Mindfulness versus Physical Exercise: Effects of Two Recovery Strategies on Mental Health, Stress and Immunoglobulin A during Lunch Breaks. A Randomized Controlled Trial

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
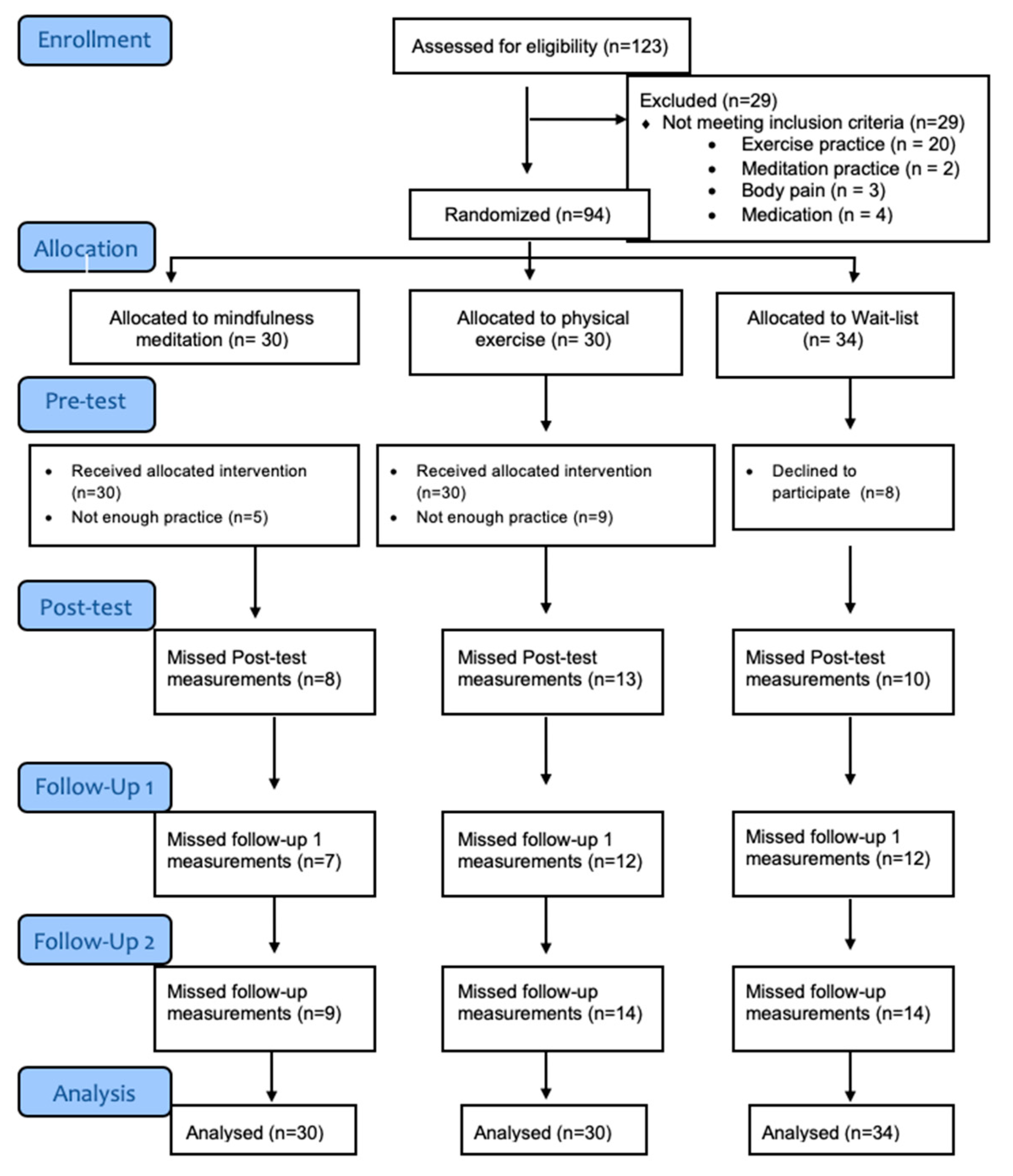
2.1. Participants
2.2. Procedure
2.3. Instruments
2.3.1. Perceived Stress Questionnaire (PSQ)
2.3.2. General Health Questionnaire (GHQ-12)
2.3.3. Salivary Immunoglobulin A (sIgA)
2.4. Data Analyses
3. Results
3.1. Main Effects
3.2. Simple Effects
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Stansfeld, S.; Candy, B. Psychosocial work environment and mental health—A meta analytic review. Scand. J. Work Environ. Health 2006, 32, 443–462. [Google Scholar] [CrossRef] [PubMed]
- Schneiderman, N.; Ironson, G.; Siegel, S.D. Stress and health: Psychological, behavioral, and biological determinants. Annu. Rev. Clin. Psychol. 2005, 1, 607–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassmén, P.; Koivula, N.; Uutela, A. Physical exercise and psychological well-being: A population study in Finland. Am. J. Prev. Med. 2000, 30, 17–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leone, S.S.; Wessely, S.; Huibers, M.J.H.; Knottnerus, J.A.; Kant, I. Two sides of the same coin? On the history and phenomenology of chronic fatigue and burnout. Psychol. Health 2011, 26, 449–464. [Google Scholar] [CrossRef]
- Netterstrøm, B.; Conrad, N.; Bech, P.; Fink, P.; Olsen, O.; Rugulies, R. The relation between work-related psychosocial factors and the development of depression. Epidemiol. Rev. 2008, 30, 118–132. [Google Scholar] [CrossRef] [Green Version]
- McEwen, B.S.; Sapolsky, R.M. Stress and cognitive function. Curr. Opin. Neurobiol. 1995, 5, 205–216. [Google Scholar] [CrossRef]
- Wolever, R.Q.; Bobinet, K.J.; McCabe, K.; Mackenzie, E.R.; Fekete, E.; Kusnick, C.A. Effective and viable mind-body stress reduction in the workplace: A randomized controlled trial. J. Occup. Health Psychol. 2012, 17, 246–258. [Google Scholar] [CrossRef]
- McEwen, B. Interacting mediators of allostasis and allostatic load: Towards an understanding of resilience in aging. Metabolism 2003, 52, 10–16. [Google Scholar] [CrossRef]
- Phillips, A.C.; Carroll, D.; Evans, P.; Bosch, J.A.; Clow, A.; Hucklebridge, F.; Der, G. Stressful life events are associated with low secretion rates of immunoglobulin A in saliva in the middle aged and elderly. Brain Behav. Immunity 2006, 20, 191–197. [Google Scholar] [CrossRef] [Green Version]
- Segerstrom, S.C.; Miller, G.E. Psychological stress and the human immune system: A meta-analytic study of 30 years of inquiry. Psychol. Bull. 2004, 130, 601–630. [Google Scholar] [CrossRef] [Green Version]
- Bellosta-Batalla, M.; Ruiz-Robledillo, N.; Sariñana-González, P.; Capella-Solano, T.; Vitoria-Estruch, S.; Hidalgo-Moreno, G. Increased salivary IgA response as an indicator of immunocompetence after a mindfulness and self-compassion-based intervention. Mindfulness 2018, 9, 905–913. [Google Scholar] [CrossRef]
- Bosch, J.A.; Ring, C.; De Geus, E.J.; Veerman, E.C.; Amerongen, A.V. Stress and secretory immunity. Int. Rev. Neurobiol. 2002, 52, 213–253. [Google Scholar] [PubMed]
