The Relationship of IL-8 and IL-10 Myokines and Performance in Male Marathon Runners Presenting Exercise-Induced Bronchoconstriction

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Methods
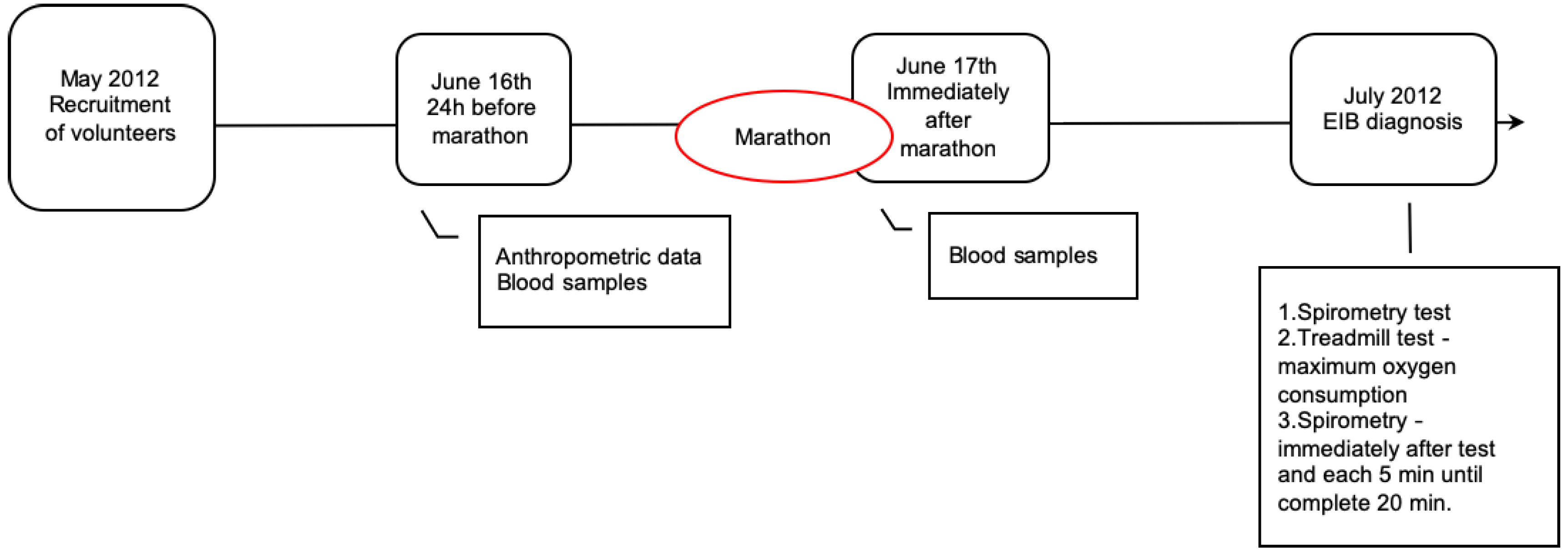
2.1. Subjects and Study Design
2.2. Cytokines Measurements and Cellular Counting
2.3. Evaluation of Aerobic and Pulmonary Capacity
2.4. Statistical Analysis
2.5. Data Availability Statement
3. Results
3.1. Physical Characteristics, and Pulmonary and Aerobic Capacity of All Volunteers
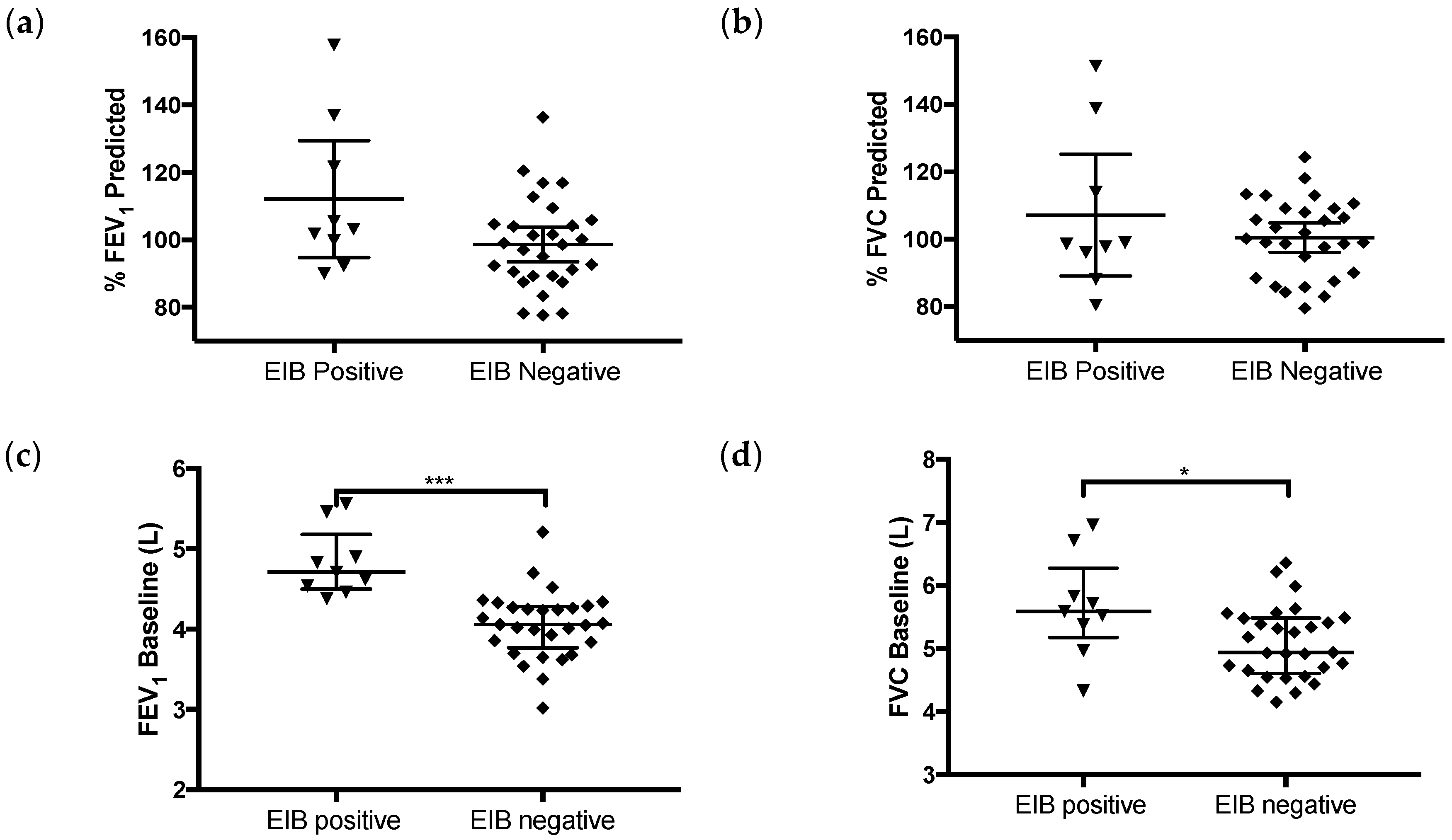
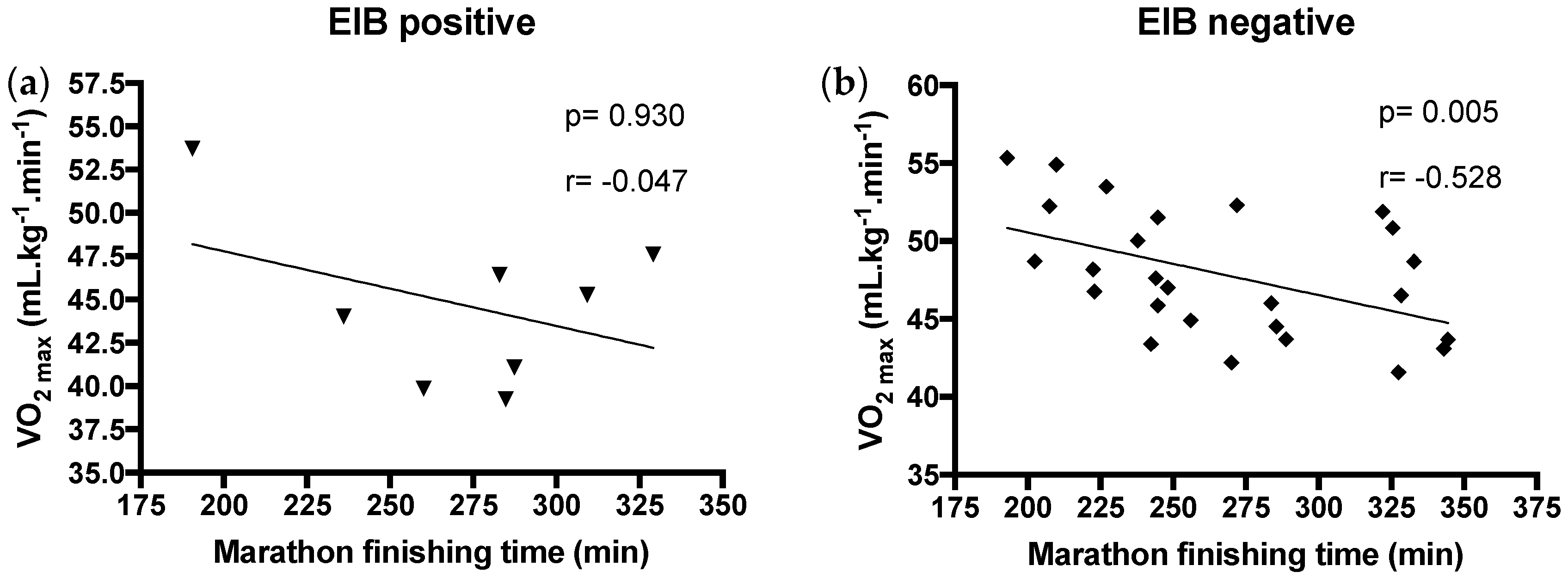
3.2. Exercise-Induced Bronchoconstriction Diagnosis, Pulmonary and Aerobic Capacity, and Performance of Volunteers Presenting or not EIB
3.3. Inflammatory Markers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- MacCallum, D.S.; Comeau, D. Exercise-Induced Bronchoconstriction. Curr. Sports Med. Rep. 2016, 15, 128–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbasi, A.; Vieira, R.P.; Northoff, H. Letter to the editor: The evidence of exercise-induced bronchoconstriction in endurance runners; genetic basis and gender differences. Exerc. Immunol. Rev. 2015, 21, 186–188. [Google Scholar] [PubMed]
