Effects of a Rehabilitation Programme with a Nasal Inspiratory Restriction Device on Exercise Capacity and Quality of Life in COPD

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
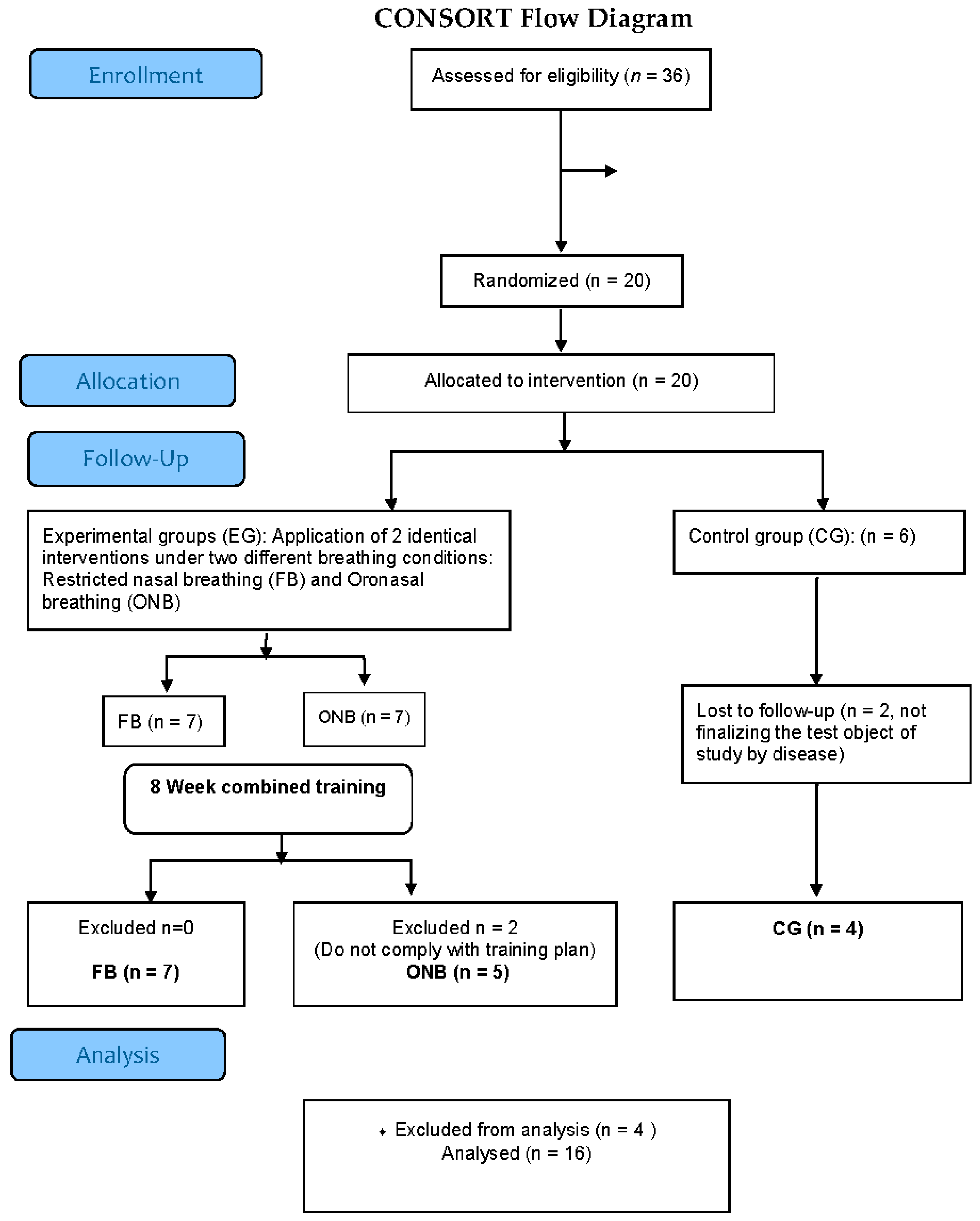
2.1. Study Population
2.2. Study Protocol
2.3. Training Program
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Miravitlles, M.; Soler-Cataluña, J.J.; Calle, M.; Molina, J.; Almagro, P.; Quintano, J.A.; Trigueros, J.A.; Cosío, B.G.; Casanova, C.; Antonio Riesco, J.; et al. Guía española de la enfermedad pulmonar obstructiva crónica (GesEPOC) 2017. Tratamiento farmacológico en fase estable. Arch. Bronconeumol. 2017, 53, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Agusti, A.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Criner, G.J.; Frith, P.; Halpin, D.M.G.; Han, M.; et al. Global strategy for the diagnosis, management, and prevention of Chronic obstructive pulmonary disease. Eur. Respir. J. 2019, 53, 1900164. [Google Scholar] [CrossRef] [PubMed]
- Celli, B.R.; MacNee, W.; Agusti, A.; Anzueto, A.; Berg, B.; Buist, A.S.; Calverley, P.M.A.; Chavannes, N.; Dillard, T.; Fahy, B.; et al. Standards for the diagnosis and treatment of patients with COPD: A summary of the ATS/ERS position paper. Eur. Respir. J. 2004, 23, 932–946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; Zu Wallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.C.; et al. An official American thoracic society/European respiratory society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef] [PubMed]
- Rochester, C.L.; Vogiatzis, I.; Holland, A.E.; Lareau, S.C.; Marciniuk, D.D.; Puhan, M.A.; Spruit, M.A.; Masefield, S.; Casaburi, R.; Clini, E.M.; et al. An official American Thoracic Society/European Respiratory Society policy statement: Enhancing implementation, use, and delivery of pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2015, 192, 1373–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orozco-Levi, M.; Gea Guiral, J. Cambios musculares en la enfermedad pulmonar obstructiva crónica: La teoría de los compartimientos. Arch. Bronconeumol. 2000, 36, 95–102. [Google Scholar] [CrossRef]
- Lacasse, Y.; Guyatt, G.H.; Goldstein, R.S. The components of a respiratory rehabilitation program: A systematic overview. Chest 1997, 111, 1077–1088. [Google Scholar] [CrossRef] [Green Version]
- Pothirat, C.; Limsukon, A.; Chaiwong, W.; Phetsuk, N.; Liwsrisakun, C.; Bumroongkit, C.; Deesomchok, A.; Theerakittikul, T. Long-term efficacy of intensive cycle ergometer exercise training program for advanced COPD patients. Int. J. Chron. Obstruct. Pulmon. Dis. 2015, 10, 133. [Google Scholar] [CrossRef] [Green Version]
- Gosselink, R.; De Vos, J.; Van Den Heuvel, S.P.; Segers, J.; Decramer, M.; Kwakkel, G. Impact of inspiratory muscle training in patients with COPD: What is the evidence? Eur. Respir. J. 2011, 37, 416–425. [Google Scholar] [CrossRef]
