Mother–Infant Co-Sleeping and Maternally Reported Infant Breathing Distress in the UK Millennium Cohort

Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Variables and Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Logistic Regression Results
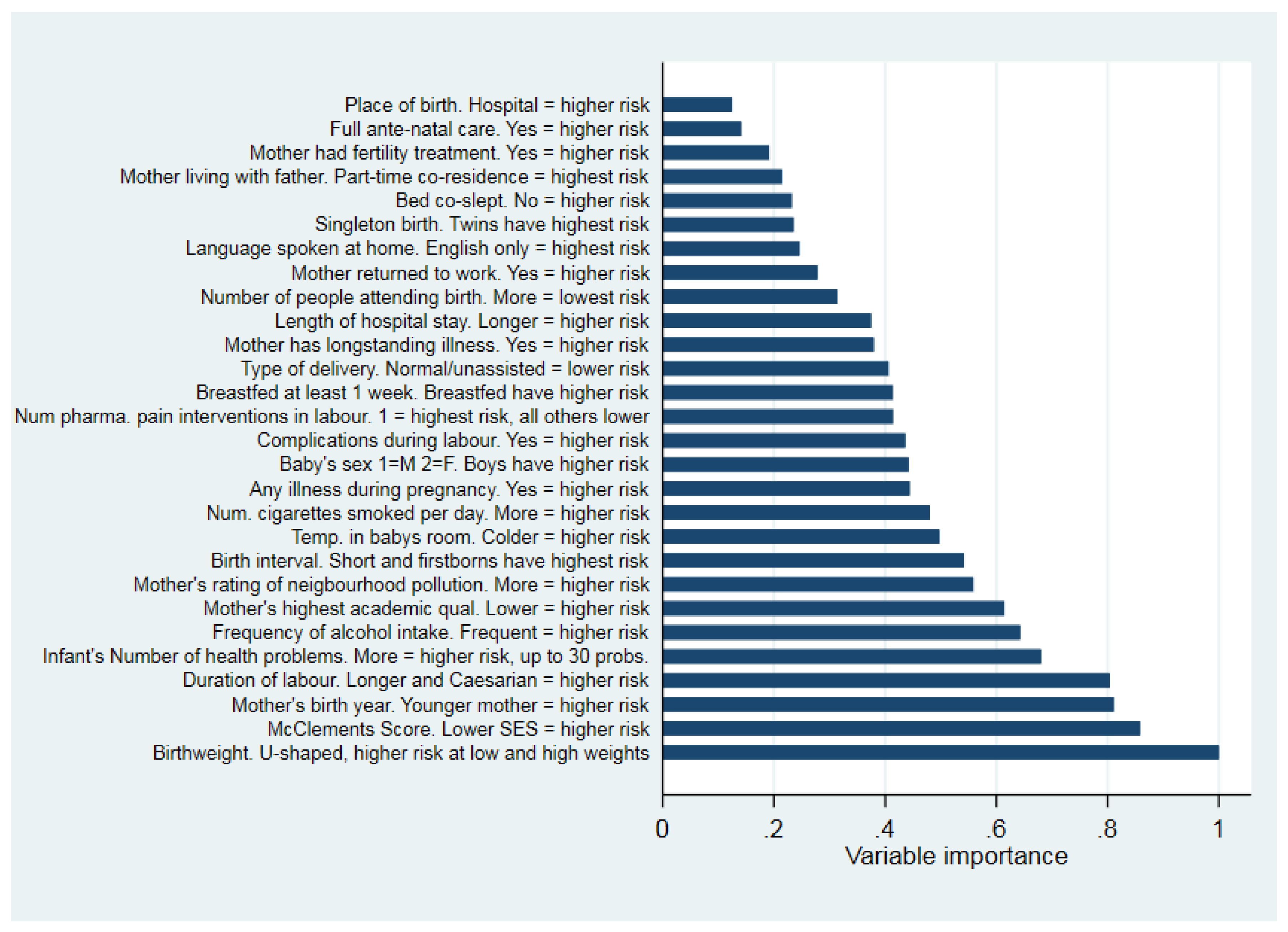
3.3. RF Results
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Conflicts of Interest
References
- Airhihenbuwa, C.; Iwelunmor, J.; Ezepue, C.; Williams, N.; Jean-Louis, G. I sleep, because we sleep: A synthesis on the role of culture in sleep behavior research. Sleep Med. 2016, 18, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Iii, H.B.; Paxson, L.M. Infancy and Early Childhood: Cross-Cultural Codes 2. Ethnology 1971, 10, 466. [Google Scholar] [CrossRef]
- Carpenter, R.; McGarvey, C.; Mitchell, E.A.; Tappin, D.M.; Vennemann, M.M.; Smuk, M.; Carpenter, J. Bed sharing when parents do not smoke: Is there a risk of SIDS? An individual level analysis of five major case–control studies. BMJ Open 2013, 3, e002299. [Google Scholar] [CrossRef] [PubMed]
- Blair, P.S.; Sidebotham, P.; Pease, A.; Fleming, P.J. Bedsharing in the absence of hazardous circumstances: Is there a risk of sudden infant death syndrome? An analysis from twocase-control studies conducted in the UK. PLoS ONE 2014, 9, e107799. [Google Scholar]