- Bonini, M.; Gramiccioni, C.; Fioretti, D.; Ruckert, B.; Rinaldi, M.; Akdis, C.; Todaro, A.; Palange, P.; Carlsen, K.H.; Pelliccia, A.; et al. Asthma, allergy and the Olympics: A 12-year survey in elite athletes. Curr. Opin. Allergy Clin. Immunol. 2015, 15, 184–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torrie, A.M.; Craig, T.J. Exercise-Induced Bronchoconstriction. In Allergy and Asthma; Springer: Berlin, Germany, 2016; pp. 241–251. [Google Scholar]
- Kippelen, P.; Anderson, S.D.; Hallstrand, T.S. Mechanisms and biomarkers of exercise-induced bronchoconstriction. Immunol. Allergy Clin. 2018, 38, 165–182. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, B.; Mulgirigama, A.; Berend, N. Exercise-induced bronchoconstriction: Prevalence, pathophysiology, patient impact, diagnosis and management. NPJ Prim. Care Respir. Med. 2018, 28, 31. [Google Scholar] [CrossRef]
- Couto, M.; Kurowski, M.; Moreira, A.; Bullens, D.M.A.; Carlsen, K.H.; Delgado, L.; Kowalski, M.L.; Seys, S.F. Mechanisms of exercise-induced bronchoconstriction in athletes: Current perspectives and future challenges. Allergy 2018, 73, 8–16. [Google Scholar] [CrossRef] [Green Version]
- Seys, S.F.; Hox, V.; Van Gerven, L.; Dilissen, E.; Marijsse, G.; Peeters, E.; Dekimpe, E.; Kasran, A.; Aertgeerts, S.; Troosters, T.; et al. Damage-associated molecular pattern and innate cytokine release in the airways of competitive swimmers. Allergy 2015, 70, 187–194. [Google Scholar] [CrossRef]
