Cost-Effectiveness of Supervised versus Unsupervised Rehabilitation for Rotator-Cuff Repair: Systematic Review and Meta-Analysis

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
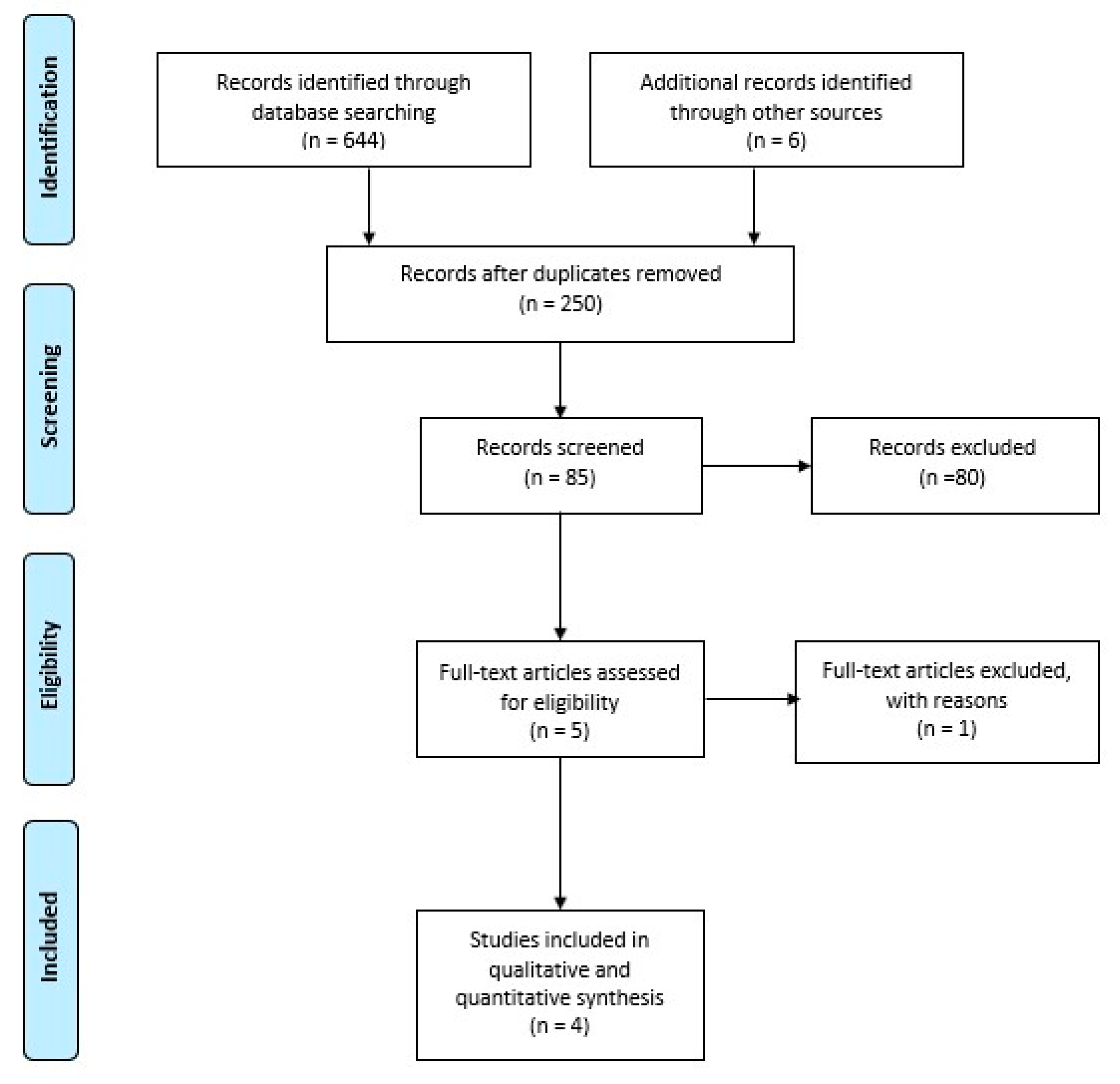
2.1. Literature-Search Strategy and Study Selection
2.2. Data-Extraction Process
2.3. Meta-Analysis
2.4. Quality Assessment
3. Results
3.1. Demographics
3.2. RC Tear Characteristics
3.3. Clinical Outcomes
3.4. Range of Motion
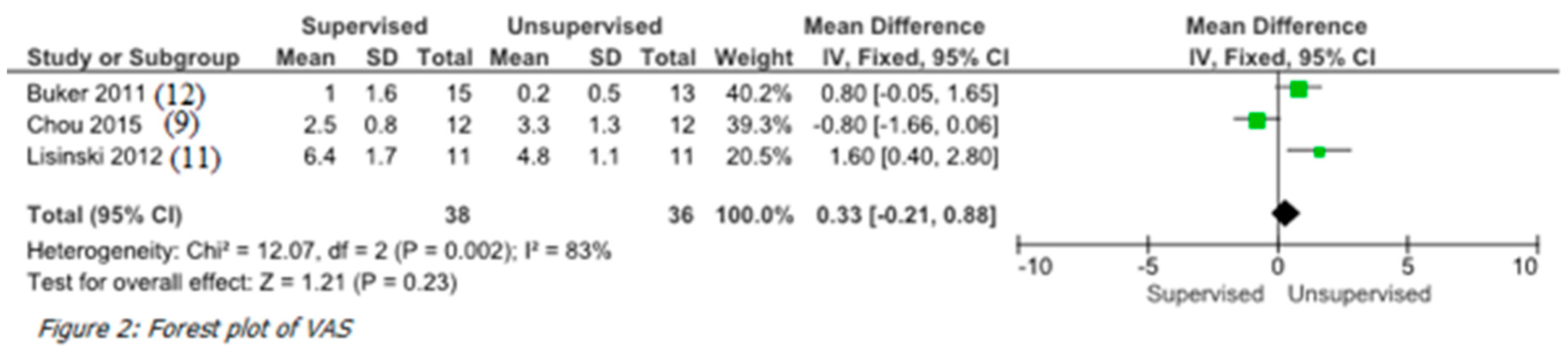
3.5. VAS Score
3.6. Meta-Analysis
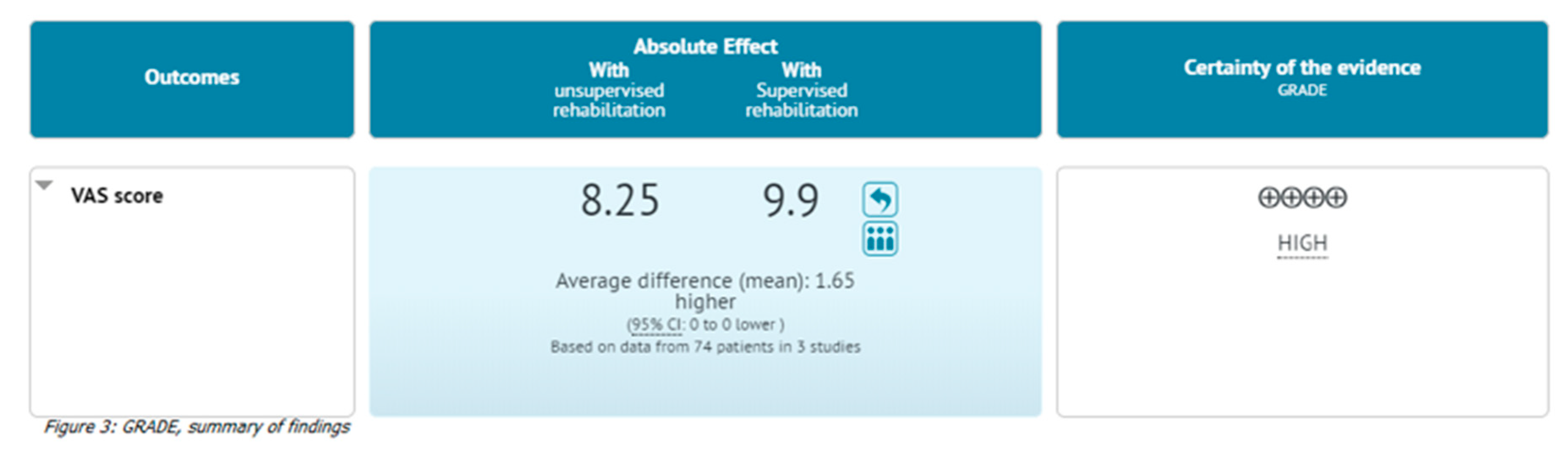
3.7. Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dickinson, R.N.; Kuhn, J.E.; Bergner, J.L.; Rizzone, K.H. A systematic review of cost-effective treatment of postoperative rotator cuff repairs. J. Shoulder Elb. Surg. 2017, 26, 915–922. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Berton, A.; Papapietro, N.; Maffulli, N.; Denaro, V. Epidemiology, genetics and biological factors of rotator cuff tears. Med. Sport Sci. 2012, 57, 1–9. [Google Scholar] [PubMed]
- Salvatore, G.; Longo, U.G.; Candela, V.; Berton, A.; Migliorini, F.; Petrillo, S.; Ambrogioni, L.R.; Denaro, V. Epidemiology of rotator cuff surgery in Italy: Regional variation in access to health care. Results from a 14-year nationwide registry. Musculoskelet. Surg. 2019. [Google Scholar] [CrossRef]
- Longo, U.G.; Salvatore, G.; Rizzello, G.; Berton, A.; Ciuffreda, M.; Candela, V.; Denaro, V. The burden of rotator cuff surgery in Italy: A nationwide registry study. Arch. Orthop. Trauma Surg. 2017, 137, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Petrillo, S.; Candela, V.; Rizzello, G.; Loppini, M.; Maffulli, N.; Denaro, V. Arthroscopic rotator cuff repair with and without subacromial decompression is safe and effective: A clinical study. Bmc Musculoskelet. Disord. 2020, 21, 24. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Petrillo, S.; Loppini, M.; Candela, V.; Rizzello, G.; Maffulli, N.; Denaro, V. Metallic versus biodegradable suture anchors for rotator cuff repair: A case control study. Bmc Musculoskelet. Disord. 2019, 20, 477. [Google Scholar] [CrossRef]
- Moosmayer, S.; Lund, G.; Seljom, U.S.; Haldorsen, B.; Svege, I.C.; Hennig, T.; Pripp, A.H.; Smith, H.J. At a 10-Year Follow-up, Tendon Repair Is Superior to Physiotherapy in the Treatment of Small and Medium-Sized Rotator Cuff Tears. J. Bone Jt. Surg. Am. 2019, 101, 1050–1060. [Google Scholar] [CrossRef]
