Fear and Practice Modifications among Dentists to Combat Novel Coronavirus Disease (COVID-19) Outbreak

 ,
,  ,
,  ,
, 
 and
and 
Abstract
:1. Introduction
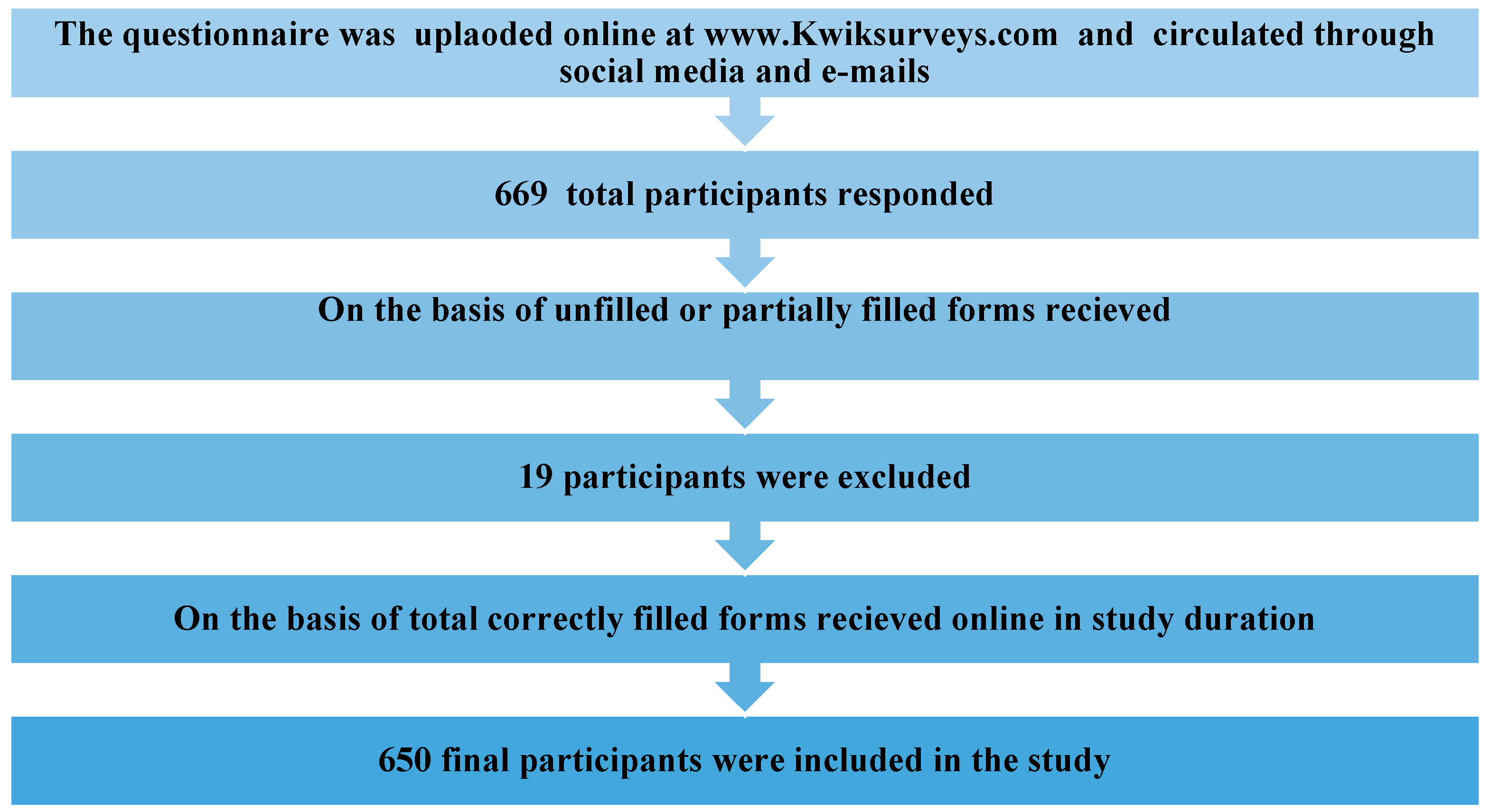
2. Materials and Methods
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gralinski, L.E.; Menachery, V.D. Return of the coronavirus: 2019-nCoV. Viruses 2020, 12, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neher, R.A.; Dyrdak, R.; Druelle, V.; Hodcroft, E.B.; Albert, J. Potential impact of seasonal forcing on a SARS-CoV-2 pandemic. Swiss Med. Wkly. 2020, 150, w20224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khurshid, Z.; Asiri, F.Y.I.; Wadaani, H. Al Human Saliva: Non-Invasive Fluid for Detecting Novel Coronavirus (2019-nCoV). Int. J. Environ. Res. Public Health 2020, 17, 2225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zu, Z.Y.; Jiang, M.D.; Xu, P.P.; Chen, W.; Ni, Q.Q.; Lu, G.M.; Zhang, L.J. Coronavirus Disease 2019 (COVID-19): A Perspective from China. Radiology 2020, 200490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Liu, Q.; Guo, D. Emerging coronaviruses: Genome structure, replication, and pathogenesis. J. Med. Virol. 2020, 92, 418–423. [Google Scholar] [CrossRef]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission routes of 2019-nCoV and controls in dental practice. Int. J. Oral Sci. 2020, 12, 1–6. [Google Scholar] [CrossRef]
- Backer, J.A.; Klinkenberg, D.; Wallinga, J. Incubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020. Euro Surveill. 2020, 25. [Google Scholar] [CrossRef] [Green Version]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill. 2020, 25, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Liu, Y. Potential interventions for novel coronavirus in China: A systematic review. J. Med. Virol. 2020, 479–490. [Google Scholar] [CrossRef] [Green Version]
- Wu, P.; Hao, X.; Lau, E.H.Y.; Wong, J.Y.; Leung, K.S.M.; Wu, J.T.; Cowling, B.J.; Leung, G.M. Real-time tentative assessment of the epidemiological characteristics of novel coronavirus infections in Wuhan, China, as at 22 January 2020. Euro Surveill. 2020, 25, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Chen, J. Pathogenicity and transmissibility of 2019-nCoV—A quick overview and comparison with other emerging viruses. Microbes Infect. 2020, 22, 69–71. [Google Scholar] [CrossRef] [PubMed]
- Ather, A.; Patel, B.; Ruparel, N.B.; Diogenes, A.; Hargreaves, K.M. Coronavirus Disease 19 (COVID-19): Implications for Clinical Dental Care. J. Endod. 2020. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020. [Google Scholar] [CrossRef] [Green Version]
- Fazel, M.; Hoagwood, K.; Stephan, S.; Ford, T. Mental health interventions in schools in high-income countries. Lancet Psychiatry 2014, 1, 377–387. [Google Scholar] [CrossRef] [Green Version]
