Injury Profile of Male and Female Senior and Youth Handball Players: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Study Coding and Data Extraction
2.4. Methodological Quality Assessment
3. Results
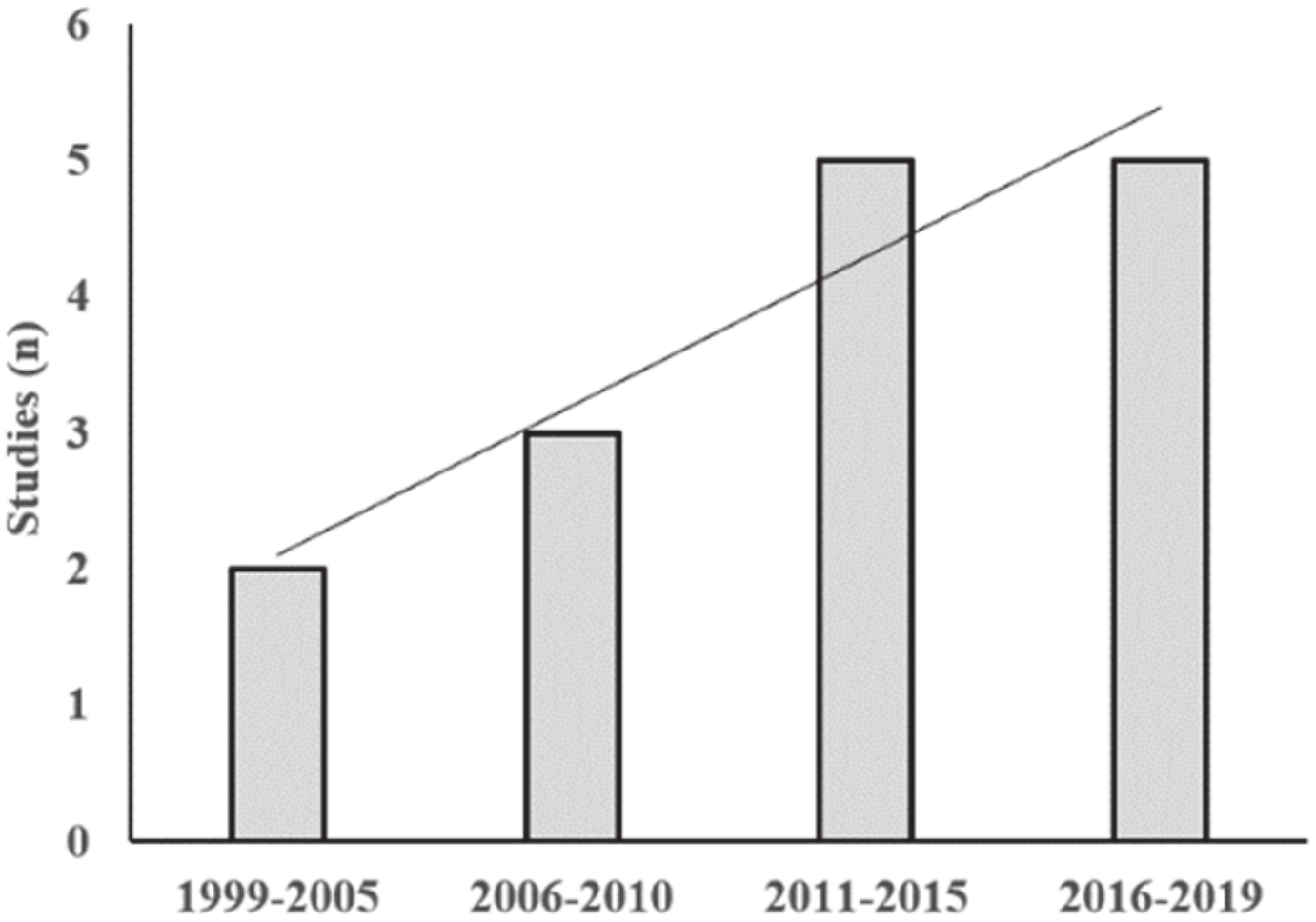
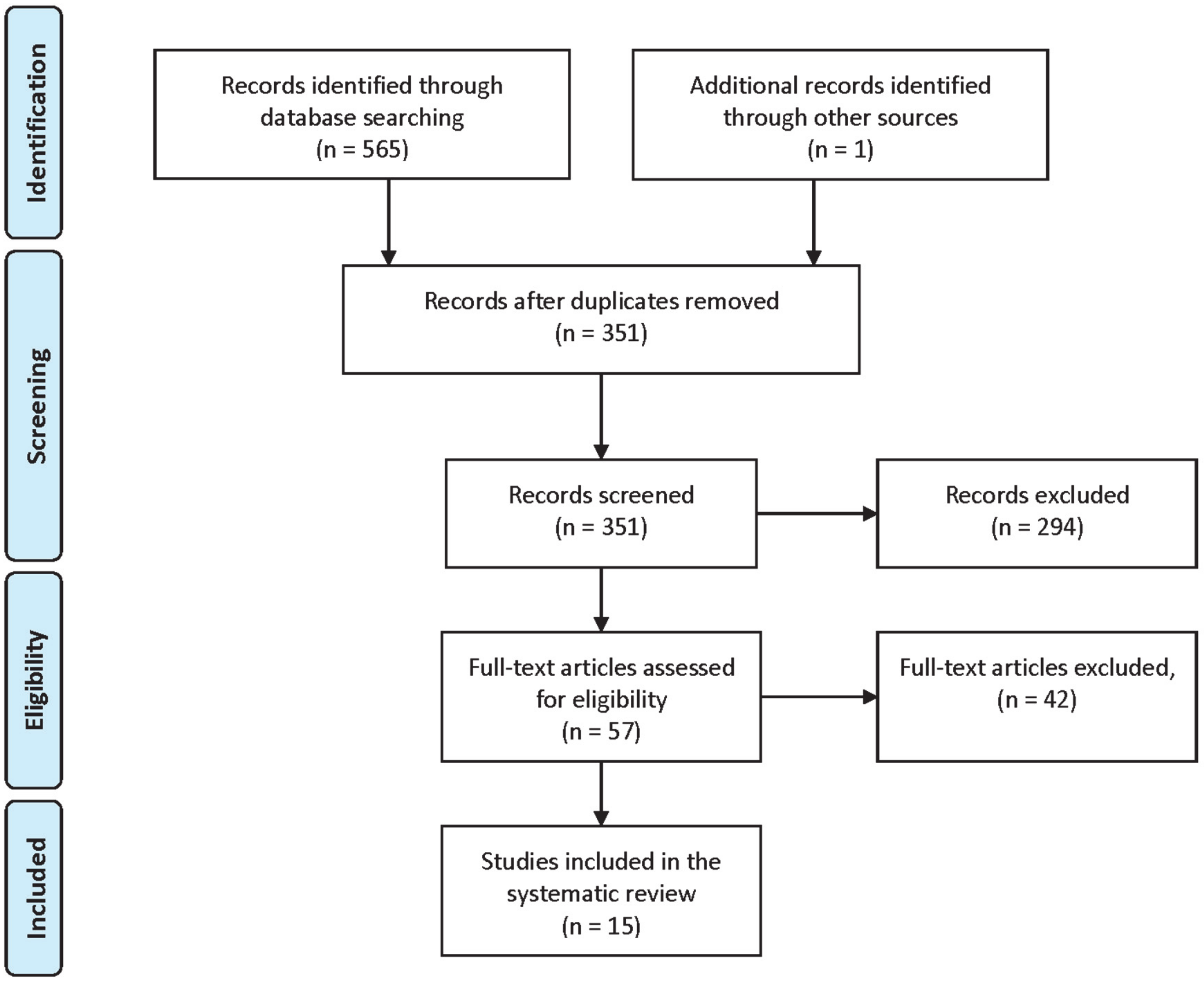
3.1. Search Results
3.2. Descriptive Characteristics of the Studies
3.2.1. Injury Incidence: Overall, Training and Match
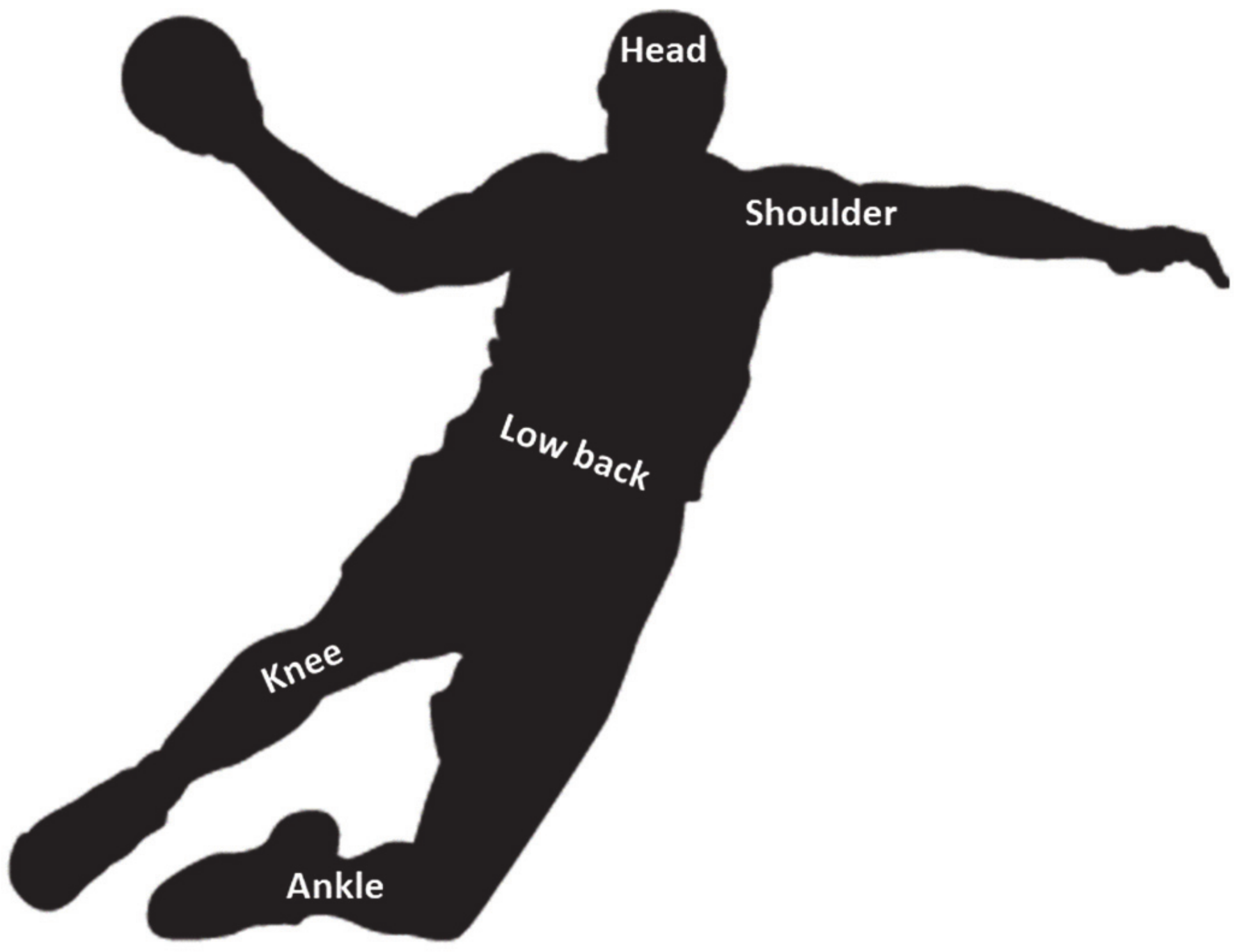
3.2.2. Location and Type of Injuries
3.2.3. Severity and Mechanism
3.2.4. Playing Position and Competition
3.3. Methodological Quality Assessment
4. Discussion
4.1. Injury Incidence: Overall, Training and Match
4.2. Location and Type of Injuries
4.3. Severity and Mechanism
4.4. Playing Position and Competition
4.5. Limitations
4.6. Practical Applications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Luig, P.; Krutsch, W.; Nerlich, M.; Henke, T.; Klein, C.; Bloch, H.; Platen, P.; Achenbach, L. Increased injury rates after the restructure of Germany’s national second league of team handball. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 26, 1884–1891. [Google Scholar] [CrossRef]
- Nikolaidis, P.T.; Ingebrigtsen, J. Physical and physiological characteristics of elite male handball players from teams with a different ranking. J. Hum. Kinet. 2013, 38, 115–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moller, M.; Attermann, J.; Myklebust, G.; Wedderkopp, N. Injury risk in Danish youth and senior elite handball using a new SMS text messages approach. Br. J. Sport. Med. 2012, 46, 