2016 update. Br. J. Derm. 2018, 178, 776–780. [Google Scholar] [CrossRef] [PubMed]
- Dittmar, D.; Schuttelaar, M.L.A. Contact sensitization to hydroperoxides of limonene and linalool: Results of consecutive patch testing and clinical relevance. Contact Derm. 2019, 80, 101–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, F.; Mu, Z.; He, C.; Xue, C.; Li, W.; Wang, Q.; Chen, Z.; Zhang, J. Patch testing in facial dermatitis using chinese baseline series (60 allergens) and cosmetic series (58 allergens). J. Eur. Acad. Derm. Venereol. 2018, 32, E288–E289. [Google Scholar] [CrossRef]
- Hennen, J.; Silva, E.; Sousa, M.; Sahli, F.; Lichter, J.; Lepoittevin, J.-P.; Giménez-Arnau, E.; Blömeke, B. Sensitization potential and potency of terpene hydroperoxides in the cocultured activation test method. Contact Derm. 2019, 81, 97–103. [Google Scholar] [CrossRef]
- Bennike, N.H.; Oturai, N.B.; Müller, S.; Kirkeby, C.S.; Jørgensen, C.; Christensen, A.B.; Zachariae, C.; Johansen, J.D. Fragrance contact allergens in 5588 cosmetic products identified through a novel smartphone application. J. Eur. Acad. Derm. Venereol. 2018, 32, 79–85. [Google Scholar] [CrossRef]
- Wieck, S.; Olsson, O.; Kümmerer, K.; Klaschka, U. Fragrance allergens in household detergents. Regul. Toxicol. Pharm. 2018, 97, 163–169. [Google Scholar] [CrossRef]
- Gatica-Ortega, M.-E.; Pastor-Nieto, M.-A.; Schoendorff-Ortega, C.; Mollejo-Villanueva, M.; Giménez-Arnau, A. Lymphomatoid contact dermatitis caused by limonene hydroperoxides confirmed by an exposure provocation test with the involved personal hygiene products. Contact Derm. 2018, 78, 230–233. [Google Scholar] [CrossRef] [PubMed]
- Isaksson, M.; Karlberg, A.-T.; Nilsson, U. Allergic contact dermatitis caused by oxidized linalool in a deodorant. Contact Derm. 2019, 81, 213–214. [Google Scholar] [CrossRef] [PubMed]
- Bennike, N.H.; Palangi, L.; Christensson, J.B.; Nilsson, U.; Zachariae, C.; Johansen, J.D.; Hagvall, L. Allergic contact dermatitis caused by hydroperoxides of limonene and dose-response relationship-A repeated open application test (ROAT) study. Contact Derm. 2019, 80, 208–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagvall, L.; Bruze, M.; Engfeldt, M.; Isaksson, M.; Lindberg, M.; Ryberg, K.; Stenberg, B.; Svedman, C.; Karlberg, A.-T.; Bråred Christensson, J. Contact allergy to oxidized geraniol among swedish dermatitis patients-A multicentre study by the swedish contact dermatitis research group. Contact Derm. 2018, 79, 232–238. [Google Scholar] [CrossRef] [Green Version]
- Silvestre, J.F.; Mercader, P.; González-Pérez, R.; Hervella-Garcés, M.; Sanz-Sánchez, T.; Córdoba, S.; Sánchez-Pérez, J.; Heras-Mendoza, F.; Giménez-Arnau, A.M.; Gatica-Ortega, M.E.; et al. Sensitization to fragrances in Spain: A 5-year multicentre study (2011–2015). Contact Derm. 2019, 80, 94–100. [Google Scholar] [CrossRef]
- Paulsen, E.; Andersen, F. Fragrant and sticky allergens from the pinewood: Cohabiting and coreacting. Contact Dermat. 2019, 81, 374–377. [Google Scholar] [CrossRef]
- Moss, E.; Debeuckelaere, C.; Berl, V.; Elbayed, K.; Moussallieh, F.-M.; Namer, I.-J.; Lepoittevin, J.-P. In situ metabolism of cinnamyl alcohol in reconstructed human epidermis: new insights into the activation of this fragrance skin sensitizer. Chem. Res. Toxicol. 2016, 29, 1172–1178. [Google Scholar] [CrossRef]
- Goossens, A.; Huygens, S.; Stoskute, L.; Lepoittevin, J.-P. Primary sensitization to cinnamyl chloride in an operator of a pharmaceutical company. Contact Derm. 2006, 55, 364–365. [Google Scholar] [CrossRef]
- Hagvall, L.; Niklasson, I.B.; Luthman, K.; Karlberg, A.-T. Can the epoxides of cinnamyl alcohol and cinnamal show new cases of contact allergy? Contact Derm. 2018, 78, 399–405. [Google Scholar] [CrossRef]
- Bruze, M.; Mowitz, M.; Ofenloch, R.; Coenraads, P.-J.; Diepgen, T.L.; Elsner, P.; Gonçalo, M.; Naldi, L.; Svensson, Å. The significance of batch and patch test method in establishing contact allergy to fragrance mix I-EDEN fragrance study group. Contact Derm. 2019, 81, 104–109. [Google Scholar] [CrossRef]
- De Groot, A.; Gilissen, L.; Geier, J.; Orton, D.; Goossens, A. Adding sorbitan sesquioleate to the European baseline series: Necessary, reasonable, or unavoidable? Contact Derm. 2019, 81, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, R.L.; Agius, R.; Wilkinson, S.M.; Carder, M. UK trends of allergic occupational skin disease attributed to fragrances 1996–2015. Contact Derm. 2018, 78, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Carøe, T.K.; Ebbehøj, N.E.; Bonde, J.P.; Agner, T. Occupational hand eczema and/or contact urticaria: Factors associated with change of profession or not remaining in the workforce. Contact Derm. 2018, 78, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Tous-Romero, F.; Prieto-Barrios, M.; Andrés-Lencina, J.J.; de Frutos, J.O. Allergic contact dermatitis caused by benzyl salicylate in hair products. Contact Derm. 2018, 79, 310–311. [Google Scholar] [CrossRef] [PubMed]
- Bui, T.N.P.T.; Mose, K.F.; Andersen, F. Eugenol allergy mimicking burning mouth syndrome. Contact Derm. 2019, 80, 54–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kroona, L.; Isaksson, M.; Ahlgren, C.; Dahlin, J.; Bruze, M.; Warfvinge, G. carvone contact allergy in southern sweden: A 21-year retrospective study. Acta Derm. Venereol. 2018, 98, 938–942. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Herrero, A.; Vergara-de Caso, E.; Vera-Álvarez, S.; Espinosa-Hidalgo, I.; Silvestre Salvador, J.F. Burning mouth syndrome triggered by cinnamal present in a denture fixative cream. Contact Derm. 2019, 81, 147–149. [Google Scholar] [CrossRef]
- Shim, T.N.; Kosztyuova, T. Allergic contact dermatitis to electronic cigarette. Dermatitis 2018, 29, 94–95. [Google Scholar] [CrossRef]
- Azevedo, A.; Lobo, I.; Selores, M. Allergic contact dermatitis and electronic cigarettes: Is nickel to blame? Contact Derm. 2019, 81, 135–136. [Google Scholar] [CrossRef]
- Shah, K.M.; Goldman, S.E.; Agim, N.G. Airborne contact dermatitis caused by essential oils in a child. Dermatitis 2019, 30, 79–80. [Google Scholar] [CrossRef]
- Elshimy, N.; Sheraz, F.; Lyon, C. The secret sensitizer gets out of the bag. Contact Derm. 2018, 79, 54–55. [Google Scholar] [CrossRef] [PubMed]
- SCCS (Scientific Committee on Consumer Safety). Opinion on Fragrance Allergens in Cosmetic Products. 26–27 June 2012. Available online: https://ec.europa.eu/health/scientific_committees/consumer_safety/docs/sccs_o_102.pdf (accessed on 1 April 2020).
