Effects of the Healthy Children, Healthy Families, Healthy Communities Program for Obesity Prevention among Vulnerable Children: A Cluster-Randomized Controlled Trial


Abstract
:1. Introduction
2. Materials and Methods
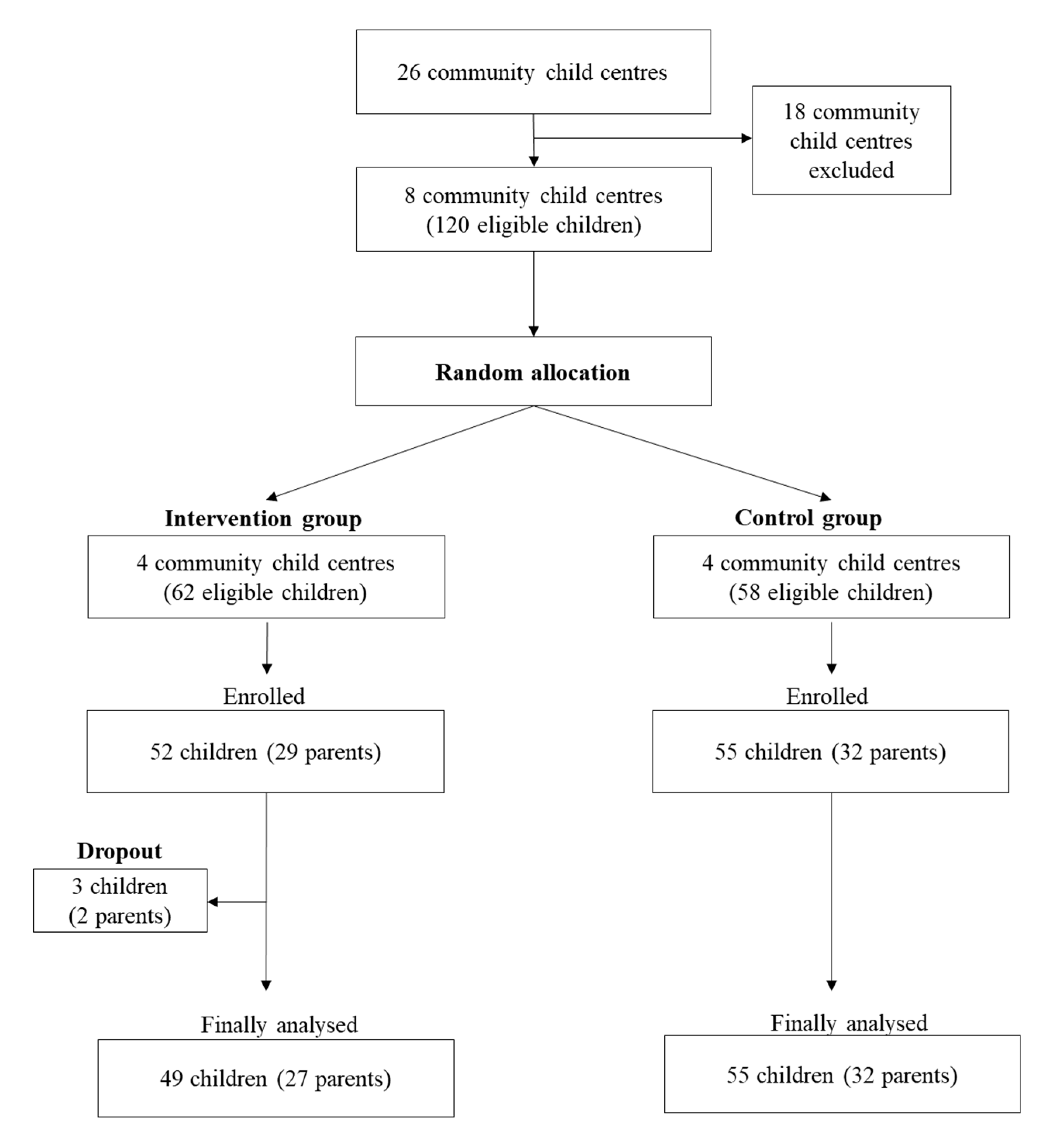
2.1. Study Design and Participants
2.2. The Three-Healthy Programme
2.3. Measures
2.3.1. Participants’ Baseline General Characteristics
2.3.2. Children’s Knowledge of Healthy Lifestyle Behaviors
2.3.3. Children’s Healthy Lifestyle Behaviors
2.3.4. Children’s Obesity Status
2.3.5. Parenting Behaviors
2.4. Ethical Considerations
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Strategy on Diet, Physical Activity and Health: Childhood Overweight and Obesity. Available online: https://www.who.int/dietphysicalactivity/childhood/en/ (accessed on 15 April 2020).