- Romero-Martínez, A.; Lila, M.; Conchell, R.; González-Bono, E.; Moya-Albiol, L. Immunoglobulin A response to acute stress in intimate partner violence perpetrators: The role of anger expression-out and testosterone. Biol. Psychol. 2014, 96, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Romero-Martínez, A.; Lila, M.; Vitoria-Estruch, S.; Moya-Albiol, L. High immunoglobulin A levels mediate the association between high anger expression and low somatic symptoms in intimate partner violence perpetrators. J. Interpers. Violence 2016, 31, 732–742. [Google Scholar] [CrossRef] [PubMed]
- Black, D.S.; Slavich, G.M. Mindfulness meditation and the immune system: A systematic review of randomized controlled trials. Ann. N. Y. Acad. Sci. 2017, 1373, 13–24. [Google Scholar] [CrossRef]
- Hayney, M.S.; Coe, C.L.; Muller, D. Age and psychological influences on immune responses to trivalent inactivated influenza vaccine in the meditation or exercise for preventing acute respiratory infection (MEPARI) trial. Hum. Vaccin. Immunother. 2014, 10, 83–91. [Google Scholar] [CrossRef] [Green Version]
- Davidson, R.J.; Kabat-Zinn, J.; Schumacher, J. Alterations in brain and immune function produced by mindfulness meditation. Psychosom. Med. 2003, 65, 564–570. [Google Scholar] [CrossRef]
- Green, M.L.; Green, R.G.; Santoro, W. Daily relaxation modifies serum and salivary immunoglobulins and psychophysiologic symptom severity. Biofeed-Back Self-Regul. 1988, 13, 187–199. [Google Scholar] [CrossRef]
- Rein, G.; Atkinson, M.; McCraty, R. The physiological and psychological effects of compassion and anger. J. Adv. Med. 1995, 8, 87–105. [Google Scholar]
- Paszynska, E.; Dmitrzak-Weglarz, M.; Tyszkiewicz-Nwafor, M.; Slopien, A. Salivary alpha-amylase, secretory IgA and free cortisol as neurobiological components of the stress response in the acute phase of anorexia nervosa. World Psychiatry 2016, 17, 266–273. [Google Scholar] [CrossRef]
- De Andrés-García, S.; Moya-Albiol, L.; González-Bono, E. Salivary cortisol and immunoglobulin A: Responses to stress as predictors of health complaints reported by caregivers of offspring with autistic spectrum disorder. Horm. Behav. 2012, 62, 464–474. [Google Scholar] [PubMed]
- Dhabhar, F.S. Effects of stress on immune function: The good, the bad, and the beautiful. Immunol. Res. 2014, 58, 193–210. [Google Scholar] [PubMed]
- Heikkilä, K.; Fransson, E.I.; Nyberg, S.T.; Zins, M.; Westerlund, H.; Westerholm, P. Job strain and health-related lifestyle: Findings from an individual-participant meta-analysis of 118,000 working adults. Am. J. Public Health 2013, 103, 2090–2097. [Google Scholar] [PubMed]
- Ratnawat, R.G.; Jha, P.C. Impact of Job Related Stress on Employee Performance: A review and research agenda. IOSR-JBM 2014, 16, 2319–7668. [Google Scholar] [CrossRef]
- International Labour Organization. Workplace Stress. A Collective Challenge; ILO Cataloguing in Publication Data: Turin, Italy, 2016. [Google Scholar]
- European Agency for Safety and health at Work. Calculating the Cost of Work-Related Stress and Psychosocial Risks; Publications Office of the European Union: Luxembourg, 2014; p. 7.