- Pasnick, S.D.; Carlos, W.G.; Arunachalam, A.; Celestin, F.M.; Parsons, J.P.; Hallstrand, T.S.; Anderson, S.D.; Wilson, K.C.; Thomson, C.C.; Force, A.T.S.I.T. Exercise-induced bronchoconstriction. Ann. Am. Thorac. Soc. 2014, 11, 1651–1652. [Google Scholar] [CrossRef]
- Rundell, K.W.; Slee, J.B. Exercise and other indirect challenges to demonstrate asthma or exercise-induced bronchoconstriction in athletes. J. Allergy Clin. Immunol. 2008, 122, 238–246. [Google Scholar] [CrossRef]
- Holzer, K.; Anderson, S.D.; Douglass, J. Exercise in elite summer athletes: Challenges for diagnosis. J. Allergy Clin. Immunol. 2002, 110, 374–380. [Google Scholar] [CrossRef]
- Esteve-Lanao, J.; Lucia, A.; deKoning, J.J.; Foster, C. How do humans control physiological strain during strenuous endurance exercise? PLoS ONE 2008, 3, e2943. [Google Scholar] [CrossRef] [PubMed]
- Vaisberg, M.; Suguri, V.M.; Gregorio, L.C.; Lopes, J.D.; Bachi, A.L. Cytokine kinetics in nasal mucosa and sera: New insights in understanding upper-airway disease of marathon runners. Exerc. Immunol. Rev. 2013, 19, 49–59. [Google Scholar] [PubMed]
- Andersen, J. The State of Running 2019. Available online: https://runrepeat.com/state-of-running (accessed on 15 January 2020).
