Hyperacusis in Children with Attention Deficit Hyperactivity Disorder: A Preliminary Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Diagnosis of Attention Deficit Hyperactivity Disorder
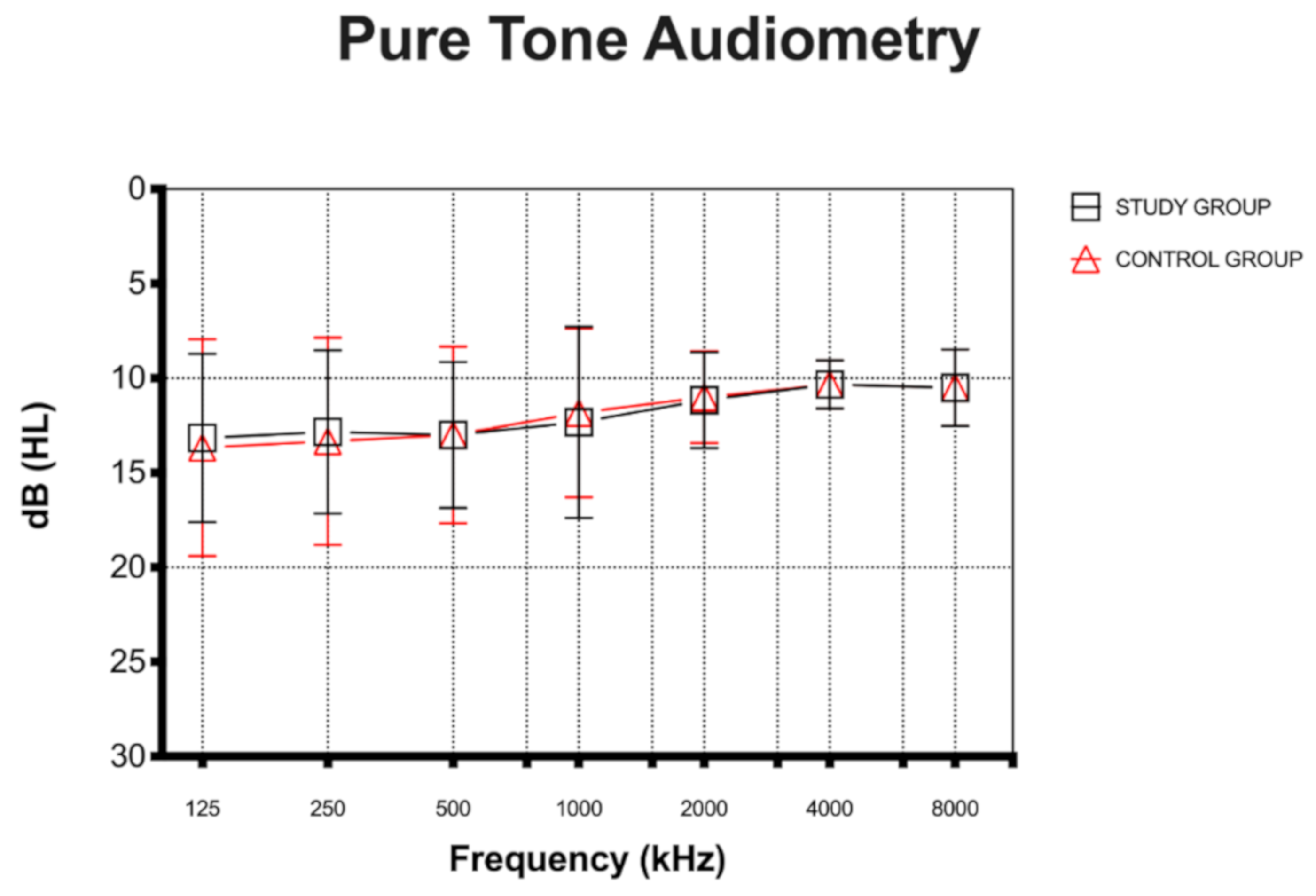
2.3. Auditory Evaluation
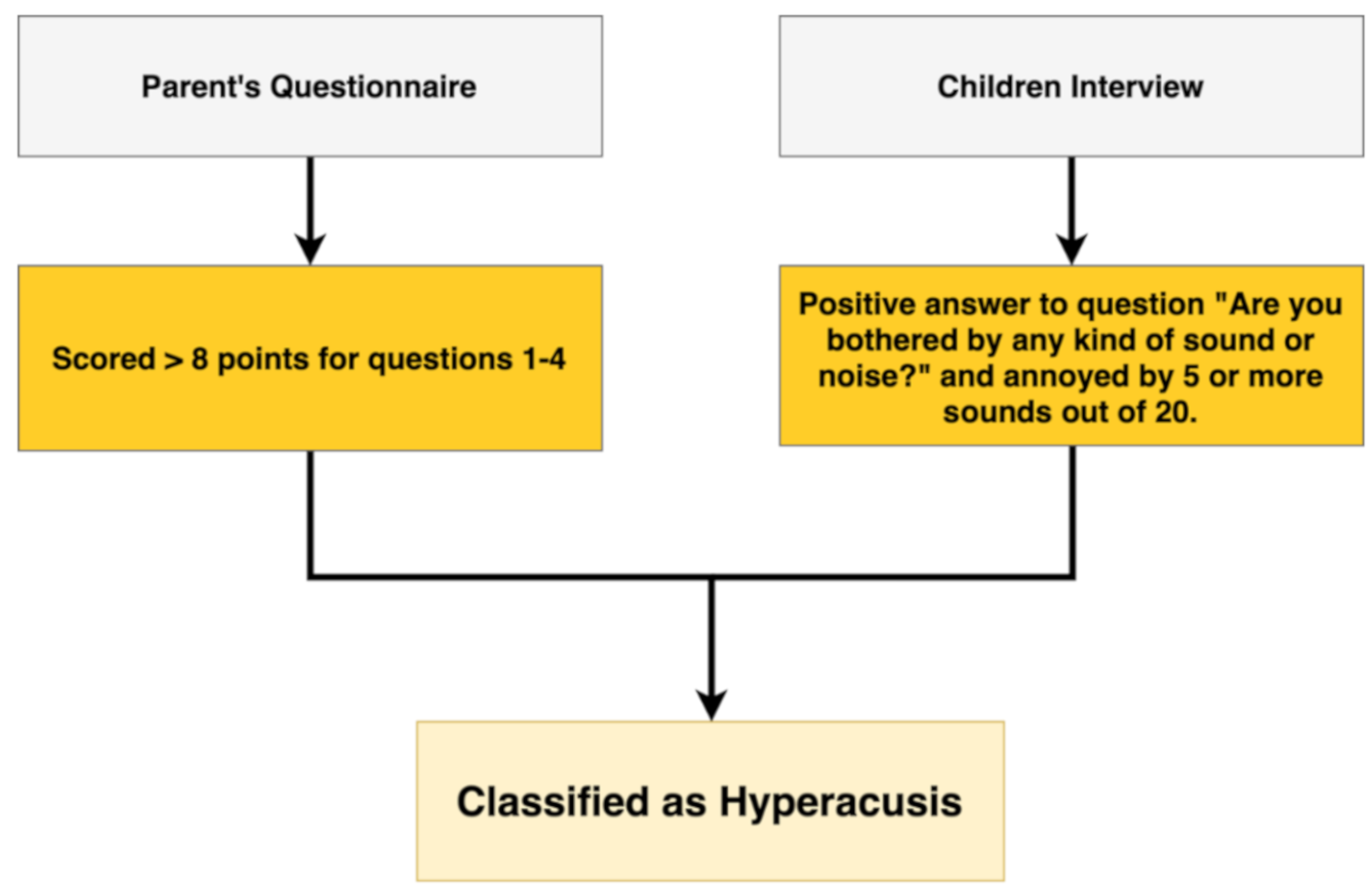
2.4. Diagnosis of Hyperacusis
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
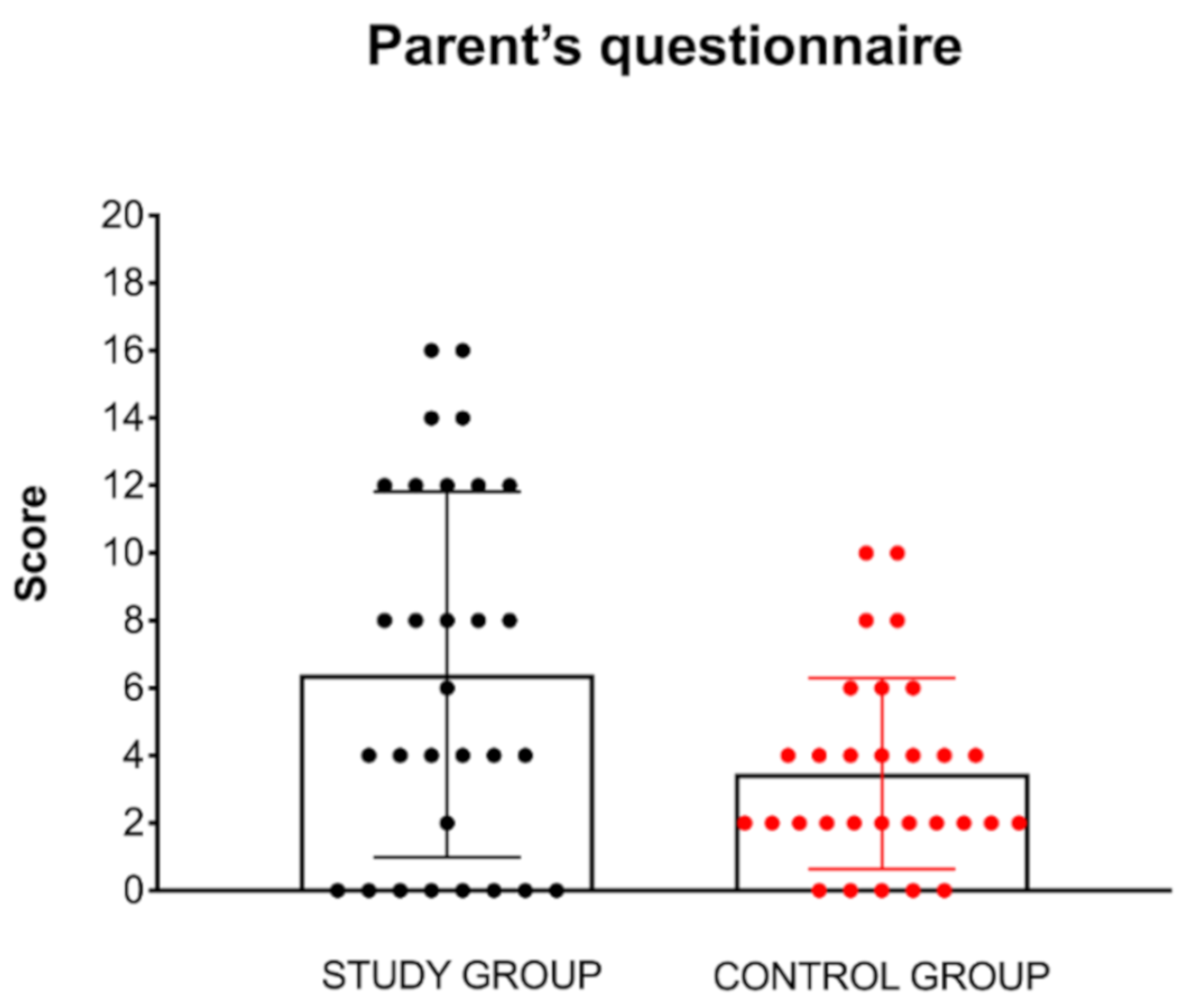
3.2. Parent’s Questionnaire
3.3. Children’s Interview
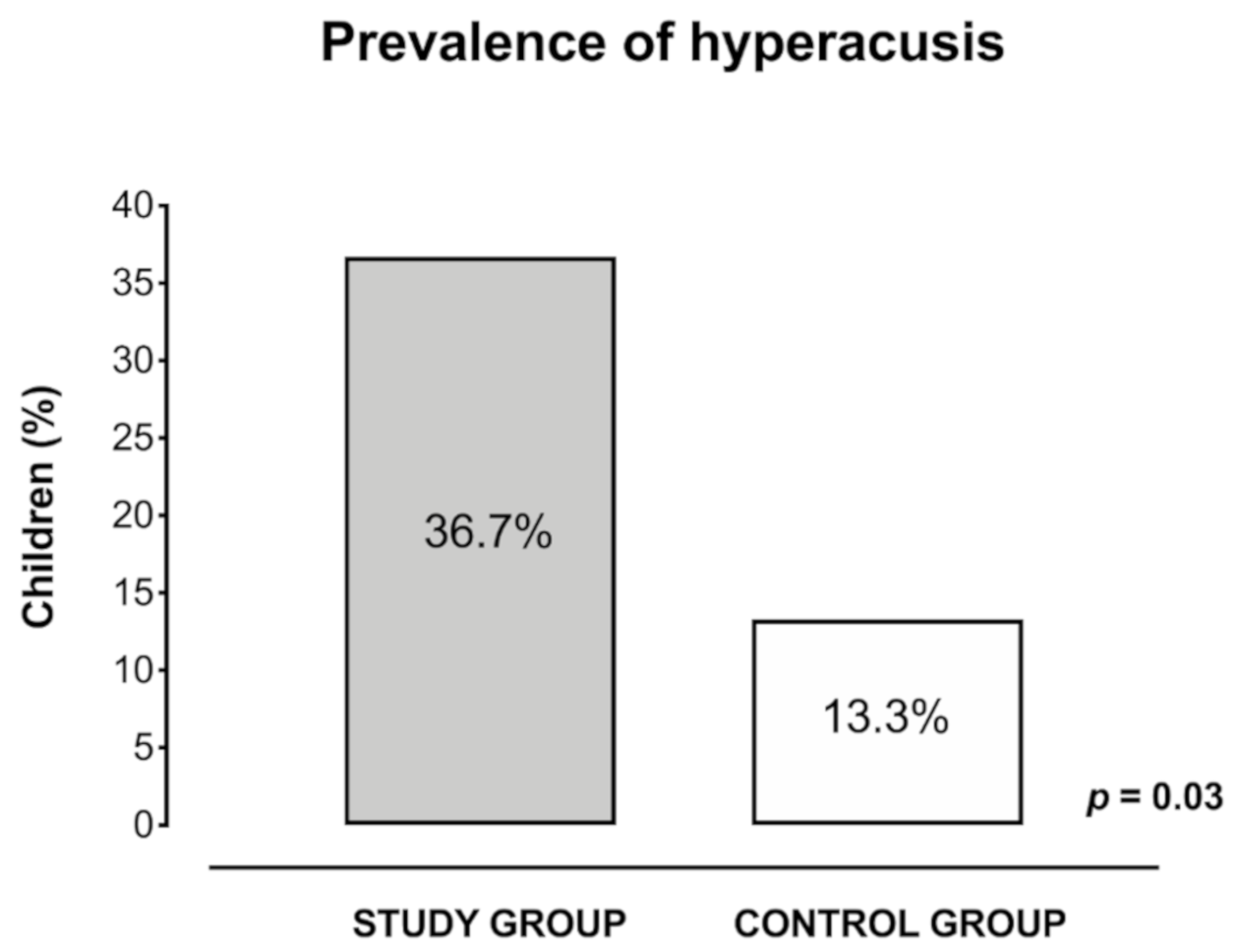
3.4. Prevalence of Hyperacusis
4. Discussion
Limits of Our Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Aazh, H.; McFerran, D.; Salvi, R.; Prasher, D.; Jastreboff, M.; Jastreboff, P. Insights from the First International Conference on Hyperacusis: Causes, evaluation, diagnosis and treatment. Noise Health 2014, 16, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Li, X.; Liu, L.; Wang, J.; Lu, C.Q.; Yang, M.; Jiao, Y.; Zang, F.C.; Radziwon, K.; Chen, G.D.; et al. Tinnitus and hyperacusis involve hyperactivity and enhanced connectivity in auditory-limbic-arousal-cerebellar network. eLife 2015, 4, e06576. [Google Scholar] [CrossRef] [PubMed]
- Middleton, J.W.; Tzounopoulos, T. Imaging the neural correlates of tinnitus: A comparison between animal models and human studies. Front. Syst. Neurosci. 2012, 6, 35. [Google Scholar] [CrossRef] [Green Version]
- Auerbach, B.D.; Rodrigues, P.V.; Salvi, R.J. Central gain control in tinnitus and hyperacusis. Front. Neurol. 2014, 5, 206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baguley, D.M. Hyperacusis. J. R. Soc. Med. 2003, 96, 582–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katzenell, U.; Segal, S. Hyperacusis: Review and clinical guidelines. Otol. Neurotol. 2001, 22, 321–327. [Google Scholar] [CrossRef]
- Tyler, R.S.; Pienkowski, M.; Roncancio, E.R.; Jun, H.J.; Brozoski, T.; Dauman, N.; Dauman, N.; Andersson, G.; Keiner, A.J.; Cacace, A.T.; et al. A review of hyperacusis and future directions: Part I. Definitions and manifestations. Am. J. Audiol. 2014, 23, 402–419. [Google Scholar] [CrossRef] [Green Version]
- Ralli, M.; Salvi, R.J.; Greco, A.; Turchetta, R.; De Virgilio, A.; Altissimi, G.; Attanasio, G.; Cianfrone, G.; de Vincentiis, M. Characteristics of somatic tinnitus patients with and without hyperacusis. PLoS ONE 2017, 12, e0188255. [Google Scholar] [CrossRef] [Green Version]