- Goodier, M.C.; Zhang, A.J.; Nikle, A.B.; Hylwa, S.A.; Goldfarb, N.I.; Warshaw, E.M. Use of essential oils: A general population survey. Contact Derm. 2019, 80, 391–393. [Google Scholar] [CrossRef] [PubMed]
- Attasuriyanan, M.; Sajjachareonpong, P.; Tresukosol, P.; Puangpet, P. Occupational allergic contact dermatitis in Thai spa therapists. Contact Derm. 2019, 81, 299–300. [Google Scholar] [CrossRef] [PubMed]
- Bingham, L.J.; Tam, M.M.; Palmer, A.M.; Cahill, J.L.; Nixon, R.L. Contact allergy and allergic contact dermatitis caused by lavender: A retrospective study from an australian clinic. Contact Derm. 2019, 81, 37–42. [Google Scholar] [CrossRef]
- Corazza, M.; Amendolagine, G.; Borghi, A.; Toni, G.; Lauriola, M.M. Aromatherapy and occupational allergic contact dermatitis: Two further cases caused by lavender oil and other essential oils. Contact Derm. 2019, 81, 378–379. [Google Scholar] [CrossRef]
- Bennike, N.H.; Zachariae, C.; Johansen, J.D. Optimal patch test concentration for three widely used sensitizing fragrance substances without mandatory labelling in cosmetics. Contact Derm. 2019, 80, 325–327. [Google Scholar] [CrossRef]
- Uter, W.; Aalto-Korte, K.; Agner, T.; Andersen, K.E.; Bircher, A.J.; Brans, R.; Bruze, M.; Diepgen, T.L.; Foti, C.; Giménez Arnau, A.; et al. The epidemic of methylisothiazolinone contact allergy in Europe: Follow-up on changing exposures. J. Eur. Acad. Derm. Venereol. 2019, 34, 333–339. [Google Scholar] [CrossRef] [Green Version]
- Marrero-Alemán, G.; Saavedra Santana, P.; Liuti, F.; Hernández, N.; López-Jiménez, E.; Borrego, L. The role of cleaning products in epidemic allergic contact dermatitis to methylchloroisothiazolinone/methylisothiazolinone. Dermatitis 2018, 29, 77–80. [Google Scholar] [CrossRef]
- Flury, U.; Palmer, A.; Nixon, R. The methylisothiazolinone contact allergy epidemic in Australia. Contact Derm. 2018, 79, 189–191. [Google Scholar] [CrossRef]
- Salman, A. Methylchloroisothiazolinone and methylisothiazolinone contact allergy: A retrospective cohort study from a tertiary dermatology clinic in Turkey. Contact Derm. 2019, 80, 193–194. [Google Scholar] [CrossRef]
- Sukakul, T.; Chaweekulrat, P.; Limphoka, P.; Boonchai, W. Changing trends of contact allergens in Thailand: A 12-year retrospective study. Contact Derm. 2019, 81, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Sukakul, T.; Kanchanapenkul, D.; Bunyavaree, M.; Limphoka, P.; Kumpangsin, T.; Boonchai, W. Methylchloroisothiazolinone and/or methylisothiazolinone in cosmetic products-A market survey. Contact Derm. 2019, 80, 110–113. [Google Scholar] [CrossRef] [PubMed]
- DeKoven, J.G.; Warshaw, E.M.; Zug, K.A.; Maibach, H.I.; Belsito, D.V.; Sasseville, D.; Taylor, J.S.; Fowler, J.F.; Mathias, C.G.T.; Marks, J.G.; et al. North American contact dermatitis group patch test results: 2015–2016. Dermatitis 2018, 29, 297–309. [Google Scholar] [CrossRef] [PubMed]
- Panasoff, J. Widespread eczema in an elderly patient. Contact Derm. 2018, 78, 299–301. [Google Scholar] [CrossRef]
- Thomsen, A.V.; Schwensen, J.F.; Bossi, R.; Banerjee, P.; Giménez-Arnau, E.; Lepoittevin, J.-P.; Lidén, C.; Uter, W.; White, I.R.; Johansen, J.D. Isothiazolinones are still widely used in paints purchased in five European countries: A follow-up study. Contact Derm. 2018, 78, 246–253. [Google Scholar] [CrossRef] [Green Version]
- Goodier, M.C.; Siegel, P.D.; Zang, L.-Y.; Warshaw, E.M. Isothiazolinone in residential interior wall paint: A high-performance liquid chromatographic-mass spectrometry analysis. Dermatitis 2018, 29, 332–338. [Google Scholar] [CrossRef]
- Goodier, M.C.; Zang, L.-Y.; Siegel, P.D.; Warshaw, E.M. Isothiazolinone content of us consumer adhesives: Ultrahigh-performance liquid chromatographic mass spectrometry analysis. Dermatitis 2019, 30, 129–134. [Google Scholar] [CrossRef]
- Amsler, E.; Aerts, O.; Raison-Peyron, N.; Debons, M.; Milpied, B.; Giordano-Labadie, F.; Waton, J.; Ferrier-Le Bouëdec, M.C.; Lartigau, I.; Pecquet, C.; et al. Airborne allergic contact dermatitis caused by isothiazolinones in water-based paints: A retrospective study of 44 cases. Contact Derm. 2017, 77, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Sechi, A.; Vincenzi, C.; Tengattini, V.; Piraccini, B.M.; Neri, I.; La Placa, M. Airborne dermatitis in a child caused by isothiazolinones in a water-based paint in Italy: Call for better regulations. Contact Derm. 2018, 79, 45–46. [Google Scholar] [CrossRef]
- Martinez-Mera, C.; González, M.A.; Hospital, M.; Turrión-Merino, L. Isothiazolinones in paint as a cause of airborne contact dermatitis in a patient with psoriasis receiving anti-interleukin-17 therapy. Contact Derm. 2019, 80, 328–329. [Google Scholar] [CrossRef]
- Christiansen, M.S.; Agner, T.; Ebbehøj, N.E. Long-lasting allergic contact dermatitis caused by methylisothiazolinone in wall paint: A case report. Contact Derm. 2018, 79, 112–113. [Google Scholar] [CrossRef] [PubMed]
- Aerts, O.; Goossens, A.; Marguery, M.-C.; Castelain, M.; Boursault, L.; Giordano-Labadie, F.; Lambert, J.; Milpied, B. Photoaggravated allergic contact dermatitis and transient photosensitivity caused by methylisothiazolinone. Contact Dermat. 2018, 78, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Ljubojević Hadžavdić, S.; Uter, W.; Ilijanić Samošćanec, M.; Johansen, J.D. Methylisothiazolinone contact allergy in Croatia: Epidemiology and course of disease following patch testing. Contact Derm. 2018, 79, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Bouschon, P.; Waton, J.; Pereira, B.; Schmutz, J.-L.; Le Bouëdec, M.-C.F.; D’Incan, M. Methylisothiazolinone allergic contact dermatitis: Assessment of relapses in 139 patients after avoidance advice. Contact Derm. 2019, 80, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Boonchai, W.; Maneeprasopchoke, P.; Chaweekulrat, P.; Kasemsarn, P. Associated factors of widespread pattern of dermatitis among patch test population: 12-Year retrospective study. Australas. J. Derm. 2019, 60, e40–e45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aerts, O.; De Fré, C.; van Hoof, T.; Ghys, K.; Ortopelea, R.A.; Lambert, J. “Slime”: A new fashion among children causing severe hand dermatitis. Contact Derm. 2018, 79, 385–387. [Google Scholar] [CrossRef] [PubMed]
- Ducharme, O.; Labadie, M.; Briand, S.M.; Milpied, B. Allergic contact dermatitis in a child caused by isothiazolinones in a “noise putty”. Contact Derm. 2018, 79, 393–394. [Google Scholar] [CrossRef]
- Alipour Tehrany, Y.; Quenan, S.; Bugey, A.; Piletta, P. Contact dermatitis caused by homemade “slime”: Report of two cases with chemical analysis. Contact Derm. 2019, 80, 407–408. [Google Scholar] [CrossRef]
- Salman, A.; Demir, G.; Apti, O. “Slime”: A trending cause of isothiazolinone contact allergy in children. Contact Derm. 2019, 80, 409–411. [Google Scholar] [CrossRef]
- Zhang, A.J.; Boyd, A.H.; Asch, S.; Warshaw, E.M. Allergic contact dermatitis to slime: The epidemic of isothiazolinone allergy encompasses school glue. Pediatr. Derm. 2019, 36, e37–e38. [Google Scholar] [CrossRef] [Green Version]
- Vincenzi, C.; Ravaioli, G.M.; Lambertini, M.; Guicciardi, F.; Piraccini, B.M.; Bardazzi, F.; La Placa, M. Allergic contact dermatitis caused by glitter glue used as make-up containing methylchloroisothiazolinone. Contact Derm. 2019, 80, 128–130. [Google Scholar] [CrossRef] [PubMed]
- Mamodaly, M.; Dereure, O.; Raison-Peyron, N. A new source for isothiazolinone contact allergy in traditional, non-digital photography. Contact Derm. 2019, 81, 76–77. [Google Scholar] [CrossRef] [PubMed]
- Sandvik, A.; Holm, J.-Ø. Severe allergic contact dermatitis in a detergent production worker caused by exposure to methylisothiazolinone. Contact Derm. 2019, 80, 243–245. [Google Scholar] [CrossRef] [PubMed]
- Maillard, A.; Quenan, S.; Piletta-Zanin, P.-A. Occupational contact dermatitis caused by benzylisothiazolinone in two fragrance industry workers. Contact Derm. 2019, 81, 140–141. [Google Scholar] [CrossRef] [PubMed]
- Hamnerius, N.; Pontén, A.; Mowitz, M. Textile contact dermatitis caused by octylisothiazolinone in compression stockings. Contact Derm. 2018, 78, 419–421. [Google Scholar] [CrossRef] [PubMed]
- Alipour Tehrany, Y.; Quenan, S.; Bugey, A.; Piletta, P. Allergic contact dermatitis caused by octylisothiazolinone in a leather sofa. Contact Derm. 2018, 79, 188–189. [Google Scholar] [CrossRef] [PubMed]
- Felmingham, C.; Nixon, R.; Palmer, A.; Lee, A. Allergic contact dermatitis caused by benzisothiazolinone in a continuous positive airway pressure mask liquid soap. Contact Derm. 2019, 81, 152–153. [Google Scholar] [CrossRef]
- Kerre, S.; Naessens, T.; Theunis, M.; Foubert, K.; Goossens, A.; Aerts, O. Facial dermatitis caused by undeclared methylisothiazolinone in a gel mask: Is the preservation of raw materials in cosmetics a cause of concern? Contact Derm. 2018, 78, 421–424. [Google Scholar] [CrossRef]
- Dendooven, E.; Foubert, K.; Naessens, T.; Pieters, L.; Lambert, J.; Aerts, O. Periocular contact allergy from spectacle frames cleaned with methylisothiazolinone-containing household detergents. J. Eur. Acad. Derm. Venereol. 2019, 33, e412–e413. [Google Scholar] [CrossRef]