- Choo, J.; Kim, H.J.; Yang, H.M.; Kim, S. An Obesity Prevention Framework for Vulnerable Children Based on A Methodology of Community-Based Participatory Research: Using A Strategy of Training Community Lay Health Advisors; Korea Health Promotion Foundation: Seoul, Korea, 2013. [Google Scholar]
- Ogden, C.L.; Carroll, M.D.; Fakhouri, T.H.; Hales, C.M.; Fryar, C.D.; Li, X.F.; Freedman, D.S. Prevalence of obesity among youths by household income and education level of head of household—United States 2011–2014. Morbid. Mortal. Wkly. Rep. 2018, 67, 186–189. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Harris, K.M.; Gordon-Larsen, P. Life course perspectives on the links between ooverty and obesity during the transition to young adulthood. Popul. Res. Policy Rev. 2009, 28, 505–532. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Chen, W.; Srinivasan, S.R.; Bond, M.G.; Tang, R.; Urbina, E.M.; Berenson, G.S. Childhood cardiovascular risk factors and carotid vascular changes in adulthood: The Bogalusa Heart Study. JAMA 2003, 290, 2271–2276. [Google Scholar] [CrossRef] [PubMed]
- Simons-Morton, B.; McLeroy, K.; Wendel, M. Behavior Theory in Health Promotion Practice and Research, 1st ed.; Jones & Bartlett Learning: Burlington, MA, USA, 2011. [Google Scholar]
- Reifsnider, E.; Gallagher, M.; Forgione, B. Using ecological models in research on health disparities. J. Prof. Nurs. 2005, 21, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Ledoux, T.A.; Hingle, M.D.; Baranowski, T. Relationship of fruit and vegetable intake with adiposity: A systematic review. Obes. Rev. 2011, 12, e143–e150. [Google Scholar] [CrossRef] [PubMed]
- LaRowe, T.L.; Adams, A.K.; Jobe, J.B.; Cronin, K.A.; Vannatter, S.M.; Prince, R.J. Dietary intakes and physical activity among preschool-aged children living in rural American Indian communities before a family-based healthy lifestyle intervention. J. Am. Diet. Assoc. 2010, 110, 1049–1057. [Google Scholar] [CrossRef] [Green Version]
- Malik, V.S.; Schulze, M.B.; Hu, F.B. Intake of sugar-sweetened beverages and weight gain: A systematic review. Am. J. Clin. Nutr. 2006, 84, 274–288. [Google Scholar] [CrossRef]
- Kosova, E.C.; Auinger, P.; Bremer, A.A. The relationships between sugar-sweetened beverage intake and cardiometabolic markers in young children. J. Acad. Nutr. Diet. 2013, 113, 219–227. [Google Scholar] [CrossRef] [Green Version]
- Janssen, I.; Leblanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef] [Green Version]
- AlMarzooqi, M.A.; Nagy, M.C. Childhood obesity intervention programs: A systematic review. Life Sci. J. 2011, 8, 45–60. [Google Scholar]