- Blair, P.; Ball, H. The prevalence and characteristics associated with parent–infant bed-sharing in England. Arch. Dis. Child. 2004, 89, 1106–1110. [Google Scholar] [CrossRef] [Green Version]
- Cole, R.; Young, J.; Kearney, L.; Thompson, J.M. Infant care practices and parent uptake of safe sleep messages: A cross-sectional survey in Queensland, Australia. BMC Pediatr. 2020, 20, 27. [Google Scholar] [CrossRef] [Green Version]
- NHS Bed-Sharing Guidelines. Available online: https://www.sth.nhs.uk/clientfiles/File/Sleep%20Safe%20inners%20%5Bweb%5D%5B1%5D.pdf (accessed on 18 March 2020).
- CDC Bed-Sharing Guidelines. Available online: https://www.cdc.gov/grand-rounds/pp/2018/20181023-sudden-infant-death.html (accessed on 18 March 2020).
- Bartick, M.; Tomori, C.; Ball, H. Babies in boxes and the missing links on safe sleep: Human evolution and cultural revolution. Matern. Child Nutr. 2017, 14, e12544. [Google Scholar] [CrossRef]
- Co-Sleeping with Your Baby: Advice from the Lullaby Trust. Available online: https://www.lullabytrust.org.uk/safer-sleep-advice/co-sleeping/ (accessed on 20 April 2020).
- Co-Sleeping and Bed-Sharing ACM Position Statement. Available online: https://www.midwives.org.au/resources/co-sleeping-and-bed-sharing-acm-position-statement-2014 (accessed on 20 April 2020).
