Equine-Assisted Intervention to Improve Perceived Value of Everyday Occupations and Quality of Life in People with Lifelong Neurological Disorders: A Prospective Controlled Study


Abstract
:1. Introduction
Aim
2. Materials and Methods
2.1. Setting
2.2. Intervention
2.3. Study Population
2.3.1. Intervention Group
2.3.2. Control Groups
2.4. Quantitative Measures
Secondary Outcome Measures Were the Following
2.5. Qualitative Methods
3. Results
3.1. Quantitative Measures
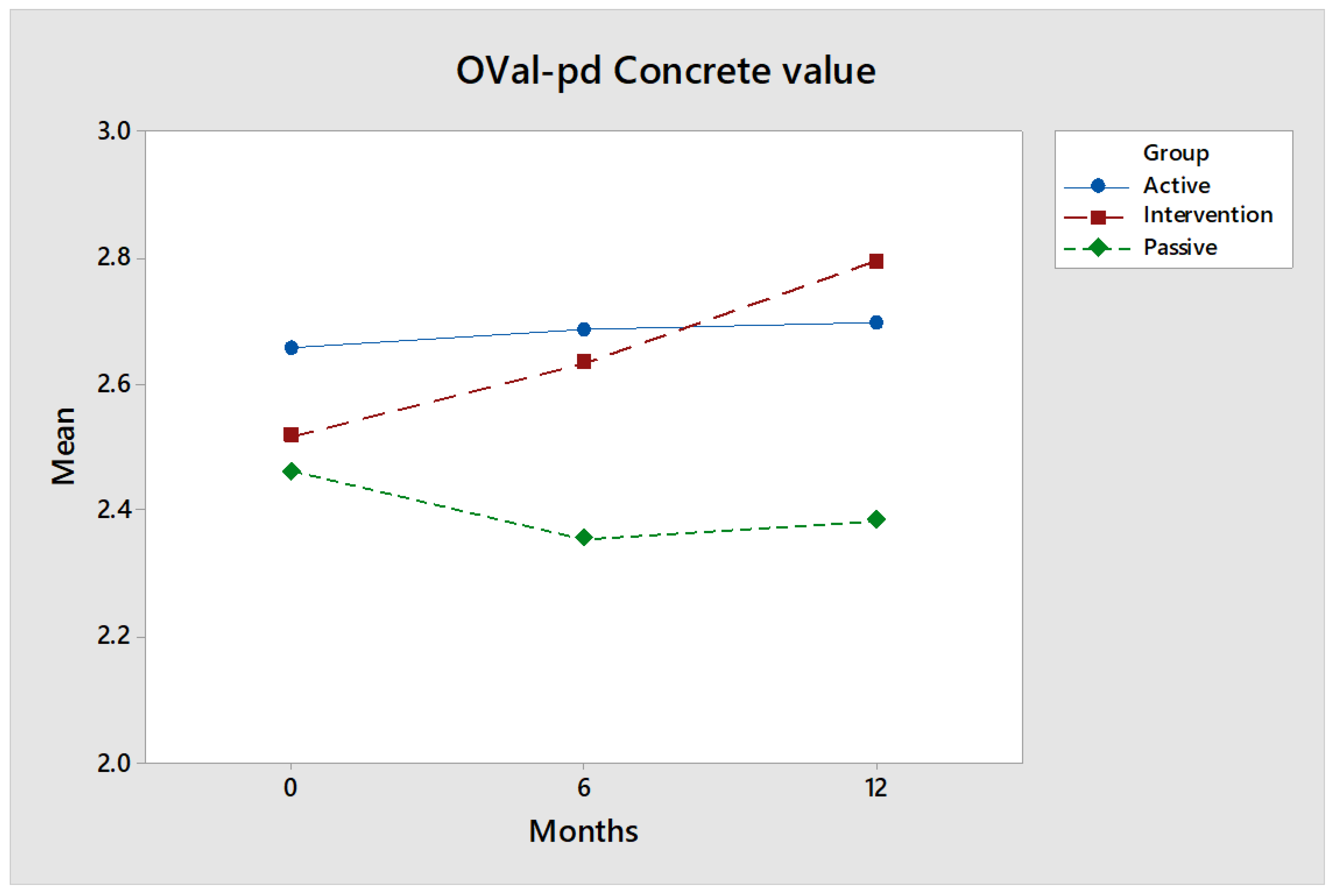
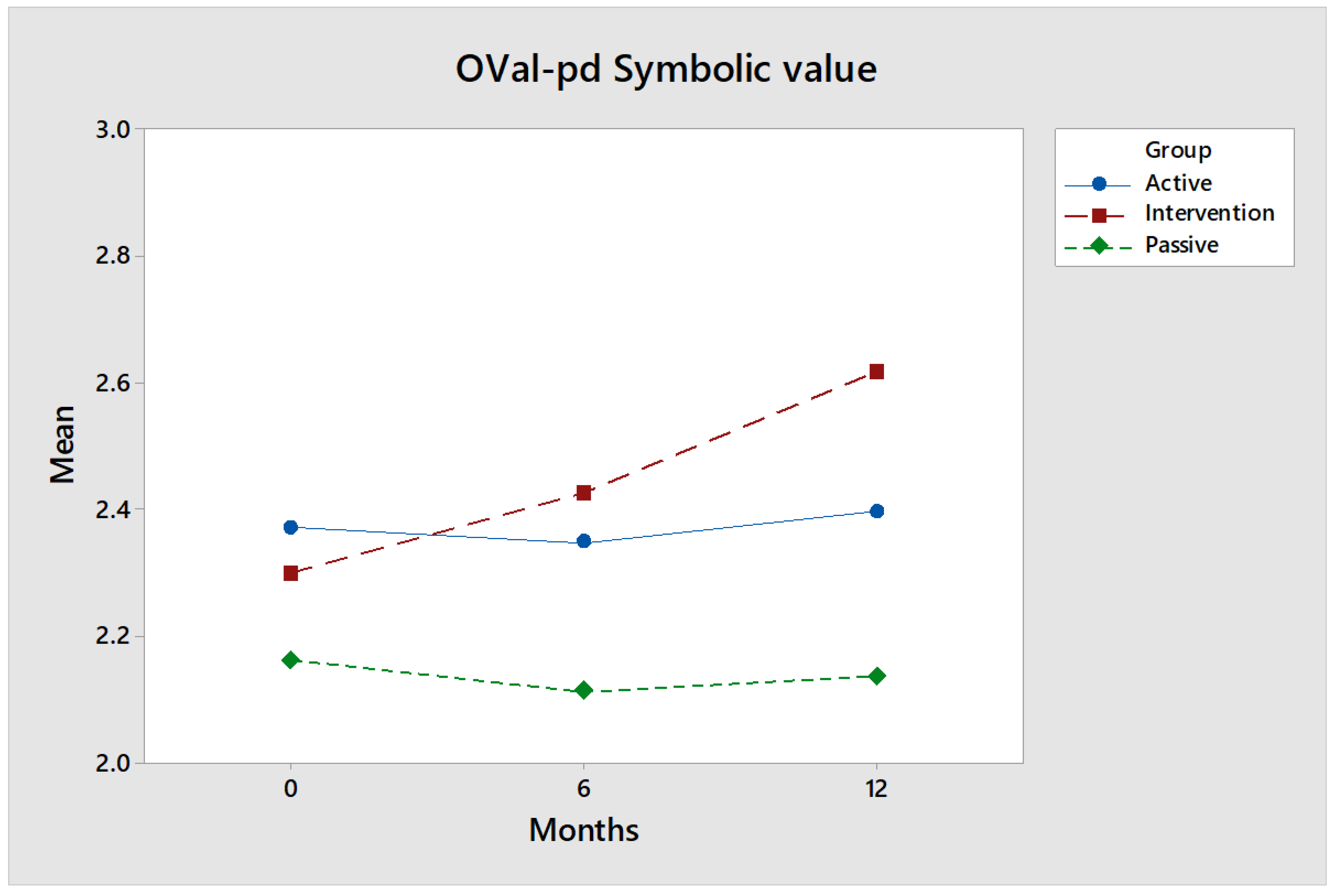
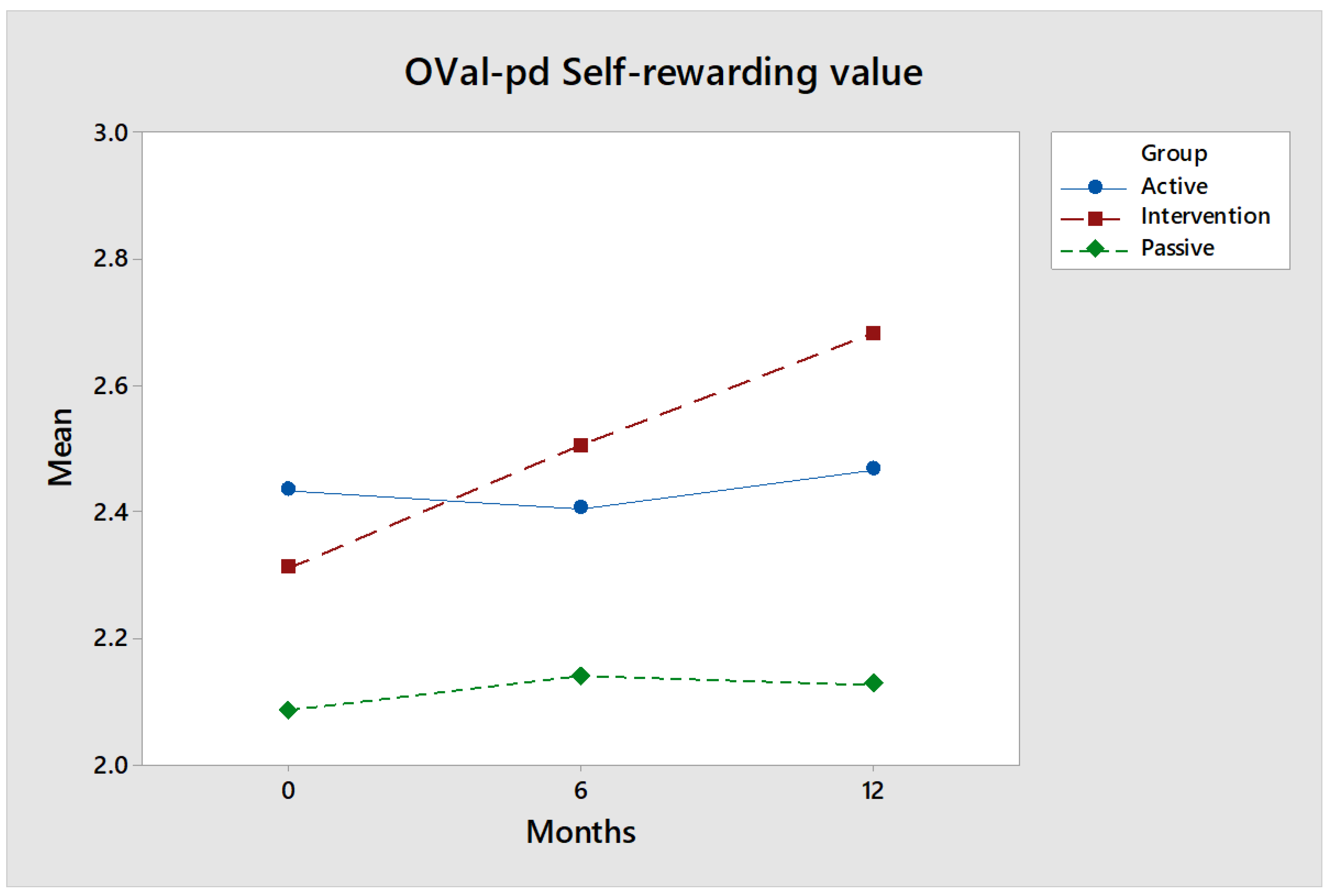
3.1.1. OVal-pd
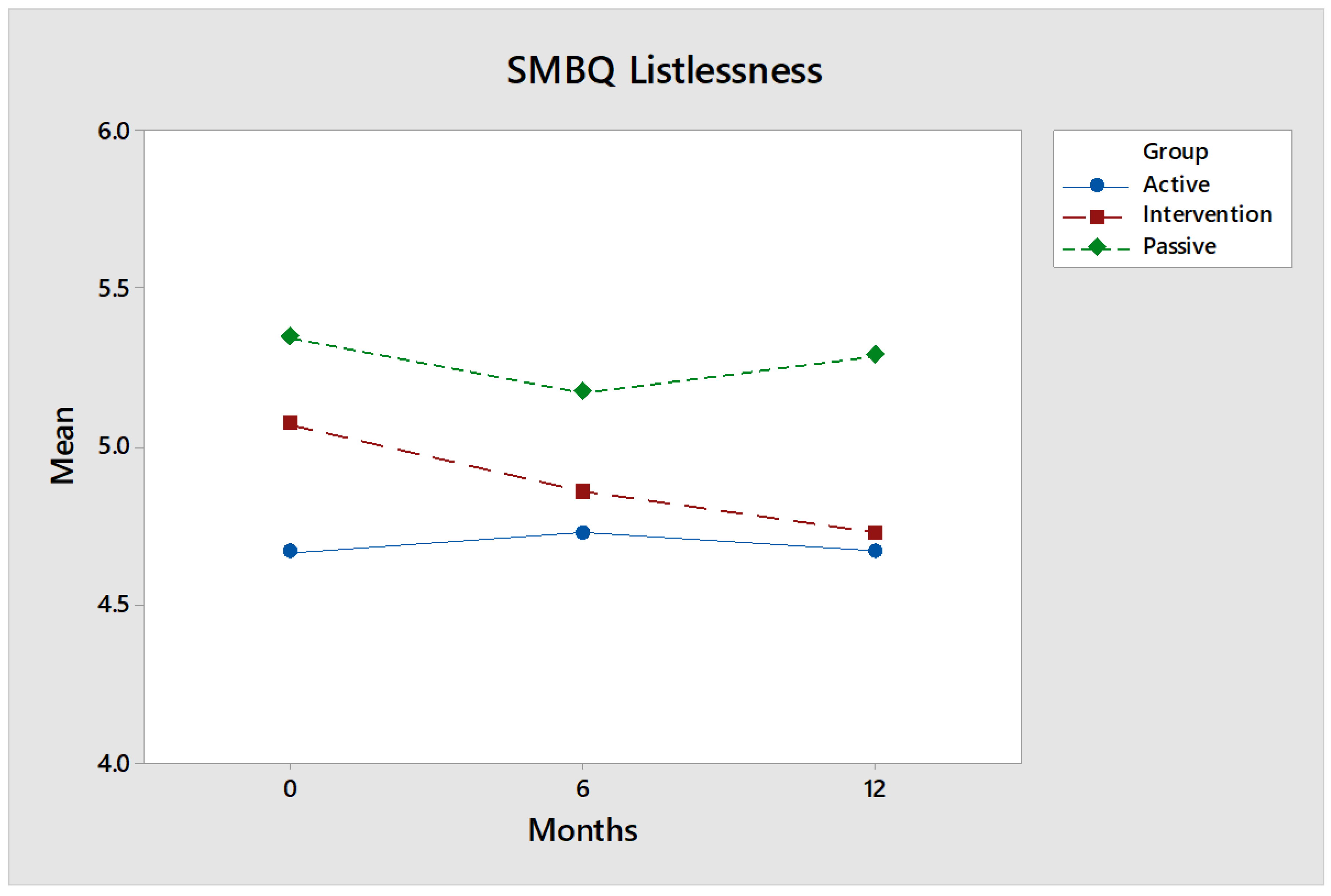
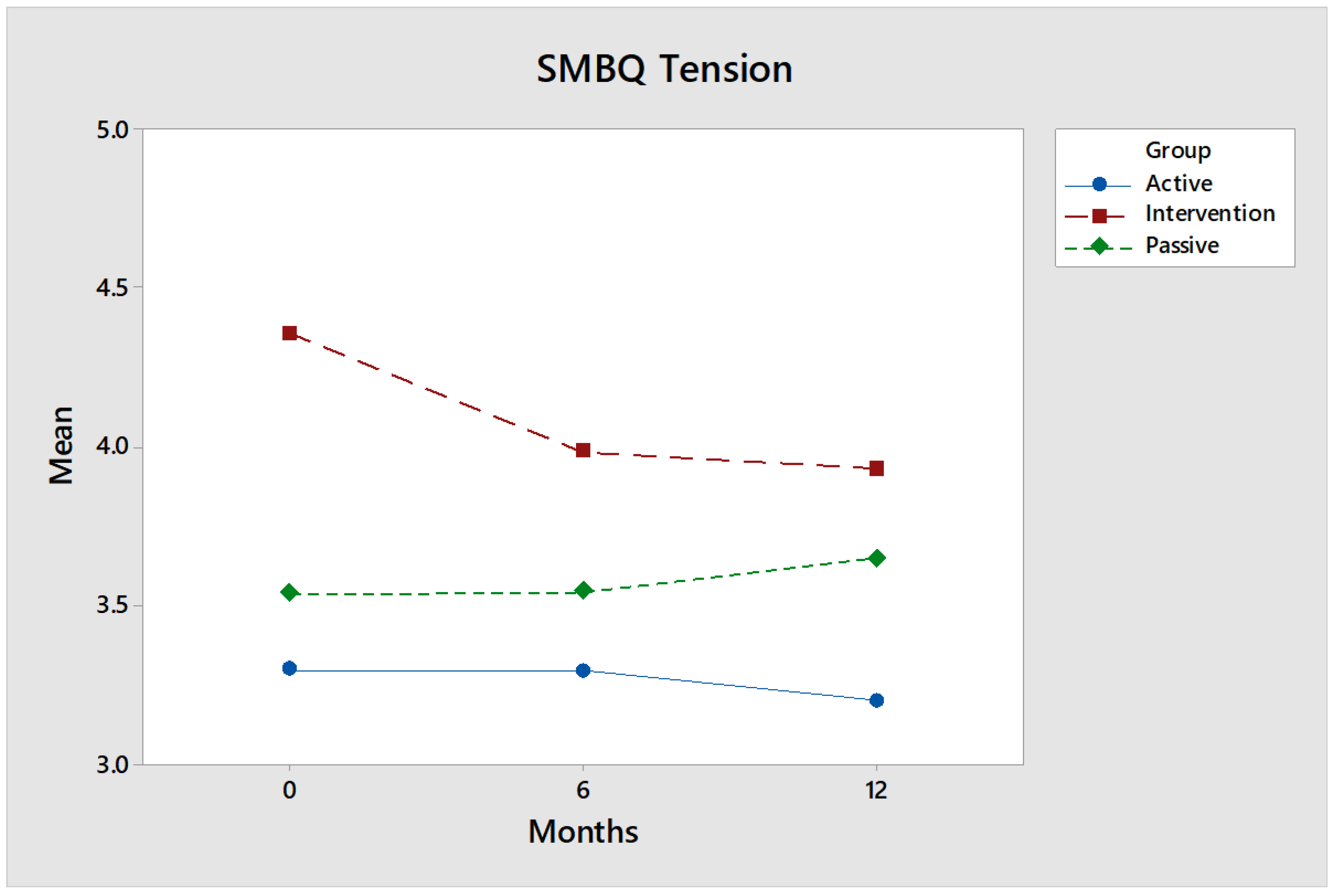
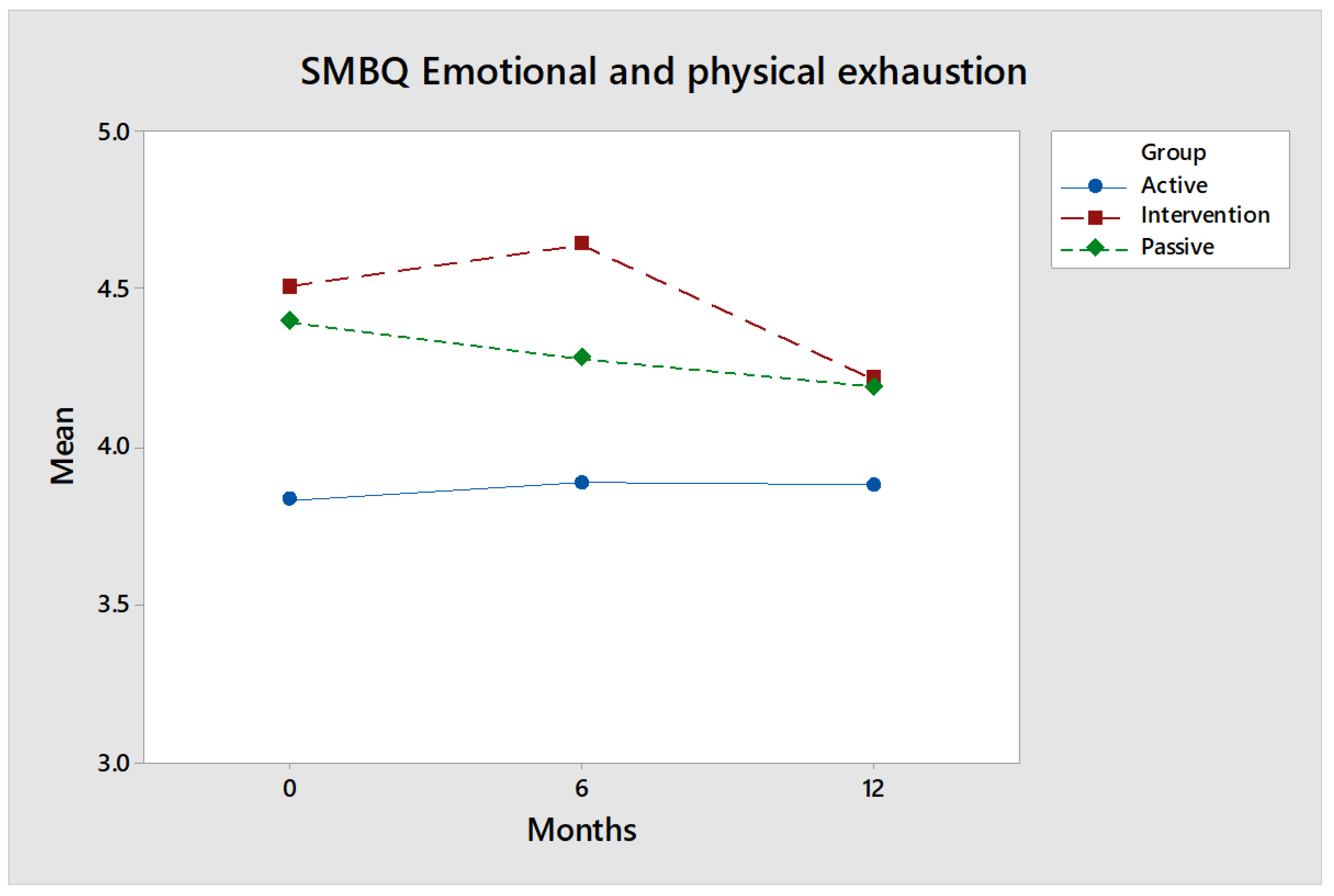
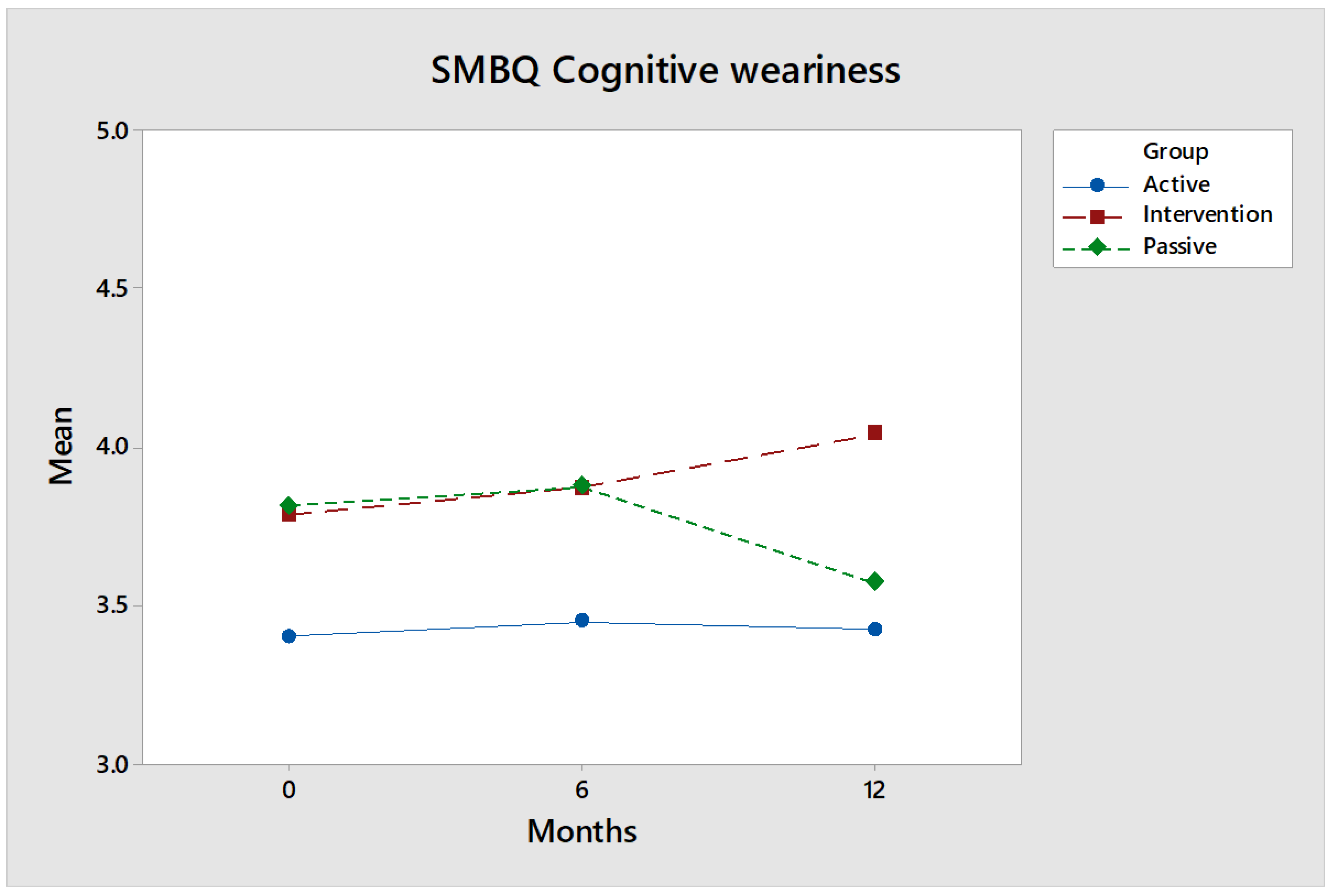
3.1.2. Shirom-Melamed Burnout Questionnaire (SMBQ)
3.1.3. EQ-VAS
3.2. Qualitative Analysis
- 1:
- Strengthening and promoting abilities and well-being
- 2:
- Increased empowerment
- 3:
- Equality and justice through increased accessibility
- 4:
- The horse and its surroundings as a resource
3.2.1. Theme 1: Strengthening and Promoting Abilities and Well-Being
3.2.2. Theme 2: Increased Empowerment
3.2.3. Theme 3: Equality and Justice through Increased Accessibility
3.2.4. Theme 4: The Horse and Surrounding Environment as a Resource
4. Discussion
4.1. Issues Regarding Future Policy
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fine, H. Handbook on Animal Assisted Therapy: Theoretical Foundations and Guidelines for Practice, 3rd ed.; Academic Press: San Diego, CA, USA, 2010. [Google Scholar]