- Piper, C.C.; Hughes, A.J.; Ma, Y.; Wang, H.; Neviaser, A.S. Operative versus nonoperative treatment for the management of full-thickness rotator cuff tears: A systematic review and meta-analysis. J. Shoulder Elb. Surg. 2018, 27, 572–576. [Google Scholar] [CrossRef]
- Longo, U.G.; Franceschi, F.; Berton, A.; Maffulli, N.; Droena, V. Conservative treatment and rotator cuff tear progression. Med. Sport Sci. 2012, 57, 90–99. [Google Scholar]
- Kukkonen, J.; Joukainen, A.; Lehtinen, J.; Mattila, K.T.; Tuominen, E.K.; Kauko, T.; Äärimaa, V. Treatment of Nontraumatic Rotator Cuff Tears: A Randomized Controlled Trial with Two Years of Clinical and Imaging Follow-up. J. Bone Jt. Surg. Am. 2015, 97, 1729–1737. [Google Scholar] [CrossRef]
- Lambers Heerspink, F.O.; van Raay, J.J.; Koorevaar, R.C.; van Eerden, P.J.; Westerbeek, R.E.; van ‘t Riet, E.; van den Akker-Scheek, I.; Diercks, R.L. Comparing surgical repair with conservative treatment for degenerative rotator cuff tears: A randomized controlled trial. J. Shoulder Elb. Surg. 2015, 24, 1274–1281. [Google Scholar] [CrossRef] [PubMed]
- Carnevale, A.; Longo, U.G.; Schena, E.; Massaroni, C.; Lo Presti, D.; Berton, A.; Candela, V.; Denaro, D. Wearable systems for shoulder kinematics assessment: A systematic review. Bmc Musculoskelet. Disord. 2019, 20, 546. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Facchinetti, G.; Marchetti, A.; Candela, V.; Risi Ambrogioni, L.; Faldetta, A.; de Marinis, M.G.; Denaro, V. Sleep Disturbance and Rotator Cuff Tears: A Systematic Review. Medicina (Kaunas) 2019, 55, 453. [Google Scholar] [CrossRef] [Green Version]
- Longo, U.G.; Risi Ambrogioni, L.; Berton, A.; Candela, V.; Carnevale, A.; Schena, E.; Gugliemelli, E.; Denaro, V. Physical therapy and precision rehabilitation in shoulder rotator cuff disease. Int. Orthop. 2020. [Google Scholar] [CrossRef]
- Roddey, T.S.; Olson, S.L.; Gartsman, G.M.; Hanten, W.P.; Cook, K.F. A randomized controlled trial comparing 2 instructional approaches to home exercise instruction following arthroscopic full-thickness rotator cuff repair surgery. J. Orthop. Sports Phys. 2002, 32, 548–559. [Google Scholar] [CrossRef] [PubMed]