- Ball, H.; Tomori, C.; McKenna, J.J. Toward an Integrated Anthropology of Infant Sleep. Am. Anthr. 2019, 121, 595–612. [Google Scholar] [CrossRef]
- Ball, H.L. Night-time infant care: Cultural practice, evolution, and infant development. In Childrearing and Infant Care Issues: A Cross-Cultural Perspective; Liamputtong, P., Ed.; Nova: New York, NY, USA, 2006; pp. 47–61. [Google Scholar]
- Blair, P.S.; Sidebotham, P.; Berry, P.J.; Evans, M.; Fleming, P.J. Major changes in the epidemiology of sudden infant death syndrome: A 20 year population based study of all unexpected deaths in infancy. Lancet 2006, 367, 314–319. [Google Scholar] [CrossRef] [Green Version]
- Tappin, D.; Brooke, H.; Ecob, R.; Gibson, A. Used infant mattresses and sudden infant death syndrome in Scotland: Case-control study. BMJ 2002, 325, 1007. [Google Scholar] [CrossRef] [Green Version]
- Hauck, F.R.; Herman, S.M.; Donovan, M.; Iyasu, S.; Moore, C.M.; Donoghue, E.; Kirschner, R.H.; Willinger, M. Sleep environment and the risk of sudden infant death syndrome in an urban population: The Chicago Infant Mortality Study. Pediatrics 2003, 111, 1207–1214. [Google Scholar] [PubMed]
- Beijers, R.; Riksen-Walraven, J.M.A.; De Weerth, C. Cortisol regulation in 12-month-old human infants: Associations with the infants’ early history of breastfeeding and co-sleeping. Stress 2012, 16, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Tollenaar, M.; Beijers, R.; Jansen, J.; Riksen-Walraven, J.; De Weerth, C. Solitary sleeping in young infants is associated with heightened cortisol reactivity to a bathing session but not to a vaccination. Psychoneuroendocrinology 2012, 37, 167–177. [Google Scholar] [CrossRef]
- Waynforth, D. The influence of parent-infant co-sleeping, nursing, and childcare on cortisol and SlgA immunity in a sample of British Children. Dev. Psychobiol. 2007, 49, 640–648. [Google Scholar] [CrossRef] [PubMed]
- Trevathan, W.R.; McKenna, J.J. Evolutionary environments of human birth and infancy: Insights to apply to contemporary life. Child. Environ. 1994, 11, 88–104. [Google Scholar]
- Selley, W.G.; Ellis, R.E.; Flack, F.C.; Brooks, W.A. Coordination of suckling, swallowing and breathing in the newborn: Its relationship to infant feeding and normal development. Brit. J. Disord. Commun. 1990, 25, 311–327. [Google Scholar] [CrossRef]
- Karlberg, P.; Koch, G. Respiratory studies in newborn infants III: Developmental of mechanics of breathing during the first week of life, a longitudinal study. Acta Paediatr. 1962, 51, 121–129. [Google Scholar] [CrossRef]
- Connelly, R.; Platt, L. Cohort Profile: UK Millennium Cohort Study (MCS). Int. J. Epidemiol. 2014, 43, 1719–1725. [Google Scholar] [CrossRef]
- McIntire, D.D.; Bloom, S.L.; Leveno, K.; Casey, B.M. Birth Weight in Relation to Morbidity and Mortality among Newborn Infants. N. Engl. J. Med. 1999, 340, 1234–1238. [Google Scholar] [CrossRef]
- Ketterlinus, R.D.; Henderson, S.H.; Lamb, M.E. Maternal age, sociodemographics, prenatal health and behavior: Influences on neonatal risk status. J. Adolesc. Heal. Care 1990, 11, 423–431. [Google Scholar] [CrossRef]
- Alio, A.P.; Salihu, H.M.; Kornosky, J.L.; Richman, A.M.; Marty, P.J. Feto-infant Health and Survival: Does Paternal Involvement Matter? Matern. Child Heal. J. 2009, 14, 931–937. [Google Scholar] [CrossRef]
- Anyaegbu, G. Using the OECD equivalence scale in taxes and benefits analysis. Econ. Labour Mark. Rev. 2010, 4, 49–54. [Google Scholar] [CrossRef] [Green Version]