- Bizub, A.L.; Joy, A.; Davidson, L. “It’s like being in another world”: Demonstrating the benefits of therapeutic horseback riding for individuals with psychiatric disability. Psychiatr. Rehabil. J. 2003, 26, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Lessick, M.; Shinaver, R.; Post, K.M.; Rivera, J.E.; Lemon, B. Therapeutic Horseback Riding. Nurs. Women’s Health 2004, 8, 46–53. [Google Scholar] [CrossRef] [PubMed]
- All, A.C.; Loving, G.L.; Crane, L.L. Animals, horseback riding, and implications for rehabilitation therapy. J. Rehabil. 1999, 65, 49. [Google Scholar]
- Fry, N.E. Equine-Assisted Therapy: An Overview. In Biotherapy—History, Principles and Practice; Grassberger, M., Sherman, R., Gileva, O., Kim, C., Mumcuoglu, K., Eds.; Springer: Dordrecht, The Netherlands, 2013; pp. 255–284. [Google Scholar]
- Macauley, B. Animal-assisted therapy for persons with aphasia: A pilot study. J. Rehabil. Res. Dev. 2006, 43, 357–366. [Google Scholar] [CrossRef]
- Matuszek, S. Animal-Facilitated Therapy in Various Patient Populations. Holist. Nurs. Pract. 2010, 24, 187–203. [Google Scholar] [CrossRef] [Green Version]
- Traetteberg, E. Ridning Som Rehabilitering; [Horseback riding as rehabilitation]; Akilles: Oslo, Norway, 2006. [Google Scholar]
- Silfverberg, G.; Lerner, H. Hästen, Hunden och den Mänskliga Hälsan: Vård, Behandling och Terapi; [The horse, the dog and human Health]; Ersta Sköndal Högskola Förlag: Stockholm, Sweden, 2014. [Google Scholar]
- Kamioka, H.; Okada, S.; Tsutani, K.; Park, H.; Okuizumi, H.; Handa, S.; Oshio, T.; Park, S.-J.; Kitayuguchi, J.; Abe, T.; et al. Effectiveness of animal-assisted therapy: A systematic review of randomized controlled trials. Complementary Ther. Med. 2014, 22, 371–390. [Google Scholar] [CrossRef]