- Hwang, J.H.; Chou, P.H.; Wu, C.W.; Chen, J.H.; Liu, T.C. Brain activation in patients with idiopathic hyperacusis. Am. J. Otolaryngol. 2009, 30, 432–434. [Google Scholar] [CrossRef]
- Veuillet, E.; Khalfa, S.; Collet, L. Clinical relevance of medial efferent auditory pathways. Scand. Audiol. Suppl. 1999, 51, 53–62. [Google Scholar]
- Ralli, M.; Greco, A.; Altissimi, G.; Tagliaferri, N.; Carchiolo, L.; Turchetta, R.; Fusconi, M.; Polimeni, A.; Cianfrone, G.; Vincentiis, M. Hyperacusis in Children: A Preliminary Study on the Effects of Hypersensitivity to Sound on Speech and Language. Int. Tinnitus J. 2018, 22, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Amir, I.; Lamerton, D.; Montague, M.L. Hyperacusis in children: The Edinburgh experience. Int. J. Pediatr. Otorhinolaryngol. 2018, 112, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Coelho, C.B.; Sanchez, T.G.; Tyler, R.S. Hyperacusis, sound annoyance, and loudness hypersensitivity in children. Prog. Brain. Res. 2007, 166, 169–178. [Google Scholar]
- Nemholt, S.S.; Schmidt, J.H.; Wedderkopp, N.; Baguley, D.M. Prevalence of tinnitus and/or hyperacusis in children and adolescents: Study protocol for a systematic review. BMJ Open 2015, 5, e006649. [Google Scholar] [CrossRef]
- Paulin, J.; Andersson, L.; Nordin, S. Characteristics of hyperacusis in the general population. Noise Health 2016, 18, 178–184. [Google Scholar] [CrossRef]
- Hall, A.J.; Humphriss, R.; Baguley, D.M.; Parker, M.; Steer, C.D. Prevalence and risk factors for reduced sound tolerance (hyperacusis) in children. Int. J. Audiol. 2016, 55, 135–141. [Google Scholar] [CrossRef]
- Elsabbagh, M.; Cohen, H.; Cohen, M.; Rosen, S.; Karmiloff-Smith, A. Severity of hyperacusis predicts individual differences in speech perception in Williams Syndrome. J. Intellect. Disabil. Res. 2011, 55, 563–571. [Google Scholar] [CrossRef] [PubMed]
- Carvalho Ade, J.; Lemos, S.M.; Goulart, L.M. Language development and its relation to social behavior and family and school environments: A systematic review. CoDAS 2016, 28, 470–479. [Google Scholar] [PubMed]
- Barkley, R.A.; Brown, T.E. Unrecognized attention-deficit/hyperactivity disorder in adults presenting with other psychiatric disorders. CNS Spectr. 2008, 13, 977–984. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Adler, L.; Barkley, R.; Biederman, J.; Conners, C.K.; Demler, O.; Faraone, S.V.; Greenhill, L.L.; Howes, M.J.; Secnik, K.; et al. The prevalence and correlates of adult ADHD in the United States: Results from the National Comorbidity Survey Replication. Am. J. Psychiatry 2006, 163, 716–723. [Google Scholar] [CrossRef]