531–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alesi, M.; Gómez-López, M.; Borrego, C.C.; Monteiro, D.; Granero-Gallegos, A. Effects of a motivational climate on psychological needs satisfaction, motivation and commitment in teen handball players. Int. J. Environ. Res. Public Health 2019, 16, 2702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hornstrup, T.; Póvoas, S.; Helge, J.W.; Melcher, P.S.; Fristrup, B.; Andersen, J.L.; Møgelvang, R.; Hansen, P.R.; Nybo, L.; Krustrup, P. Cardiovascular and metabolic health effects of team handball training in overweight women: Impact of prior experience. Scand. J. Med. Sci. Sports 2020, 30, 281–294. [Google Scholar] [CrossRef]
- Hornstrup, T.; Løwenstein, F.T.; Larsen, M.A.; Helge, E.W.; Póvoas, S.; Helge, J.W.; Nielsen, J.J.; Fristrup, B.; Andersen, J.L.; Gliemann, L.; et al. Cardiovascular, muscular, and skeletal adaptations to recreational team handball training: A randomized controlled trial with young adult untrained men. Eur. J. Appl. Physiol. 2019, 119, 561–573. [Google Scholar] [CrossRef]
- Engebretsen, L.; Soligard, T.; Steffen, K.; Alonso, J.M.; Aubry, M.; Budgett, R.; Dvorak, J.; Jegathesan, M.; Meeuwisse, W.H.; Mountjoy, M.; et al. Sports injuries and illnesses during the London Summer Olympic Games 2012. Br. J. Sport. Med. 2013, 47, 407–414. [Google Scholar] [CrossRef] [Green Version]
- Póvoas, S.C.A.; Seabra, A.F.T.; Ascensão, A.A.M.R.; Magalhães, J.; Soares, J.M.C.; Rebelo, A.N.C. Physical and physiological demands of elite team handball. J. Strength Cond. Res. 2012, 26, 3365–3375. [Google Scholar] [CrossRef]