- De Bruin, E.I.; Van der Zwan, J.E.; Bogels, S.M. A RCT comparing daily mindfulness meditations, biofeedback exercises, and daily physical exercise on attention control, executive functioning, mindful awareness, self-com- passion, and worrying in stressed young adults. Mindfulness 2016, 7, 1182–1192. [Google Scholar] [CrossRef] [Green Version]
- Shanafelt, T.D.; Hasan, O.; Dyrbye, L.N.; Sinsky, C.; Satele, D.; Sloan, J. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014. Clin. Proc. 2015, 90, 1600–1613. [Google Scholar]
- Matrix Insight. Economic Analysis of Workplace Mental Health Promotion and Mental Disorder Prevention Programmes and of Their Potential Contribution to EU Health, Social and Economic Policy Objectives; Final Report; Matrix Insight. Executive Agency for Health and Consumers: Rochester, NY, USA, 2012.
- Awa, W.L.; Plaumann, M.; Walter, U. Burnout prevention: A review of intervention programs. Patient Educ. Couns. 2010, 78, 184–190. [Google Scholar] [CrossRef]
- Richardson, K.; Rothstein, H. Effects of occupational stress management intervention programs: A meta-analysis. J. Occup. Health Psychol. 2008, 13, 69–93. [Google Scholar]
- LaMontagne, A.D.; Keegel, T.; Louie, A.M.; Ostry, A.; Landsbergis, P.A. A systematic review of the job-stress intervention evaluation literature, 1990–2005. Int. J. Occup. Environ. Psychol. Health 2007, 13, 268–280. [Google Scholar]
- Kröll, C.; Doebler, P.; Nüesch, S. Meta-analytic evidence of the effectiveness of stress management at work. EJWOP 2017, 26, 677–693. [Google Scholar]
- Fritz, C.; Sonnentag, S. Recovery, health, and job performance: Effects of weekend experiences. J. Occup. Health Psychol. 2005, 10, 187–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geurts, S.A.E.; Sonnentag, S. Recovery as an explanatory mechanism in the relation between acute stress reactions and chronic health impairment. Scand. J. Work Environ. Health 2006, 32, 482–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zijlstra, F.R.H.; Sonnentag, S. After work is done: Psychological perspectives on recovery from work. EJWOP 2006, 15, 129–138. [Google Scholar] [CrossRef]
- Meijman, T.F.; Mulder, G. Psychological aspects of workload. In Handbook of Work and Organizational Psychology: Volume 2. Work Psychology; Drenth, P.J.D., Thierry, H., Eds.; Psychology Press: Hove, UK, 1998; pp. 5–33. [Google Scholar]
- Fritz, C.; Sonnentag, S. Recovery, well-being, and performance related outcomes: The role of workload and vacation experiences. J. Appl. Psychol. 2006, 91, 936–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veldhoven, M.J.P.M.; Sluiter, J.K. Recovery opportunities and health at work. Gedrag Organ. 2010, 23, 275–295. [Google Scholar]
- Alcover, C.M. Recuperación del trabajo, bienestar psicosocial y salud ocupacional. In Psicología del Trabajo. Conceptos Claves y Temas Emergentes; Sanz y Torres: Madrid, Spain, 2016. [Google Scholar]
- Trougakos, J.P.; Beal, D.J.; Green, S.G.; Weiss, H.M. Making the break count: An episodic examination of recovery, activities, emotional experiences, and positive affective displays. Acad. Manag. J. 2008, 51, 131–146. [Google Scholar] [CrossRef]
- Krajewski, J.; Wieland, R.; Sauerland, M. Regulating strain states by using the recovery potential of lunch breaks. J. Occup. Health Psychol. 2010, 15, 131–139. [Google Scholar] [CrossRef] [Green Version]
- Trougakos, J.P.; Hideg, I.; Cheng, B.; Beal, H.; Daniel, J. Lunch breaks unpacked: The role of autonomy as a moderator of recovery during lunch. Acad. Manag. J. 2014, 57, 405–421. [Google Scholar] [CrossRef] [Green Version]
- Coffeng, J.K.; Van Sluijs, E.M.; Hendriksen, I.; Van Mechelen, J.M.; Boot, W. Physical Activity and Relaxation during and after Work Are Independently Associated with the Need for Recovery. J. Phys. Act. Health 2015, 12, 109–115. [Google Scholar] [CrossRef]