- Nieman, D.C.; Henson, D.A.; Smith, L.L.; Utter, A.C.; Vinci, D.M.; Davis, J.M.; Kaminsky, D.E.; Shute, M. Cytokine changes after a marathon race. J. Appl. Physiol. (1985) 2001, 91, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Niemelä, M.; Kangastupa, P.; Niemelä, O.; Bloigu, R.; Juvonen, T. Acute Changes in Inflammatory Biomarker Levels in Recreational Runners Participating in a Marathon or Half-Marathon. Sports Med. Open 2016, 2, 21. [Google Scholar] [CrossRef] [Green Version]
- Coates, A.L.; Wanger, J.; Cockcroft, D.W.; Culver, B.H.; Carlsen, K.-H.; Diamant, Z.; Gauvreau, G.; Hall, G.L.; Hallstrand, T.S.; Horvath, I. ERS technical standard on bronchial challenge testing: General considerations and performance of methacholine challenge tests. Eur. Respir. J. 2017, 49, 1601526. [Google Scholar] [CrossRef] [Green Version]
- Sierra, A.P.; Oliveira-Junior, M.C.; Almeida, F.M.; Benetti, M.; Oliveira, R.; Felix, S.N.; Genaro, I.S.; Romanholo, B.M.S.; Ghorayeb, N.; Kiss, M.A.P.D.; et al. Impairment on Cardiopulmonary Function after Marathon: Role of Exhaled Nitric Oxide. Oxid. Med. Cell. Longev. 2019, 2019, 5134360. [Google Scholar] [CrossRef]
- Becker, J.M.; Rogers, J.; Rossini, G.; Mirchandani, H.; D’Alonzo, G.E. Asthma deaths during sports: Report of a 7-year experience. J. Allergy Clin. Immunol. 2004, 113, 264–267. [Google Scholar] [CrossRef]
- Parsons, J.P.; Mastronarde, J.G. Exercise-induced bronchoconstriction in athletes. Chest 2005, 128, 3966–3974. [Google Scholar] [CrossRef]
- Carlsen, K.H.; Anderson, S.D.; Bjermer, L.; Bonini, S.; Brusasco, V.; Canonica, W.; Cummiskey, J.; Delgado, L.; Del Giacco, S.R.; Drobnic, F.; et al. Exercise-induced asthma, respiratory and allergic disorders in elite athletes: Epidemiology, mechanisms and diagnosis: Part I of the report from the Joint Task Force of the European Respiratory Society (ERS) and the European Academy of Allergy and Clinical Immunology (EAACI) in cooperation with GA2LEN. Allergy 2008, 63, 387–403. [Google Scholar]
- Teixeira, R.N.; Teixeira, L.R.; Costa, L.A.; Martins, M.A.; Mickleborough, T.D.; Carvalho, C.R. Exercise-induced bronchoconstriction in elite long-distance runners in Brazil. J. Bras. Pneumol. 2012, 38, 292–298. [Google Scholar] [CrossRef] [Green Version]
- Bekos, C.; Zimmermann, M.; Unger, L.; Janik, S.; Mitterbauer, A.; Koller, M.; Fritz, R.; Gäbler, C.; Didcock, J.; Kliman, J.; et al. Exercise-induced bronchoconstriction, temperature regulation and the role of heat shock proteins in non-asthmatic recreational marathon and half-marathon runners. Sci. Rep. 2019, 9, 4168. [Google Scholar] [CrossRef] [PubMed]
- Bassett, D.R.; Howley, E.T. Limiting factors for maximum oxygen uptake and determinants of endurance performance. Med. Sci. Sports Exerc. 2000, 32, 70–84. [Google Scholar] [CrossRef] [PubMed]
- ACSM. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2013. [Google Scholar]
- Bozzini, B.; Pellegrino, J.; Walker, A.; McFadden, B.; Poyssick, A.; Arent, S. Running economy and its correlation to performance and fitness variables in recreationally-trained distance runners. Comp. Exerc. Physiol. 2020, 16, 107–112. [Google Scholar] [CrossRef]
- Junior, L.A.L.; dos Santo, J.d.M.B.; Bachi, A.L.L.; Foster, R.; Amaro, A.S.; de Oliveira, A.P.L.; Sierra, A.P.R.; Kiss, M.A.P.D.M.; Vaisberg, M.W. Relationship between cytokines and running economy in marathon runners. Open Life Sci. 2016, 11, 308–312. [Google Scholar] [CrossRef]
- Walsh, N.P.; Gleeson, M.; Shephard, R.J.; Woods, J.A.; Bishop, N.C.; Fleshner, M.; Green, C.; Pedersen, B.K.; Hoffman-Goetz, L.; Rogers, C.J.; et al. Position statement. Part one: Immune function and exercise. Exerc. Immunol. Rev. 2011, 17, 6–63. [Google Scholar]