- Thomas, R.; Sanders, S.; Doust, J.; Beller, E.; Glasziou, P. Prevalence of attention-deficit/hyperactivity disorder: A systematic review and meta-analysis. J. Pediatrics 2015, 135, e994–e1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fayyad, J.; De Graaf, R.; Kessler, R.; Alonso, J.; Angermeyer, M.; Demyttenaere, K.; De Girolamo, G.; Haro, J.M.; Karam, E.G.; Lara, C.; et al. Cross-national prevalence and correlates of adult attention-deficit hyperactivity disorder. Br. J. Psychiatry 2007, 190, 402–409. [Google Scholar] [CrossRef] [Green Version]
- Faraone, S.V.; Sergeant, J.; Gillberg, C.; Biederman, J. The worldwide prevalence of ADHD: Is it an American condition? World Psychiatry 2003, 2, 104–113. [Google Scholar] [PubMed]
- Salmeron, P.A. Childhood and adolescent attention-deficit hyperactivity disorder: Diagnosis, clinical practice guidelines, and social implications. J. Am. Acad. Nurse Pract. 2009, 21, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Adler, L.A. Diagnosing and treating adult ADHD and comorbid conditions. J. Clin. Psychiatry 2008, 69, e31. [Google Scholar] [CrossRef]
- Biederman, J.; Faraone, S.V.; Spencer, T.; Wilens, T.; Norman, D.; Lapey, K.A.; Mick, E.; Lehman, B.K.; Doyle, A. Patterns of psychiatric comorbidity, cognition, and psychosocial functioning in adults with attention deficit hyperactivity disorder. Am. J. Psychiatry 1993, 150, 1792–1798. [Google Scholar]
- Fuermaier, A.B.M.; Hupen, P.; De Vries, S.M.; Muller, M.; Kok, F.M.; Koerts, J.; Heutink, J.; Tucha, L.; Gerlach, M.; Tucha, O. Perception in attention deficit hyperactivity disorder. Atten. Defic. Hyperact. Disord. 2018, 10, 21–47. [Google Scholar] [CrossRef]
- Kaat, A.J.; Gadow, K.D.; Lecavalier, L. Psychiatric symptom impairment in children with autism spectrum disorders. J. Abnorm. Child. Psychol. 2013, 41, 959–969. [Google Scholar] [CrossRef]
- Jensen, C.M.; Steinhausen, H.C. Comorbid mental disorders in children and adolescents with attention-deficit/hyperactivity disorder in a large nationwide study. Atten. Defic. Hyperact. Disord. 2015, 7, 27–38. [Google Scholar] [CrossRef]
- Thapar, A. Discoveries on the Genetics of ADHD in the 21st Century: New Findings and Their Implications. Am. J. Psychiatry 2018, 175, 943–950. [Google Scholar] [CrossRef] [Green Version]