- Lasa, S.M.; Bocanegra, N.M.; Alcaide, R.V.; Arratibel, M.A.A.; Donoso, E.V.; Ferriero, G. Animal assisted interventions in neurorehabilitation: A review of the most recent literature. Neurología 2015, 30, 1–7. [Google Scholar] [CrossRef]
- Bronson, C.; Brewerton, K.; Ong, J.; Palanca, C.; Sullivan, S.J. Does hippotherapy improve balance in persons with multiple sclerosis: A systematic review. Eur. J. Phys. Rehabil. Med. 2010, 46, 347–353. [Google Scholar]
- Zadnikar, M.; Kastrin, A. Effects of hippotherapy and therapeutic horseback riding on postural control or balance in children with cerebral palsy: A meta-analysis. Dev. Med. Child Neurol. 2011, 53, 684–691. [Google Scholar] [CrossRef]
- Stergiou, A.; Tzoufi, M.; Ntzani, E.; Varvarousis, D.; Beris, A.; Ploumis, A. Therapeutic Effects of Horseback Riding Interventions. A Systematic Review and Meta-analysis. Am. J. Phys. Med. Rehabil. 2017, 96, 717–725. [Google Scholar] [CrossRef]
- McGibbon, N.H.; Andrade, C.K.; Widener, G.; Cintas, H.L. Effect of an equine-movement therapy program on gait, energy expenditure, and motor function in children with spastic cerebral palsy: A pilot study. Dev. Med. Child Neurol. 1998, 40, 754–762. [Google Scholar] [CrossRef] [PubMed]
- Benda, W.; McGibbon, N.H.; Grant, K.L. Improvements in Muscle Symmetry in Children with Cerebral Palsy after Equine-Assisted Therapy (Hippotherapy). J. Altern. Complementary Med. 2003, 9, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Casady, R.L.; Nichols-Larsen, D.S. The effect of hippotherapy on ten children with cerebral palsy. Pediatric Phys. Ther. 2004, 16, 165–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Germain, S.M.; Wilkie, K.D.; Milbourne, V.M.K.; Theule, J. Animal-assisted Psychotherapy and Trauma: A Meta-analysis. Anthrozoös 2018, 31, 141–164. [Google Scholar] [CrossRef]