- Sianoja, M.; Kinnunen, U.; de Bloom, J.; Korpela, K.; Geurts, S. Recovery during Lunch Breaks: Testing Long-Term Relations with Energy Levels at Work. Scand. J. Work Environ. Health 2016, 1, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Fritz, C.; Ellis, A.M.; Demsky, C.A.; Lin, B.C.; Guros, F. Embracing work breaks: Recovering from work stress. Organ. Dyn. 2013, 42, 274–280. [Google Scholar] [CrossRef]
- Jazaieri, H.; Goldin, P.R.; Werner, K.; Ziv, M.; Gross, J.J. A randomized trial of MBSR versus aerobic exercise for social anxiety disorder. J. Clin. Psychol. 2012, 68, 715–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rusch, N.; Evans-Lacko, S.E.; Henderson, C.; Flach, C.; Thornicroft, G. Knowledge and attitudes as predictors of intentions to seek help for and disclose a mental illness. Psychiatr. Serv. 2011, 62, 675–678. [Google Scholar] [CrossRef] [PubMed]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be smart, exercise your heart: Exercise effects on brain and cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Eisendrath, S.J.; Gillung, E.; Delucchi, K.L. A randomized controlled trial of mindfulness- based cognitive therapy for treatment-resistant depression. Psychother. Psychosom. 2016, 85, 99–110. [Google Scholar] [CrossRef] [Green Version]
- Lavie, C.J.; Menezes, A.R.; De Schutter, A. Impact of cardiac rehabilitation and exercise training on psychological risk factors and subsequent prognosis in patients with cardiovascular disease. Can. J. Cardiol. 2016, 32, S365–S373. [Google Scholar] [CrossRef] [Green Version]
- Rebar, A.L.; Stanton, R.; Geard, D. A meta-meta-analysis of the effect of physical activity on depression and anxiety in non-clinical adult populations. Health Psychol. Rev. 2015, 9, 366–378. [Google Scholar] [CrossRef]
- Dubbert, P.M. Exercise in behavioral medicine. J. Consult. Clin. Psychol. 2015, 60, 613–618. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: Theoretical considerations and preliminary results. Gen. Hosp. Psychiatry 1982, 4, 33–47. [Google Scholar] [CrossRef]
- Martin, J.E.; Dubbert, P.M. Exercise applications and promotion in behavioral medicine: Current status and future directions. J. Consult. Clin. Psychol. 1982, 50, 1004–1017. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body Andmind to Face Stress, Pain, and Illness; Delacorte Press: New York, NY, USA, 1990. [Google Scholar]
- Hilton, L.; Hempel, S.; Ewing, B.A.; Apaydin, E.; Xenakis, L.; Newberry, S. Mindfulness Meditation for Chronic Pain: Systematic Review and Meta-analysis. Ann. Behav. Med. 2017, 51, 199–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacKenzie, M.B.; Abbott, K.A.; Kocovski, N.L. Mindfulness-based cognitive therapy in patients with depression: Current perspectives. Neuropsychiatr. Dis. Treat. 2018, 14, 1599–1605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoge, E.A.; Bui, E.; Palitz, S.A.; Schwarz, N.R.; Owens, M.E.; Johnston, J.M. The effect of mindfulness meditation training on biological acute stress responses in generalized anxiety disorder. Psychiatry Res. 2018, 262, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Singh, S.; Sibinga, E.M.; Gould, N.F.; Rowland-Seymour, A.; Sharma, R. Meditation programs for psychological stress and well-being: A systematic review and meta-analysis. JAMA Intern. Med. 2014, 174, 357–368. [Google Scholar] [CrossRef] [Green Version]
- Rash, J.A.; Kavanagh, V.A.J.; Garland, S.N. A Meta-Analysis of Mindfulness-Based Therapies for Insomnia and Sleep Disturbance. Sleep Med. Clin. 2019, 14, 209–233. [Google Scholar] [CrossRef]
- Sonne, J.W.H.; Gash, D.M. Psychopathy to Altruism: Neurobiology of the Selfish–Selfless Spectrum. Front. Psychol. 2018, 9, 575. [Google Scholar] [CrossRef] [Green Version]