- Rosing, S.N.; Schmidt, J.H.; Wedderkopp, N.; Baguley, D.M. Prevalence of tinnitus and hyperacusis in children and adolescents: A systematic review. BMJ Open 2016, 6, e010596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, L.B.; Comeau, M.; Clarke, K.D. Hyperacusis in Williams syndrome. J. Otolaryngol. 2001, 30, 90–92. [Google Scholar] [CrossRef] [PubMed]
- Myne, S.; Kennedy, V. Hyperacusis in children: A clinical profile. Int. J. Pediatr. Otorhinolaryngol. 2018, 107, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Klein, A.J.; Armstrong, B.L.; Greer, M.K.; Brown, F.R., III. Hyperacusis and otitis media in individuals with Williams syndrome. J. Speech Hear. Disord. 1990, 55, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Thabet, E.M.; Zaghloul, H.S. Auditory profile and high resolution CT scan in autism spectrum disorders children with auditory hypersensitivity. Eur. Arch. Otorhinolaryngol. 2013, 270, 2353–2358. [Google Scholar] [CrossRef]
- Wilson, U.S.; Sadler, K.M.; Hancock, K.E.; Guinan, J.J., Jr.; Lichtenhan, J.T. Efferent inhibition strength is a physiological correlate of hyperacusis in children with autism spectrum disorder. J. Neurophysiol. 2017, 118, 1164–1172. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Otolaryngology and the American Council of Otolaryngology. Guide for the evaluation of hearing handicap. JAMA 1979, 241, 2055–2059. [Google Scholar] [CrossRef]
- Posner, J.; Polanczyk, G.V.; Sonuga-Barke, E. Attention-deficit hyperactivity disorder. Lancet 2020, 395, 450–462. [Google Scholar] [CrossRef]
- Ida-Eto, M.; Hara, N.; Ohkawara, T.; Narita, M. Mechanism of auditory hypersensitivity in human autism using autism model rats. Pediatr. Int. 2017, 59, 404–407. [Google Scholar] [CrossRef]
- Khalfa, S.; Bruneau, N.; Roge, B.; Georgieff, N.; Veuillet, E.; Adrien, J.L.; Barthelemy, C.; Collet, L. Increased perception of loudness in autism. Hear. Res. 2004, 198, 87–92. [Google Scholar] [CrossRef]
- Aazh, H.; Knipper, M.; Danesh, A.A.; Cavanna, A.E.; Andersson, L.; Paulin, J.; Schecklmann, M.; Heinonen-Guzejev, M.; Moore, B.C.J. Insights from the third international conference on hyperacusis: Causes, evaluation, diagnosis, and treatment. Noise Health 2018, 20, 162–170. [Google Scholar] [PubMed]