- Franken, S.M.; van der Waal, R.I.F.; Rustemeyer, T. Occupational contact dermatitis caused by “Chrysal flower food”. Contact Derm. 2019, 81, 400–401. [Google Scholar] [CrossRef]
- Santiago, L.; Gonçalo, M. Occupational allergic contact dermatitis caused by acticide MV, a brand name for the mixture methylchloroisothiazolinone/methylisothiazolinone. Contact Derm. 2018, 79, 46–47. [Google Scholar] [CrossRef] [PubMed]
- Gallo, R.; Gariazzo, L.; Gasparini, G.; Basso, D.; Torino, A.; Cozzani, E.; Parodi, A. Contact allergy caused by methylisothiazolinone in a mouthwash as the likely trigger of oral pemphigus vulgaris. Contact Derm. 2018, 79, 104–105. [Google Scholar] [CrossRef] [PubMed]
- Linauskienė, K.; Isaksson, M. Allergic contact dermatitis from formaldehyde mimicking impetigo and initiating rosacea. Contact Derm. 2018, 78, 359–361. [Google Scholar] [CrossRef] [PubMed]
- Nikle, A.; Ericson, M.; Warshaw, E. Formaldehyde release from personal care products: Chromotropic acid method analysis. Dermatitis 2019, 30, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Fasth, I.M.; Ulrich, N.H.; Johansen, J.D. Ten-year trends in contact allergy to formaldehyde and formaldehyde-releasers. Contact Derm. 2018, 79, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Liou, Y.L.; Schlarbaum, J.P.; Kimyon, R.S.; Hylwa, S.A. Formaldehyde in hypoallergenic household gloves. Dermatitis 2019, 30, 75–77. [Google Scholar] [CrossRef]
- Voller, L.M.; Persson, L.; Bruze, M.; Ericson, M.E.; Hylwa, S.A. Formaldehyde in “Nontoxic” nail polish. Dermatitis 2019, 30, 259–263. [Google Scholar] [CrossRef]
- Ham, J.E.; Siegel, P.D.; Maibach, H. Undeclared formaldehyde levels in patient consumer products: Formaldehyde test kit utility. Cutan. Ocul. Toxicol. 2019, 38, 112–117. [Google Scholar] [CrossRef]
- Wilkinson, M.; Gonçalo, M.; Aerts, O.; Badulici, S.; Bennike, N.H.; Bruynzeel, D.; Dickel, H.; Garcia-Abujeta, J.L.; Giménez-Arnau, A.M.; Hamman, C.; et al. The European baseline series and recommended additions: 2019. Contact Derm. 2019, 80, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Borges, A.S.; Valejo Coelho, M.M.; Fernandes, C.; Brasileiro, A.; Gonçalo, M. Systemic allergic dermatitis caused by sodium metabisulfite in rectal enemas. Contact Derm. 2018, 78, 429–430. [Google Scholar] [CrossRef]
- Guha-Niyogi, B.; Sabroe, R.; Holden, C. An unusual case of a systemic delayed hypersensitivity reaction to sodium metabisulfite. Contact Derm. 2018, 79, 246–247. [Google Scholar] [CrossRef]
- Raison-Peyron, N.; Roulet, A.; Dereure, O. Occupational allergic contact dermatitis caused by sulfite in a seafood section worker of a supermarket. Contact Derm. 2019, 80, 412–414. [Google Scholar] [CrossRef] [PubMed]
- Schlarbaum, J.P.; Kimyon, R.S.; Liou, Y.L.; Voller, L.M.; Seyfer, S.J.; Warshaw, E.M. Hold the spice: Allergy to garlic and sulfites-possible relevance in a patient with cheilitis granulomatosa. Contact Derm. 2019, 81, 397–398. [Google Scholar] [CrossRef] [PubMed]
- Foley, C.C.; White, S.; Merry, S.; Nolan, U.; Moriarty, B.; Kirby, B.; Collins, P.; Lally, A. Understanding the role of cutaneous allergy testing in anogenital dermatoses: A retrospective evaluation of contact sensitization in anogenital dermatoses. Int. J. Derm. 2019, 58, 806–810. [Google Scholar] [CrossRef] [PubMed]
- Fransway, A.F.; Fransway, P.J.; Belsito, D.V.; Warshaw, E.M.; Sasseville, D.; Fowler, J.F.; DeKoven, J.G.; Pratt, M.D.; Maibach, H.I.; Taylor, J.S.; et al. Parabens. Dermatitis 2019, 30, 3–31. [Google Scholar] [CrossRef]
- Assier, H.; Wolkenstein, P.; Chosidow, O. Very late sensitization to parabens induced by repeated applications of an anaesthetic therapeutic plaster to non-damaged skin. Contact Dermat. 2018, 79, 194–195. [Google Scholar] [CrossRef]
- Aschenbeck, K.A.; Warshaw, E.M. Clinically relevant reactions to thimerosal (the “Nonallergen”) exist! Dermatitis 2018, 29, 44–45. [Google Scholar] [CrossRef]
- Zhang, A.J.; Boyd, A.H.; Schlarbaum, J.P.; Warshaw, E.M. Allergic contact dermatitis secondary to the use of a bandage impregnated with benzalkonium chloride. Contact Derm. 2018, 79, 387–388. [Google Scholar] [CrossRef]
- Herman, A.; Goossens, A.; Tennstedt, D.; Bergendorff, O.; Isaksson, M.; Mowitz, M.; Baeck, M. The preservative 2-(thiocyanomethylthio)benzothiazole: A potential allergen in leather products. Contact Derm. 2019, 81, 262–265. [Google Scholar] [CrossRef]
- Dittmar, D.; Schuttelaar, M.L. Comparing patch test results of methylchloroisothiazolinone/methylisothiazolinone tested with both TRUE Test® and 100 ppm using investigator-loaded chambers. Contact Derm. 2018, 78, 159–161. [Google Scholar] [CrossRef] [Green Version]
- Heratizadeh, A.; Werfel, T.; Schubert, S.; Geier, J. IVDK Contact sensitization in dental technicians with occupational contact dermatitis. Data of the information network of departments of dermatology (IVDK) 2001–2015. Contact Derm. 2018, 78, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Gonçalo, M.; Pinho, A.; Agner, T.; Andersen, K.E.; Bruze, M.; Diepgen, T.; Foti, C.; Giménez-Arnau, A.; Goossens, A.; Johanssen, J.D.; et al. Allergic contact dermatitis caused by nail acrylates in Europe. An EECDRG study. Contact Derm. 2018, 78, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Stingeni, L.; Tramontana, M.; Bianchi, L.; Foti, C.; Patruno, C.; Gallo, R.; Corazza, M.; Schena, D.; Milanesi, N.; Guarneri, F.; et al. Contact sensitivity to 2-hydroxyethyl methacrylate in consecutive patients: A 1-year multicentre SIDAPA study. Contact Derm. 2019, 81, 216–218. [Google Scholar] [CrossRef] [PubMed]
- Fisch, A.; Hamnerius, N.; Isaksson, M. Dermatitis and occupational (meth)acrylate contact allergy in nail technicians-A 10-year study. Contact Derm. 2019, 81, 58–60. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, M.; Hanada, M.; Amano, H. Occupational contact dermatitis in a manicurist. J. Derm. 2019, 46, 1039–1041. [Google Scholar] [CrossRef]
- Nedeva, D.; Petkova, E.; Valerieva, A.; Uzunov, S.; Krusheva, B.; Staevska, M. Airborne contact dermatitis and hand eczema caused by 2-Hydroxyethylmethacrylate (2-Hema)-case report of occupational contact allergy. Allergy 2019, 74, 499. [Google Scholar]
- Gatica-Ortega, M.-E.; Pastor-Nieto, M.-A.; Gil-Redondo, R.; Martínez-Lorenzo, E.-R.; Schöendorff-Ortega, C. Non-occupational allergic contact dermatitis caused by long-lasting nail polish kits for home use: “the tip of the iceberg”. Contact Derm. 2018, 78, 261–265. [Google Scholar] [CrossRef]
- Lee, S.; Maor, D.; Palmer, A.; Nixon, R.L. Declining prevalence of allergic contact dermatitis caused by toslyamide/formaldehyde in nail polish. Contact Derm. 2018, 79, 184–185. [Google Scholar] [CrossRef]
- Mukaijo, J.; Inomata, N.; Higashihira, M.; Koh, N.; Togashi, Y.; Asai, C.; Watanabe, Y.; Kurihara, S.; Aihara, M. Allergic contact dermatitis caused by 2-hydroxyethyl acrylate in a moisturizing face pack in a handmade acrylic accessory enthusiast. Contact Derm. 2018, 79, 383–385. [Google Scholar] [CrossRef]
- Alamri, A.; Lill, D.; Summer, B.; Thomas, P.; Thomas, B.; Oppel, E. Artificial nail wearing: Unexpected elicitor of allergic contact dermatitis, oral lichen planus and risky arthroplasty. Contact Derm. 2019, 81, 210–211. [Google Scholar] [CrossRef]
- McCarthy, S.; Flynn, A.; Bennett, M.; Bourke, J.F. It’s not lupus, it’s your nails! Contact Derm. 2019, 80, 67–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgado, F.; Batista, M.; Gonçalo, M. Short exposures and glove protection against (meth)acrylates in nail beauticians-thoughts on a rising concern. Contact Dermat. 2019, 81, 62–63. [Google Scholar] [CrossRef] [PubMed]
- Lambertini, M.; Vincenzi, C.; Lorenzi, S.; Piraccini, B.M.; La Placa, M. Allergic contact dermatitis caused by triethylenetetramine: The glue is the clue. Contact Derm. 2018, 78, 416–417. [Google Scholar] [CrossRef] [PubMed]
- Sasseville, D.; Shamout, Y.; Moreau, L. Occupational allergic contact dermatitis caused by hexahydrophthalic acid diglycidyl ester and anhydride epoxy hardeners. Contact Derm. 2018, 79, 39–40. [Google Scholar] [CrossRef] [PubMed]
- Loranger, C.; Moreau, L.; Sasseville, D. Occupational contact dermatitis in the canadian aircraft industry. Dermatitis 2018, 29, 139–150. [Google Scholar] [CrossRef]
- Suuronen, K.; Bäck, B.; Aalto-Korte, K.; Pesonen, M.; Jungewelter, S.; Henriks-Eckerman, M.-L.; Mäkelä, E. Skin exposure to epoxy chemicals in construction coating, assessed by observation, interviews, and measurements. Contact Derm. 2019, 80, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Oosterhaven, J.A.F.; Uter, W.; Aberer, W.; Armario-Hita, J.C.; Ballmer-Weber, B.K.; Bauer, A.; Czarnecka-Operacz, M.; Elsner, P.; García-Gavín, J.; Giménez-Arnau, A.M.; et al. European surveillance system on contact allergies (ESSCA): Contact allergies in relation to body sites in patients with allergic contact dermatitis. Contact Derm. 2019, 80, 263–272. [Google Scholar] [CrossRef] [Green Version]
- Brans, R.; Schröder-Kraft, C.; Skudlik, C.; John, S.M.; Geier, J. Tertiary prevention of occupational skin diseases: Prevalence of allergic contact dermatitis and pattern of patch test results. Contact Derm. 2019, 80, 35–44. [Google Scholar] [CrossRef] [Green Version]
- Geier, J.; Amschler, K.; Claßen, A.; Buhl, T. Sensitization to diphenylmethane-diisocyanate isomers by a single accidental exposure. Contact Derm. 2018, 78, 90–92. [Google Scholar] [CrossRef]