- Janssen, M.; Heerkens, Y.; Kuijer, W.; van der Heijden, B.; Engels, J. Effects of Mindfulness- Based Stress Reduction on employees’ mental health: A systematic review. PLoS ONE 2018, 13, e0191332. [Google Scholar] [CrossRef]
- Bouchard, C.; Shephard, R.J.; Stephens, T. Exercise, Fitness, and Health. Consensus of Current Knowledge; Human Kinetics Publishers: Champaign, IL, USA, 1990. [Google Scholar]
- Conn, V.S. Anxiety outcomes after physical activity interventions: Meta-analysis findings. Nurs. Res. 2010, 59, 224–231. [Google Scholar] [CrossRef] [Green Version]
- Conn, V.S. Depressive symptom outcomes of physical activity interventions: Meta-analysis findings. Ann. Behav. Med. 2010, 39, 128–138. [Google Scholar] [CrossRef] [Green Version]
- McGale, N.; McArdle, S.; Gaffney, P. Exploring the effectiveness of an integrated exercise/CBT intervention for young men’s mental health. Br. J. Health Psychol. 2011, 16, 457–471. [Google Scholar] [CrossRef]
- Callaghan, P. Exercise: A neglected intervention in mental health care? J. Psychiatr. Ment. Health Nurs. 2004, 11, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Van der Zwan, J.E.; De Vente, W.; Huizink, A.C. Physical activity, mindfulness meditation, or heart rate variability biofeedback for stress reduction: A randomized controlled trial. Appl. Psychophysiol. Biofeedback 2015, 40, 257–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farias, M.; Wikholm, C. Has the science of mindfulness losts its mind? Br. J. Psychiatr. 2016, 40, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, S.B.; Tucker, R.P.; Greene, P.A.; Simpson, T.L.; Hoyt, W.T.; Kearney, D.J.; Davidson, R.J. What can we learn from randomized clinical trials about the construct validity of self-report measures of mindfulness? A meta-analysis. Mindfulness 2019, 10, 775–785. [Google Scholar] [CrossRef] [Green Version]
- Barrett, B.; Hayney, M.S.; Muller, D.; Rakel, D.; Brown, R.; Zgierska, A.E. Meditation or exercise for preventing acute respiratory infection (MEPARI-2): A randomized controlled trial. PLoS ONE 2018, 13, e0197778. [Google Scholar] [CrossRef]
- MacDonald, L.; Minahan, C. Mindfulness training attenuates the increase in salivary cortisol concentration associated with competition in highly trained wheelchair-basketball players. J. Sports Sci. 2018, 36, 378–383. [Google Scholar] [CrossRef]
- Leicht, C.; Goosey-Tolfrey, V.; Bishop, N. Exercise intensity and its impact on relationships between salivary immunoglobulin A, saliva flow rate and plasma cortisol concentration. Eur. J. App. Physiol. 2018, 118, 1179–1187. [Google Scholar] [CrossRef] [Green Version]
- Levenstein, S.; Prantera, V.; Varvo, V.; Scribano, M.L.; Berto, E.; Luzi, C. Development of the Perceived Stress Questionnaire: A new tool for psychosomatic research. J. Psychosom. Res. 1993, 37, 19–32. [Google Scholar] [CrossRef]
- Cohen, S.; Janicki-Deverts, D. Who’s stressed? Distributions of psychological stress in the united states in probability samples from 1983, 2006, and 2009. J. Appl. Soc. Psychol. 2012, 42, 1320–1334. [Google Scholar] [CrossRef]
- Goldberg, D.P.; Williams, P. A user’s Guide to the General Health Questionnaire; NFER-Nelson: Windsor, UK, 1988. [Google Scholar]
- Sanz-Carrillo, C.; García-Campayo, J.; Rubio, A.; Santed, M.A.; Montoro, M. Validation of the Spanish version of the Perceived Stress Questionnaire. J. Psychosom. Res. 2002, 52, 167–172. [Google Scholar] [CrossRef]
- Rocha, K.; Pérez, K.; Rodríguez-Sanz, M.; Borrell, C.; Obiols, J.E. Propiedades psicométricas y valores normativos del General Health Questionnaire (GHQ-12) en la población general española. Int. J. Clin. Health Psychol. 2011, 11, 125–139. [Google Scholar]
- Ruiz, M.; Pardo, A.; San Martín, R. Modelos de ecuaciones estructurales. Papeles del Psicólogo 2010, 31, 151–157. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Holm, S. A simple sequentially rejective multiple test procedure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- Demarzo, M.M.; Montero-Marin, J.; Stein, P.K. Mindfulness may both moderate and mediate the effect of physical fitness on cardiovascular responses to stress: A speculative hypothesis. Front. Physiol. 2014, 5, 105–120. [Google Scholar] [CrossRef] [Green Version]