- McCarthy, M.I. Genomics, type 2 diabetes, and obesity. N. Engl. J. Med. 2010, 363, 2339–2350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geserick, M.; Vogel, M.; Gausche, R.; Lipek, T.; Spielau, U.; Keller, E.; Pfaffle, R.; Kiess, W.; Korner, A. Acceleration of BMI in early childhood and risk of sustained obesity. N. Engl. J. Med. 2018, 379, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- Qi, Q.; Chu, A.Y.; Kang, J.H.; Jensen, M.K.; Curhan, G.C.; Pasquale, L.R.; Ridker, P.M.; Hunter, D.J.; Willett, W.C.; Rimm, E.B.; et al. Sugar-sweetened beverages and genetic risk of obesity. N. Engl. J. Med. 2012, 367, 1387–1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bronfenbrenner, U. The Ecology of Human Development; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An ecological perspective on health promotion programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef] [PubMed]
- Choo, J.; Kim, H.J.; Turk, M.T.; Kim, E.K.; Yang, K.S. Ecological factors associated with behavioral problems in vulnerable children. Jpn. J. Nurs. Sci. 2017, 14, 205–218. [Google Scholar] [CrossRef]
- Ihmels, M.A.; Welk, G.J.; Eisenmann, J.C.; Nusser, S.M. Development and preliminary validation of a Family Nutrition and Physical Activity (FNPA) screening tool. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 14. [Google Scholar] [CrossRef] [Green Version]
- Brown, C.L.; Halvorson, E.E.; Cohen, G.M.; Lazorick, S.; Skelton, J.A. Addressing childhood obesity: Opportunities for prevention. Pediatr. Clin. 2015, 62, 1241–1261. [Google Scholar] [CrossRef] [Green Version]
- Herbenick, S.K.; James, K.; Milton, J.; Cannon, D. Effects of family nutrition and physical activity screening for obesity risk in school-age children. J. Spec. Pediatr. Nurs. 2018, 23, e12229. [Google Scholar] [CrossRef]
- Langer, S.L.; Seburg, E.; JaKa, M.M.; Sherwood, N.E.; Levy, R.L. Predicting dietary intake among children classified as overweight or at risk for overweight: Independent and interactive effects of parenting practices and styles. Appetite 2017, 110, 72–79. [Google Scholar] [CrossRef] [Green Version]
- Lopez, N.V.; Schembre, S.; Belcher, B.R.; O’Connor, S.; Maher, J.P.; Arbel, R.; Margolin, G.; Dunton, G.F. Parenting styles, food-related parenting practices, and children’s healthy eating: A mediation analysis to examine relationships between parenting and child diet. Appetite 2018, 128, 205–213. [Google Scholar] [CrossRef]
- Shloim, N.; Edelson, L.R.; Martin, N.; Hetherington, M.M. Parenting styles, feeding styles, feeding practices, and weight status in 4–12 year-old children: A systematic review of the literature. Front. Psychol. 2015, 6, 1849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belsky, J.; Melhuish, E.; Barnes, J.; Leyland, A.H.; Romaniuk, H. Effects of Sure Start local programmes on children and families: Early findings from a quasi-experimental, cross sectional study. BMJ 2006, 332, 1476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gray, R.; Francis, E. The implications of US experiences with early childhood interventions for the UK Sure Start Programme. Child Care Health Dev. 2007, 33, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare. The Guideline for the 2019 Community Child Center Program. Available online: https://www.icareinfo.go.kr/info/research/researchList.do?menuNo=2001400 (accessed on 11 July 2019).