- Castelain, F.; Girardin, P.; Penven, E.; Pelletier, F. Occupational contact dermatitis caused by polyurethane foam: 6 cases. Contact Derm. 2018, 79, 52–54. [Google Scholar] [CrossRef]
- Aizawa, A.; Ito, A.; Masui, Y.; Sasaki, K.; Ishimura, Y.; Numata, M.; Abe, R. A case of allergic contact dermatitis caused by goalkeeper gloves. Contact Derm. 2018, 79, 113–115. [Google Scholar] [CrossRef] [PubMed]
- Aalto-Korte, K.; Suuronen, K. Occupational allergic contact dermatitis caused by phenol formaldehyde resin in an interior coating for beverage cans. Contact Derm. 2019, 80, 134–135. [Google Scholar] [CrossRef] [PubMed]
- Shono, M.; Numata, M.; Sasaki, K. Allergic contact dermatitis caused by Solvent Orange 60 in spectacle frames in Japan. Contact Derm. 2018, 78, 83–84. [Google Scholar] [CrossRef]
- Linauskienė, K.; Zimerson, E.; Antelmi, A.; Bruze, M.; Hagvall, L.; Hamnerius, N.; Hauksson, I.; Ryberg, K.; Isaksson, M. Solvent orange 60 is a potent contact sensitizer in occupational and everyday life. Contact Derm. 2018, 79, 123–126. [Google Scholar] [CrossRef]
- Hald, M.; Bergendorff, O.; Isaksson, M.; Johansen, J.D. Allergic contact dermatitis caused by plastic items containing the ultraviolet absorber drometrizole. Contact Derm. 2018, 79, 110–112. [Google Scholar] [CrossRef]
- Hamnerius, N.; Svedman, C.; Bergendorff, O.; Björk, J.; Bruze, M.; Engfeldt, M.; Pontén, A. Hand eczema and occupational contact allergies in healthcare workers with a focus on rubber additives. Contact Derm. 2018, 79, 149–156. [Google Scholar] [CrossRef]
- Crépy, M.-N.; Lecuen, J.; Ratour-Bigot, C.; Stocks, J.; Bensefa-Colas, L. Accelerator-free gloves as alternatives in cases of glove allergy in healthcare workers. Contact Derm. 2018, 78, 28–32. [Google Scholar] [CrossRef]
- Fustà-Novell, X.; Gómez-Armayones, S.; Morgado-Carrasco, D.; Mascaró, J.M. Systemic allergic dermatitis caused by disulfiram (Antabuse) in a patient previously sensitized to rubber accelerators. Contact Derm. 2018, 79, 239–240. [Google Scholar] [CrossRef]
- Hamann, D.; Sköld, M.B.; Hamann, C.R.; Thyssen, J.P. Thiuram allergic contact dermatitis on the hands after skin contact with a rubber cellphone case. Contact Derm. 2019, 80, 130–131. [Google Scholar] [CrossRef]
- Goodier, M.C.; Ronkainen, S.D.; Hylwa, S.A. Rubber accelerators in medical examination and surgical gloves. Dermatitis 2018, 29, 66–76. [Google Scholar] [CrossRef]
- Hamnerius, N.; Pontén, A.; Björk, J.; Persson, C.; Bergendorff, O. Skin exposure to the rubber accelerator diphenylguanidine in medical gloves-an experimental study. Contact Derm. 2019, 81, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Isaac, J.; Goldminz, A.M.; Scheinman, P.L. Don’t forget the sponge. Contact Derm. 2019, 81, 149–150. [Google Scholar] [CrossRef] [PubMed]
- Dejonckheere, G.; Herman, A.; Baeck, M. Allergic contact dermatitis caused by synthetic rubber gloves in healthcare workers: Sensitization to 1,3-diphenylguanidine is common. Contact Derm. 2019, 81, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Leuzzi, M.; Vincenzi, C.; Sechi, A.; Tomasini, C.; Giuri, D.; Piraccini, B.M.; La Placa, M. Delayed hypersensitivity to natural rubber latex: Does it exist or not? Contact Derm. 2019, 81, 404–405. [Google Scholar] [CrossRef] [PubMed]
- Mercader-García, P.; Pastor-Nieto, M.A.; García-Doval, I.; Giménez-Arnau, A.; González-Pérez, R.; Fernández-Redondo, V.; Serra-Baldrich, E.; Cordoba-Guijarro, S.; Gatica-Ortega, M.E.; Silvestre-Salvador, J.F.; et al. Are the Spanish baseline series markers sufficient to detect contact allergy to corticosteroids in Spain? A GEIDAC prospective study. Contact Derm. 2018, 78, 76–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos-Alarcón, S.; Benavente-Villegas, F.-C.; Farzanegan-Miñano, R.; Pérez-Francés, C.; Sánchez-Motilla, J.-M.; Mateu-Puchades, A. Delayed hypersensitivity to topical and systemic corticosteroids. Contact Derm. 2018, 78, 86–88. [Google Scholar] [CrossRef]
- Ljubojević Hadžavdić, S.; Gojčeta Burnić, S.; Hadžavdić, A.; Marinović Kulišić, S.; Jurakić Tončić, R. Erythema of the penis after use of a latex condom—Latex allergy or something else? Contact Derm. 2018, 78, 168–169. [Google Scholar] [CrossRef] [Green Version]
- Matos-Pires, E.; Pina-Trincão, D.; Brás, S.; Lobo, L. Baboon syndrome caused by anti-haemorrhoidal ointment. Contact Derm. 2018, 78, 170–171. [Google Scholar] [CrossRef]
- Forkel, S.; Baltzer, A.B.; Geier, J.; Buhl, T. Contact dermatitis caused by diltiazem cream and cross-reactivity with other calcium channel blockers. Contact Derm. 2018, 79, 244–246. [Google Scholar] [CrossRef]
- Flury, U.; Cahill, J.L.; Nixon, R.L. Occupational contact dermatitis caused by opioids: A case series. Contact Derm. 2019. [Google Scholar] [CrossRef]
- Corazza, M.; Amendolagine, G.; Musmeci, D.; Forconi, R.; Borghi, A. Sometimes even Dr Google is wrong: An unusual contact dermatitis caused by benzoyl peroxide. Contact Derm. 2018, 79, 380–381. [Google Scholar] [CrossRef] [PubMed]
- Gilissen, L.; Huygens, S.; Goossens, A. Allergic contact dermatitis caused by calcipotriol. Contact Derm. 2018, 78, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Lazzarini, R.; Hafner, M.F.S.; Miguel, B.A.F.; Kawakami, N.T.; Nakagome, B.H.Y. Allergic contact dermatitis caused by topical ketoconazole: A relevant issue? Review of ketoconazole-positive patch tests. Contact Derm. 2018, 78, 234–236. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Mesonero, R.; Schneller-Pavelescu, L.; Ochando-Ibernón, G.; Vergara-Sánchez, A.; Sánchez-Herreros, C.; Martín-Alcalde, E.; Gatica-Ortega, M.E.; Silvestre-Salvador, J.F.; Pastor-Nieto, M.A. Is tioconazole contact dermatitis still a concern? Bringing allergic contact dermatitis caused by topical tioconazole back into the spotlight. Contact Derm. 2019, 80, 168–169. [Google Scholar] [CrossRef]
- Ochando-Ibernón, G.; Schneller-Pavelescu, L.; Vergara de Caso, E.F.; Silvestre-Salvador, J.F. Allergic contact dermatitis caused by undecylenic acid in an antifungal nail solution. Contact Derm. 2019, 80, 313–314. [Google Scholar]
- Romita, P.; Stingeni, L.; Hansel, K.; De Prezzo, S.; Ambrogio, F.; Bonamonte, D.; Foti, C. Allergic contact dermatitis caused by amorolfine in a nail lacquer. Contact Derm. 2019, 81, 407–408. [Google Scholar] [CrossRef]
- Fernandes, R.A.; Santiago, L.; Gouveia, M.; Gonçalo, M. Allergic contact dermatitis caused by dexpanthenol-probably a frequent allergen. Contact Derm. 2018, 79, 276–280. [Google Scholar] [CrossRef]
- Sacchelli, L.; Vincenzi, C.; La Placa, M.; Piraccini, B.M.; Neri, I. Allergic contact dermatitis caused by timolol eyedrop application for infantile haemangioma. Contact Derm. 2019, 80, 255–256. [Google Scholar] [CrossRef]
- Pinheiro, V.; Pestana, C.; Pinho, A.; Antunes, I.; Gonçalo, M. Occupational allergic contact dermatitis caused by antibiotics in healthcare workers-relationship with non-immediate drug eruptions. Contact Derm. 2018, 78, 281–286. [Google Scholar] [CrossRef]
- Herrera-Mozo, I.; Sanz-Gallen, P.; Saéz, B.; Marti-Amengual, G. Occupational contact dermatitis caused by hydroxychloroquine sulfate. Contact Derm. 2018, 79, 102–103. [Google Scholar] [CrossRef]
- Veraldi, S.; Guanziroli, E.; Ferrucci, S.; Nazzaro, G. Allergic contact dermatitis caused by clindamycin. Contact Derm. 2019, 80, 68–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilissen, L.; De Decker, L.; Hulshagen, T.; Goossens, A. Allergic contact dermatitis caused by topical ophthalmic medications: Keep an eye on it! Contact Derm. 2019, 80, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Assier, H.; Hirsch, G.; Wolkenstein, P.; Chosidow, O. Severe contact allergy to mupirocin in a polysensitized patient. Contact Derm. 2019, 80, 397–398. [Google Scholar] [CrossRef] [PubMed]
- Veraldi, S.; Benzecry, V.; Faraci, A.G.; Nazzaro, G. Allergic contact dermatitis caused by paromomycin. Contact Derm. 2019, 81, 393–394. [Google Scholar] [CrossRef] [PubMed]
- Khalid, A.; Ghaffar, S. Two cases of occupational allergic contact dermatitis caused by abacavir. Contact Derm. 2019, 80, 187–188. [Google Scholar] [CrossRef]
- Zhang, A.J.; Warshaw, E.M. Pet Consort Dermatitis: The importance of asking about pets. Dermatitis 2018, 29, 45–46. [Google Scholar] [CrossRef]
- Scheers, C.; Dehavay, F.; Andre, J.; Neczyporenko, F.; Kolivras, A. A case of recalcitrant face eczema. Contact Derm. 2019, 80, 242–243. [Google Scholar] [CrossRef]
- Toma, N.; Horst, N.; Dandelooy, J.; Romaen, E.; Leysen, J.; Aerts, O. Contact allergy caused by stannous fluoride in toothpaste. Contact Derm. 2018, 78, 304–306. [Google Scholar] [CrossRef]
- Boonstra, M.; Rustemeyer, T.; Middelkamp-Hup, M.A. Both children and adult patients with difficult-to-treat atopic dermatitis have high prevalences of concomitant allergic contact dermatitis and are frequently polysensitized. J. Eur. Acad. Derm. Venereol. 2018, 32, 1554–1561. [Google Scholar] [CrossRef] [Green Version]
- Fransen, M.; Overgaard, L.E.K.; Johansen, J.D.; Thyssen, J.P. Contact allergy to lanolin: Temporal changes in prevalence and association with atopic dermatitis. Contact Derm. 2018, 78, 70–75. [Google Scholar] [CrossRef]