- Ng, K.; Poon, B.H.; Kiat Puar, T.H.; Shan Quah, J.L.; Loh, W.J.; Wong, Y.J.; Tan, T.Y.; Raghuram, J. COVID-19 and the Risk to Health Care Workers: A Case Report. Ann. Intern. Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- Lydeard, S. The questionnaire as a research tool. Fam. Pract. 1991, 8, 84–91. [Google Scholar] [CrossRef]
- Tam, C.W.C.; Pang, E.P.F.; Lam, L.C.W.; Chiu, H.F.K. Severe acute respiratory syndrome (SARS) in Hongkong in 2003: Stress and psychological impact among frontline healthcare workers. Psychol. Med. 2004, 34, 1197–1204. [Google Scholar] [CrossRef]
- McAlonan, G.M.; Lee, A.M.; Cheung, V.; Cheung, C.; Tsang, K.W.T.; Sham, P.C.; Chua, S.E.; Wong, J.G.W.S. Immediate and sustained psychological impact of an emerging infectious disease outbreak on health care workers. Can. J. Psychiatry 2007, 52, 241–247. [Google Scholar] [CrossRef] [Green Version]
- Moorthy, V.; Restrepo, A.M.H.; Preziosi, M.P.; Swaminathan, S. Active quarantine measures are the primary means to reduce the fatality rate of COVID-19. Bull. World Health Organ. 2020, 98, 150. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated with Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Ge, Z.; Yang, L.; Xia, J.; Fu, X.; Zhang, Y. Possible aerosol transmission of COVID-19 and special precautions in dentistry. J. Zhejiang Univ. B 2020, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Person, B.; Sy, F.; Holton, K.; Govert, B.; Liang, A.; Garza, B.; Gould, D.; Hickson, M.; McDonald, M.; Meijer, C.; et al. Fear and Stigma: The Epidemic within the SARS Outbreak. Emerg. Infect. Dis. 2004, 10, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Madarati, A.; Abid, S.; Tamimi, F.; Ezzi, A.; Sammani, A.; Shaar, M.; Zafar, M. Dental-Dam for Infection Control and Patient Safety during Clinical Endodontic Treatment: Preferences of Dental Patients. Int. J. Environ. Res. Public Health 2018, 15, 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, H.; Zhou, Y.; Liu, X.; Tan, J. The impact of the COVID-19 epidemic on the utilization of emergency dental services. J. Dent. Sci. 2020. [Google Scholar] [CrossRef] [PubMed]
- van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Marui, V.C.; Souto, M.L.S.; Rovai, E.S.; Romito, G.A.; Chambrone, L.; Pannuti, C.M. Efficacy of preprocedural mouthrinses in the reduction of microorganisms in aerosol: A systematic review. J. Am. Dent. Assoc. 2019, 150, 1015–1026.e1. [Google Scholar] [CrossRef]
- Azimi, M.; Jouybari, L.; Moghadam, S.; Ghaemi, E.; Behnampoor, N.; Sanagoo, A.; Hesam, M. Antimicrobial effects of chlorhexidine, matrica drop mouthwash (chamomile extract), and normal saline on hospitalized patients with endotracheal tubes. Iran. J. Nurs. Midwifery Res. 2016, 21, 458. [Google Scholar] [CrossRef] [Green Version]