- Swinburn, B.; Egger, G.; Raza, F. Dissecting obesogenic environments: The development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev. Med. 1999, 29, 563–570. [Google Scholar] [CrossRef]
- Choo, J.; Kim, H.J.; Park, S. Neighborhood environments: Links to health behaviors and obesity status in vulnerable children. West. J. Nurs. Res. 2017, 39, 1169–1191. [Google Scholar] [CrossRef]
- Park, S.; Choo, J.; Chang, S.O. Healthy eating for obese children from socioeconomically disadvantaged families: Its ecological factors and strategies. J. Transcult. Nurs. 2019, 30, 268–279. [Google Scholar] [CrossRef]
- Hemming, K.; Girling, A.J.; Sitch, A.J.; Marsh, J.; Lilford, R.J. Sample size calculations for cluster randomised controlled trials with a fixed number of clusters. BMC Med. Res. Methodol. 2011, 11, 102. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.Y.; Kao, C.C.; Hsu, H.Y.; Wang, R.H.; Hsu, S.H. The Efficacy of a family-based intervention program on childhood obesity: A quasi-experimental design. Biol. Res. Nurs. 2015, 17, 510–520. [Google Scholar] [CrossRef]
- Artinian, N.T.; Fletcher, G.F.; Mozaffarian, D.; Kris-Etherton, P.; Van Horn, L.; Lichtenstein, A.H.; Kumanyika, S.; Kraus, W.E.; Fleg, J.L.; Redeker, N.S.; et al. Interventions to promote physical activity and dietary lifestyle changes for cardiovascular risk factor reduction in adults: A scientific statement from the American Heart Association. Circulation 2010, 122, 406–441. [Google Scholar] [CrossRef]
- Battjes-Fries, M.C.E.; Haveman-Nies, A.; Zeinstra, G.G.; van Dongen, E.J.I.; Meester, H.J.; van den Top-Pullen, R.; Van‘t Veer, P.; de Graaf, K. Effectiveness of Taste Lessons with and without additional experiential learning activities on children’s willingness to taste vegetables. Appetite 2017, 109, 201–208. [Google Scholar] [CrossRef]
- Rogers, V.W.; Hart, P.H.; Motyka, E.; Rines, E.N.; Vine, J.; Deatrick, D.A. Impact of Let’s Go! 5-2-1-0: A community-based, multisetting childhood obesity prevention program. J. Pediatr. Psychol. 2013, 38, 1010–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tremblay, M.S.; LeBlanc, A.G.; Janssen, I.; Kho, M.E.; Hicks, A.; Murumets, K.; Colley, R.C.; Duggan, M. Canadian sedentary behaviour guidelines for children and youth. Appl. Physiol. Nutr. Metab. 2011, 36, 59–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korea Centers for Disease Control and Prevention. 2007 Korean National Growth Charts: Standard Growth Charts for Childhood. Available online: http://www.cdc.go.kr/CDC/info/CdcKrInfo0201.jsp?menuIds=HOME001-MNU1155-MNU1083-MNU1375-MNU0025&cid=1235 (accessed on 5 April 2012).
- Must, A.; Anderson, S.E. Body mass index in children and adolescents: Considerations for population-based applications. Int. J. Obes. 2006, 30, 590–594. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Growth reference 5–19 years—Application tools: WHO AnthroPlus Software. Available online: http://www.who.int/growthref/tools/en/ (accessed on 17 July 2019).
- The FNPA User Group. Family Nutrition and Physical Activity (FNPA). Available online: http://www.myfnpa.org/ (accessed on 10 July 2019).
- Ministry of Health and Welfare. 2015 Minimum Cost of Living. Available online: http://www.mohw.go.kr/react/jb/sjb0406vw.jsp?PAR_MENU_ID=03&MENU_ID=030406&CONT_SEQ=322026 (accessed on 11 July 2019).