- Uter, W.; Schnuch, A.; Geier, J. IVDK Contact sensitization to lanolin alcohols and Amerchol® L101-analysis of IVDK data. Contact Derm. 2018, 78, 367–369. [Google Scholar] [CrossRef] [PubMed]
- Knijp, J.; Bruynzeel, D.P.; Rustemeyer, T. Diagnosing lanolin contact allergy with lanolin alcohol and Amerchol L101. Contact Derm. 2019, 80, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Miroux-Catarino, A.; Silva, L.; Amaro, C.; Viana, I. Allergic contact dermatitis caused dexpanthenol—But is that all? Contact Derm. 2019, 81, 391–392. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Chinchilla, P.; Poveda-Montoyo, I.; González, I.; Silvestre, J.F. Cetearyl isononanoate, an underestimated contact allergen? Contact Derm. 2018, 79, 243–244. [Google Scholar] [CrossRef]
- Özkaya, E.; Kılıç, S. Polyethylene glycol as marker for nitrofurazone allergy: 20 years of experience from Turkey. Contact Derm. 2018, 78, 211–215. [Google Scholar] [CrossRef]
- Kerre, S.; Strobbe, T.; Naessens, T.; Theunis, M.; Foubert, K.; Aerts, O. Alkyl glucosides: Newly identified allergens in foam wound dressings. Contact Derm. 2018, 79, 191–193. [Google Scholar] [CrossRef]
- Schlarbaum, J.P.; Liou, Y.L.; Kimyon, R.S.; Olson, C.L.; Warshaw, E.M. Oh my glucosides! Occult sources in medical products. Dermatitis 2019, 30, 228–230. [Google Scholar] [CrossRef]
- Assier, H.; Tetart, F.; Avenel-Audran, M.; Barbaud, A.; Ferrier-le Boueedec, M.-C.; Giordano-Labadie, F.; Milpied, B.; Amsler, E.; Collet, E.; Girardin, P.; et al. Is a specific eyelid patch test series useful? Results of a french prospective study. Contact Dermat. 2018, 79, 157–161. [Google Scholar] [CrossRef]
- Boucneau, F.; Goossens, A.; Huygens, S.; Gilissen, L. Arachidyl glucoside: Another cosmetic allergen. Contact Derm. 2018, 79, 321–323. [Google Scholar] [CrossRef]
- Bhoyrul, B.; Solman, L.; Kirk, S.; Orton, D.; Wilkinson, M. Patch testing with alkyl glucosides: Concomitant reactions are common but not ubiquitous. Contact Derm. 2019, 80, 286–290. [Google Scholar] [CrossRef]
- Scheman, A.; Te, R. Contact allergy to cocamide diethanolamine and cross-reactions. Dermatitis 2018, 29, 91–92. [Google Scholar] [CrossRef] [PubMed]
- Mamodaly, M.; Dereure, O.; Raison-Peyron, N. A new case of allergic contact dermatitis caused by 3-o-ethyl ascorbic acid in facial antiageing cosmetics. Contact Derm. 2019, 81, 315–316. [Google Scholar] [CrossRef] [PubMed]
- Dens, A.-C.; Goossens, A.; Darcis, J.; Huygens, S.; Lambrecht, C.; Gilissen, L. Allergic contact dermatitis caused by ethylhexyl salicylate with possible cross-reactivity with benzyl salicylate. Contact Derm. 2019, 81, 317–318. [Google Scholar] [CrossRef]
- Sánchez-Herrero, A.; Mateos-Mayo, A.; Rodríguez-Lomba, E.; Molina-López, I.; Campos-Domínguez, M.; Suárez Fernández, R. Allergic contact cheilitis in an adolescent to ricinus communis seed oil (castor oil) in a lip balm. Contact Derm. 2018, 79, 176–178. [Google Scholar] [CrossRef] [PubMed]
- Nishioka, K.; Koizumi, A.; Takita, Y. Allergic contact dermatitis caused by cysteamine hydrochloride in permanent wave agent—A new allergen for hairdressers in Japan. Contact Derm. 2019, 80, 174–175. [Google Scholar] [CrossRef]
- Herman, A.; Goossens, A. The need to disclose the composition of medical devices at the European level. Contact Derm. 2019, 81, 159–160. [Google Scholar] [CrossRef]
- Raison-Peyron, N.; Mowitz, M.; Bonardel, N.; Aerts, O.; Bruze, M. Allergic contact dermatitis caused by isobornyl acrylate in OmniPod, an innovative tubeless insulin pump. Contact Derm. 2018, 79, 76–80. [Google Scholar] [CrossRef]
- Oppel, E.; Högg, C.; Summer, B.; Ruëff, F.; Reichl, F.-X.; Kamann, S. Isobornyl acrylate contained in the insulin patch pump OmniPod as the cause of severe allergic contact dermatitis. Contact Derm. 2018, 79, 178–180. [Google Scholar] [CrossRef]
- Corazza, M.; Scuderi, V.; Musmeci, D.; Foti, C.; Romita, P.; Borghi, A. Allergic contact dermatitis caused by isobornyl acrylate in a young diabetic patient using a continous glucose monitoring system (FreeStyle Libre). Contact Derm. 2018, 79, 320–321. [Google Scholar] [CrossRef]
- Herman, A.; de Montjoye, L.; Tromme, I.; Goossens, A.; Baeck, M. Allergic contact dermatitis caused by medical devices for diabetes patients: A review. Contact Derm. 2018, 79, 331–335. [Google Scholar] [CrossRef] [Green Version]
- Hyry, H.S.I.; Liippo, J.P.; Virtanen, H.M. Allergic contact dermatitis caused by glucose sensors in type 1 diabetes patients. Contact Derm. 2019, 81, 161–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jáuregui, I.; Sánchez, J.; Segurola, A.; Galán, C.; Seras, Y.; Gamboa, P.M. Allergic contact dermatitis by isobornyl acrylate in glucose monitoring devices: Report of two cases. Contact Derm. 2019, 81, 219–220. [Google Scholar] [CrossRef] [PubMed]
- Kamann, S.; Aerts, O.; Heinemann, L. Further evidence of severe allergic contact dermatitis from isobornyl acrylate while using a continuous glucose monitoring system. J. Diabetes Sci. Technol. 2018, 12, 630–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mowitz, M.; Herman, A.; Baeck, M.; Isaksson, M.; Antelmi, A.; Hamnerius, N.; Pontén, A.; Bruze, M. N,N-dimethylacrylamide—A new sensitizer in the FreeStyle Libre glucose sensor. Contact Derm. 2019, 81, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Passanisi, S.; Lombardo, F.; Barbalace, A.; Caminiti, L.; Panasiti, I.; Crisafulli, G.; Salzano, G.; Pajno, G.B. Allergic contact dermatitis and diabetes medical devices: 2 clinical cases. Contact Derm. 2018, 79, 115–117. [Google Scholar] [CrossRef]
- Oppel, E.; Kamann, S.; Reichl, F.-X.; Högg, C. The Dexcom glucose monitoring system—An isobornyl acrylate-free alternative for diabetic patients. Contact Derm. 2019, 81, 32–36. [Google Scholar] [CrossRef] [Green Version]
- Kamann, S.; Oppel, E.; Liu, F.; Reichl, F.-X.; Heinemann, L.; Högg, C. Evaluation of isobornyl acrylate content in medical devices for diabetes treatment. Diabetes Technol. 2019, 21, 533–537. [Google Scholar] [CrossRef]
- Shinkawa, E.; Washio, K.; Tatsuoka, S.; Fukunaga, A.; Sakaguchi, K.; Nishigori, C. A case of contact dermatitis caused by isobornyl acrylate in FreeStyle Libre: The usefulness of film-forming agents. Contact Derm. 2019, 81, 56–57. [Google Scholar] [CrossRef]
- Kamann, S.; Oppel, E. Hydrocolloid blister plaster decreases allergic contact dermatitis caused by Freestyle Libre and isobornyl acrylate. Contact Derm. 2019, 81, 380–381. [Google Scholar] [CrossRef]
- Herman, A.; Mowitz, M.; Aerts, O.; Pyl, J.; de Montjoye, L.; Goossens, A.; Bruze, M.; Baeck, M. Unexpected positive patch test reactions to sesquiterpene lactones in patients sensitized to the glucose sensor FreeStyle Libre. Contact Derm. 2019, 81, 354–367. [Google Scholar] [CrossRef]
- Mestach, L.; Huygens, S.; Goossens, A.; Gilissen, L. Allergic contact dermatitis caused by acrylic-based medical dressings and adhesives. Contact Dermat. 2018, 79, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Garval, E.; Plee, J.; Lesage, C.; Grange-Prunier, A.; Bernard, P.; Perceau, G. Frequency of contact sensitization to modern dressings used to treat chronic leg ulcer. Ann. Derm. Venereol. 2018, 145, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Foti, C.; Lopalco, A.; Stingeni, L.; Hansel, K.; Lopedota, A.; Denora, N.; Romita, P. Contact allergy to electrocardiogram electrodes caused by acrylic acid without sensitivity to methacrylates and ethyl cyanoacrylate. Contact Derm. 2018, 79, 118–121. [Google Scholar] [CrossRef] [PubMed]
- Caroppo, F.; Brumana, M.B.; Biolo, G.; Giorato, E.; Barbierato, M.; Belloni Fortina, A. Peristomal allergic contact dermatitis caused by ostoma pastes and role of Gantrez ES-425. G. Ital. Derm. Venereol. 2019, 154, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Milanesi, N.; Gola, M.; Francalanci, S. Allergic contact dermatitis caused by a polyurethane catheter. Contact Derm. 2018, 79, 313–314. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Wan, J.; McKenna, R.A.; Jackson, O.A.; Treat, J.R. Allergic contact dermatitis caused by dermabond in a paediatric patient undergoing skin surgery. Contact Derm. 2019, 80, 61–62. [Google Scholar] [CrossRef] [Green Version]
- Cook, K.A.; White, A.A.; Shaw, D.W. Patch testing ingredients of dermabond and other cyanoacrylate-containing adhesives. Dermatitis 2019, 30, 314–322. [Google Scholar] [CrossRef]
- Watts, T.J.; Thursfield, D.; Haque, R. Allergic contact dermatitis caused by VenaSeal tissue adhesive. Contact Derm. 2019, 80, 393–395. [Google Scholar] [CrossRef]
- Schuttelaar, M.L.; Meijer, J.M.; Engfeldt, M.; Lapeere, H.; Goossens, A.; Bruze, M.; Persson, C.; Bergendorff, O. Allergic contact dermatitis caused by dimethylthiocarbamylbenzothiazole sulfide (DMTBS) in canvas shoes: In search of the culprit allergen. Contact Derm. 2018, 78, 7–11. [Google Scholar] [CrossRef]
- Hulstaert, E.; Bergendorff, O.; Persson, C.; Goossens, A.; Gilissen, L.; Engfeldt, M.; Bruze, M.; Schuttelaar, M.L.; Meijer, J.M.; Lapeere, H. Contact dermatitis caused by a new rubber compound detected in canvas shoes. Contact Derm. 2018, 78, 12–17. [Google Scholar] [CrossRef]
- Ota, A.; Takehara, Y.; Okawa, T.; Ikegami, R.; Sasaki, K.; Numata, M. Contact allergy to Tinuvin 770, a hindered amine light stabilizer in sandals contributing to hyperkeratotic foot dermatitis. Contact Derm. 2019, 81, 288–290. [Google Scholar] [CrossRef] [PubMed]