- Eggers, M.; Koburger-Janssen, T.; Eickmann, M.; Zorn, J. In Vitro Bactericidal and Virucidal Efficacy of Povidone-Iodine Gargle/Mouthwash against Respiratory and Oral Tract Pathogens. Infect. Dis. Ther. 2018, 7, 249–259. [Google Scholar] [CrossRef] [Green Version]
- Kitamura, T.; Satomura, K.; Kawamura, T.; Yamada, S.; Takashima, K.; Suganuma, N.; Namai, H.; Komura, Y.; Great Cold Investigators-I. Can We Prevent Influenza-like Illnesses by Gargling? Intern. Med. 2007, 46, 1623–1624. [Google Scholar] [CrossRef] [Green Version]
- Wood, A.; Payne, D. The action of three antiseptics/disinfectants against enveloped and non-enveloped viruses. J. Hosp. Infect. 1998, 38, 283–295. [Google Scholar] [CrossRef]
- Fung, I.C.-H.; Cairncross, S. Effectiveness of handwashing in preventing SARS: A review. Trop. Med. Int. Health 2006, 11, 1749–1758. [Google Scholar] [CrossRef] [PubMed]
- Jefferson, T.; Foxlee, R.; Del Mar, C.; Dooley, L.; Ferroni, E.; Hewak, B.; Prabhala, A.; Nair, S.; Rivetti, A. Interventions for the interruption or reduction of the spread of respiratory viruses. Cochrane Database Syst. Rev. 2007. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographics | Number (%) | |
|---|---|---|
| Gender | Male | 160 (25) |
| Female | 490 (75) | |
| Age | 20 to 30 | 350 (54) |
| 31 to 40 | 254 (39) | |
| 41 to 50 | 37 (5) | |
| 51 to 60 | 8 (1.85) | |
| Above 60 | 1 (0.15) | |
| Designation | General Dental Practitioner | 511 (78) |
| Specialist | 97 (14) | |
| Consultant | 42 (8) | |
| Qualification | Graduates | 511 (78) |
| Postgraduates | 139 (22) | |
| Workplace | Hospital | 495 (76) |
| Clinic | 155 (24) | |
| Work Setting | Private | 482 (74) |
| Semiprivate | 37 (6) | |
| Government | 131 (20) |
| Yes n (%) | No n (%) | Unaware n (%) | |
|---|---|---|---|
| Are You Afraid of Getting Infected with COVID-19 from a Patient and Co-Worker? | 566 (87) | 66 (10) | 18 (3) |
| Are You Anxious When Providing Treatment to a Patient who is Coughing or Suspected of being Infected with COVID-19? | 585 (90) | 48 (7) | 17 (3) |
| Do You want to Close Your Dental Practice until the Number of COVID-19 Cases Starts Declining? | 431 (66) | 153 (23) | 66 (11) |
| Do You Feel Nervous when Talking to Patients in Close Vicinity? | 467 (72) | 160 (24) | 23 (4) |
| Do You have Fear that You Could Carry the Infection from Your Dental Practice back to Your Family? | 600 (92) | 40 (6) | 10 (2) |
| Are You Afraid of Getting Quarantined if get Infected | 505 (77) | 121 (19) | 24 (4) |
| Are You Anxious about the Cost of Treatment if You Get Infected? | 476 (73) | 141 (22) | 33 (5) |
| Do You feel Afraid when you Hear that People are Dying Because of COVID-19? | 547 (85) | 87 (12) | 16 (3) |