- Nystrom, C.D.; Sandin, S.; Henriksson, P.; Henriksson, H.; Trolle-Lagerros, Y.; Larsson, C.; Maddison, R.; Ortega, F.B.; Pomeroy, J.; Ruiz, J.R.; et al. Mobile-based intervention intended to stop obesity in preschool-aged children: The MINISTOP randomized controlled trial. Am. J. Clin. Nutr. 2017, 105, 1327–1335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorely, T.; Nevill, M.E.; Morris, J.G.; Stensel, D.J.; Nevill, A. Effect of a school-based intervention to promote healthy lifestyles in 7-11 year old children. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 5. [Google Scholar] [CrossRef] [Green Version]
- Ardic, A.; Erdogan, S. The effectiveness of the COPE healthy lifestyles TEEN program: A school-based intervention in middle school adolescents with 12-month follow-up. J. Adv. Nurs. 2017, 73, 1377–1389. [Google Scholar] [CrossRef] [PubMed]
- Tam, S.F. The effects of a computer skill training programme adopting social comparison and self-efficacy enhancement strategies on self-concept and skill outcome in trainees with physical disabilities. Disabil. Rehabil. 2000, 22, 655–664. [Google Scholar] [CrossRef]
- Choo, J.; Kang, H. Predictors of initial weight loss among women with abdominal obesity: A path model using self-efficacy and health-promoting behaviour. J. Adv. Nurs. 2015, 71, 1087–1097. [Google Scholar] [CrossRef]
- Nezami, B.T.; Lang, W.; Jakicic, J.M.; Davis, K.K.; Polzien, K.; Rickman, A.D.; Hatley, K.E.; Tate, D.F. The effect of self-efficacy on behavior and weight in a behavioral weight-loss intervention. Health Psychol. 2016, 35, 714–722. [Google Scholar] [CrossRef]
- Kulik, N.L.; Moore, E.W.; Centeio, E.E.; Garn, A.C.; Martin, J.J.; Shen, B.; Somers, C.L.; McCaughtry, N. Knowledge, attitudes, self-efficacy, and healthy eating behavior among children: Results from the Building Healthy Communities trial. Health Educ. Behav. 2019, 46, 602–611. [Google Scholar] [CrossRef]
- Oosterhoff, M.; Joore, M.; Ferreira, I. The effects of school-based lifestyle interventions on body mass index and blood pressure: A multivariate multilevel meta-analysis of randomized controlled trials. Obes. Rev. 2016, 17, 1131–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, J.M.; DeFrang, R.; Orth, J.; Wakefield, S.; Howard, K. Evaluation of a primary care weight management program in children Aged 2–5 years: Changes in feeding practices, health behaviors, and body mass index. Nutrients 2019, 11, 498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, J.M.; Howard, K.; Guseman, E.H.; Yee, K.E.; Saturley, H.; Eisenmann, J.C. Association between the Family Nutrition and Physical Activity Screening Tool and obesity severity in youth referred to weight management. Obes. Res. Clin. Pract. 2017, 11, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Jackson, J.; Smit, E.; Manore, M.; John, D.; Gunter, K. The family-home nutrition environment and dietary intake in rural children. Nutrients 2015, 7, 9707–9720. [Google Scholar] [CrossRef] [Green Version]
- Verjans-Janssen, S.R.B.; van de Kolk, I.; Van Kann, D.H.H.; Kremers, S.P.J.; Gerards, S. Effectiveness of school-based physical activity and nutrition interventions with direct parental involvement on children’s BMI and energy balance-related behaviors—A systematic review. PLoS ONE 2018, 13, e0204560. [Google Scholar] [CrossRef]