- Mather, R.C.; Koenig, L.; Acevedo, D.; Dall, T.M.; Gallo, P.; Romeo, A.; Tongue, J.; Williams, G. The societal and economic value of rotator cuff repair. J. Bone Jt. Surg. Am. 2013, 95, 1993–2000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikolaidou, O.; Migkou, S.; Karampalis, C. Rehabilitation after Rotator Cuff Repair. Open Orthop. J. 2017, 11, 154–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, K.V.; Hung, C.Y.; Han, D.S.; Chen, W.S.; Wang, T.G.; Chien, K.L. Early Versus Delayed Passive Range of Motion Exercise for Arthroscopic Rotator Cuff Repair: A Meta-analysis of Randomized Controlled Trials. Am. J. Sports Med. 2015, 43, 1265–1273. [Google Scholar] [CrossRef]
- Düzgün, I.; Baltacı, G.; Atay, O.A. Comparison of slow and accelerated rehabilitation protocol after arthroscopic rotator cuff repair: Pain and functional activity. Acta Orthop. Traumatol. Turc. 2011, 45, 23–33. [Google Scholar] [CrossRef]
- Düzgün, İ.; Baltacı, G.; Turgut, E.; Atay, O.A. Effects of slow and accelerated rehabilitation protocols on range of motion after arthroscopic rotator cuff repair. Acta Orthop. Traumatol. Turc. 2014, 48, 642–648. [Google Scholar] [CrossRef]
- Longo, U.G.; Rizzello, G.; Petrillo, S.; Loppini, M.; Maffulli, N.; Denaro, V. Conservative Rehabilitation Provides Superior Clinical Results Compared to Early Aggressive Rehabilitation for Rotator Cuff Repair: A Retrospective Comparative Study. Medicina (Kaunas) 2019, 55, 402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, C.T.; Hu, W.; Wen, C.S.; Wang, S.F.; Lieu, F.K.; Teng, J.T. Efficacy of informed versus uninformed physiotherapy on postoperative retear rates of medium-sized and large rotator cuff tears. J. Shoulder Elb. Surg. 2015, 24, 1413–1420. [Google Scholar] [CrossRef] [PubMed]
- Buker, N.; Kitis, A.; Akkaya, S.; Akkaya, N. [Comparison of the results of supervised physiotherapy program and home-based exercise program in patients treated with arthroscopic-assisted mini-open rotator cuff repair]. Eklem Hast. Cerrahisi 2011, 22, 134–139. [Google Scholar]
- Hayes, K.; Ginn, K.A.; Walton, J.R.; Szomor, Z.L.; Murrell, G.A. A randomised clinical trial evaluating the efficacy of physiotherapy after rotator cuff repair. Aust. J. Physiother. 2004, 50, 77–83. [Google Scholar] [CrossRef] [Green Version]