- Lötters, F.; van Tol, B.; Kwakkel, G.; Gosselink, R. Effects of controlled inspiratory muscle training in patients with COPD: A meta-analysis. Eur. Respir. J. 2002, 20, 570–576. [Google Scholar] [CrossRef]
- Beaumont, M.; Forget, P.; Couturaud, F.; Reychler, G. Effects of inspiratory muscle training in COPD patients: A systematic review and meta-analysis. Clin. Respir. J. 2018, 12, 2178–2188. [Google Scholar] [CrossRef] [PubMed]
- González-Montesinos, J.L.; Vaz Pardal, C.; Fernández Santos, J.R.; Arnedillo Muñoz, A.; Costa Sepúlveda, J.L.; Gómez Espinosa de los Monteros, R. Efectos del entrenamiento de la musculatura respiratoria sobre el rendimiento. Revisión bibliográfica. Rev. Andal. Med. Deport. 2012, 5, 163–170. [Google Scholar] [CrossRef] [Green Version]
- González Montesinos, J.L.; Fernández Santos, J.; Vaz Pardal, C.; Arnedillo Muñoz, A. Dispositivo para el Entrenamiento de la Musculatura nasal. Oficina Española de Patentes y Marcas U201930922, 3 June 2019. [Google Scholar]
- Morton, A.R.; King, K.; Papalia, S.; Goodman, C.; Turley, K.R.; Wilmore, J.H. Comparison of maximal oxygen consumption with oral and nasal breathing. Aust. J. Sci. Med. Sport 1995, 27, 51–55. [Google Scholar]
- Bailey, S.J.; Romer, L.M.; Kelly, J.; Wilkerson, D.P.; DiMenna, F.J.; Jones, A.M. Inspiratory muscle training enhances pulmonary O(2) uptake kinetics and high-intensity exercise tolerance in humans. J. Appl. Physiol. 2010, 109, 457–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Illi, S.K.; Held, U.; Frank, I.; Spengler, C.M. Effect of respiratory muscle training on exercise performance in healthy individuals: A systematic review and meta-analysis. Sport. Med. 2012, 42, 707–724. [Google Scholar] [CrossRef] [PubMed]
- González-Montesinos, J.L.; Ponce-González, J.G.; Vicente-Campos, D.; López-Chicharro, J.; Fernández-Santos, J.R.; Vaz-Pardal, C.; Costa-Sepúlveda, J.L.; Conde-Caveda, J.; Castro-Piñero, J. Efectos de un dispositivo de restricción ventilatoria nasal sobre la ventilación pulmonar e intercambio gaseoso durante el ejercicio en personas sanas. Nutr. Hosp. 2016, 33. [Google Scholar] [CrossRef] [Green Version]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582. [Google Scholar] [CrossRef]
- Cotes, J.E.; Chinn, D.J. MRC questionnaire (MRCQ) on respiratory symptoms. Occup. Med. 2007, 57, 388. [Google Scholar] [CrossRef] [Green Version]
- Jones, P.W.; Harding, G.; Berry, P.; Wiklund, I.; Chen, W.-H.; Kline Leidy, N. Development and first validation of the COPD Assessment Test. Eur. Respir. J. 2009, 34, 648–654. [Google Scholar] [CrossRef] [Green Version]
- Culver, B.H.; Graham, B.L.; Coates, A.L.; Wanger, J.; Berry, C.E.; Clarke, P.K.; Hallstrand, T.S.; Hankinson, J.L.; Kaminsky, D.A.; MacIntyre, N.R.; et al. Recommendations for a Standardized Pulmonary Function Report. An Official American Thoracic Society Technical Statement. Am. J. Respir. Crit. Care Med. 2017, 196, 1463–1472. [Google Scholar] [CrossRef]