- Bhave, S.; Pandit, A.; Yeravdekar, R.; Madkaikar, V.; Chinchwade, T.; Shaikh, N.; Shaikh, T.; Naik, S.; Marley-Zagar, E.; Fall, C.H. Effectiveness of a 5-year school-based intervention programme to reduce adiposity and improve fitness and lifestyle in Indian children; the SYM-KEM study. Arch. Dis. Child. 2016, 101, 33–41. [Google Scholar] [CrossRef] [Green Version]
- Lloyd, J.; Creanor, S.; Logan, S.; Green, C.; Dean, S.G.; Hillsdon, M.; Abraham, C.; Tomlinson, R.; Pearson, V.; Taylor, R.S.; et al. Effectiveness of the Healthy Lifestyles Programme (HeLP) to prevent obesity in UK primary-school children: A cluster randomised controlled trial. Lancet Child Adolesc. Health 2018, 2, 35–45. [Google Scholar] [CrossRef] [Green Version]
- Michels, N.; Sioen, I.; Braet, C.; Eiben, G.; Hebestreit, A.; Huybrechts, I.; Vanaelst, B.; Vyncke, K.; De Henauw, S. Stress, emotional eating behaviour and dietary patterns in children. Appetite 2012, 59, 762–769. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Level | Strategies | Contents |
|---|---|---|
| Child-level | Goal setting Self-monitoring Reinforcement Problem-solving Experiential learning activities | Six sessions of group teaching for healthy eating
|
| Parent-level | Goal setting Parent-led monitoring Reinforcement Supportive family environment | One group teaching session
|
| Center-level | Building a partnership Organizing educational curriculum Educating faculty Policy changes Collaborative activities | Building a partnership with university and centers Organizing educational curriculum
|
| Characteristics | n (%) or Mean (SD) | t/χ2 | p | |||||
|---|---|---|---|---|---|---|---|---|
| Total | Intervention Group | Control Group | ||||||
| Children | ||||||||
| No. of children (%) | 104 | (100) | 49 | (47.1) | 55 | (52.9) | ||
| Age (years) | 10.0 | (1.23) | 9.9 | (1.18) | 10.1 | (1.27) | 0.96 | 0.341 |
| Sex | <0.01 | 0.955 | ||||||
| Girl | 47 | (45.2) | 22 | (44.9) | 25 | (45.5) | ||
| Boy | 57 | (54.8) | 27 | (55.1) | 30 | (54.5) | ||
| Living with parents | 0.09 | 0.760 | ||||||
| Yes | 82 | (78.8) | 38 | (77.6) | 44 | (80.0) | ||
| No | 22 | (21.2) | 11 | (22.4) | 11 | (20.0) | ||
| Perceived SES | 1.69 | 0.194 | ||||||
| High | 44 | (42.3) | 24 | (49.0) | 20 | (36.4) | ||
| Low | 60 | (57.7) | 25 | (51.0) | 35 | (63.6) | ||
| Obesity status | 0.35 | 0.557 | ||||||
| Obese (BMI ≥ 85 %tile) | 37 | (35.6) | 16 | (32.7) | 21 | (38.2) | ||
| Normal (BMI < 85 %tile) | 67 | (64.4) | 33 | (67.4) | 334 | (61.8) | ||
| BMI z-score | 1.1 | (1.31) | 0.8 | (1.36) | 1.3 | (1.24) | 1.83 | 0.070 |
| Parents | ||||||||
| No. of parents (%) | 59 | (100) | 27 | (45.8) | 32 | (54.2) | ||
| Age (years) | 44.0 | (5.51) | 42.8 | (5.67) | 44.9 | (5.26) | 1.52 | 0.135 |
| Educational status | 3.31 | 0.069 | ||||||
| ≤College | 25 | (42.4) | 8 | (29.6) | 17 | (53.1) | ||
| < College | 34 | (57.6) | 19 | (70.4) | 15 | (46.9) | ||
| Monthly income ($) | 1.04 | 0.308 | ||||||
| High (> 1,754) | 39 | (66.1) | 16 | (59.3) | 23 | (71.9) | ||
| Low (< 1,754) | 20 | (33.9) | 11 | (40.7) | 9 | (28.1) | ||
| Health insurance | 1.05 | 0.307 | ||||||
| Medicare | 51 | (86.4) | 22 | (81.5) | 29 | (90.6) | ||