- Lisinski, P.; Huber, J.; Wilkosz, P.; Witkowska, A.; Wytrazek, M.; Samborski, W.; Zagloba, A. Supervised versus uncontrolled rehabilitation of patients after rotator cuff repair-clinical and neurophysiological comparative study. Int. J. Artif. Organs. 2012, 35, 45–54. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Montori, V.; Akl, E.A.; Djulbegovic, B.; Falck-Ytter, Y.; et al. GRADE guidelines: 4. Rat. Qual. Evid. -Study Limit. (Risk Bias). J. Clin. Epidemiol. 2011, 64, 407–415. [Google Scholar] [CrossRef]
- Longo, U.G.; Lamberti, A.; Maffulli, N.; Denaro, V. Tissue engineered biological augmentation for tendon healing: A systematic review. Br. Med. Bull. 2011, 98, 31–59. [Google Scholar] [CrossRef] [Green Version]
- Longo, U.G.; Candela, V.; Berton, A.; Salvatore, G.; Guarnieri, A.; DeAngelis, J.; Nazarian, A.; Denaro, V. Genetic basis of rotator cuff injury: A systematic review. Bmc Med. Genet. 2019, 20, 149. [Google Scholar] [CrossRef] [Green Version]
- Del Buono, A.; Oliva, F.; Longo, U.G.; Rodeo, S.A.; Orchard, J.; Denaro, V.; Maffulli, N. Metalloproteases and rotator cuff disease. J. Shoulder Elb. Surg. 2012, 21, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Berton, A.; Khan, W.S.; Maffulli, N.; Denaro, V. Histopathology of rotator cuff tears. Sports Med. Arthrosc. Rev. 2011, 19, 227–236. [Google Scholar] [CrossRef]
- Maffulli, N.; Margiotti, K.; Longo, U.G.; Loppini, M.; Fazio, V.M.; Denaro, V. The genetics of sports injuries and athletic performance. MusclesLigaments Tendons J. 2013, 3, 173–189. [Google Scholar] [CrossRef] [Green Version]
- Longo, U.G.; Ciuffreda, M.; Locher, J.; Buchmann, S.; Maffulli, N.; Denaro, V. The effectiveness of conservative and surgical treatment for shoulder stiffness: A systematic review of current literature. Br. Med. Bull. 2018, 127, 111–143. [Google Scholar] [CrossRef] [PubMed]
- Khan, W.S.; Adesida, A.B.; Tew, S.R.; Longo, U.G.; Hardingham, T.E. Fat pad-derived mesenchymal stem cells as a potential source for cell-based adipose tissue repair strategies. Cell Prolif. 2012, 45, 111–120. [Google Scholar] [CrossRef]
- Franceschi, F.; Longo, U.G.; Ruzzini, L.; Rizzello, G.; Maffulli, N.; Denaro, V. Soft tissue tenodesis of the long head of the biceps tendon associated to the Roman Bridge repair. Bmc Musculoskelet. Disord. 2008, 9, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longo, U.G.; Franceschi, F.; Spiezia, F.; Marinozzi, A.; Maffulli, N.; Denaro, V. The low-profile Roman bridge technique for knotless double-row repair of the rotator cuff. Arch. Orthop. Trauma Surg. 2011, 131, 357–361. [Google Scholar] [CrossRef]