- Danesh, A.A.; Lang, D.; Kaf, W.; Andreassen, W.D.; Scott, J.; Eshraghi, A.A. Tinnitus and hyperacusis in autism spectrum disorders with emphasis on high functioning individuals diagnosed with Asperger’s Syndrome. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1683–1688. [Google Scholar] [CrossRef] [PubMed]
- Matson, J.L.; Rieske, R.D.; Williams, L.W. The relationship between autism spectrum disorders and attention-deficit/hyperactivity disorder: An overview. Res. Dev. Disabil. 2013, 34, 2475–2484. [Google Scholar] [CrossRef] [PubMed]
- Roberts, L.E.; Salvi, R. Overview: Hearing loss, tinnitus, hyperacusis, and the role of central gain. Neuroscience 2019, 407, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Aazh, H.; McFerran, D.; Moore, B.C.J. Uncomfortable loudness levels among children and adolescents seeking help for tinnitus and/or hyperacusis. Int. J. Audiol. 2018, 57, 618–623. [Google Scholar] [CrossRef]
- Moller, A.R.; Salvi, R.; De Ridder, D.; Kleinjung, T.; Vanneste, S. Pathology of Tinnitus and Hyperacusis-Clinical Implications. Biomed. Res. Int. 2015, 2015, 608437. [Google Scholar] [CrossRef]
- Jastreboff, P.J.; Jastreboff, M.M. Decreased sound tolerance: Hyperacusis, misophonia, diplacousis, and polyacousis. Handb. Clin. Neurol. 2015, 129, 375–387. [Google Scholar]
- Sedley, W. Tinnitus: Does Gain Explain? Neuroscience 2019, 407, 213–228. [Google Scholar] [CrossRef]
- Brotherton, H.; Plack, C.J.; Maslin, M.; Schaette, R.; Munro, K.J. Pump up the volume: Could excessive neural gain explain tinnitus and hyperacusis? Audiol. Neurootol. 2015, 20, 273–282. [Google Scholar] [CrossRef]
- Chemali, Z.; Nehme, R.; Fricchione, G. Sensory neurologic disorders: Tinnitus. Handb. Clin. Neurol. 2019, 165, 365–381. [Google Scholar]
- Jones, E.J.H.; Dawson, G.; Webb, S.J. Sensory hypersensitivity predicts enhanced attention capture by faces in the early development of ASD. Dev. Cogn. Neurosci. 2018, 29, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takarae, Y.; Sablich, S.R.; White, S.P.; Sweeney, J.A. Neurophysiological hyperresponsivity to sensory input in autism spectrum disorders. J. Neurodev. Disord. 2016, 8, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panagopoulos, V.N.; Greene, D.J.; Campbell, M.C.; Black, K.J. Towards objectively quantifying sensory hypersensitivity: A pilot study of the “Ariana effect”. PeerJ 2013, 1, e121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghanizadeh, A. Tactile sensory dysfunction in children with ADHD. Behav. Neurol. 