Ultrasonic Assessment of Optic Nerve Sheath Diameter in Patients at Risk of Sepsis-Associated Brain Dysfunction: A Preliminary Report



Abstract
:1. Introduction
2. Materials and Methods
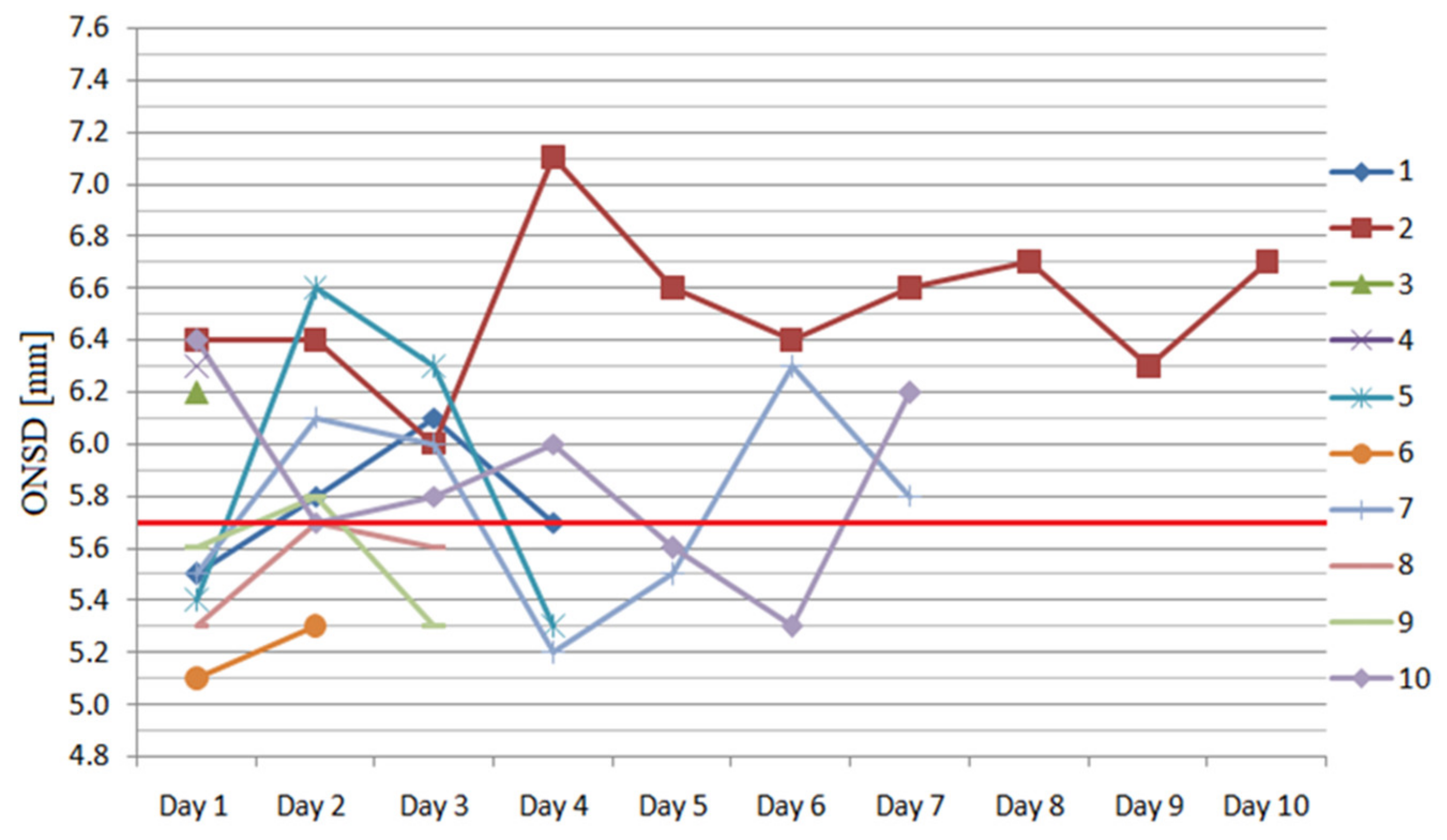
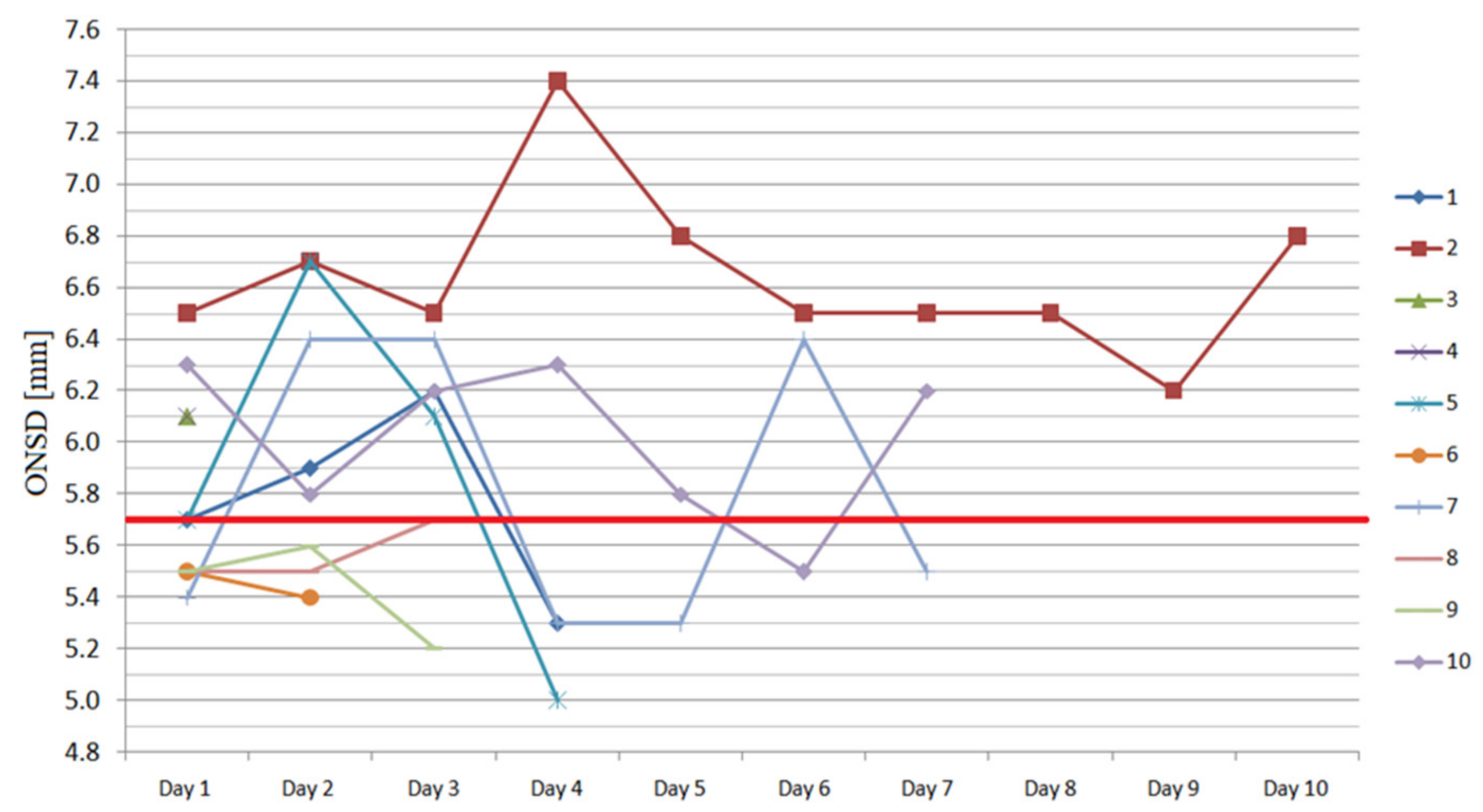
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lang, E.W.; Chesnut, R.M. Intracranial pressure. Monitoring and management. Neurosurg. Clin. N. Am. 1994, 5, 573–605. [Google Scholar] [CrossRef]
- Chacko, J. Optic nerve sheath diameter: An ultrasonographic window to view raised intracranial pressure? Indian J. Crit. Care Med. 2014, 18, 707–708. [Google Scholar] [CrossRef] [Green Version]
- Kavi, T.; Gupta, A.; Hunter, K.; Schreiber, C.; Shaikh, H.; Turtz, A.R. Optic Nerve Sheath Diameter Assessment in Patients with Intracranial Pressure Monitoring. Cureus 2018, 10, e3546. [Google Scholar] [CrossRef] [Green Version]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of Clinical Criteria for Sepsis. JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Gofton, T.E.; Young, G.B. Sepsis-associated encephalopathy. Nat. Rev. Neurol. 2012, 8, 557–566. [Google Scholar] [CrossRef]
- Bolton, C.F.; Young, G.B. Managing the nervous system effects of sepsis. Chest 2007, 131, 1273–1274. [Google Scholar] [CrossRef]
- Heming, N.; Mazeraud, A.; Verdonck, F.; Bozza, F.A.; Chrétien, F.C.; Sharshar, T. Neuroanatomy of sepsis-associated encephalopathy. Crit. Care 2017, 21, 65. [Google Scholar] [CrossRef] [Green Version]
- Crippa, I.A.; Subirà, C.; Vincent, J.-L.; Fernandez, R.; Hernandez, S.C.; Cavicchi, F.Z.; Creteur, J.; Taccone, F.S. Impaired cerebral autoregulation is associated with brain dysfunction in patients with sepsis. Crit. Care 2018, 22, 327. [Google Scholar] [CrossRef] [Green Version]
- Pfister, D.; Siegemund, M.; Dell-Kuster, S.; Smieleweski, P.; Rüegg, S.; Strebel, S.P.; Marsch, S.C.; Pargger, H.; A Steiner, L. Cerebral perfusion in sepsis-associated delirium. Crit. Care 2008, 12, R63. [Google Scholar] [CrossRef] [Green Version]