- Franceschi, F.; Longo, U.G.; Ruzzini, L.; Rizzello, G.; Maffulli, N.; Denaro, V. The Roman Bridge: A “double pulley-suture bridges” technique for rotator cuff repair. Bmc Musculoskelet. Disord. 2007, 8, 123. [Google Scholar] [CrossRef] [Green Version]
- Longo, U.G.; Margiotti, K.; Petrillo, S.; Rizzello, G.; Fusilli, C.; Maffulli, N.; De Luca, A.; Denaro, D. Genetics of rotator cuff tears: No association of col5a1 gene in a case-control study. Bmc Med. Genet. 2018, 19, 217. [Google Scholar] [CrossRef]
- Longo, U.G.; Franceschi, F.; Ruzzini, L.; Spiezia, F.; Maffulli, N.; Denaro, V. Higher fasting plasma glucose levels within the normoglycaemic range and rotator cuff tears. Br. J. Sports Med. 2009, 43, 284–287. [Google Scholar] [CrossRef]
- Maffulli, N.; Longo, U.G.; Berton, A.; Loppini, M.; Denaro, V. Biological factors in the pathogenesis of rotator cuff tears. Sports Med. Arthrosc. Rev. 2011, 19, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Forriol, F.; Campi, S.; Maffulli, N.; Denaro, V. Animal models for translational research on shoulder pathologies: From bench to bedside. Sports Med. Arthrosc. Rev. 2011, 19, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Thorpe, A.M.; O’Sullivan, P.B.; Mitchell, T.; Hurworth, M.; Spencer, J.; Booth, G.; Goebel, S.; Khoo, P.; Tay, A.; Smith, S. Are Psychologic Factors Associated With Shoulder Scores After Rotator Cuff Surgery? Clin. Orthop. Relat. Res. 2018, 476, 2062–2073. [Google Scholar] [CrossRef] [PubMed]
- Analay Akbaba, Y.; Kaya Mutlu, E.; Altun, S.; Celik, D. Does the patients’ expectations on kinesiotape affect the outcomes of patients with a rotator cuff tear? A randomized controlled clinical trial. Clin. Rehabil. 2018, 32, 1509–1519. [Google Scholar] [CrossRef] [PubMed]
- Khazzam, M.S.; Mulligan, E.P.; Brunette-Christiansen, M.; Shirley, Z. Sleep Quality in Patients With Rotator Cuff Disease. J. Am. Acad. Orthop. Surg. 2018, 26, 215–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillespie, M.A.; MCznik, A.; Wassinger, C.A.; Sole, G. Rotator cuff-related pain: Patients’ understanding and experiences. Musculoskelet. Sci. Pr. 2017, 30, 64–71. [Google Scholar] [CrossRef]
- Serbest, S.; Tiftikçi, U.; Askın, A.; Yaman, F.; Alpua, M. Preoperative and post-operative sleep quality evaluation in rotator cuff tear patients. Knee Surg. Sports Traumatol Arthrosc. 2017, 25, 2109–2113. [Google Scholar] [CrossRef]