2008, 20, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.J.; Anzalone, M.E.; Lane, S.J.; Cermak, S.A.; Osten, E.T. Concept evolution in sensory integration: A proposed nosology for diagnosis. Am. J. Occup. Ther. 2007, 61, 135–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomchek, S.D.; Dunn, W. Sensory processing in children with and without autism: A comparative study using the short sensory profile. Am. J. Occup. Ther. 2007, 61, 190–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yochman, A.; Ornoy, A.; Parush, S. Co-occurrence of developmental delays among preschool children with attention-deficit-hyperactivity disorder. Dev. Med. Child. Neurol. 2006, 48, 483–488. [Google Scholar] [CrossRef]
- Rogers, S.J.; Hepburn, S.; Wehner, E. Parent reports of sensory symptoms in toddlers with autism and those with other developmental disorders. J. Autism Dev. Disord. 2003, 33, 631–642. [Google Scholar] [CrossRef]
- Dunn, W.; Myles, B.S.; Orr, S. Sensory processing issues associated with Asperger syndrome: A preliminary investigation. Am. J. Occup. Ther. 2002, 56, 97–102. [Google Scholar] [CrossRef] [Green Version]
- Mangeot, S.D.; Miller, L.J.; McIntosh, D.N.; McGrath-Clarke, J.; Simon, J.; Hagerman, R.J.; Goldson, E. Sensory modulation dysfunction in children with attention-deficit-hyperactivity disorder. Dev. Med. Child. Neurol. 2001, 43, 399–406. [Google Scholar] [CrossRef] [Green Version]
- Moller, A.R.; Rollins, P.R. The non-classical auditory pathways are involved in hearing in children but not in adults. Neurosci. Lett. 2002, 319, 41–44. [Google Scholar] [CrossRef]
- Gibson, B.S.; Healey, M.K.; Gondoli, D.M. ADHD reflects impaired externally directed and enhanced internally directed attention in the immediate free-recall task. J. Abnorm. Psychol. 2019, 128, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.Y.; Hsieh, H.C.; Lee, P.; Hong, F.Y.; Chang, W.D.; Liu, K.C. Auditory and Visual Attention Performance in Children With ADHD: The Attentional Deficiency of ADHD Is Modality Specific. J. Atten. Disord. 2017, 21, 856–864. [Google Scholar] [CrossRef]
- McAvinue, L.P.; Vangkilde, S.; Johnson, K.A.; Habekost, T.; Kyllingsbaek, S.; Bundesen, C.; Robertson, I.H. A Componential Analysis of Visual Attention in Children With ADHD. J. Atten. Disord. 2015, 19, 882–894. [Google Scholar] [CrossRef] [PubMed]