- Cabiddu, R.; Borghi-Silva, A.; Trimer, R.; Trimer, V.; Ricci, P.A.; Monteiro, C.I.; Maniglia, M.C.M.; Pereira, A.M.S.; das Chagas, G.R.; Carvalho, E.M. Hippotherapy acute impact on heart rate variability non-linear dynamics in neurological disorders. Physiol. Behav. 2016, 159, 88–94. [Google Scholar] [CrossRef]
- Anestis, M.D.; Anestis, J.C.; Zawilinski, L.L.; Hopkins, T.A.; Lilienfeld, S.O. Equine-related treatments for mental disorders lack empirical support: A systematic review of empirical investigations. J. Clin. Psychol. 2014, 70, 1115–1132. [Google Scholar] [CrossRef]
- Selby, A.; Smith-Osborne, A. A systematic review of effectiveness of complementary and adjunct therapies and interventions involving equines. Health Psychol. 2013, 32, 418–432. [Google Scholar] [CrossRef] [Green Version]
- Shaw, K. Effekt av Ridning Som Behandling: Sammanställning av Evidens. [The Effects of Horse Riding as Treatment: Evidence]; Evidensrapport, Habilitering & Hälsa, Stockholms läns landsting: Stockholm, Sweden, 2015. [Google Scholar]
- Marquez, J.; Weerasekara, I.; Chambers, L. Hippotherapy in adults with acquired brain injury: A systematic review. Physiother. Theory Pract. 2018. [Google Scholar] [CrossRef]
- Stern, C.; Chur-Hansen, A. An umbrella review of the evidence for equine-assisted interventions. Aust. J. Psychol. 2019, 71, 361–374. [Google Scholar] [CrossRef]
- De Santis, M.; Contalbrigo, L.; Borgi, M.; Cirulli, F.; Luzi, F.; Redaelli, V.; Stefani, A.; Toson, M.; Odore, R.; Vercelli, C.; et al. Equine Assisted Interventions (EAIs): Methodological Considerations for Stress Assessment in Horses. Vet. Sci. 2017, 4, 44. [Google Scholar] [CrossRef] [Green Version]