- Redlich, C.A.; Tarlo, S.M.; Hankinson, J.L.; Townsend, M.C.; Eschenbacher, W.L.; Von Essen, S.G.; Sigsgaard, T.; Weissman, D.N.; American Thoracic Society Committee on Spirometry in the Occupational Setting Official. American Thoracic Society technical standards: Spirometry in the occupational setting. Am. J. Respir. Crit. Care Med. 2014, 189, 983–993. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [CrossRef] [PubMed]
- Foster, C.; Florhaug, J.A.; Franklin, J.; Gottschall, L.; Hrovatin, L.A.; Parker, S.; Doleshal, P.; Dodge, C. A New Approach to Monitoring Exercise Training. J. Strength Cond. Res. 2001, 15, 109–115. [Google Scholar] [PubMed]
- Van de Schoot, R.; Broere, J.J.; Perryck, K.H.; Zondervan-Zwijnenburg, M.; Van Loey, N.E. Analyzing small data sets using Bayesian estimation: The case of posttraumatic stress symptoms following mechanical ventilation in burn survivors. Eur. J. Psychotraumatol. 2015, 6, 25216. [Google Scholar] [CrossRef]
- Van de Schoot, R.; Sijbrandij, M.; Depaoli, S.; Winter, S.D.; Olff, M.; van Loey, N.E. Bayesian PTSD-trajectory analysis with informed priors based on a systematic literature search and expert elicitation. Multivariate Behav. Res. 2018, 53, 267–291. [Google Scholar] [CrossRef] [Green Version]
- Gelman, A.; Simpson, D.; Betancourt, M. The prior can often only be understood in the context of the likelihood. Entropy 2017, 19, 555. [Google Scholar] [CrossRef] [Green Version]
- Bürkner, P.-C. brms: An R package for Bayesian multilevel models using stan. J. Stat. Softw. 2017, 80, 21555. [Google Scholar] [CrossRef] [Green Version]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Saey, D.; Mccormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; Wanger, J.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef]
- Kon, S.S.C.; Canavan, J.L.; Jones, S.E.; Nolan, C.M.; Clark, A.L.; Dickson, M.J.; Haselden, B.M.; Polkey, M.I.; Man, W.D.C. Minimum clinically important difference for the COPD Assessment Test: A prospective analysis. Lancet Respir. Med. 2014, 2, 195–203. [Google Scholar] [CrossRef] [Green Version]
- Xi, F.; Wang, Z.; Qi, Y.; Brightwell, R.; Roberts, P.; Stewart, A.; Sim, M.; Wang, W. Long-term effect of respiratory training for chronic obstructive pulmonary disease patients at an outpatient clinic: A randomised controlled trial. Clin. Transl. Med. 2015, 4, 31. [Google Scholar] [CrossRef] [Green Version]
- Jaeschke, R.; Singer, J.; Guyatt, G.H. Measurement of health status. Ascertaining the minimal clinically important difference. Control. Clin. Trials 1989, 10, 407–415. [Google Scholar] [CrossRef]
- Puhan, M.A.; Chandra, D.; Mosenifar, Z.; Ries, A.; Make, B.; Hansel, N.N.; Wise, R.A.; Sciurba, F. The minimal important difference of exercise tests in severe COPD. Eur. Respir. J. 2011, 37, 784–790. [Google Scholar] [CrossRef] [PubMed]