- Branchett, W.J.; Lloyd, C.M. Regulatory cytokine function in the respiratory tract. Mucosal Immunol. 2019, 12, 589–600. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, B.K.; Akerström, T.C.; Nielsen, A.R.; Fischer, C.P. Role of myokines in exercise and metabolism. J. Appl. Physiol. (1985) 2007, 103, 1093–1098. [Google Scholar] [CrossRef] [Green Version]
- Sessions, J.; Bourbeau, K.; Rosinski, M.; Szczygiel, T.; Nelson, R.; Sharma, N.; Zuhl, M. Carbohydrate gel ingestion during running in the heat on markers of gastrointestinal distress. Eur. J. Sport Sci. 2016, 16, 1064–1072. [Google Scholar] [CrossRef]
- Bachi, A.L.; Rios, F.J.; Vaisberg, P.H.; Martins, M.; de Sá, M.C.; Victorino, A.B.; Foster, R.; Sierra, A.P.; Kiss, M.A.; Vaisberg, M. Neuro-immuno-endocrine modulation in marathon runners. Neuroimmunomodulation 2015, 22, 196–202. [Google Scholar] [CrossRef]
- Vaisberg, M.; Paixão, V.; Almeida, E.B.; Santos, J.M.B.; Foster, R.; Rossi, M.; Pithon-Curi, T.C.; Gorjão, R.; Momesso, C.M.; Andrade, M.S.; et al. Daily Intake of Fermented Milk Containing. Nutrients 2019, 11, 1678. [Google Scholar] [CrossRef] [Green Version]
- Passos, B.N.; Lima, M.C.; Sierra, A.P.R.; Oliveira, R.A.; Maciel, J.F.S.; Manoel, R.; Rogante, J.I.; Pesquero, J.B.; Cury-Boaventura, M.F. Association of Daily Dietary Intake and Inflammation Induced by Marathon Race. Mediat. Inflamm. 2019, 2019, 1537274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neidhart, M.; Müller-Ladner, U.; Frey, W.; Bosserhoff, A.K.; Colombani, P.C.; Frey-Rindova, P.; Hummel, K.M.; Gay, R.E.; Häuselmann, H.; Gay, S. Increased serum levels of non-collagenous matrix proteins (cartilage oligomeric matrix protein and melanoma inhibitory activity) in marathon runners. Osteoarthr. Cartil. 2000, 8, 222–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baggiolini, M.; Walz, A.; Kunkel, S.L. Neutrophil-activating peptide-1/interleukin 8, a novel cytokine that activates neutrophils. J. Clin. Investig. 1989, 84, 1045–1049. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, A.R.; Pedersen, B.K. The biological roles of exercise-induced cytokines: IL-6, IL-8, and IL-15. Appl. Physiol. Nutr. Metab. 2007, 32, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Akerstrom, T.; Steensberg, A.; Keller, P.; Keller, C.; Penkowa, M.; Pedersen, B.K. Exercise induces interleukin-8 expression in human skeletal muscle. J. Physiol. 2005, 563 Pt 2, 507–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buford, T.W.; Cooke, M.B.; Shelmadine, B.D.; Hudson, G.M.; Redd, L.; Willoughby, D.S. Effects of eccentric treadmill exercise on inflammatory gene expression in human skeletal muscle. Appl. Physiol. Nutr. Metab. 2009, 34, 745–753. [Google Scholar] [CrossRef]
- Frydelund-Larsen, L.; Penkowa, M.; Akerstrom, T.; Zankari, A.; Nielsen, S.; Pedersen, B.K. Exercise induces interleukin-8 receptor (CXCR2) expression in human skeletal muscle. Exp. Physiol. 2007, 92, 233–240. [Google Scholar] [CrossRef] [Green Version]
- Chimenti, L.; Morici, G.; Paternò, A.; Santagata, R.; Bonanno, A.; Profita, M.; Riccobono, L.; Bellia, V.; Bonsignore, M.R. Bronchial epithelial damage after a half-marathon in nonasthmatic amateur runners. Am. J. Physiol. Lung Cell. Mol. Physiol. 2010, 298, L857–L862. [Google Scholar] [CrossRef] [Green Version]
- McGrath-Morrow, S.A.; Collaco, J.M.; Detrick, B.; Lederman, H.M. Serum Interleukin-6 Levels and Pulmonary Function in Ataxia-Telangiectasia. J. Pediatrics 2016, 171, 256–261. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, C.J.; Quigley, K.; Cheng, X.; Suresh, A.; Tahir, S.; Ahmed-Jushuf, F.; Nawab, K.; Choy, K.; Walker, S.A.; Mathie, S.A.; et al. Lung Defense through IL-8 Carries a Cost of Chronic Lung Remodeling and Impaired Function. Am. J. Respir. Cell Mol. Biol. 2018, 59, 557–571. [Google Scholar] [CrossRef]
- Adegoke, S.A.; Kuti, B.P.; Omole, K.O.; Smith, O.S.; Oyelami, O.A.; Adeodu, O.O. Acute chest syndrome in sickle cell anaemia: Higher serum levels of interleukin-8 and highly sensitive C-reactive proteins are associated with impaired lung function. Paediatr. Int. Child Health 2018, 38, 244–250. [Google Scholar] [CrossRef] [PubMed]