- Wylie, J.D.; Suter, T.; Potter, M.Q.; Granger, E.K.; Tashjian, R.Z. Mental Health Has a Stronger Association with Patient-Reported Shoulder Pain and Function Than Tear Size in Patients with Full-Thickness Rotator Cuff Tears. J. Bone Jt. Surg. Am. 2016, 98, 251–256. [Google Scholar] [CrossRef] [Green Version]
- Hiscock, N.; Bell, S.; Coghlan, J. Pain, depression and the postoperative stiff shoulder. Bmc Musculoskelet Disord. 2015, 16, 376. [Google Scholar] [CrossRef] [Green Version]
- Potter, M.Q.; Wylie, J.D.; Greis, P.E.; Burks, R.T.; Tashjian, R.Z. Psychological distress negatively affects self-assessment of shoulder function in patients with rotator cuff tears. Clin. Orthop. Relat. Res. 2014, 472, 3926–3932. [Google Scholar] [CrossRef] [Green Version]
- Klein, J.S.; Davis, D.E.; Wells, Z.S.; Kane, L.T.; Sholder, D.; Namdari, S.; Abboud, J.A. The Distress and Risk Assessment Method predicts postoperative narcotic use in patients undergoing rotator cuff repair. J. Shoulder Elb. Surg. 2019, 28, S146–S153. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Authors | Study Design | No. of Patients | Rehabilitation Form (Shoulder No.) | Sex | Mean Age ± SD (Range, Year) | Dominant (%) | Not Dominant (%) | Size of Lesion ± SD (Range, cm) | Time of Follow-Up (Weeks) | No. of Rotator-Cuff Tendons Torn | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M (%) | F (%) | 1 | 2 | 3 | 4 | |||||||||
| Buker N. et al., 2011 [23] | Randomized clinical trial (II) | 28 | Supervised (15) | 5 (18%) | 23 (82%) | 59.8 ± 9.1 (40–83) | - | - | - | 12 | - | - | - | - |
| Unsupervised (13) | - | - | - | - | - | - | - | |||||||
| Chou C. et al., 2015 [22] | Randomized clinical trial (II) | 24 | Supervised (12) | 4 (33%) | 8 (67%) | 65.1 ± 8.7 | - | - | 2.42 ± 1.10 | 12 | - | - | - | - |
| Unsupervised (12) | 3 (25%) | 9 (75%) | 67.9 ± 9.6 | - | - | 2.8 ± 1.47 | - | - | - | - | ||||
| Hayes K. et al., 2004 [24] | Randomized clinical trial (II) | 58 | Supervised (26) | 20 (77%) | 6 (23%) | 58 ± 10 (41–81) | 20 (77%) | 6 (23%) | 2.23 ± 2.64 (1–5.2) | 24 | 18 | 6 | 2 | 0 |
| Unsupervised (32) | 20 (63%) | 12 (37%) | 62 ± 11 (42–83) | 19 (59%) | 13 (41%) | 2.45 ± 2.82 (1–5.47) | 20 | 7 | 5 | 0 | ||||
| Lisinski P. et al., 2012 [25] | Randomized clinical trial (II) | 22 | Supervised (11) | 6 (55%) | 5 (45%) | 45 (15–60) | - | - | 2.66 (1–5) | 5 | - | - | - | - |