- Kniubaite, A.; Skarbalius, A.; Clemente, F.M.; Conte, D. Quantification of external and internal match loads in elite female team handball. Biol. Sport 2019, 36, 311–316. [Google Scholar] [CrossRef]
- Tsigilis, N.; Hatzimanouil, D. Injuries in handball: Examination of the risk factors. Eur. J. Sport Sci. 2005, 5, 137–142. [Google Scholar] [CrossRef]
- Fredriksen, H.; Cools, A.; Bahr, R.; Myklebust, G. Does an effective shoulder injury prevention program affect risk factors in handball? A randomized controlled study. Scand. J. Med. Sci. Sports 2020. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Hägglund, M.; Waldén, M.; Magnusson, H.; Kristenson, K.; Bengtsson, H.; Ekstrand, J. Injuries affect team performance negatively in professional football: An 11-year follow-up of the UEFA Champions League injury study. Br. J. Sports Med. 2013, 47, 738–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekstrand, J. Keeping your top players on the pitch: The key to football medicine at a professional level. Br. J. Sport. Med. 2013, 47, 723–724. [Google Scholar] [CrossRef] [Green Version]
- Bahr, R.; Holme, I. Risk factors for sports injuries—A methodological approach. Br. J. Sports Med. 2003, 37, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Øiestad, B.E.; Holm, I.; Risberg, M.A. Return to pivoting sport after ACL reconstruction: Association with osteoarthritis and knee function at the 15-year follow-up. Br. J. Sports Med. 2018, 52, 1199–1204. [Google Scholar] [CrossRef]