- Goldin, P.; Ziv, M.; Jazaieri, H. Randomized controlled trial of mindfulness-based stress reduction versus aerobic exercise: Effects on the self-referential brain network in social anxiety disorder. Front. Hum. Neurosci. 2014, 6, 295. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, E.; Topitzes, J.; Brown, R.L.; Barrett, B. Mediational pathways of meditation and exercise on mental health and perceived stress: A randomized controlled trial. J. Health Psichol. 2018, in press. [Google Scholar] [CrossRef]
- Baer, R.A.; Carmody, J.; Hunsinger, M. Weekly change in mindfulness and perceived stress in a mindfulness-based stress reduction program. J. Clin. Psychol. 2012, 68, 755–765. [Google Scholar] [CrossRef]
- Barrett, B.; Hayney, M.S.; Muller, D. Meditation or exercise for preventing acute respiratory infection: A randomized controlled trial. Ann. Fam. Med. 2012, 10, 337–346. [Google Scholar] [CrossRef]
- Tsafou, K.E.; Lacroix, J.P.; Van, E.R. The relation of trait and state mindfulness with satisfaction and physical activity: A cross-sectional study in 305 Dutch participants. J. Health Psychol. 2017, 22, 1221–1232. [Google Scholar] [CrossRef]
- Song, Z.; Baicker, K. Effect of a Workplace Wellness Program on Employee Health and Economic Outcomes: A Randomized Clinical Trial. J. Am. Med. Assoc. 2019, 15, 1491–1501. [Google Scholar] [CrossRef]
- Zgierska, A.; Obasi, C.N.; Brown, R. Randomized controlled trial of mindfulness meditation and exercise for the prevention of acute respiratory infection: Possible mechanisms of action. J. Evid. Based Complementary Altern. Med. 2013, 2013, 952716. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, B.T.; Stanton, W.; Lord, R.; Petocz, P.; Pepping, G.-J. Factors Affecting Measurement of Salivary Cortisol and Secretory Immunoglobulin a in Field Studies of Athletes. Front. Endocrinol. 2017, 8, 168–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witek-Janusek, L.; Albuquerque, K.; Chroniak, K.R.; Chroniak, C.; Durazo-Arvizu, R.; Mathews, H.L. Effect of mindfulness-based stress reduction on immune function, quality of life and coping in women newly diagnosed with early stage breast cancer. Brain Behav. Immun. 2008, 22, 969–981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Bloom, J.; Sianoja, M.; Korpela, K.; Tuomisto, M.; Lilja, A.; Geurts, S.; Kinnunen, U. Effects of park walks and relaxation exercises during lunch breaks on recovery from job stress: Two randomized controlled trials. J. Environ. Psychol. 2017, 51, 14–30. [Google Scholar] [CrossRef] [Green Version]
- Edwards, M.; Loprinzi, P.D. Comparative effects of meditation and exercise on physical and psychosocial health outcomes: A review of randomized controlled trials. Postgrad. Med. 2018, 130, 222–228. [Google Scholar] [CrossRef]
- Asztalos, M.; Wijndaele, K.; De Bourdeaudhuij, I.; Philippaerts, R.; Matton, L.; Duvigneaud, N. Sport participation and stress among women and men. Psychol. Sport Exerc. 2012, 13, 466–483. [Google Scholar] [CrossRef]
- Kawachi, I.; Berkman, L.F. Social ties and mental health. J. Urban Health 2001, 78, 458–467. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | MM (n = 30) | PE (n = 30) | CG (n = 34) | Total (N = 94) | |
|---|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | M (SD) | F/p 1 | |
| Age | 47.40 (3.84) | 47.77 (5.16) | 45.44 (8.66) | 46.81 (6.37) | F = 1.26, p = 0.29 |
| PSQ 2 | |||||
| Harassment-SA | 0.48 (0.20) | 0.47 (0.15) | 0.45 (0.15) | 0.47 (0.17) | F = 0.23, p = 0.80 |
| Overload | 0.76 (0.19) | 0.76 (0.13) | 0.73 (0.15) | 0.75 (0.16) | F = 0.63, p = 0.54 |