- Dodd, J.W.; Hogg, L.; Nolan, J.; Jefford, H.; Grant, A.; Lord, V.M.; Falzon, C.; Garrod, R.; Lee, C.; Polkey, M.I.; et al. The COPD assessment test (CAT): Response to pulmonary rehabilitation. A multicentre, prospective study. Thorax 2011, 66, 425–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osterling, K.; MacFadyen, K.; Gilbert, R.; Dechman, G. The effects of high intensity exercise during pulmonary rehabilitation on ventilatory parameters in people with moderate to severe stable COPD: A systematic review. Int. J. Chron. Obstruct. Pulmon. Dis. 2014, 9, 1069–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wadell, K.; Webb, K.A.; Preston, M.E.; Amornputtisathaporn, N.; Samis, L.; Patelli, J.; Guenette, J.A.; O’Donnell, D.E. Impact of Pulmonary Rehabilitation on the Major Dimensions of Dyspnea in COPD. COPD J. Chronic Obstr. Pulm. Dis. 2013, 10, 425–435. [Google Scholar] [CrossRef]
- Scherer, T.A.; Spengler, C.M.; Owassapian, D.; Imhof, E.; Boutellier, U. Respiratory muscle endurance training in chronic obstructive pulmonary disease: Impact on exercise capacity, dyspnea, and quality of life. Am. J. Respir. Crit. Care Med. 2000, 162, 1709–1714. [Google Scholar] [CrossRef] [Green Version]
- Sonne, L.J.; Davis, J.A. Increased exercise performance in patients with severe COPD following inspiratory resistive training. Chest 1982, 81, 436–439. [Google Scholar] [CrossRef] [Green Version]
- Magadle, R.; McConnell, A.K.; Beckerman, M.; Weiner, P. Inspiratory muscle training in pulmonary rehabilitation program in COPD patients. Respir. Med. 2007, 7, 1500–1505. [Google Scholar] [CrossRef] [Green Version]
- Beaumont, M.; Mialon, P.; Ber-Moy, C.; Lochon, C.; Péran, L.; Pichon, R.; Gut-Gobert, C.; Leroyer, C.; Morelot-Panzini, C.; Couturaud, F. Inspiratory muscle training during pulmonary rehabilitation in chronic obstructive pulmonary disease. Chron. Respir. Dis. 2015, 12, 305–312. [Google Scholar] [CrossRef]
- Camillo, C.A.; Osadnik, C.R.; van Remoortel, H.; Burtin, C.; Janssens, W.; Troosters, T. Effect of “add-on” interventions on exercise training in individuals with COPD: A systematic review. ERJ Open Res. 2016, 2, 00078–02015. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | FB (n = 7) | ONB (n = 5) | CG (n = 4) | FB vs. ONB | FB vs. CG | ONB vs. CG |
|---|---|---|---|---|---|---|
| Age (years) | 65 ± 8.0 | 72 ± 7.4 | 70.2 ± 25.9 | −4.8 (−14.8, 6.2) | −6.6 (−15.5, 3.6) | 1.7 (−10.0, 12.9) |
| BMI (m/kg2) | 28.4 ± 4.2 | 26.8 ± 2.5 | 25.9 ± 2.1 | 1.5 (−2.4, 5.4) | 2.3 (−2.0, 6.3) | 0.8 (−3.6, 5.5) |
| DLCO (%) | 72.3 ± 20.0 | 71.4 ± 8.8 | 75.2 ± 16.4 | 0.85 (-9.8, 11.5) | −2.95 (−13.5, 10.5) | −3.8 (−15.8, 8.2) |
| RV/TLC (%) | 86.0 ± 10.6 | 84.5 ± 12.0 | 85.8 ± 14.6 | 1.5 (-6.4, 9.4) | 0.3 (−7.6, 8,1) | 1.3 (−7.4, 9.9) |