- Koumaki, D.; Bergendorff, O.; Bruze, M.; Orton, D. Allergic contact dermatitis to shin pads in a hockey player: acetophenone is an emerging allergen. Dermatitis 2019, 30, 162–163. [Google Scholar] [CrossRef] [PubMed]
- Darrigade, A.S.; Raison-Peyron, N.; Courouge-Dorcier, D.; Vital-Durand, D.; Milpied, B.; Giordano-Labadie, F.; Aerts, O. The chemical acetophenone azine: An important cause of shin and foot dermatitis in children. J. Eur. Acad. Derm. Venereol. 2019, 34, e61–e62. [Google Scholar] [CrossRef] [PubMed]
- Hedberg, Y.S.; Uter, W.; Banerjee, P.; Lind, M.-L.; Skovvang Steengaard, S.; Teo, Y.; Lidén, C. Non-oxidative hair dye products on the european market: What do they contain? Contact Derm. 2018, 79, 281–287. [Google Scholar] [CrossRef]
- Schubert, S.; Lessmann, H.; Schnuch, A.; Uter, W.; Geier, J. IVDK Factors associated with p-phenylenediamine sensitization: Data from the information network of departments of dermatology, 2008–2013. Contact Derm. 2018, 78, 199–207. [Google Scholar] [CrossRef] [Green Version]
- Schuttelaar, M.L.A.; van Amerongen, C.C.A.; Lichter, J.; Blömeke, B. Evaluation of risk modification for p-phenylenediamine sensitization by N-acetyltransferase 1 and 2 for two highly sensitive cases. Contact Derm. 2019, 81, 138–140. [Google Scholar] [CrossRef]
- Romita, P.; Foti, C.; Mascia, P.; Guida, S. Eyebrow allergic contact dermatitis caused by m-aminophenol and toluene-2,5-diamine secondary to a temporary black henna tattoo. Contact Derm. 2018, 79, 51–52. [Google Scholar] [CrossRef]
- Assier, H.; Wolkenstein, P.; Chosidow, O. Beard dermatitis induced by coloration. Contact Derm. 2019, 81, 471–473. [Google Scholar] [CrossRef]
- Corazza, M.; Amendolagine, G.; Toni, G.; Mantovani, L.; Borghi, A. Side-effects of tango: Connubial contact dermatitis. Contact Derm. 2019, 80, 241–242. [Google Scholar] [CrossRef]
- Ferreira, C.; Rezende, I.; Guilherme, A.; Rosmaninho, I.; Lopes, I. Allergic contact connubial dermatitis caused by hair products. Contact Derm. 2019, 80, 186–187. [Google Scholar] [CrossRef]
- Young, E.; Andersen, K.E.; Bruze, M.; Giménez-Arnau, A.; Ross-Hansen, K.; Johansen, J.D.; Madsen, J.T.; Zimerson, E.; Svedman, C. Twenty-eight-day follow-up of patch test reactions to p-phenylenediamine and p-phenylenediamine dihydrochloride: A multicentre study on behalf of the european environmental and contact dermatitis research group. Contact Derm. 2019, 81, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, T.; Sabroe, R.; Holden, C. Allergic contact dermatitis caused by 1-naphthol, a red coupler, in a purple permanent oxidative hair dye. Contact Derm. 2018, 79, 99–100. [Google Scholar] [CrossRef] [PubMed]
- Schuttelaar, M.L.; Dittmar, D.; Burgerhof, J.G.M.; Bloemeke, B.; Goebel, C. Cross-elicitation responses to 2-methoxymethyl-p-phenylenediamine in p-phenylenediamine-allergic individuals: Results from open use testing and diagnostic patch testing. Contact Dermat. 2018, 79, 288–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ameur, K.; Youssef, M.; Belhadjali, H.; Soua, Y.; Korbi, M.; Henchi, M.A.; Zili, J. Occupational acute generalized exanthematous pustulosis induced by disperse dyes in a textile. Contact Derm. 2019, 80, 411–412. [Google Scholar] [CrossRef]
- Bil, W.; van der Bent, S.A.S.; Spiekstra, S.W.; Nazmi, K.; Rustemeyer, T.; Gibbs, S. Comparison of the skin sensitization potential of 3 red and 2 black tattoo inks using interleukin-18 as a biomarker in a reconstructed human skin model. Contact Derm. 2018, 79, 336–345. [Google Scholar] [CrossRef]
- Van der Bent, S.A.S.; Berg, T.; Karst, U.; Sperling, M.; Rustemeyer, T. Allergic reaction to a green tattoo with nickel as a possible allergen. Contact Derm. 2019, 81, 64–66. [Google Scholar] [CrossRef] [Green Version]
- Bauer, A.; Geier, J.; Schreiber, S.; Schubert, S. IVDK Contact sensitization to plants of the Compositae family: Data of the information network of departments of dermatology (IVDK) from 2007 to 2016. Contact Derm. 2019, 80, 222–227. [Google Scholar] [CrossRef]
- Paulsen, E.; Andersen, K.E. Screening for compositae contact sensitization with sesquiterpene lactones and compositae mix 2.5% pet. Contact Derm. 2019, 81, 368–373. [Google Scholar] [CrossRef]
- Zawar, V.; Daga, S.; Pawar, M.; Kumavat, S. “Chaturthy fingers” caused by hibiscus rosasinensis. Contact Derm. 2018, 78, 161–162. [Google Scholar] [CrossRef]
- Lin, N.; Tang, X.; Zhou, H.; Han, J. Erythema multiforme-like contact dermatitis caused by herbal medicine. Contact Derm. 2019, 80, 189–190. [Google Scholar] [CrossRef]
- Romita, P.; Calogiuri, G.; Bellino, M.; De Prezzo, S.; Ambrogio, F.; Foti, C. Allergic contact dermatitis caused by neem oil: An underrated allergen? Contact Derm. 2019, 81, 133–134. [Google Scholar] [CrossRef] [PubMed]
- Paulsen, E.; Thormann, H.; Vestergaard, L. Eucalyptus species as a cause of airborne allergic contact dermatitis. Contact Derm. 2018, 78, 301–303. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, T.; Yokozeki, H. Occupational contact dermatitis caused by eucalyptus species and tanacetum parthenium. Contact Derm. 2019, 80, 333–334. [Google Scholar] [CrossRef] [PubMed]
- Gilissen, L.; Huygens, S.; Goossens, A. Allergic contact dermatitis caused by topical herbal remedies: Importance of patch testing with the patients’ own products. Contact Dermat. 2018, 78, 177–184. [Google Scholar] [CrossRef]
- Paulsen, E.; Andersen, K.E. Clinical patterns of compositae dermatitis in danish monosensitized patients. Contact Derm. 2018, 78, 185–193. [Google Scholar] [CrossRef]
- Paulsen, E.; El-Houri, R.B.; Andersen, K.E.; Christensen, L.P. Parthenolide in danish biodynamic and organic milk: A new source of exposure to an allergenic sesquiterpene lactone. Contact Derm. 2018, 79, 208–212. [Google Scholar] [CrossRef]
- Hassan, I.; Rasool, F.; Akhtar, S.; Kamili, A.; Rather, P.; Kanth, R.; Bhat, Y.; Rather, S.; Mubashir, S.; Yaseen, A.; et al. Contact dermatitis caused by tulips: Identification of contact sensitizers in tulip workers of Kashmir valley in north India. Contact Derm. 2018, 78, 64–69. [Google Scholar] [CrossRef]
- Sharma, A.; Mahajan, V.K.; Mehta, K.S.; Chauhan, P.S.; Sharma, V.; Sharma, A.; Wadhwa, D.; Chauhan, S. Pesticide contact dermatitis in agricultural workers of Himachal Pradesh (India). Contact Derm. 2018, 79, 213–217. [Google Scholar] [CrossRef]
- Uter, W.; Amario-Hita, J.C.; Balato, A.; Ballmer-Weber, B.; Bauer, A.; Belloni Fortina, A.; Bircher, A.; Chowdhury, M.M.U.; Cooper, S.M.; Czarnecka-Operacz, M.; et al. European surveillance system on contact allergies (ESSCA): Results with the european baseline series, 2013/14. J. Eur. Acad. Derm. Venereol. 2017, 31, 1516–1525. [Google Scholar] [CrossRef]
- Martínez Pallás, I.; Conejero Del Mazo, C.; Prieto Torres, L. Allergic contact stomatitis caused by propolis candies. Contact Derm. 2018, 78, 418–419. [Google Scholar] [CrossRef]
- Muehlenbein, S.; Eming, A.; Pfützner, W. Therapy of aphthous stomatitis with serious consequences-contact-allergic glossitis and contact-allergic stomatitis to propolis. Allergologie 2018, 41, 199–202. [Google Scholar]
- Lee, S.X.; Boontaveeyuwat, E.; Thaiwat, S.; Rustin, M.; McFadden, J. Severe allergic contact dermatitis mimicking angioedema caused by propolis used as a traditional remedy. Contact Derm. 2018, 79, 185–186. [Google Scholar] [CrossRef] [PubMed]
- Freedman, J.; Griggs, J.; De Padova, M.P.; Tosti, A. What’s the “buzz” about propolis? Propolis-induced systemic contact dermatitis. Contact Derm. 2019, 80, 65–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyman, G.S.A.; Tang, M.; Inerot, A.; Osmancevic, A.; Malmberg, P.; Hagvall, L. Contact allergy to beeswax and propolis among patients with cheilitis or facial dermatitis. Contact Derm. 2019, 81, 110–116. [Google Scholar] [CrossRef]
- Mauro, M.; Fortina, A.B.; Corradin, T.; Marino, A.; Bovenzi, M.; Filon, F.L. Sensitization to, and allergic contact dermatitis caused by, colophonium in north-eastern Italy in 1996 to 2016 with a focus on occupational exposures. Contact Derm. 2018, 79, 303–309. [Google Scholar] [CrossRef]
- Pesonen, M.; Suuronen, K.; Suomela, S.; Aalto-Korte, K. Occupational allergic contact dermatitis caused by colophonium. Contact Derm. 2019, 80, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Corazza, M.; Musmeci, D.; Scuderi, V.; Bernardi, T.; Cristofaro, D.; Borghi, A. Occupational systemic allergic dermatitis in a football player sensitized to colophonium. Contact Derm. 2018, 79, 325–326. [Google Scholar] [CrossRef]
- Hamnerius, N.; Mowitz, M. Two cases of contact allergic reactions to finn chamber AQUA test chambers. Contact Derm. 2019, 81, 320–322. [Google Scholar] [CrossRef]
- Sánchez-Gilo, A.; Gómez-de la Fuente, E.; Vicente-Martín, F.J. Allergic contact dermatitis caused by finn chambers AQUA in two patients. Contact Derm. 2019, 80, 246–247. [Google Scholar] [CrossRef]
- Bach, R.O.; Paulsen, E.; Vestergaard, L.; Andersen, F. A tale of 2 poles. Contact Derm. 2019, 80, 131–132. [Google Scholar] [CrossRef]
- Santos, R.P.; Almeida, F.; Pereira, T.; Brito, C. Erythema multiforme major induced by exotic wood. Contact Derm. 2018, 79, 252–253. [Google Scholar] [CrossRef] [PubMed]