- Pfister, D.; Schmidt, B.; Smieleweski, P.; Siegemund, M.; Strebel, S.P.; Rüegg, S.; Marsch, S.C.U.; Pargger, H.; A Steiner, L. Intracranial pressure in patients with sepsis. Acta Neurochir. Suppl. 2008, 102, 71–75. [Google Scholar] [PubMed]
- Salahuddin, N.; Mohamed, A.; Alharbi, N.; Ansari, H.; Zaza, K.J.; Marashly, Q.; Hussain, I.; Solaiman, O.; Wetterberg, T.V.; Maghrabi, K. The incidence of increased ICP in ICU patients with non-traumatic coma as diagnosed by ONSD and CT: A prospective cohort study. BMC Anesthesiol. 2016, 16, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.J.; Yao, Y.; Feng, L.S.; Wang, Y.Z.; Zheng, N.N.; Feng, J.C.; Xing, Y.Q. Non-invasive and quantitative intracranial pressure estimation using ultrasonographic measurement of optic nerve sheath diameter. Sci. Rep. 2017, 7, 42063. [Google Scholar] [CrossRef] [PubMed]
- Robba, C.; Bragazzi, N.L.; Bertuccio, A.; Cardim, D.; Donnelly, J.; Sekhon, M.; Lavinio, A.; Duane, D.; Burnstein, R.; Matta, B.; et al. Effects of Prone Position and Positive End-Expiratory Pressure on Non-invasive Estimators of ICP: A Pilot Study. J. Neurosurg. Anesth. 2017, 29, 243–250. [Google Scholar] [CrossRef] [Green Version]
- Toms, D.A. The mechanical index, ultrasound practices, and the ALARA principle. J. Ultrasound Med. 2006, 25, 560–561. [Google Scholar]
- The Safety Group of the British Medical Ultrasound Society. Guidelines for the safe use of diagnostic ultrasound equipment. Ultrasound 2010, 18, 52–59. [Google Scholar] [CrossRef]
- Weidner, N.; Bomberg, H.; Antes, S.; Meiser, A.; Volk, T.; Groesdonk, H. Real-time evaluation of optic nerve sheath diameter (ONSD) in awake neurosurgical patients. Intensiv. Care Med. Exp. 2015, 3, A608. [Google Scholar] [CrossRef] [Green Version]
- Kim, N.H.; Jun, J.-S.; Kim, R. Ultrasonographic measurement of the optic nerve sheath diameter and its association with eyeball transverse diameter in 585 healthy volunteers. Sci. Rep. 2017, 7, 15906. [Google Scholar] [CrossRef]
- Lee, S.U.; Jeon, J.P.; Lee, H.; Han, J.H.; Seo, M.; Byoun, H.S.; Cho, W.-S.; Ryu, H.G.; Kang, H.-S.; Kim, J.E.; et al. Optic nerve sheath diameter threshold by ocular ultrasonography for detection of increased intracranial pressure in Korean adult patients with brain lesions. Medicine (Baltimore) 2016, 95, e5061. [Google Scholar] [CrossRef]