- Nikiéma, B.; Zunzunegui, M.V.; Séguin, L.; Gauvin, L.; Potvin, L. Poverty and Cumulative Hospitalization in Infancy and Early Childhood in the Quebec Birth Cohort: A Puzzling Pattern of Association. Matern. Child Heal. J. 2007, 12, 534–544. [Google Scholar] [CrossRef] [PubMed]
- Andreev, K.F. Sex differentials in survival in the Canadian population, 1921–1997. Demogr. Res. 2000, 3, 12. [Google Scholar] [CrossRef]
- Conde-Agudelo, A.; Castaño, F.; Norton, M.H.; Rosas-Bermudez, A. Effects of Birth Spacing on Maternal, Perinatal, Infant, and Child Health: A Systematic Review of Causal Mechanisms. Stud. Fam. Plan. 2012, 43, 93–114. [Google Scholar] [CrossRef] [PubMed]
- Kalland, M.; Sinkkonen, J.; Gissler, M.V.M.; Meriläinen, J.; Siimes, M.A. Maternal smoking behavior, background and neonatal health in Finnish children subsequently placed in foster care. Child Abus. Negl. 2006, 30, 1037–1047. [Google Scholar] [CrossRef]
- Samueloff, A.; Mor-Yosef, S.; Seidman, D.S.; Adler, I.; Persitz, E.; Schenker, J.G. Ranking risk factors for perinatal mortality. Acta Obstet. Gynecol. Scand. 1989, 68, 677–682. [Google Scholar] [CrossRef]
- Ball, H.; Moya, E.; Fairley, L.; Westman, J.; Oddie, S.; Wright, J. Infant care practices related to sudden infant death syndrome in South Asian and White British families in the UK. Paediatr. Périnat. Epidemiol. 2011, 26, 3–12. [Google Scholar] [CrossRef]
- Waynforth, D. Effects of Conception Using Assisted Reproductive Technologies on Infant Health and Development: An Evolutionary Perspective and Analysis Using UK Millennium Cohort Data. Yale J. Boil. Med. 2018, 91, 225–235. [Google Scholar]
- Raisler, J.; Alexander, C.; O’Campo, P. Breast-feeding and infant illness: A dose-response relationship? Am. J. Public Heal. 1999, 89, 25–30. [Google Scholar] [CrossRef]
- Breiman, L. Random Forests. Mach. Learn 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Breiman, L. Statistical modelling: The two cultures. Stat. Sci. 2001, 16, 199–231. [Google Scholar] [CrossRef]
- Abel, S.; Tipene-Leach, D.C. SUDI prevention: A review of Maori safe sleep innovations for infants. N. Z. Med. J. 2013, 126, 86–94. [Google Scholar] [PubMed]


{kind=link}
| Variable Name | Description/Coding | Reason for Inclusion | Included in Logistic Model |
|---|---|---|---|
| Breathing distress in first week reported by parent | 0 = no, 1 = yes | Dependent variable | ✓ |
| Bed co-sleeping with a parent was main sleeping arrangement in first 9 months | 1 = no, 2 = yes | Main independent variable | ✓ |
| Breastfed at least 1 week | 1 = no, 2 = yes | (see text) | ✓ |
| Birthweight | Recorded in kg | Predicts infant health [24] | ✓ |
| Mother’s birth year | Year of birth | Studies demonstrate risk associated with young mothers [25] | ✓ |
| Father present in household | 1 = yes, 2 = part of the time, 3 = no | Associated with low maternal income and increased health risk in infants [26] | ✓ |
| Infant’s total number of illnesses reported (first 9 months) | Illnesses reported in infancy | Included to statistically control for poor general health in infancy | ✓ |
| Singleton birth, twin or triplet | 1 = singleton birth, 2 = twin, 3 = triplet | Twins and triplets have poorer health outcomes in infancy [24] | ✓ |
| Household living standard | McClement’s equivalised income [27] | Socioeconomic status predicts infant health [28] | ✓ |
| Mother’s highest qualification | 1 = highest, 6 = lowest. Qualifications which could not be coded assigned mid-value | Socioeconomic status predicts infant health [28] | ✓ |
| Infant’s sex | 1 = Male, 2 = Female | Boys have poorer health in infancy [29] | ✓ |