| Unsupervised (11) | 6 (55%) | 5 (45%) | 46 (19–50) | - | - | 2.83 (1–5) | - | - | - | - | ||||
| Authors | Rehabilitation Form (Shoulder No.) | Clinical Outcomes | ROM | VAS Score | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Constant–Murley Score | SPADI | UPenn | ASES | UCLA | DASH | BDI | Forward Elevation ± SD (Range, Degrees) | Abduction ± SD (Range, Degrees) | External Rotation ± SD (Range, Degrees) | |||
| Buker N. et al., 2011 [23] | Supervised (15) | 51.53 ± 10.69 | - | - | - | - | - | 7.8 ± 4.16 | - | - | - | 1.00 |
| Unsupervised (13) | 72.23 ± 7.35 | - | - | - | - | - | 7.77 ± 6.69 | - | - | - | 0.15 | |
| Chou C. et al., 2015 [22] | Supervised (12) | 22.6 | - | - | 73.2 | 24.2 | 42.4 | - | - | - | - | 2.5 |
| Unsupervised (12) | 27.7 | - | - | 62.6 | 17.9 | 45.4 | - | - | - | - | 3.3 | |
| Hayes K. et al., 2004 [24] | Supervised (26) | - | - | - | - | - | - | - | 150 (142–158) | 142 (130–154) | 51 (46–56) | - |
| Unsupervised (32) | - | - | - | - | - | - | - | 144 (132–156) | 130 (117–143) | 43 (36–50) | - | |
| Lisinski P. et al., 2012 [25] | Supervised (11) | - | - | - | - | - | - | - | - | - | - | 6.4 |
| Unsupervised (11) | - | - | - | - | - | - | - | - | - | - | 4.8 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Longo, U.G.; Berton, A.; Risi Ambrogioni, L.; Lo Presti, D.; Carnevale, A.; Candela, V.; Stelitano, G.; Schena, E.; Nazarian, A.; Denaro, V. Cost-Effectiveness of Supervised versus Unsupervised Rehabilitation for Rotator-Cuff Repair: Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 2852. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082852
Longo UG, Berton A, Risi Ambrogioni L, Lo Presti D, Carnevale A, Candela V, Stelitano G, Schena E, Nazarian A, Denaro V. Cost-Effectiveness of Supervised versus Unsupervised Rehabilitation for Rotator-Cuff Repair: Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(8):2852. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082852
Chicago/Turabian StyleLongo, Umile Giuseppe, Alessandra Berton, Laura Risi Ambrogioni, Daniela Lo Presti, Arianna Carnevale, Vincenzo Candela, Giovanna Stelitano, Emiliano Schena, Ara Nazarian, and Vincenzo Denaro. 2020. "Cost-Effectiveness of Supervised versus Unsupervised Rehabilitation for Rotator-Cuff Repair: Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 8: 2852. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082852