- Cabezas Arteaga, J.E.; Marques Gonçalves, D.L.; Samorano, L.P.; Chen Wu, S.L.; Silva Reis, V.M. Allergic contact dermatitis caused by a Brazilian exotic hardwood. Contact Derm. 2019, 81, 136–137. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Longenecker, A.; ElSohly, M.A.; Gul, W.; Hage, R.J.; Hamann, C.P.; Marks, J.G. Urushiol patch test using the T.R.U.E. TEST system. Dermatitis 2018, 29, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Bonnekoh, H.; Poch, G.; Metz, M. Severe contact dermatitis caused by urushiol in japanese lacquer. Contact Derm. 2019, 80, 55–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraft, M.; Schubert, S.; Geier, J.; Worm, M. IVDK Contact dermatitis and sensitization in professional musicians. Contact Derm. 2019, 80, 273–278. [Google Scholar] [CrossRef]
- Vihervaara, A.; Liippo, J. African blackwood (Dalbergia melanoxylon)—induced occupational allergic contact dermatitis in a professional piccolo flautist. Contact Derm. 2019, 81, 294–296. [Google Scholar] [CrossRef]
- Hansel, K.; Murgia, N.; Russano, A.; Crescenzi, F.; Tramontana, M.; Bianchi, L.; Neve, D.; Muzi, G.; Stingeni, L. Airborne allergic contact dermatitis caused by machaerium scleroxylon: Confirmation by in vivo and in vitro tests. Contact Derm. 2019, 81, 296–298. [Google Scholar] [CrossRef]
- Gevers, L.A.H.A.; Zweegers, J.; Bruins, F.M.; Hellenbrand-Hendriks, J.; Cornelissen-Peters, H.; Meijer-Marcu, A.; Pasch, M.C.; Jansen, A. Airborne allergic contact dermatitis caused by wood tars. Contact Derm. 2019, 80, 137–138. [Google Scholar] [CrossRef]
- Uter, W.; Goossens, A.; Gonçalo, M.; Johansen, J.D.; On behalf of the EECDRG. Guidelines for the presentation of contact allergy case reports. Contact Derm. 2017, 76, 107–113. [Google Scholar] [CrossRef]
- Geier, J.; Forkel, S.; Heetfeld, A.; Lessmann, H.; Buhl, T. Contact allergy to 2-amino-2-methyl-1-propanol in a metalworking fluid. Contact Derm. 2019, 80, 323–324. [Google Scholar] [CrossRef]
- Malinauskiene, L.; Linauskienė, K.; Černiauskas, K.; Chomičiene, A. Bakuchiol-A new allergen in cosmetics. Contact Derm. 2019, 80, 398–399. [Google Scholar] [CrossRef] [PubMed]
- Foster, E.; Nguyen, C.; Norris, P. Contact Buzz: Allergic contact dermatitis to cannabis. Dermatitis 2018, 29, 223–224. [Google Scholar] [CrossRef] [PubMed]
- Mangodt, E.A.; Dendooven, E.; De Fré, C.; Lambert, J.; Aerts, O. Capryloyl glycine: A polyfunctional cosmetic ingredient and potential skin sensitizer. Contact Derm. 2019, 80, 400–402. [Google Scholar] [CrossRef] [PubMed]
- Oscoz-Jaime, S.; Hervella-Garcés, M.; de Espronceda-Ezquerro, M.I.; Yanguas-Bayona, J.I. Allergic contact dermatitis caused by sodium cetearyl sulfate. Contact Derm. 2018, 78, 426–427. [Google Scholar] [CrossRef]
- Pastor-Nieto, M.-A.; Gatica-Ortega, M.-E.; Alcántara-Nicolás, F.-D.-A.; Pérez-Mesonero, R.; Gil-Redondo, R.; Martín-Alcalde, E.; De Eusebio, E. Allergic contact dermatitis resulting from cetyl PEG/PPG-10/1 dimethicone in a deodorant cream. Contact Derm. 2018, 78, 236–239. [Google Scholar] [CrossRef]
- Skudlik, C.; Markthaler, M.; John, S.M. Occupational contact allergy to sodium cocoamphopropionate in a skin protection cream. Contact Derm. 2018, 78, 295–296. [Google Scholar] [CrossRef]
- Ito-Watanabe, M.; Hayama, K.; Fujita, H.; Sasaki, K.; Numata, M.; Terui, T. A case of contact dermatitis caused by a polyurethane hot melt adhesive. Contact Derm. 2019, 81, 389–391. [Google Scholar] [CrossRef]
- Pousa-Martínez, M.; González-Rodríguez, C.; Rodriguez-Rodriguez, M.; Sainz-Gaspar, L.; Sardina, F.J.; Fernández-Redondo, V. Garment allergy caused by disperse blue 360: A new sensitizer. Contact Derm. 2018, 79, 37–38. [Google Scholar] [CrossRef]
- Sanz-Sánchez, T.; Valverde Garrido, R.; Maldonado Cid, P.; Díaz-Díaz, R.M. Allergic contact dermatitis caused by hydroxyacetophenone in a face cream. Contact Derm. 2018, 78, 174–175. [Google Scholar] [CrossRef]
- Raison-Peyron, N.; Dereure, O. Allergic contact dermatitis caused by 10-hydroxydecenoic acid contained in an emollient cream. Contact Derm. 2019, 81, 386–387. [Google Scholar] [CrossRef]
- Aerts, O.; Mangodt, E.; Smets, K.; Mertens, M.; Constandt, L.; Goossens, A. Occupational airborne allergic contact dermatitis caused by N-(4-hydroxyphenyl) benzenesulfonamide. Contact Derm. 2019, 80, 71–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Numata, T.; Okubo, Y.; Tsuboi, R. Allergic contact dermatitis caused by isopropyl lauroyl sarcosinate. Contact Derm. 2019, 80, 58–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iijima, S.; Takayama, N. Allergic contact dermatitis caused by isopropyl methylphenol, a new hapten. Contact Derm. 2019, 80, 402–403. [Google Scholar] [CrossRef] [PubMed]
- Kerre, S.; Goossens, A. Allergic contact cheilitis caused by lauryl PCA. Contact Derm. 2018, 79, 318–319. [Google Scholar] [CrossRef]
- Hattori, J.; Tamagawa-Mineoka, R.; Ueda, S.; Masuda, K.; Katoh, N. Allergic contact dermatitis caused by irganox 1076 used as antioxidant in non-woven fabric. Contact Derm. 2018, 79, 117–118. [Google Scholar] [CrossRef]
- Nagai, H.; Fukuda, H. Allergic contact dermatitis caused by Olanedine® (olanexidine gluconate), a new antiseptic. Contact Derm. 2018, 78, 164–165. [Google Scholar] [CrossRef]
- Jaulent, C.; Dereure, O.; Raison-Peyron, N. Contact dermatitis caused by polyacrylamide/C13-4 isoparaffin/laureth-7 mix in an emollient cream for atopic skin. Contact Derm. 2019, 81, 70–71. [Google Scholar] [CrossRef]
- Ochando-Ibernón, G.; Schneller-Pavelescu, L.; Silvestre-Salvador, J.F. Allergic contact dermatitis caused by “Rosa mosqueta” oil. Contact Derm. 2018, 79, 259–260. [Google Scholar] [CrossRef]
- Vandeweghe, J.; Decoster, E.; Lapeere, H. First report of allergic contact dermatitis caused by sorbitan caprylate. Contact Derm. 2018, 78, 162–164. [Google Scholar] [CrossRef]
- Waas, R.L.V.; Hill, G. Allergic contact dermatitis caused by vinylpyrrolidone/eicosene copolymer in a sunscreen. Contact Derm. 2019, 80, 63. [Google Scholar] [CrossRef] [Green Version]
- Uter, W.; Diepgen, T.L. Epidemiology. In Contact Dermatitis; Duus Johansen, J., Mahler, V., Lepoittevin, J.-P., Frosch, P.J., Eds.; Springer: Heidelberg, Germany, 2019. [Google Scholar]
- Arrandale, V.H.; Holness, D.L. Using health insurance administrative data to explore patch testing utilization in Ontario, Canada-An untapped resource. Contact Derm. 2019, 80, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Ibekwe, P.U.; Bagudu, Z.S. Patch test results obtained with the European baseline series at a diagnostics centre in Abuja, Nigeria. Contact Derm. 2019, 81, 154–155. [Google Scholar] [CrossRef] [PubMed]
- Constantin, M.-M.; Bucur, S.; Matei, C.; Nita, I.E.; Constantin, T. The european baseline series in romania: Results of patch testing in contact dermatitis and determination of the most frequently awareness in adult patients. Rev. Chim. 2019, 70, 1337–1341. [Google Scholar] [CrossRef]
- Corrêa-Fissmer, M.; Dalazen, C.C.; Ferreira, B.P.; Iser, B.P.M. Assessment of patch test results carried out during ten years in a city in southern Brazil. Bras Derm. 2018, 93, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Dusefante, A.; Mauro, M.; Belloni Fortina, A.; Corradin, M.T.; Larese Filon, F. Contact allergy to methylchloroisothiazolinone/methylisothiazolinone in north-eastern Italy: A temporal trend from 1996 to 2016. J. Eur. Acad. Derm. Venereol. 2019, 33, 912–917. [Google Scholar] [CrossRef] [PubMed]
- Ezendam, J.; Bokkers, B.G.H.; Bil, W.; Delmaar, J.E. Skin sensitisation quantitative risk assessment (QRA) based on aggregate dermal exposure to methylisothiazolinone in personal care and household cleaning products. Food Chem. Toxicol. 2018, 112, 242–250. [Google Scholar] [CrossRef] [PubMed]
- SCCS. Opinion on Skin Sensitisation Quantitative Risk Assessment for Fragrance Ingredients (Qra2), Preliminary version of 24–25 October 2017, final version of 30 July 2018 (SCCS/1589/17); European Union: Luxembourg, 2018; ISBN 978-92-76-00241-3. [Google Scholar]
- Jongeneel, W.P.; Delmaar, J.E.; Bokkers, B.G.H. Health impact assessment of a skin sensitizer: Analysis of potential policy measures aimed at reducing geraniol concentrations in personal care products and household cleaning products. Env. Int. 2018, 118, 235–244. [Google Scholar] [CrossRef]
- Friis, U.F.; Goosens, A.; Giménez-Arnau, A.M.; Lidén, C.; Giménez-Arnau, E.; White, I.R.; Alfonso, J.H.; Uter, W.; Johansen, J.D. Self-testing for contact allergy to hair dyes-a 5-year follow-up multicentre study. Contact Derm. 2018, 78, 131–138. [Google Scholar] [CrossRef]
- Coenraads, P.-J.; Aberer, W.; Cristaudo, A.; Diepgen, T.; Holden, C.; Koch, L.; Schuttelaar, M.-L.; Weisshaar, E.; Fuchs, A.; Schlotmann, K.; et al. Allergy alert test for p-phenylenediamine-allergic hair dye users. Dermatitis 2018, 29, 250–257. [Google Scholar] [CrossRef]
- SCCS (Scientific Committee on Consumer Safety). Opinion on Allergy Alert Test (AAT) as a Proof-of-Concept Study, Preliminary Version of 10 May 2019, Final Version of 10 September 2019, SCCS/1607/19. Available online: https://ec.europa.eu/health/sites/health/files/scientific_committees/consumer_safety/docs/sccs_o_229.pdf (accessed on 1 April 2020).