- Capri, T.; Santoddi, E.; Fabio, R.A. Multi-Source Interference Task paradigm to enhance automatic and controlled processes in ADHD. Res. Dev. Disabil. 2020, 97, 103542. [Google Scholar] [CrossRef] [PubMed]
- Fabio, R.A.; Castriciano, C.; Rondanini, A. ADHD: Auditory and Visual Stimuli in Automatic and Controlled Processes. J. Atten. Disord. 2015, 19, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Sheldrake, J.; Diehl, P.U.; Schaette, R. Audiometric characteristics of hyperacusis patients. Front. Neurol. 2015, 6, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Answer the Following Questions | |
|---|---|
| 1. | Do you think that your child is too sensitive to every day’s sounds? |
| 2. | Is there any sound that your child dislikes? |
| 3. | Is there any sound that your child considers painful? |
| 4. | Is there any sound that scares your child? |
| Indicate Your Child’s Most Frequent Reaction to Loud Sounds | |
| 5. | Cover ears |
| 6. | Cries |
| 7. | Escapes from sound |
| 8. | Steps back to avoid sound |
| 9. | Says “I don’t like it” or “It hurts” |
| 10. | Other |
| Answer the Following Questions | ||||
|---|---|---|---|---|
| 1. | Can you hear well? | |||
| 2. | Do you hear a noise inside your ears or head? | |||
| 3. | Are you bothered by any kind of sound or noise? | |||
| Do any of the Following Sounds Annoy you? | ||||
| School recess | TV | Car | Toys | Firecrackers |
| Classroom noise | Radio | Motorcycle | Balloons | Bombs |
| Screams | Mixer | Truck | Whistle | Thunder |
| School bell | Telephone | Ambulance | Musical instruments | Dogs |
| Are You Annoyed by “…” | Number of Children that Considered the Sound Annoying | |
|---|---|---|
| Study Group (n = 30) | Control Group (n = 30) | |
| School recess | 10 (33.3%) | 4 (13.3%) |
| Classroom noise | 16 (53.3%) | 6 (20%) |
| Screams | 16 (53.3%) | 8 (26.7%) |
| School bell | 11 (36.7%) | 6 (20%) |
| TV | 3 (10%) | 3 (10%) |
| Radio | 3 (10%) | 1 (3.3%) |
| Mixer | 8 (26.7%) | 4 (13.3%) |
| Telephone | 2 (6.7%) | 1 (3.3%) |
| Car | 5 (16.7%) | 3 (10%) |
| Motorcycle | 6 (20%) | 4 (13.3%) |
| Truck | 5 (16–7%) | 3 (10%) |
| Ambulance | 4 (13.3%) | 2 (6.7%) |
| Toys | 6 (20%) | 3 (10%) |
| Balloons | 10 (33.3%) | 5 (16.7%) |
| Whistle | 8 (26.7%) | 4 (13.3%) |
| Musical instruments | 8 (26.7%) | 4 (13.3%) |
| Bombs | 13 (43.3%) | 7 (23.3%) |
| Firecrackers | 9 (30%) | 6 (20%) |
| Thunders | 10 (33.3%) | 8 (26.7%) |
| Dogs | 8 (26.7%) | 4 (13.3%) |
| ID # | Study Group | ID# | Control Group | ||||
|---|---|---|---|---|---|---|---|