| Length of hospital stay after birth | Recorded as hours, days, weeks. Categorical. 1 = shortest, 3 = longest | Mothers & infants remaining in hospital will not have the same opportunities to co-sleep as those at home. | ✓ |
| Duration of labour | Recorded in hours | Plausible predictor of neonatal health | |
| Mother’s alcohol consumption | Reported after birth. 1 = most frequent, to 7 = never | Predicts some infant health conditions and unsafe co-sleeping [15,16] | |
| Mother’s report of pollution in neighbourhood | Reported on a 4-point scale, 1 = most, to 4 = least pollution | Plausible predictor of neonatal health and breathing difficulties | |
| Birth interval | Categorised into quartiles. First births coded as 5 and added to scale | Often found to be associated with infant health [30] | |
| Mother’s smoking: number of cigarettes daily | Reported after birth | Predictor of neonatal health and breathing problems [3,31] | |
| Temperature in room where baby sleeps | On a 5-point scale where 1 = warmest and 5 = cold | Plausible predictor of neonatal health | |
| Mother returned to paid work within 9 months of birth | 1 = yes, 2 = no | Plausibly interacts with co-sleeping via need for infant independence | |
| Complications during labour | 0 = no, 1 = yes | Predictor of neonatal health [32] | |
| Number of pharmacological pain interventions during labour | Recorded as the number of different pain interventions | Plausible predictor of neonatal health | |
| Normal delivery | 1 = normal, all else = 2 (including forceps, Caesarean, etc.) | Predictor of neonatal health [32] | |
| Maternal longstanding illness prior to pregnancy | 1 = yes, 2 = no. Includes all chronic illness and disability | Predictor of neonatal health [32] | |
| Maternal illness during pregnancy | 1 = yes, 2 = no | Predictor of neonatal health [32] | |
| Number of people who attended birth | Reported by mother | Measure of social support for mother and neonate | |
| Language other than English spoken at home | 1 = English only, 2 = English plus another language, 3 = Other language only | Plausibly interacts with co-sleeping [33] | |
| Infant born in hospital not home | 1 = yes, 2 = no | Plausible predictor of neonatal health if home births are typically low-risk | |
| Received full ante-natal care | 1 = yes, 2 = no | Plausible predictor of neonatal health | |
| IVF or ART pregnancy | 1 = yes, 2 = no | Predictor of neonatal health [34] |
| N | Mean | Min | Max | St.Dev | |
|---|---|---|---|---|---|
| Breathing distress in first week reported by parent | 18,552 | 0.037 | 0 | 1 | 0.189 |
| Father present in household | 18,525 | 1.115 | 1 | 3 | 0.447 |
| IVF or ART pregnancy | 18,545 | 1.974 | 1 | 2 | 0.159 |
| Maternal illness during pregnancy | 18,497 | 1.623 | 1 | 2 | 0.485 |
| Infant born in hospital not home | 18,502 | 1.021 | 1 | 2 | 0.142 |
| Normal delivery | 18,499 | 1.313 | 1 | 2 | 0.464 |
| Duration of labour (hrs) | 17,773 | 9.15 | 0 | 100 | 11.137 |
| Complications during labour | 18,552 | 0.32 | 0 | 1 | 0.466 |
| Mother’s smoking | 18,540 | 3.318 | 0 | 60 | 6.273 |
| Mother’s alcohol consumption | 18,529 | 5.133 | 1 | 7 | 1.49 |
| Mother’s report of pollution in neighbourhood | 18,315 | 3.089 | 1 | 4 | 0.892 |
| Number of pharmacological pain interventions during labour | 18,413 | 0.731 | 0 | 4 | 0.667 |
| Number of people who attended birth | 18,552 | 1.119 | 0 | 4 | 0.495 |
| Infant’s sex M = 1 F = 2 | 18,552 | 1.486 | 1 | 2 | 0.5 |
| Household equivalised income | 16,941 | 296.999 | 14 | 1251 | 227.33 |
| Maternal illness during pregnancy | 18,524 | 1.789 | 1 | 2 | 0.408 |
| Infant’s total number of illnesses reported | 18,521 | 1.633 | 0 | 50 | 1.991 |