- Ng, Z.; Albright, J.; Fine, A.H.; Peralta, J. Our Ethical and Moral Responsibility: Ensuring the Welfare of Therapy Animals. In Handbook on Animal-Assisted Therapy. Foundations and Guidelines for Animal-Assisted Interventions, 4th ed.; Fine, A.H., Ed.; Academic Press: Cambridge, MA, USA, 2015; pp. 357–376. [Google Scholar]
- Gallagher, M.B.; Orla, T.; Muldoon, O.T.; Pettigrew, J. An integrative review of social and occupational factors influencing health and wellbeing. Front. Psychol. 2015, 6, 1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwanen, T.; Wang, D. Well-Being, Context, and Everyday Activities in Space and Time. Ann. Assoc. Am. Geogr. 2014, 104, 833–851. [Google Scholar] [CrossRef]
- Cochrane Non-Randomized Controlled Study Designs. 2020. Available online: https://childhoodcancer.cochrane.org/non-randomised-controlled-study-nrs-designs (accessed on 15 February 2020).
- Cochrane EPOC Resources for Review Authors. 2020. Available online: https://epoc.cochrane.org/resources/epoc-resources-review-authors (accessed on 15 February 2020).
- Grimshaw, J.; Campbell, M.; Ecclesa, M.; Steena, N. Experimental and quasi-experimental designs for evaluating guideline implementation strategies. Fam. Pract. 2000, 17, 11–16. [Google Scholar] [CrossRef]
- Andrews, K. The limitations of randomized controlled trials in rehabilitation research. Clin. Rehabil. 1991, 5, 5–8. [Google Scholar] [CrossRef]