- Ko, L.N.; Kroshinsky, D.; Schalock, P.C. Assessing the validity of self-reported history of rash caused by metal or jewellery. Contact Derm. 2018, 78, 208–210. [Google Scholar] [CrossRef]
- Linauskienė, K.; Zimerson, E.; Malinauskiene, L.; Isaksson, M. Low amount of formaldehyde in topical medication and cosmetics: Is it clinically relevant? Contact Derm. 2019, 81, 60–61. [Google Scholar] [CrossRef] [PubMed]
- Schneller-Pavelescu, L.; Ochando-Ibernón, G.; Vergara-de Caso, E.; Silvestre-Salvador, J.F. “Crossed” allergic contact dermatitis caused by oxidized vitamin K1 in a patient previously sensitized to non-oxidized vitamin K1. Contact Derm. 2019, 80, 64–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, G.N.; Shen, S.; Nixon, R. Severe allergic contact dermatitis caused by topical bufexamac requiring hospitalization. Contact Derm. 2019, 80, 395–397. [Google Scholar] [CrossRef] [PubMed]
- Bennike, N.H.; Heisterberg, M.S.; White, I.R.; Mahler, V.; Silvestre-Salvador, J.F.; Giménez-Arnau, A.; Johansen, J.D. Quality of life and disease severity in dermatitis patients with fragrance allergy—A cross-sectional european questionnaire study. Contact Derm. 2019, 81, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Vanhoutte, C.; Goossens, A.; Gilissen, L.; Huygens, S.; Vital-Durand, D.; Dendooven, E.; Aerts, O. Concomitant contact-allergic reactions to iodopropynyl butylcarbamate and iodine. Contact Dermat. 2019, 81, 17–23. [Google Scholar] [CrossRef]
- Batista, M.; Morgado, F.; Gonçalo, M. Patch test reactivity to iodopropynyl butylcarbamate in consecutive patients during a period of 7 years. Contact Derm. 2019, 81, 54–55. [Google Scholar] [CrossRef]
- Uter, W.; Johansen, J.D.; Lidén, C.; Lepoittevin, J.-P.; White, I.R. Criteria for the evidence-based categorisation of skin sensitisers. Food Chem. Toxicol. 2017, 105, 14–21. [Google Scholar] [CrossRef]
- OECD. The Adverse Outcome Pathway for Skin Sensitization Initiated by Covalent Binding to Proteins. Part 2: Use of the Aop to Develop Chemical Categories and Integrated Assessment and Testing Approaches; OECD Environment Health and Safety Publication Series on Testing and Assessment; OECD: Paris, France, 2012. [Google Scholar]
- OECD. The Adverse Outcome Pathway for Skin Sensitization Initiated by Covalent Binding to Proteins. Part 1: Scientific Evidence; OECD Environment Health and Safety Publication Series on Testing and Assessment; OECD: Paris, France, 2012. [Google Scholar]
- OECD. Test No. 442C. In Chemico Skin Sensitisation: Assays Addressing the Adverse Outcome Pathway Key Event on Covalent Binding to Proteins. OECD Guidelines for the Testing of Chemicals, Section 4; Éditions OCDE: Paris, France, 2019. [Google Scholar]
- OECD. Test No. 442D. In In Vitro Skin Sensitisation: ARE-Nrf2 Luciferase Test Method. OECD Guidelines for the Testing of Chemicals, Section 4; Éditions OCDE: Paris, France, 2018. [Google Scholar]
- OECD. Test No. 442E. In In Vitro Skin Sensitisation Assays Addressing the Key Event on Activation of Dendritic Cells on the Adverse Outcome Pathway for Skin Sensitisation. OECD Guidelines for The Testing of Chemicals, Section 4; Éditions OCDE: Paris, France, 2018. [Google Scholar]
- Cottrez, F.; Boitel, E.; Auriault, C.; Aeby, P.; Groux, H. Genes specifically modulated in sensitized skins allow the detection of sensitizers in a reconstructed human skin model. Development of the SENS-IS assay. Toxicol. Vitr. 2015, 29, 787–802. [Google Scholar] [CrossRef]
- Eskes, C.; Hennen, J.; Schellenberger, M.T.; Hoffmann, S.; Frey, S.; Goldinger-Oggier, D.; Peter, N.; Van Vliet, E.; Blömeke, B. The HaCaT/THP-1 cocultured activation test (COCAT) for skin sensitization: A study of intra-lab reproducibility and predictivity. ALTEX 2019, 36, 613–622. [Google Scholar] [CrossRef]
- OECD. The Adverse Outcome Pathway for Skin Sensitization Initiated by Covalent Binding to Proteins. Part 1: Scientific Evidence; OECD Environment Health and Safety Publication Series on Testing and Assessment; OECD: Paris, France, 2016. [Google Scholar]
- Li, B.S.; Cary, J.H.; Maibach, H.I. Relapsing polyisoprene glove allergic contact dermatitis: Another call for more complete glove package label declaration. Contact Derm. 2018, 79, 242–243. [Google Scholar] [CrossRef]
- Kluger, N. Contact allergy to moisturizers in Finland: The tale of the lurking tube in the medicine cupboard. Contact Derm. 2018, 78, 289–290. [Google Scholar] [CrossRef] [PubMed]



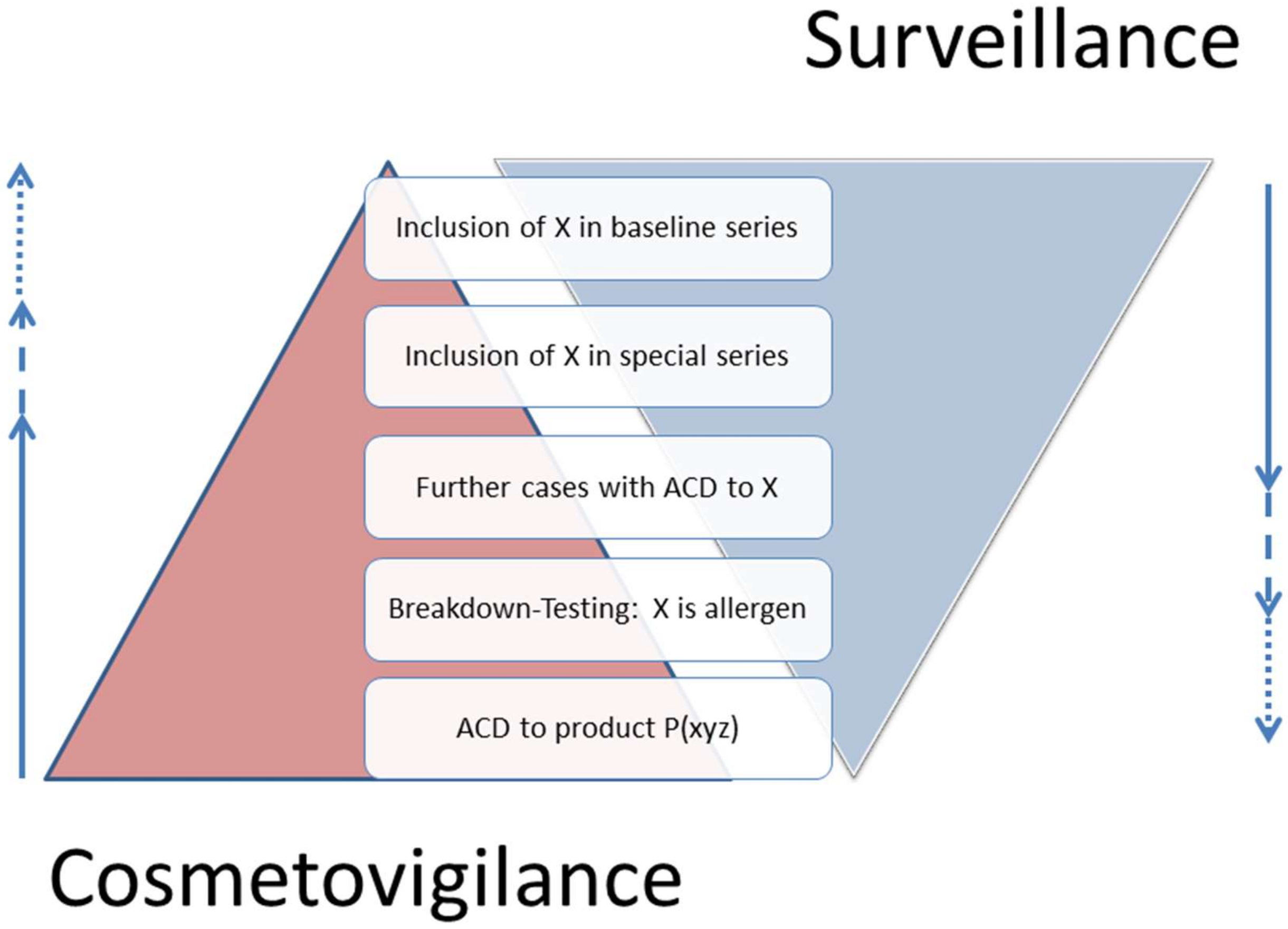{kind=link}
{kind=link}
| Case(s) | Exposure | Allergen | Ref. |
|---|---|---|---|
| M (55) | Water-based metalworking fluid | 2-Amino-2-methyl-1-propanol (2% pet.) | [302] |
| F (33) | “Hypoallergenic cosmetic product for sensitive skin” | Bakuchiol (0.1% pet.) | [303] |
| F (67) | Home-grown Cannabis sativa and C. indica | Positive to entire dried flower (10 controls negative) | [304] |
| M (50) | Body lotion | Capryloyl glycine (1% aq./ethanol 1:1) | [305] |
| F (51) | Brand hand and foot cream, respectively | Sodium cetearyl sulfate (10% pet.) | [306] |
| M (47) | Cream deodorant | Cetyl PEG/PPG-10/1 dimethicone (copolymer) 5% pet. | [307] |
| 3 M, (35–60) | Skin protection cream | Cocoamphopropionate (1% aq.) | [308] |
| F (36) | “Label dermatitis” due to hot melt adhesive | dimethyl (p-methoxybenzylidene)malonate (2% pet.) | [309] |
| F (34) | Multicoloured bikini and black and white dress | Disperse Blue 360 tested on polyester fabrich swatches | [310] |
| M (79) | Eyedrops … and wife’s face cream | Face cream “as is” and ingredient hydroxyacetophenone 0.6% aq. | [311] |
| M (21) | Moisturising cream | 10-hydroxydecenoic acid | [312] |
| M (53,58) | Production of heat-sensitive polyethylene terephthalate films | N-(4-hydroxyphenyl)benzenesulfonamide | [313] |
| F (43) | Face cream | Isopropyl lauroyl sarcosinate (5% ethanol) | [314] |
| F (55, 59,92) | Antimicrobial ointments/bandage | Isopropyl methylphenol (0.001–1.5% pet.) | [315] |
| F (20,51), M (55) | Lip balm causing cheilitis | Lauryl PCA (20% pet.) | [316] |
| M (10) | Non-woven polyethylene sheets used during surgery | Octadecyl 3-(3,5-di-tert-butyl-4-hydroxyphenyl)propionate (Irganox 1076) (0.05–2% pet.) | [317] |
| F (66), M (65) | Perioperative antiseptic | Olanexidine gluconate (“as is”); excipients negative | [318] |
| F (33) | Moisturizing cream for atopic skin | Polyacrylamide/C13-4 isoparaffin/laureth-7 mix (tested “as is”) | [319] |
| F (26) | “Rosa mosqueta” oil | Positive ROAT with product (R. canina fruit oil; R. rubiginosa seed oil), negative to tocopherol (antioxidant in product) | [320] |
| 4 F (26–52) | Brand deodorant | Sorbitan caprylate (1% pet.) | [321] |
| M (46) | Brand sunscreen | Vinylpyrrolidone/eicosene copolymer 5% pet. | [322] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uter, W.; Werfel, T.; Lepoittevin, J.-P.; White, I.R. Contact Allergy—Emerging Allergens and Public Health Impact. Int. J. Environ. Res. Public Health 2020, 17, 2404. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072404
Uter W, Werfel T, Lepoittevin J-P, White IR. Contact Allergy—Emerging Allergens and Public Health Impact. International Journal of Environmental Research and Public Health. 2020; 17(7):2404. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072404
Chicago/Turabian StyleUter, Wolfgang, Thomas Werfel, Jean-Pierre Lepoittevin, and Ian R. White. 2020. "Contact Allergy—Emerging Allergens and Public Health Impact" International Journal of Environmental Research and Public Health 17, no. 7: 2404. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072404