| Irritab.-Fatigue | 0.65 (0.21) | 0.62 (0.14) | 0.60 (0.14) | 0.62 (0.16) | F = 0.71, p = 0.49 |
| Energy-joy | 0.55 (0.19) | 0.55 (0.19) | 0.56 (0.15) | 0.56 (0.17) | F = 0.03, p = 0.97 |
| Fear-anxiety | 0.53 (0.26) | 0.47 (0.18) | 0.47 (0.23) | 0.49 (.22) | F = 0.71, p = 0.49 |
| Self-realisation | 0.57 (0.23) | 0.56 (0.15) | 0.53 (0.20) | 0.55 (0.19) | F = 0.44, p = 0.64 |
| Total | 0.63 (0.18) | 0.61 (0.11) | 0.59 (0.12) | 0.61 (0.14) | F = 0.51, p = 0.60 |
| GHQ 3 | |||||
| Coping | 6.96 (3.31) | 6.50 (1.70) | 7.40 (2.86) | 6.95 (2.69) | F = 0.84, p = 0.44 |
| Self-esteem | 5.07 (3.91) | 3.63 (2.58) | 3.67 (2.93) | 4.10 (3.20) | F = 1.92, p = 0.15 |
| Stress | 5.11 (2.04) | 4.77 (1.36) | 4.43 (1.77) | 4.76 (1.74) | F = 1.09, p = 0.34 |
| Total | 17.14 (7.20) | 14.90 (4.71) | 15.50 (6.32) | 15.82 (6.14) | F = 1.03, p = 0.36 |
| IgA | 2.66 (1.41) | 3.05 (1.09) | 2.61 (1.07) | 2.76 (1.21) | F = 0.84, p = 0.44 |
| n (%) | n (%) | n (%) | N (%) | X2/p 1 | |
| Sex | X2 = 2.01, p= 0.36 | ||||
| Woman | 23 (76.7%) | 18 (60.0%) | 22 (64.7%) | 63 (67.0%) | |
| Man | 7 (23.3%) | 12 (40.0%) | 12 (35.3%) | 31 (33.0%) | |
| Marital status | X2 = 10.56, p = 0.23 | ||||
| Married | 17 (56.7% | 25 (83.3%) | 17 (50.0%) | 59 (62.8%) | |
| Stable partner | 7 (23.3%) | 2 (6.7%) | 9 (26.5%) | 18 (19.1%) | |
| Single | 3 (10.0%) | 1 (3.3%) | 2 (5.9%) | ||
| Separated/Divorced | 3 (10.0% | 2 (6.7%) | 5 (14.7%) | 10 (10.6% | |
| Widower | 0 (10.0%) | 0 (10.0%) | 1 (2.9%) | 1 (1.1%) | |
| Level of education | X2 = 6.40, p = 0.38 | ||||
| Second. education | 1 (3.3%) | 2 (6.7%) | 2 (5.9%) | 5 (5.3%) | |
| Bachelor’s degree | 19 (63.3%) | 12 (40.0%) | 13 (38.2%) | 44 (46.8%) | |
| Master’s degree | 10 (33.3%) | 53.3 (17.0%) | 18 (52.9%) | 44 (46.8%) | |
| Doctoral degree | 0 (0.0%) | 0 (0.0%) | 1 (2.9%) | 1 (1.1%) | |
| Variable | Interaction | Time | Group | α | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| F | p | ω 2 | F | p | ω 2 | F | p | ω 2 | ||
| GHQ | ||||||||||
| Coping | 1.37 | 0.23 | 0.02 | 11.55 | <0.01 * | 0.25 ## | 2.94 | 0.06 | 0.04 | 0.82 |
| Self-esteem | 1.21 | 0.30 | 0.01 | 9.25 | <0.01 * | 0.21 ## | 1.28 | 0.28 | 0.01 | 0.86 |
| Stress | 1.49 | 0.18 | 0.03 | 9.16 | <0.01 * | 0.21 ## | 0.70 | 0.50 | <0.01 | 0.42 |
| Total | 1.74 | 0.11 | 0.04 | 16.67 | <0.01 * | 0.33 ## | 0.54 | 0.58 | <0.01 | 0.82 |
| PSQ | ||||||||||
| Harassment-SA | 3.63 | <0.01 * | 0.14 # | 6.96 | <0.01 * | 0.22 ## | 1.79 | 0.17 | 0.02 | 0.72 |
| Overload | 2.34 | <0.01 * | 0.08 # | 8.54 | <0.01 * | 0.19 ## | 0.88 | 0.42 | <0.01 | 0.69 |
| Irritab.-fatigue | 2.25 | 0.04 * | 0.07 # | 8.66 | <0.01 * | 0.20 ## | 1.92 | 0.15 | 0.02 | 0.80 |
| Energy-joy | 0.69 | 0.66 | <0.01 | 1.59 | 0.19 | 0.02 | 1.24 | 0.29 | 0.01 | 0.59 |
| Fear-anxiety | 1.42 | 0.21 | 0.03 | 6.85 | <0.01 * | 0.16 ## | 0.28 | 0.76 | <0.01 | 0.18 |
| Self-realisation | 1.25 | 0.28 | 0.01 | 5.17 | <0.01 * | 0.12 # | 1.57 | 0.21 | 0.01 | 0.47 |
| Total | 2.62 | 0.02 * | 0.09 # | 9.13 | <0.01 * | 0.21 ## | 2.06 | 0.13 | 0.02 | 0.89 |
| IgA | 0.77 | 0.55 | <0.01 | 0.88 | 0.42 | <0.01 | 0.98 | 0.38 | <0.01 | |
| Variable | Groups | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MM 1 vs. PE 2 | MM vs. CG 3 | PE vs. CG | |||||||||||||
| t | p | d | I.C.95% | t | p | d | I.C. 95% | t | p | d | I.C. 95% | ||||
| Haras. | |||||||||||||||
| Pre-Post | −2.59 | 0.01 * | 0.68 | [−0.23, −0.03] | 1.55 | 0.12 | 0.40 | [−0.02, 0.16] | 4.15 | <0.01 * | 1.05 | [0.10, 0.30] | |||
| Pre-Fup 1 | 0.43 | 0.67 | 0.11 | [−0.10, 0.16] | 1.62 | 0.11 | 0.41 | [−0.02, 0.23] | 1.10 | 0.27 | 0.28 | [−0.06, 0.21] | |||
| Pre-Fup 2 | −0.35 | 0.72 | 0.09 | [−0.16, 0.11] | 0.82 | 0.41 | 0.21 | [−0.08, 0.19] | 1.15 | 0.25 | 0.29 | [−0.06, 0.21] | |||
| Overl. | |||||||||||||||
| Pre-Post | −0.77 | 0.44 | 0.20 | [−0.14, 0.06] | 2.36 | 0.02 * | 0.60 | [0.02, 0.21] | 3.07 | <0.01 * | 0.78 | [0.05, 0.25] | |||