- Graham, J.E.; Karmarkar, A.M.; Ottenbacher, K.J. Small sample research designs for evidence-based rehabilitation: Issues and methods. Arch. Phys. Med. Rehabil. 2012, 93, 111–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hart, T.; Whyte, J.; Poulsen, I.; Spangsberg Kristensen, K.; Nordenbo, A.M.; Chervoneva, I.; Vaccaro, M.J. How do intensity and duration of rehabilitation services affect outcomes from severe traumatic brain injury? A natural experiment comparing health care delivery systems in 2 developed nations. Arch. Phys. Med. Rehabil. 2016, 97, 2045–2053. [Google Scholar] [CrossRef]
- Prvu Bettger, J.A.; Stineman, M.G. Effectiveness of multidisciplinary rehabilitation services in postacute care: State-of-the-science. A review. Arch. Phys. Med. Rehabil. 2007, 88, 1526–1534. [Google Scholar] [CrossRef] [Green Version]
- Axelrod, D.A.; Hayward, R. Nonrandomized interventional study designs. In Clinical Research Methods for Surgeons; Penson, D.F., Wei, J.T., Eds.; Humane Press: Totowa, NJ, USA, 2007; pp. 63–76. [Google Scholar]
- Craig, P.; Cooper, C.; Gunnell, D.; Haw, S.; Lawson, K.; Macintyre, S.; Ogilvie, D.; Petticrew, M.; Reeves, B.; Sutton, M.; et al. Using natural experiments to evaluate population health interventions: New Medical Research Council guidance. J. Epidemiol. Community Health 2012, 66, 1182–1186. [Google Scholar] [CrossRef] [Green Version]
- Hallberg, K.; Eno, J. Quasi-Experimental Designs. In International Encyclopedia of the Social & Behavioral Sciences, 2nd ed.; Wright, J., Ed.; Elsevier: Amsterdam, The Netherlands, 2015; pp. 742–746. [Google Scholar]
- World Medical Association. The WMA Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects; World Medical Association: Ferney-Voltaire, France, 2018; Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 18 February 2020).