- LeVan, T.D.; Romberger, D.J.; Siahpush, M.; Grimm, B.L.; Ramos, A.K.; Johansson, P.L.; Michaud, T.L.; Heires, A.J.; Wyatt, T.A.; Poole, J.A. Relationship of systemic IL-10 levels with proinflammatory cytokine responsiveness and lung function in agriculture workers. Respir. Res. 2018, 19, 166. [Google Scholar] [CrossRef] [PubMed]
- Santos, J.M.B.D.; Foster, R.; Jonckheere, A.C.; Rossi, M.; Luna Junior, L.A.; Katekaru, C.M.; de Sá, M.C.; Pagani, L.G.; Almeida, F.M.; Amaral, J.D.B.; et al. Outdoor Endurance Training with Air Pollutant Exposure Versus Sedentary Lifestyle: A Comparison of Airway Immune Responses. Int. J. Environ. Res. Public Health 2019, 16, 4418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.; Nyasha, M.R.; Koide, M.; Tsuchiya, M.; Suzuki, N.; Hagiwara, Y.; Aoki, M.; Kanzaki, M. In vitro exercise model using contractile human and mouse hybrid myotubes. Sci. Rep. 2019, 9, 11914. [Google Scholar] [CrossRef] [PubMed]
- Leal, L.G.; Lopes, M.A.; Batista, M.L. Physical Exercise-Induced Myokines and Muscle-Adipose Tissue Crosstalk: A Review of Current Knowledge and the Implications for Health and Metabolic Diseases. Front. Physiol. 2018, 9, 1307. [Google Scholar] [CrossRef]
- Perrin, L.; Loizides-Mangold, U.; Skarupelova, S.; Pulimeno, P.; Chanon, S.; Robert, M.; Bouzakri, K.; Modoux, C.; Roux-Lombard, P.; Vidal, H.; et al. Human skeletal myotubes display a cell-autonomous circadian clock implicated in basal myokine secretion. Mol. Metab. 2015, 4, 834–845. [Google Scholar] [CrossRef]
- Rigonato-Oliveira, N.C.; Mackenzie, B.; Bachi, A.L.L.; Oliveira-Junior, M.C.; Santos-Dias, A.; Brandao-Rangel, M.A.R.; Delle, H.; Costa-Guimaraes, T.; Damaceno-Rodrigues, N.R.; Dulley, N.R.; et al. Aerobic exercise inhibits acute lung injury: From mouse to human evidence Exercise reduced lung injury markers in mouse and in cells. Exerc. Immunol. Rev. 2018, 24, 36–44. [Google Scholar]
- Andrade-Sousa, A.S.; Rogério Pereira, P.; MacKenzie, B.; Oliveira-Junior, M.C.; Assumpção-Neto, E.; Brandão-Rangel, M.A.; Damaceno-Rodrigues, N.R.; Garcia Caldini, E.; Velosa, A.P.; Teodoro, W.R.; et al. Aerobic Exercise Attenuated Bleomycin-Induced Lung Fibrosis in Th2-Dominant Mice. PLoS ONE 2016, 11, e0163420. [Google Scholar] [CrossRef]
- Stelmach, I.; Zaczeniuk, M.; Sztafińska, A.; Majak, P.; Jerzyńska, J.; Kuklinska-Pijanka, A.; Stelmach, W. Serum tryptase level and inflammatory markers in exhaled breath condensate of children with exercise-induced symptoms. Allergy Asthma Proc. 2016, 37, 84–92. [Google Scholar] [CrossRef]
- Flohr, C.; Tuyen, L.; Quinnell, R.; Lewis, S.; Minh, T.; Campbell, J.; Simmons, C.; Telford, G.; Brown, A.; Hien, T. Reduced helminth burden increases allergen skin sensitization but not clinical allergy: A randomized, double-blind, placebo-controlled trial in Vietnam. Clin. Exp. Allergy 2010, 40, 131–142. [Google Scholar] [CrossRef]
- Ricciardolo, F.L.; Sorbello, V.; Ciprandi, G. FeNO as biomarker for asthma phenotyping and management. Allergy Asthma Proc. 2015, 36, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Schoos, A.M.; Christiansen, C.F.; Stokholm, J.; Bønnelykke, K.; Bisgaard, H.; Chawes, B.L. FeNO and Exercise Testing in Children at Risk of Asthma. J. Allergy Clin. Immunol. Pract. 2018, 6, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Kotsiou, O.S.; Peletidou, S.; Vavougios, G.; Karetsi, E.; Stavrou, V.; Zakynthinos, G.; Gourgoulianis, K.I.; Daniil, Z. Exhaled nitric oxide as a marker of chlorine exposure in young asthmatic swimmers. Ann. Allergy Asthma Immunol. 2019, 123, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Pagani, L.G.; Santos, J.; Foster, R.; Rossi, M.; Luna Junior, L.A.; Katekaru, C.M.; de Sá, M.C.; Jonckheere, A.-C.; Almeida, F.M.; Amaral, J.B. The Effect of Particulate Matter Exposure on the Inflammatory Airway Response of Street Runners and Sedentary People. Atmosphere 2020, 11, 43. [Google Scholar] [CrossRef] [Green Version]