- Wang, L.; Feng, L.; Yao, Y.; Wang, Y.; Chen, Y.; Feng, J.; Xing, Y. Optimal optic nerve sheath diameter threshold for the identification of elevated opening pressure on lumbar puncture in a Chinese population. PLoS ONE 2015, 10, e0117939. [Google Scholar] [CrossRef] [Green Version]
- Jeon, J.P.; Lee, S.U.; Kim, S.-E.; Kang, S.; Yang, J.S.; Choi, H.J.; Cho, Y.J.; Ban, S.P.; Byoun, H.S.; Kim, Y.S. Correlation of optic nerve sheath diameter with directly measured intracranial pressure in Korean adults using bedside ultrasonography. PLoS ONE 2017, 12, e0183170. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Deng, Y.; Li, H.; Qiao, S.; Yu, M.; Xu, Q.; Wang, C. Ratio of Optic Nerve Sheath Diameter to Eyeball Transverse Diameter by Ultrasound Can Predict Intracranial Hypertension in Traumatic Brain Injury Patients: A Prospective Study. Neurocrit. Care 2019, 32, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Li, J.; Ye, T.; Zeng, Y. Ultrasound measurements versus invasive intracranial pressure measurement method in patients with brain injury: A retrospective study. BMC Med. Imaging 2019, 19, 53. [Google Scholar] [CrossRef] [PubMed]
- Pierrakos, C.; Attou, R.; Decorte, L.; Kolyviras, A.; Malinverni, S.; Gottignies, P.; Devriendt, J.; de Bels, D. Transcranial Doppler to assess sepsis-associated encephalopathy in critically ill patients. BMC Anesth. 2014, 14, 45. [Google Scholar] [CrossRef]
- Robba, C.; Crippa, I.A.; Taccone, F.S. Septic Encephalopathy. Curr. Neurol. Neurosci. Rep. 2018, 18, 82. [Google Scholar] [CrossRef]
- Kuperberg, S.J.; Wadgaonkar, R. Sepsis-Associated Encephalopathy: The Blood–Brain Barrier and the Sphingolipid Rheostat. Front. Immunol. 2017, 8, 597. [Google Scholar] [CrossRef] [Green Version]
- Payen, J.-F.; Fauvage, B.; Falcon, D.; Lavagne, P. Brain oedema following blood-brain barrier disruption: Mechanisms and diagnosis. Ann. Fr. Anesth. Réanim. 2003, 22, 220–225. [Google Scholar] [CrossRef]