- Burke Johnson, R.; Onwuegbuzie, A.J. Mixed Methods Research. Educ. Res. 2004, 33, 14–26. [Google Scholar] [CrossRef] [Green Version]
- IAHAO White Paper. The IAHAO Definitions for Animal Assisted Intervention and Guidelines for Wellness of Animals Involved in AAI; The International Association of Human-Animal Interaction Organizations—IAHAIO: Seattle, WA, USA, 2018; Available online: https://iahaio.org/wp/wp-content/uploads/2018/04/iahaio_wp_updated-2018-final.pdf (accessed on 14 March 2020).
- PATH International. Learn about EAAT; The Professional Association of Therapeutic Horsemanship International: Denver, CO, USA, 2020; Available online: https://www.pathintl.org/resources-education/resources/eaat/193-eaat-definitions (accessed on 14 March 2020).
- Grahn, P.; Tenngart Ivarsson, C.; Stigsdotter, U.K.; Bengtsson, I.-L. Using affordances as a health promoting tool in a therapeutic garden. In Innovative Approaches to Researching Landscape and Health; Ward Thompson, C., Aspinal, P., Bell, S., Eds.; Routledge: London, UK, 2010; pp. 116–154. [Google Scholar]
- Pálsdóttir, A.M.; Grahn, P.; Persson, D. Changes in experienced value of everyday occupations after nature-based vocational rehabilitation. Scand. J. Occup. Ther. 2014, 21, 58–68. [Google Scholar] [CrossRef]
- Grahn, P.; Pálsdóttir, A.M.; Ottosson, J.; Jonsdottir, I.H. Longer nature-based rehabilitation may contribute to a faster return to work in patients with reactions to severe stress and/or depression. Int. J. Environ. Res. Public Health 2017, 14, 1310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, R.E.; Lubinsky, J. Rehabilitation Research: Principles and Applications; Elsevier: St. Louis, MO, USA, 2016. [Google Scholar]
- Eklund, M.; Erlandsson, L.-K.; Persson, D.; Hagell, P. Rasch analysis of an instrument for measuring occupational value: Implications for theory and practice. Scand. J. Occup. Ther. 2009, 16, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Persson, D. Aspects of Meaning in Everyday Occupations and Its Relationships to Health-Related Factors; Lund University: Lund, Sweden, 2001. [Google Scholar]
- Melamed, S.; Kushnir, T.; Shirom, A. Burnout and risk factors for cardiovascular diseases. Behav. Med. 1992, 18, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Shirom, A.; Melamed, S. A comparison of the construct validity of two burnout measures in two groups of professionals. Int. J. Stress Manag. 2006, 13, 176–200. [Google Scholar] [CrossRef]
- Lundgren-Nilsson, A.; Jónsdóttir, I.H.; Pallant, J.; Ahlborg, G., Jr. Internal construct validity of the Shirom-Melamed Burnout Questionnaire (SMBQ). BMC Public Health 2012, 12, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EuroQol. EQ-5D-5L User Guide. EuroQoL Research Foundation, 2019. Available online: https://euroqol.org/publications/user-guides (accessed on 18 November 2019).
- Szende, A.; Janssen, B.; Cabases, J. Self-Reported Population Health: An International Perspective Based on EQ-5D; Springer: London, UK, 2014. [Google Scholar]
- Cha, A.S.; Law, E.H.; Shaw, J.W.; Pickard, A.S. A comparison of self-rated health using EQ-5D VAS in the United States in 2002 and 2017. Qual. Life Res. 2019, 28, 3065–3069. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, S.J.; Ali, S. Health outcomes in economic evaluation: The QALY and utilities. Br. Med. Bull. 2010, 96, 5–21. [Google Scholar] [CrossRef] [Green Version]
- Tremblay, G.; de Chantal, M.; Forsythe, A.; Marsolais, C. The use of EQ-5D Visual Analog Scale (EQ-VAS) in diseases areas where EQ-5D is insensitive to changes in the disease status. Value Health 2019, 22, S901. [Google Scholar] [CrossRef]
- Freund, R.J.; Littell, R.C.; Spector, P.C. SAS System for Linear Models, 1986 ed.; SAS Institute Inc.: Cary, NC, USA, 1986. [Google Scholar]
- Goodnight, J.H. General Linear Models Procedure. In Proceedings of the First Annual SAS Users Group International Conference, Kissimmee, FL, USA, 26–28 January 1976; SAS Institute Inc.: Cary, NC, USA, 1976; pp. 1–39. [Google Scholar]
- Tukey, J. Comparing Individual Means in the Analysis of Variance. Biometrics 1949, 5, 99–114. [Google Scholar] [CrossRef]
- Pérez, M.-E.; Pericchi, L.R. Changing Statistical Significance with the Amount of Information: The Adaptive α Significance Level. Stat. Probab. Lett. 2014, 85, 20–24. [Google Scholar] [CrossRef] [Green Version]
- Jae, K. How to Choose the Level of Significance: A Pedagogical Note. In Munich Personal RePEc Archive MPRA Paper; 2015; Available online: https://mpra.ub.uni-muenchen.de/66373/ (accessed on 18 November 2019).