- Nikolaidis, P.T.; Di Gangi, S.; Chtourou, H.; Rüst, C.A.; Rosemann, T.; Knechtle, B. The Role of Environmental Conditions on Marathon Running Performance in Men Competing in Boston Marathon from 1897 to 2018. Int. J. Environ. Res. Public Health 2019, 16, 614. [Google Scholar] [CrossRef] [Green Version]
- Foster, R.; Vaisberg, M.; Bachi, A.L.L.; Dos Santos, J.M.B.; de Paula Vieira, R.; Luna-Junior, L.A.; Araújo, M.P.; Parmigiano, T.R.; Borges, F.; Di-Bella, Z.I.K.J. Premenstrual Syndrome, Inflammatory Status, and Mood States in Soccer Players. Neuroimmunomodulation 2019, 26, 1–6. [Google Scholar] [CrossRef]
- Robson-Ansley, P.; Howatson, G.; Tallent, J.; Mitcheson, K.; Walshe, I.; Toms, C.; DU Toit, G.; Smith, M.; Ansley, L. Prevalence of allergy and upper respiratory tract symptoms in runners of the London marathon. Med. Sci. Sports Exerc. 2012, 44, 999–1004. [Google Scholar] [CrossRef] [Green Version]
- Qin, F.; Yang, Y.; Wang, S.T.; Dong, Y.N.; Xu, M.X.; Wang, Z.W.; Zhao, J.X. Exercise and air pollutants exposure: A systematic review and meta-analysis. Life Sci. 2019, 218, 153–164. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Minimum | 25% Percentile | Median | 75% Percentile | Maximum |
|---|---|---|---|---|---|
| Age (years) | 24.0 | 33.0 | 38.5 | 44.0 | 56.0 |
| Height (cm) | 166.5 | 172.0 | 175.5 | 180.3 | 193.5 |
| Weight (kg) | 56.2 | 69.3 | 74.7 | 81.6 | 101.4 |
| Fat (%) | 3.0 | 15.3 | 18.6 | 20.8 | 25.7 |
| Body mass index | 19.0 | 22.4 | 24.6 | 25.9 | 30.3 |
| Predicted max HR (beats/min) | 164.0 | 176.0 | 181.5 | 187.0 | 196.0 |
| Maximal heart rate (beats/min) | 167.0 | 180.0 | 185.5 | 191.0 | 206.0 |
| % of predicted max HR (%) | 91.0 | 99.0 | 102.0 | 16.3 | 113.0 |
| Duration of test (min) | 7.7 | 10.1 | 11.5 | 12.0 | 13.8 |
| VO2 max (mL kg−1 min−1) | 38.0 | 43.6 | 46.6 | 50.2 | 55.3 |
| VO2 aerobic threshold (mL kg−1 min−1) | 28.7 | 32.7 | 34.9 | 38.4 | 47.6 |
| VO2 lactate threshold (mL kg−1 min−1) | 34.1 | 40.9 | 44.0 | 47.6 | 52.7 |
| Maximal ventilation (L) | 111.6 | 139.6 | 153.2 | 170.2 | 193.5 |
| Maximal respiratory exchange ratio (L) | 1.0 | 1.1 | 1.2 | 1.2 | 1.4 |
| Marathon finishing time (min) | 190.7 | 233.8 | 265.1 | 312.5 | 344.6 |
| Predicted FVC (L) | 4.4 | 4.8 | 5.1 | 5.5 | 6.3 |
| FVC baseline (L) | 4.2 | 4.7 | 5.3 | 5.6 | 7.0 |
| % of predicted FVC baseline (%) | 79.6 | 89.7 | 99.1 | 109.6 | 151.4 |
| FVC 0 min (L) | 4.1 | 4.6 | 5.0 | 5.4 | 6.3 |
| FVC 5 min (L) | 4.0 | 4.7 | 5.1 | 5.5 | 6.6 |
| FVC 10 min (L) | 3.7 | 4.7 | 5.1 | 5.4 | 6.4 |
| FVC 15 min (L) | 3.5 | 4.7 | 5.2 | 5.4 | 6.8 |
| FVC 20 min (L) | 4.2 | 4.7 | 5.2 | 5.5 | 6.4 |
| Predicted FEV1 (L) | 3.4 | 3.8 | 4.2 | 4.5 | 5.2 |
| FEV1 baseline (L) | 3.0 | 3.9 | 4.2 | 4.5 | 5.6 |
| % of predicted FEV1 baseline (%) | 77.7 | 90.5 | 100 | 106.8 | 157.8 |
| FEV1 0 min (L) | 3.2 | 3.9 | 4.2 | 4.5 | 5.8 |
| FEV1 5 min (L) | 3.3 | 3.9 | 4.1 | 4.4 | 5.7 |
| FEV1 10 min (L) | 3.2 | 3.8 | 4.2 | 4.4 | 5.3 |
| FEV1 15 min (L) | 3.3 | 3.8 | 4.1 | 4.4 | 5.6 |
| FEV1 20 min (L) | 3.2 | 3.8 | 4.2 | 4.5 | 5.4 |
| Volunteer | Absolut Values (L) | Relative Values (%) | Difference | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ID # | FEV1 Baseline | FEV1 0 min | FEV1 5 min | FEV1 10 min | FEV1 15 min | FEV1 20 min | FEV1 0 min | FEV1 5 min | FEV1 10 min | FEV1 15 min | FEV1 20 min | FEV1 % Maximal Fall |
| 7 | 5.46 | 3.72 | 4.04 | 3.57 | 3.65 | 3.57 | 68 | 74 | 65 | 67 | 65 | −35 |
| 12 | 4.83 | 4.24 | 3.72 | 4.02 | 3.74 | 4.6 | 88 | 77 | 83 | 77 | 95 | −23 |
| 6 | 4.38 | 3.95 | 3.87 | 3.45 | 3.66 | 4.48 | 90 | 88 | 79 | 84 | 102 | −21 |
| 25 | 5.56 | 4.63 | 4.43 | 4.73 | 5.57 | 5.39 | 83 | 80 | 85 | 100 | 97 | −20 |