| Parent’s Questionnaire | Children’s Interview | Bothered by Sounds (Y/N) | Parent’s Questionnaire | Children’s Interview | Bothered by Sounds (Y/N) | ||
| 1 * | 14 | 11 | Y | 31 | 4 | 2 | N |
| 2 * | 16 | 7 | Y | 32 | 2 | 3 | N |
| 3 | 0 | 1 | Y | 33 | 0 | 3 | N |
| 4 | 0 | 0 | N | 34 | 4 | 3 | N |
| 5 | 4 | 10 | Y | 35 | 2 | 3 | N |
| 6 * | 8 | 5 | Y | 36 | 4 | 2 | Y |
| 7 * | 12 | 7 | Y | 37 | 4 | 4 | N |
| 8 | 0 | 7 | Y | 38 * | 8 | 6 | Y |
| 9 | 2 | 0 | Y | 39 | 0 | 1 | N |
| 10 * | 16 | 11 | Y | 40 | 2 | 5 | N |
| 11 * | 9 | 5 | Y | 41 | 6 | 0 | N |
| 12 | 12 | 3 | Y | 42 | 6 | 1 | N |
| 13 | 0 | 2 | N | 43 | 2 | 2 | N |
| 14 * | 12 | 8 | Y | 44 | 0 | 0 | N |
| 15 | 0 | 5 | Y | 45 | 4 | 2 | N |
| 16 | 4 | 7 | Y | 46 | 2 | 0 | N |
| 17 | 0 | 1 | N | 47 | 2 | 2 | N |
| 18 | 8 | 4 | Y | 48 * | 10 | 5 | Y |
| 19 | 0 | 2 | N | 49 | 0 | 1 | N |
| 20 | 4 | 5 | Y | 50 | 2 | 0 | N |
| 21 * | 12 | 11 | Y | 51 | 2 | 4 | N |
| 22 | 4 | 3 | Y | 52 | 6 | 1 | N |
| 23 * | 14 | 7 | Y | 53 | 4 | 3 | Y |
| 24 | 6 | 0 | N | 54 | 4 | 0 | N |
| 25 | 0 | 4 | Y | 55 * | 10 | 8 | Y |
| 26 * | 9 | 6 | Y | 56 | 2 | 6 | Y |
| 27 | 4 | 5 | Y | 57 | 2 | 3 | N |
| 28 * | 12 | 11 | Y | 58 | 2 | 6 | N |
| 29 | 4 | 3 | Y | 59 * | 8 | 6 | Y |
| 30 | 8 | 4 | Y | 60 | 0 | 5 | N |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ralli, M.; Romani, M.; Zodda, A.; Russo, F.Y.; Altissimi, G.; Orlando, M.P.; Cammeresi, M.G.; Penge, R.; Turchetta, R. Hyperacusis in Children with Attention Deficit Hyperactivity Disorder: A Preliminary Study. Int. J. Environ. Res. Public Health 2020, 17, 3045. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093045
Ralli M, Romani M, Zodda A, Russo FY, Altissimi G, Orlando MP, Cammeresi MG, Penge R, Turchetta R. Hyperacusis in Children with Attention Deficit Hyperactivity Disorder: A Preliminary Study. International Journal of Environmental Research and Public Health. 2020; 17(9):3045. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093045
Chicago/Turabian StyleRalli, Massimo, Maria Romani, Alessio Zodda, Francesca Yoshie Russo, Giancarlo Altissimi, Maria Patrizia Orlando, Maria Gloria Cammeresi, Roberta Penge, and Rosaria Turchetta. 2020. "Hyperacusis in Children with Attention Deficit Hyperactivity Disorder: A Preliminary Study" International Journal of Environmental Research and Public Health 17, no. 9: 3045. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093045