- Kim, J.H.; Choi, I. Choosing the Level of Significance: A Decision-theoretic Approach. Abacus A J. Account. Financ. Bus. Stud. 2019. [Google Scholar] [CrossRef]
- Thiese, M.S.; Ronna, B.; Ott, U. P value interpretations and considerations. J. Thorac. Dis. 2016, 8, E928–E931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahiru, T. P-value, a true test of statistical significance? A cautionary note. Ann. Ib. Postgrad. Med. 2008, 6, 21–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, G.M.; Feinn, R. Using Effect Size—Or Why the P Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Earlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Hedges, L.V. Distribution theory for Glass’ estimator of effect size and related estimators. J. Educ. Stat. 1981, 6, 107–128. [Google Scholar] [CrossRef]
- Smith, J.A. Interpretative Phenomenological Analysis. Theory, Method and Research; SAGE: London, UK, 2009. [Google Scholar]
- Lundquist Wanneberg, P. Disability, Riding, and Identity: A Qualitative Study on the Influence of Riding on the Identity Construction of People with Disabilities. Int. J Dis. Dev. Educ. 2014, 61, 67–79. [Google Scholar] [CrossRef] [Green Version]
- Nygårdh, A.; Malm, D.; Wikby, K.; Ahlström, G. The experience of empowerment in the patient-staff encounter: The patient’s perspective. J. Clin. Nurs. 2011, 21, 897–904. [Google Scholar] [CrossRef]
- Hammell, K.W. Dimensions of meaning in the occupations of daily life. Can. J. Occup. 2004, 71, 296–305. [Google Scholar] [CrossRef]
- Persson, D.; Erlandsson, L.-K.; Eklund, M.; Iwarsson, S. Value dimensions, meaning and complexity in human occupation: A tentative structure for analysis. Scand. J. Occupther. 2001, 8, 7–18. [Google Scholar] [CrossRef]
- Erlandsson, L.-K.; Eklund, M.; Persson, D. Occupational value and relationships to meaning and health: Elaborations of the ValMO model. Scand. J. Occup. 2011, 18, 72–80. [Google Scholar] [CrossRef]
- Julius, H.; Beetz, A.; Kotrschal, K.; Turner, D.; Uvnäs-Moberg, K. Attachment to Pets; Hogrefe Publishing: Göttingen, Germany, 2013. [Google Scholar]
- Beetz, A.; Uvnäs-Moberg, K.; Julius, H.; Kotrschal, K. Psychosocial and psychophysiological effects of human-animal interactions: The possible role of oxytocin. Front. Psychol. 2012, 234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byström, K.; Grahn, P.; Hägerhäll, C. Vitality from Experiences in Nature and Contact with Animals—A Way to Develop Joint Attention and Social Engagement in Children with Autism? Int. J. Environ. Res. Public Health 2019, 16, 4673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pálsdóttir, A.M.; Persson, D.; Persson, B.; Grahn, P. The Journey of recovery and empowerment embraced by nature—Clients’ perspectives on nature-based rehabilitation in relation to the role for the natural environment. Special Issue: Health benefits of nature. Int. J. Environ. Res. Public Health 2014, 11, 7094–7115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corazon, S.S.; Olsen, L.J.; Olse, A.-M.; Sidenius, U. Nature-Based Therapy for people suffering from post-Concussion Syndrome—A Pilot Study. Health 2019, 11, 1501–1517. [Google Scholar] [CrossRef] [Green Version]
- Sahlin, E.; Johansson, B.; Karlsson, P.O.; Loberg, J.; Niklasson, M.; Grahn, P. Improved Wellbeing for Both Caretakers and Users from A Zoo-Related Nature Based Intervention—A Study at Nordens Ark Zoo, Sweden. Int. J. Environ. Res. Public Health 2019, 16, 4929. [Google Scholar] [CrossRef] [Green Version]
- Socialstyrelsen, Nationella riktlinjer för sjukdomsförebyggande metoder 2011. Tobaksbruk, riskbruk av alkohol, otillräcklig fysisk aktivitet och ohälsosamma matvanor. Stöd för styrning och ledning. Board Health Welf. 2011. Available online: https://www.swenurse.se/ (accessed on 18 November 2019). (In Swedish).
- Bunkertorp-Käll, L.; Lundgren-Nilsson, Å.; Samuelsson, H.; Pekny, T.; Blomvé, K.; Pekna, M.; Pekny, M.; Blomstrand, C.; Nilsson, M. Long-term improvements after multimodal rehabilitation in late phase after troke—A randomized controlled trial. Stroke 2017, 48, 1916–1924. [Google Scholar] [CrossRef]
- Pohl, P.; Carlsson, G.; Bunkertorp Käll, L.; Nilsson, M.; Blomstrand, C. A qualitative exploration of post-acute stroke participant’ experiences of multimodal intervention incorporating horseback riding. PLoS ONE 2018, 13, e0203933. [Google Scholar] [CrossRef] [Green Version]
- Ho, S.H.; Lin, C.J.; Ku, F.L. The effects of gardening on quality of life in people with stroke. Work (Read. Mass) 2016, 54, 557–567. [Google Scholar] [CrossRef]
- Johansson, B.; Starmark, A.; Berglund, P.; Rödholm, M.; Rönnbäck, L. A self-assessment questionnaire for mental fatigue and related symptoms after neurological disorders and injuries. Brain Inj. 2010, 24, 2–12. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention | Active | Passive | |
|---|---|---|---|
| Participants | 14 | 147 | 29 |
| Women (men) | 12 (2) | 110 (37) | 24 (5) |
| Mean age (distribution) | 52 (22–71) | 55 (27–84) | 51 (19–69) |
| Active, times/week | 1 | 3.7 | 0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pálsdóttir, A.M.; Gudmundsson, M.; Grahn, P. Equine-Assisted Intervention to Improve Perceived Value of Everyday Occupations and Quality of Life in People with Lifelong Neurological Disorders: A Prospective Controlled Study. Int. J. Environ. Res. Public Health 2020, 17, 2431. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072431
Pálsdóttir AM, Gudmundsson M, Grahn P. Equine-Assisted Intervention to Improve Perceived Value of Everyday Occupations and Quality of Life in People with Lifelong Neurological Disorders: A Prospective Controlled Study. International Journal of Environmental Research and Public Health. 2020; 17(7):2431. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072431
Chicago/Turabian StylePálsdóttir, Anna María, Marie Gudmundsson, and Patrik Grahn. 2020. "Equine-Assisted Intervention to Improve Perceived Value of Everyday Occupations and Quality of Life in People with Lifelong Neurological Disorders: A Prospective Controlled Study" International Journal of Environmental Research and Public Health 17, no. 7: 2431. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072431