| Yes n (%) | No n (%) | Don’t Know n (%) | |
|---|---|---|---|
| Are You Aware of the Mode of Transmission of COVID-19? | 631 (97) | 15 (2) | 4 (1) |
| Are You Updated with the Current CDC or WHO Guidelines for Cross-Infection Control regarding COVID-19? | 588 (90) | 54 (8) | 8 (2) |
| Are You currently Asking every Patient’s Travel History before Performing Dental Treatment? | 532 (82) | 108 (16) | 10 (2) |
| Are You currently Taking every Patient’s Body Temperature before Performing Dental Treatment? | 530 (81) | 115 (17) | 5 (2) |
| Are You Deferring Dental Treatment of Patients Showing Suspicious Symptoms? | 512 (78) | 111 (17) | 27 (5) |
| Do You Think Surgical Mask is enough to Prevent Cross-Infection of COVID 19 | 72 (11) | 553 (85) | 25 (4) |
| Do You Think N-90 Mask should be Routinely Worn in Dental Practice due to the Current Outbreak? | 548 (84) | 75 (11) | 27 (5) |
| Have You Ever Worn an N-90 Mask while Treating a Patient in Your Dental Practice? | 58 (9) | 586 (90) | 6 (1) |
| Do You Routinely Follow Universal Precautions of Infection Control for Every Patient? | 583 (89) | 58 (9) | 9 (2) |
| Do You Use Rubber Dam Isolation for Every Patient? | 93 (14) | 550 (84) | 7 (2) |
| Do You Use High-Volume Suction in Your Practice for Every Patient? | 499 (76) | 143 (22) | 8 (2) |
| Do You Ask Every Patient to Rinse His/Her Mouth with Anti-Bacterial Mouthwash before Treatment? | 160 (24) | 484 (74) | 6 (2) |
| Do You Wash Hands with Soap and Water/Use Sanitizer Before and After Treatment of Every Patient? | 611 (94) | 37 (5) | 2 (1) |
| Are You Aware of which Authority to Contact if You Come Across a Patient with Suspected COVID-19 Infection? | 519 (80) | 114 (17) | 17 (3) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, M.A.; Jouhar, R.; Ahmed, N.; Adnan, S.; Aftab, M.; Zafar, M.S.; Khurshid, Z. Fear and Practice Modifications among Dentists to Combat Novel Coronavirus Disease (COVID-19) Outbreak. Int. J. Environ. Res. Public Health 2020, 17, 2821. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082821
Ahmed MA, Jouhar R, Ahmed N, Adnan S, Aftab M, Zafar MS, Khurshid Z. Fear and Practice Modifications among Dentists to Combat Novel Coronavirus Disease (COVID-19) Outbreak. International Journal of Environmental Research and Public Health. 2020; 17(8):2821. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082821
Chicago/Turabian StyleAhmed, Muhammad Adeel, Rizwan Jouhar, Naseer Ahmed, Samira Adnan, Marziya Aftab, Muhammad Sohail Zafar, and Zohaib Khurshid. 2020. "Fear and Practice Modifications among Dentists to Combat Novel Coronavirus Disease (COVID-19) Outbreak" International Journal of Environmental Research and Public Health 17, no. 8: 2821. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082821