| FEV (mL) | 1571 ± 334 | 1608 ± 344 | 1812 ± 706 | −23.5 (−557, 469) | −218 (−760, 349) | 194 (−441, 773) |
| FEV (%) | 46.9 ± 10.6 | 51.2 ± 9.8 | 52.6 ± 19.9 | −3.7 (−18.4, 11.1) | −5.4 (−21.6, 10.8) | −1.8 (−19.8, 16.1) |
| FVC (mL) | 2869 ± 298 | 2580 ± 577 | 3270 ± 474 | 283 (−260, 801) | −382 (−929, 207) | −665 (−1317, −22.9) $ |
| FVC (%) | 63.9 ± 8.3 | 59.2 ± 10.0 | 67.1 ± 13.8 | 4.5 (−7.4, 17.1) | −3.1 (−15.9, 10.1) | −7.6 (21.5, 7.7) |
| FEV/FVC (%) | 54.1 ± 6.9 | 62.6 ± 5.6 | 54.2 ± 14.7 | −8.1 (−18.7, 2.8) | 0.0 (−11.4, 11.4) | 8.1 (−4.2, 20.8) |
| PImax (mmHg) | 93.3 ± 19.1 | 85.6 ± 23.9 | 102 ±14.85 | 7.9 (−15.6, 31.1) | −7.6(−34.3, 17.3) | −15.5 (−42.8, 12.5) |
| 6MWT (m) | 462.9 ± 71.8 | 439.1 ± 81.4 | 490.3 ± 80.0 | 23.6 (−68.6, 108.0) | −25.8 (−115.0, 75.1) | −49.4 (−148.0, 48.7) |
| CAT score | 9.7 ± 6.5 | 10.0 ± 4.5 | 6.8 ± 4.4 | −0.3 (−6.8, 6.4) | 2.7 (−3.8, 9.7) | 3.0 (−4.5, 10) |
| mMRC (score/%) | P(Y|FB) | P(Y|ONB) | P(Y|CG) | |||
| 0 | 0 (0%) | 0 (0%) | 0 (0%) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) |
| 1 | 0 (0%) | 0 (0%) | 0 (0%) | 0.0 (0.0–0.1) | 0.0 (0.0–0.2) | 0.0 (0.0–0.2) |
| 2 | 6 (85%) | 5 (100%) | 4 (100%) | 0.9 (0.6–1) $ | 0.9 (0.7–1) $ | 0.9 (0.7–1) $ |
| 3 | 1 (15%) | 0 (0%) | 0 (0%) | 0.1 (0.0–0.4) | 0.0 (0.0–0.2) | 0.0 (0.0–0.3) |
| Variables | FB vs. ONB | FB vs. CG | ONB vs. CG |
|---|---|---|---|
| CAT | −1.4 (−3.8–1.3) | −2.5 (−5.2–0.5) | −1.1 (−3.7–2.0) |
| 6MWT (m) | 34.2 (−0.2–70.7) | 45.4 (10.3–81.6) $ | 11.2 (−23.1–49.0) |
| PImax (mmHg) | 26.8 (3.7–49.4) $ | 32.3 (10.5–55.4) $ | 5.5 (−17.5–29.2) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arnedillo, A.; Gonzalez-Montesinos, J.L.; Fernandez-Santos, J.R.; Vaz-Pardal, C.; España-Domínguez, C.; Ponce-González, J.G.; Cuenca-García, M. Effects of a Rehabilitation Programme with a Nasal Inspiratory Restriction Device on Exercise Capacity and Quality of Life in COPD. Int. J. Environ. Res. Public Health 2020, 17, 3669. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103669
Arnedillo A, Gonzalez-Montesinos JL, Fernandez-Santos JR, Vaz-Pardal C, España-Domínguez C, Ponce-González JG, Cuenca-García M. Effects of a Rehabilitation Programme with a Nasal Inspiratory Restriction Device on Exercise Capacity and Quality of Life in COPD. International Journal of Environmental Research and Public Health. 2020; 17(10):3669. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103669
Chicago/Turabian StyleArnedillo, Aurelio, Jose L. Gonzalez-Montesinos, Jorge R. Fernandez-Santos, Carmen Vaz-Pardal, Carolina España-Domínguez, Jesús G. Ponce-González, and Magdalena Cuenca-García. 2020. "Effects of a Rehabilitation Programme with a Nasal Inspiratory Restriction Device on Exercise Capacity and Quality of Life in COPD" International Journal of Environmental Research and Public Health 17, no. 10: 3669. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103669