| 32 | 4.54 | 3.75 | 3.66 | 3.73 | 3.75 | 3.75 | 83 | 81 | 82 | 83 | 83 | −19 |
| 24 | 4.46 | 4.21 | 4.79 | 4.1 | 4.08 | 3.73 | 94 | 107 | 92 | 91 | 84 | −16 |
| 9 | 4.62 | 4.31 | 4.05 | 4.01 | 3.94 | 3.92 | 93 | 88 | 87 | 85 | 85 | −15 |
| 8 | 4.9 | 4.53 | 4.59 | 4.23 | 4.75 | 4.41 | 92 | 94 | 86 | 97 | 90 | −14 |
| 49 | 4.71 | 4.52 | 4.2 | 4.33 | 4.43 | 4.55 | 96 | 89 | 92 | 94 | 97 | −11 |
| Variables | EIB Positive (n = 9) | EIB Positive (n = 29) | ||||
|---|---|---|---|---|---|---|
| Baseline | Immediately after | Baseline | Immediately after | |||
| IL-1β (pg/mL) | 0.02 [0.01–0.21] | 0.13 [0.00–0.27] | 0.14 [0.05–0.27] | 0.20 [0.13–0.42] | ||
| IL-4 (pg/mL) | 0.00 [0.00–0.00] | 0.00 [0.00–2.30] | 0.00 [0.00–0.80] | 0.00 [0.00–4.68] | ||
| IL-6 (pg/mL) | 0.03 [0.00–0.12] | 23.23 [20.48–32.16] | * | 0.08 [0.03–0.18] | 28.81 [18.41–52.38] | * |
| IL-8 (pg/mL) | 1.62 [1.37–3.38] | 15.28 [7.35–19.83] | * | 2.74 [1.70–4.89] | 16.53 [10.35–24.46] | * |
| IL-10 (pg/mL) | 0.06 [0.00–1.14] | 64.13 [15.88–262.5] | * | 0.27 [0.07–0.93] | 80.83 [30.80–215.90] | * |
| TNF-α (pg/mL) | 5.78 [4.52–7.95] | 12.32 [9.39–15.19] | * | 7.95 [5.99–9.43] | 11.07 [9.04–15.52] | * |
| CPK (U/L) | 145.0 [93.5–454.0] | 496.0 [197.5–979.5] | * | 309.0 [134.0–261.8] | 490.5 [328.3–710.0] | * |
| HSPCR (mg/dL) | 0.12 [0.07–0.19] | 0.15 [0.08–0.25] | 0.07 [0.02–0.13] | 0.09 [0.03–0.15] | ||
| Parameters | EIB Positive | EIB Negative | ||
|---|---|---|---|---|
| Marathon Finishing Time | Marathon Finishing Time | |||
| r | p | r | p | |
| IL-1β Baseline | 0.4671 | 0.246 | 0.0271 | 0.898 |
| IL-1β Immediately after | 0.6138 | 0.115 | 0.3807 | 0.061 |
| IL-4 Baseline | −0.2474 | 0.750 | 0.0316 | 0.881 |
| IL-4 Immediately after | −0.1559 | 0.750 | 0.2054 | 0.325 |
| IL-6 Baseline | 0.5279 | 0.186 | 0.4387 | 0.028 |
| IL-6 Immediately after | −0.4286 | 0.299 | 0.1436 | 0.494 |
| IL-8 Baseline | 0.0476 | 0.935 | 0.1267 | 0.546 |
| IL-8 Immediately after | −0.8095 | 0.022 | −0.0535 | 0.800 |
| IL-10 Baseline | 0.0488 | 0.928 | 0.0768 | 0.715 |
| IL-10 Immediately after | −0.9762 | ≤0.001 | −0.2718 | 0.189 |
| TNF-α Baseline | 0.5952 | 0.132 | −0.0359 | 0.865 |
| TNF-α Immediately after | −0.3095 | 0.462 | −0.1471 | 0.483 |
| CPK Baseline | 0.5476 | 0.171 | −0.0551 | 0.794 |
| CPK Immediately after | 0.6190 | 0.115 | 0.1121 | 0.594 |
| HSCRP Baseline | 0.6071 | 0.167 | 0.0027 | 0.990 |
| HSCRP Immediately after | 0.7143 | 0.058 | 0.0222 | 0.916 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, J.d.M.B.d.; Bachi, A.L.L.; Luna Junior, L.A.; Foster, R.; Sierra, A.P.R.; Benetti, M.; Araújo, J.R.; Ghorayeb, N.; Kiss, M.A.P.D.; Vieira, R.P.; et al. The Relationship of IL-8 and IL-10 Myokines and Performance in Male Marathon Runners Presenting Exercise-Induced Bronchoconstriction. Int. J. Environ. Res. Public Health 2020, 17, 2622. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082622
Santos JdMBd, Bachi ALL, Luna Junior LA, Foster R, Sierra APR, Benetti M, Araújo JR, Ghorayeb N, Kiss MAPD, Vieira RP, et al. The Relationship of IL-8 and IL-10 Myokines and Performance in Male Marathon Runners Presenting Exercise-Induced Bronchoconstriction. International Journal of Environmental Research and Public Health. 2020; 17(8):2622. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082622
Chicago/Turabian StyleSantos, Juliana de Melo Batista dos, André Luis Lacerda Bachi, Luiz Antonio Luna Junior, Roberta Foster, Ana Paula Renno Sierra, Marino Benetti, José Roberto Araújo, Nabil Ghorayeb, Maria Augusta Peduti Dal’Molim Kiss, Rodolfo P. Vieira, and et al. 2020. "The Relationship of IL-8 and IL-10 Myokines and Performance in Male Marathon Runners Presenting Exercise-Induced Bronchoconstriction" International Journal of Environmental Research and Public Health 17, no. 8: 2622. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082622