- Vaiman, M.; Gottlieb, P.; Bekerman, I. Quantitative relations between the eyeball, the optic nerve, and the optic canal important for intracranial pressure monitoring. Head Face Med. 2014, 10, 32. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Patient | Sex (M/F) | Age (Years) | APACHE II 1 | SAPS II 2 | SOFA 3 | CRP 4 (mg L−1) | PCT 5 (ng mL−1) | Lactate (mmol L−1) | ONSD 6 R (mm) | ONSD 6 L (mm) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 83 | 26 | 74 | 14 | 182.8 | 3.07 | 3.55 | 5.5 | 5.7 |
| 2 | M | 55 | 21 | 44 | 12 | 204.8 | 1.62 | 2.00 | 6.4 | 6.5 |
| 3 | M | 63 | 22 | 58 | 7 | 109.5 | 1.41 | 2.60 | 6.2 | 6.1 |
| 4 | F | 69 | 35 | 61 | 15 | 470.8 | 49.51 | 2.66 | 6.3 | 6.1 |
| 5 | F | 82 | 18 | 46 | 9 | 102.4 | 2.45 | 3.99 | 5.4 | 5.6 |
| 6 | M | 65 | 22 | 52 | 10 | 327.7 | 3.54 | 16.03 | 5.1 | 5.5 |
| 7 | M | 73 | 42 | 85 | 17 | 146.7 | 3.24 | 1.99 | 5.5 | 5.4 |
| 8 | F | 40 | 16 | 27 | 9 | 331.0 | 54.57 | 5.14 | 5.3 | 5.5 |
| 9 | F | 82 | 13 | 58 | 9 | 194.3 | 60.80 | 7.59 | 5.6 | 5.5 |
| 10 | M | 35 | 15 | 33 | 8 | 72.5 | 0.94 | 3.48 | 6.4 | 6.3 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Czempik, P.F.; Gąsiorek, J.; Bąk, A.; Krzych, Ł.J. Ultrasonic Assessment of Optic Nerve Sheath Diameter in Patients at Risk of Sepsis-Associated Brain Dysfunction: A Preliminary Report. Int. J. Environ. Res. Public Health 2020, 17, 3656. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103656
Czempik PF, Gąsiorek J, Bąk A, Krzych ŁJ. Ultrasonic Assessment of Optic Nerve Sheath Diameter in Patients at Risk of Sepsis-Associated Brain Dysfunction: A Preliminary Report. International Journal of Environmental Research and Public Health. 2020; 17(10):3656. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103656
Chicago/Turabian StyleCzempik, Piotr F., Jakub Gąsiorek, Aleksandra Bąk, and Łukasz J. Krzych. 2020. "Ultrasonic Assessment of Optic Nerve Sheath Diameter in Patients at Risk of Sepsis-Associated Brain Dysfunction: A Preliminary Report" International Journal of Environmental Research and Public Health 17, no. 10: 3656. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103656