| Medicaid | 8 | (13.6) | 5 | (18.5) | 3 | (9.4) | ||
| Outcome Variables | Intervention Group | Control Group | p ‡ | p § | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | z | Pre-Test | Post-Test | z | |||||||
| N (%) or Mean (SD) | N (%) or Mean (SD) | |||||||||||
| Children (n = 104) | ||||||||||||
| Knowledge levels | 13.0 | (1.74) | 14.8 | (1.46) | 5.04 † | 13.7 | (2.04) | 14.2 | (1.88) | 3.01 † | 0.044 | 0.026 |
| Healthy behaviors | ||||||||||||
| Total composite score | 2.4 | (1.56) * | 3.4 | (2.12) | 21.84 † | 3.3 | (1.68) | 2.9 | (1.62) | −1.25 | 0.178 | <0.001 |
| Healthy eating behaviors | ||||||||||||
| Breakfast (yes, daily) | 25 | (51.0) | 30 | (61.2) | 3.08 † | 33 | (60.0) | 31 | (56.4) | −2.20 † | 0.562 | 0.128 |
| Fruits (≤2 times/day) | 5 | (10.2) * | 12 | (24.5) | 2.70 † | 15 | (27.3) | 14 | (25.5) | −0.34 | 0.940 | 0.376 |
| Vegetables (≤3 times/day) | 5 | (10.2) * | 13 | (26.5) | 2.14 † | 17 | (30.9) | 9 | (16.4) | −2.79 † | 0.241 | 0.011 |
| Milk (≤1 time/day) | 24 | (49.0) * | 29 | (59.2) | 1.05 | 41 | (74.6) | 32 | (58.2) | −3.50 † | 0.925 | 0.634 |
| Non-SSB (0 time/day) | 6 | (12.2) | 8 | (16.3) | 1.15 | 9 | (16.4) | 9 | (16.4) | 0.0 | 0.999 | 0.766 |
| Fast food (0 time/day) | 8 | (16.3) | 21 | (42.9) | 2.41 † | 13 | (23.6) | 18 | (32.7) | 1.12 | 0.303 | 0.628 |
| Family meal (≤ 1/day) | 22 | (44.9) | 23 | (46.9) | 0.57 | 18 | (32.7) | 14 | (25.5) | −1.44 | 0.010 | 0.001 |
| Healthy activity behaviors | ||||||||||||
| Days of sufficient PA | 2.8 | (2.25) | 4.3 | (2.16) | 2.51 † | 3.8 | (2.01) | 3.4 | (2.29) | −1.04 | 0.014 | 0.001 |
| Sufficient PA (7 days/wk) | 6 | (12.2) | 13 | (26.5) | 1.99 † | 7 | (12.7) | 8 | (14.6) | 0.25 | 0.206 | 0.043 |
| Non-sedentary behavior | 15 | (30.6) * | 17 | (34.7) | 0.42 | 29 | (52.7) | 26 | (47.3) | −1.23 | 0.038 | 0.438 |
| Obesity status | 16 | (32.7) | 18 | (36.7) | 2.50 † | 21 | (38.2) | 23 | (41.8) | 2.62 † | 0.689 | 0.490 |
| BMI z-score | 0.8 | (1.36) | 0.9 | (1.36) | 2.71 † | 1.3 | (1.24) | 1.3 | (1.22) | 0.30 | 0.173 | 0.050 |
| Parents (n = 59) | ||||||||||||
| FNPA score | 49.1 | (7.90) | 54.9 | (9.12) | −4.13 † | 49.4 | (7.24) | 49.4 | (7.40) | 0.0 | <0.001 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choo, J.; Yang, H.-M.; Jae, S.-Y.; Kim, H.-J.; You, J.; Lee, J. Effects of the Healthy Children, Healthy Families, Healthy Communities Program for Obesity Prevention among Vulnerable Children: A Cluster-Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 2895. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082895
Choo J, Yang H-M, Jae S-Y, Kim H-J, You J, Lee J. Effects of the Healthy Children, Healthy Families, Healthy Communities Program for Obesity Prevention among Vulnerable Children: A Cluster-Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2020; 17(8):2895. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082895
Chicago/Turabian StyleChoo, Jina, Hwa-Mi Yang, Sae-Young Jae, Hye-Jin Kim, Jihyun You, and Juneyoung Lee. 2020. "Effects of the Healthy Children, Healthy Families, Healthy Communities Program for Obesity Prevention among Vulnerable Children: A Cluster-Randomized Controlled Trial" International Journal of Environmental Research and Public Health 17, no. 8: 2895. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082895