| Mother returned to paid work within 9 months of birth | 18,542 | 1.879 | 1 | 2 | 0.327 |
| Mother’s highest qualification | 18,484 | 4.005 | 1 | 6 | 1.304 |
| Mother’s birth year | 18,549 | 1971 | 1937 | 1987 | 5.961 |
| Language other than English spoken at home | 18,552 | 1.19 | 1 | 3 | 0.481 |
| Singleton birth, twin or triplet | 18,552 | 1.014 | 1 | 3 | 0.123 |
| Bed co-sleeping with a parent | 18,531 | 1.089 | 1 | 2 | 0.285 |
| Birthweight | 18,482 | 3.344 | 0.391 | 7.229 | 0.59 |
| Breastfed at least 1 week | 18,551 | 1.536 | 1 | 2 | 0.499 |
| Length of hospital stay after birth | 18,117 | 2.046 | 1 | 3 | 0.421 |
| Received full ante-natal care | 18,492 | 1.038 | 1 | 2 | 0.191 |
| Temperature in room where baby sleeps | 18,408 | 2.301 | 1 | 5 | 0.745 |
| Birth interval | 18,527 | 3.79 | 1 | 5 | 1.461 |
| Dependent Variable: Breathing Difficulty Reported In First Week Of Infancy | Odds Ratio | St.Err. | t-Value | p-Value | 95% Confidence Intervals | Sig |
|---|---|---|---|---|---|---|
| Bed co-slept | 0.694 | 0.115 | −2.20 | 0.027 | 0.502–0.960 | ** |
| Breastfed at least 1 week | 0.974 | 0.088 | −0.30 | 0.767 | 0.815–1.162 | |
| Coslept by breastfed interaction (centred resids.) | 1.043 | 0.049 | 0.88 | 0.378 | 0.950–1.144 | |
| Mother’s birth year | 1.002 | 0.008 | 0.30 | 0.762 | 0.987–1.018 | |
| Father present in household | 0.963 | 0.113 | −0.32 | 0.747 | 0.764–1.213 | |
| Infant’s total number of reported illnesses | 1.185 | 0.039 | 5.12 | 0.000 | 1.111–1.265 | *** |
| Infant number of illnesses squared | 0.995 | 0.002 | −2.42 | 0.016 | 0.991–0.999 | ** |
| Twin or triplet | 1.290 | 0.265 | 1.24 | 0.214 | 0.863–1.928 | |
| Income (McClement’s equivalency) | 1.000 | 0.000 | −0.91 | 0.365 | 0.999–1.000 | |
| Mother’s educational qualifications | 0.962 | 0.034 | −1.09 | 0.274 | 0.897–1.031 | |
| Infant sex (1 = M 2 = F) | 0.695 | 0.060 | −4.20 | 0.000 | 0.586–0.823 | *** |
| Birthweight (kg) | 0.043 | 0.010 | −13.74 | 0.000 | 0.027–0.067 | *** |
| Birthweight squared | 1.504 | 0.058 | 10.65 | 0.000 | 1.395–1.621 | *** |
| Duration of hospital stay after birth (1 = longest, to 3 = shortest) | 0.398 | 0.039 | −9.50 | 0.000 | 0.329–0.481 | *** |
| Constant | 126.0 | 83.734 | 7.28 | 0.000 | 34.24–463.52 | *** |
| Mean dependent var: 0.037 | SD dep. var: 0.192 | |||||
| Pseudo r-squared: 0.110 | Num. obs: 16,491 | |||||
| Chi-square: 589.501 | Prob > chi2: 0.000 | |||||
| Log Likelihood −2556.144 | ||||||
| Observations Correctly Classified by Model | ||
|---|---|---|
| Logistic Regression | Random Forest | |
| Cases with breathing difficulty | 39/630 (5.87%) | 687/689 (99.7%) |
| Cases without breathing difficulty | 15,836/15,861 (99.84%) | 17,863/17,863 (100%) |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waynforth, D. Mother–Infant Co-Sleeping and Maternally Reported Infant Breathing Distress in the UK Millennium Cohort. Int. J. Environ. Res. Public Health 2020, 17, 2985. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17092985
Waynforth D. Mother–Infant Co-Sleeping and Maternally Reported Infant Breathing Distress in the UK Millennium Cohort. International Journal of Environmental Research and Public Health. 2020; 17(9):2985. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17092985
Chicago/Turabian StyleWaynforth, David. 2020. "Mother–Infant Co-Sleeping and Maternally Reported Infant Breathing Distress in the UK Millennium Cohort" International Journal of Environmental Research and Public Health 17, no. 9: 2985. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17092985