| Pre-Fup 1 | −0.87 | 0.38 | 0.23 | [−0.19, 0.07] | 1.32 | 0.19 | 0.33 | [−0.04, 0.21] | 2.07 | 0.04 * | 0.52 | [0.01, 0.28] | |||
| Pre-Fup 2 | 0.88 | 0.38 | 0.23 | [−0.07, 0.19] | 1.34 | 0.18 | 0.34 | [−0.04, 0.21] | 0.42 | 0.67 | 0.11 | [-0.10, 0.16] | |||
| Irritab. | |||||||||||||||
| Pre-Post | −2.06 | 0.04 | 0.54 | [−0.20, −0.01] | 1.12 | 0.26 | 0.28 | [−0.04, 0.15] | 3.20 | <0.01 * | 0.81 | [0.06, 0.26] | |||
| Pre-Fup 1 | −0.21 | 0.83 | 0.05 | [−0.14, 0.12] | 1.58 | 0.11 | 0.40 | [−0.02, 0.23] | 1.68 | 0.09 | 0.43 | [−0.02, 0.25] | |||
| Pre-Fup 2 | 0.50 | 0.61 | 0.13 | [−0.10, 0.17] | 1.87 | 0.06 | 0.47 | [−0.01, 0.26] | 1.32 | 0.19 | 0.33 | [−0.04, 0.22] | |||
| Total | |||||||||||||||
| Pre-Post | −2.26 | 0.02 | 0.59 | [−0.19, −0.01] | 1.44 | 0.15 | 0.36 | [−0.02, 0.14] | 3.72 | <0.01 * | 0.94 | [0.07, 0.25] | |||
| Pre-Fup 1 | −0.38 | 0.71 | 0.10 | [−0.13, 0.09] | 1.39 | 0.17 | 0.35 | [−0.03, 0.19] | 1.66 | 0.10 | 0.42 | [−0.02, 0.22] | |||
| Pre-Fup 2 | 0.31 | 0.76 | 0.08 | [−0.10, 0.14] | 1.47 | 0.14 | 0.37 | [−0.03, 0.20] | 1.13 | 0.26 | 0.29 | [−0.05, 0.18] | |||
| Variable | Group | Comparisons | M Diff 1 | S.E. | p | C.I. 95% | |
|---|---|---|---|---|---|---|---|
| LLCI 2 | ULCI 3 | ||||||
| Total | Mindfulness | Pre-Post-test | 4.64 | 1.24 | 0.00 * | 1.28 | 8.00 |
| Pre-Fup 1 | 5.48 | 1.20 | 0.00 * | 2.23 | 8.73 | ||
| Pre-Fup 2 | 4.74 | 1.48 | 0.01 * | 0.71 | 8.77 | ||
| Physical exercise | Pre-Post-test | 3.05 | 1.35 | 0.16 | −0.62 | 6.71 | |
| Pre-Fup 1 | 3.14 | 1.31 | 0.11 | −0.40 | 6.69 | ||
| Pre-Fup 2 | 0.10 | 1.62 | 0.99 | −4.30 | 4.50 | ||
| Coping | Mindfulness | Pre-Post-test | 3.24 | 0.60 | 0.00 * | 1.61 | 4.87 |
| Pre-Fup 1 | 3.24 | 0.66 | 0.00 * | 1.46 | 5.02 | ||
| Pre-Fup 2 | 3.24 | 0.79 | 0.00 * | 1.09 | 5.39 | ||
| Physical exercise | Pre-Post-test | 1.29 | 0.65 | 0.32 | −0.49 | 3.06 | |
| Pre-Fup 1 | 1.43 | 0.72 | 0.30 | −0.52 | 3.37 | ||
| Pre-Fup 2 | 0.33 | 0.86 | 0.99 | −2.02 | 2.68 | ||
| Pre-Fup 2 | -0.24 | 0.70 | 0.99 | −2.14 | 1.67 | ||
| Self-esteem | Mindfulness | Pre-Post-test | 0.88 | 0.63 | 0.99 | −0.84 | 2.60 |
| Pre-Fup 1 | 1.60 | 0.49 | 0.01 * | 0.28 | 2.92 | ||
| Pre-Fup 2 | 0.78 | 0.64 | 0.99 | −0.97 | 2.53 | ||
| Physical exercise | Pre-Post-test | 1.29 | 0.69 | 0.40 | −0.59 | 3.16 | |
| Pre-Fup 1 | 1.24 | 0.53 | 0.13 | −0.20 | 2.68 | ||
| Pre-Fup 2 | −0.24 | 0.70 | 0.99 | −2.14 | 1.67 | ||
| Stress | Mindfulness | Pre-Post-test | 0.80 | 0.44 | 0.43 | −0.39 | 1.99 |
| Pre-Fup 1 | 1.20 | 0.38 | 0.01 * | 0.17 | 2.23 | ||
| Pre-Fup 2 | 1.04 | 0.46 | 0.16 | −0.21 | 2.29 | ||
| Physical exercise | Pre-Post-test | 1.19 | 0.48 | 0.09 | −0.10 | 2.48 | |
| Pre-Fup 1 | 0.95 | 0.41 | 0.14 | −0.17 | 2.07 | ||
| Pre-Fup 2 | 0.00 | 0.50 | 0.99 | −1.36 | 1.36 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Díaz-Silveira, C.; Alcover, C.-M.; Burgos, F.; Marcos, A.; Santed, M.A. Mindfulness versus Physical Exercise: Effects of Two Recovery Strategies on Mental Health, Stress and Immunoglobulin A during Lunch Breaks. A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 2839. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082839
Díaz-Silveira C, Alcover C-M, Burgos F, Marcos A, Santed MA. Mindfulness versus Physical Exercise: Effects of Two Recovery Strategies on Mental Health, Stress and Immunoglobulin A during Lunch Breaks. A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2020; 17(8):2839. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082839
Chicago/Turabian StyleDíaz-Silveira, Cintia, Carlos-María Alcover, Francisco Burgos, Alberto Marcos, and Miguel A. Santed. 2020. "Mindfulness versus Physical Exercise: Effects of Two Recovery Strategies on Mental Health, Stress and Immunoglobulin A during Lunch Breaks. A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 17, no. 8: 2839. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082839