- O’Brien, J.; Finch, C.F.; Pruna, R.; McCall, A. A new model for injury prevention in team sports: The Team-sport Injury Prevention (TIP) cycle. Sci. Med. Footb. 2019, 3, 77–80. [Google Scholar] [CrossRef]
- Van Mechelen, W.; Hlobil, H.; Kemper, H.C. Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sport. Med. 1992, 14, 82–99. [Google Scholar] [CrossRef]
- Bahr, R.; Clarsen, B.; Ekstrand, J. Why we should focus on the burden of injuries and illnesses, not just their incidence. Br. J. Sport. Med. 2017, 52, 1018. [Google Scholar] [CrossRef]
- Bere, T.; Alonso, J.-M.; Wangensteen, A.; Bakken, A.; Eirale, C.; Dijkstra, H.P.; Ahmed, H.; Bahr, R.; Popovic, N. Injury and illness surveillance during the 24th Men’s Handball World Championship 2015 in Qatar. Br. J. Sport. Med. 2015, 49, 1151–1156. [Google Scholar] [CrossRef]
- Mónaco, M.; Rincón, J.A.G.; Ronsano, B.J.M.; Whiteley, R.; Sanz-Lopez, F.; Rodas, G. Injury incidence and injury patterns by category, player position, and maturation in elite male handball elite players. Biol. Sport 2019, 36, 67–74. [Google Scholar] [CrossRef]
- Olsen, O.-E.; Myklebust, G.; Engebretsen, L.; Bahr, R. Injury pattern in youth team handball: A comparison of two prospective registration methods. Scand. J. Med. Sci. Sports 2006, 16, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Giroto, N.; Hespanhol Junior, L.C.; Gomes, M.R.C.; Lopes, A.D. Incidence and risk factors of injuries in Brazilian elite handball players: A prospective cohort study. Scand. J. Med. Sci. Sports 2017, 27, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Rafnsson, E.T.; Valdimarsson, Ö.; Sveinsson, T.; Árnason, Á. Injury pattern in Icelandic elite male handball players. Clin. J. Sport Med. 2017, 29, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Hulme, A.; Finch, C.F. From monocausality to systems thinking: A complementary and alternative conceptual approach for better understanding the development and prevention of sports injury. Inj. Epidemiol. 2015, 2, 31. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G.; Marshall, S.W.; Quarrie, K.L.; Hume, P.A. Risk factors and risk statistics for sports injuries. Clin. J. Sport Med. 2007, 17, 208–210. [Google Scholar] [CrossRef] [PubMed]
- Mayer, C.; Rühlemann, A.; Jäger, M. Handball injuries and their prevention. Orthopade 2019, 48, 1036–1041. [Google Scholar] [CrossRef]
- Nielsen, A.; Yde, J. An epidemiologic and traumatologic study of injuries in handball. Int. J. Sport. Med. 1988, 9, 341–344. [Google Scholar] [CrossRef]
- Michalsik, L.B.; Aagaard, P. Physical demands in elite team handball: Comparisons between male and female players. J. Sport. Med. Phys. Fit. 2015, 55, 878–891. [Google Scholar]
- Hoppe, M.W.; Brochhagen, J.; Baumgart, C.; Bauer, J.; Freiwald, J. Differences in anthropometric characteristics and physical capacities between junior and adult top-level handball players. Asian J. Sport. Med. 2017, 8, 1–11. [Google Scholar]
- Langevoort, G.; Myklebust, G.; Dvorak, J.; Junge, A. Handball injuries during major international tournaments. Scand. J. Med. Sci. Sports 2006, 17, 400–407. [Google Scholar] [CrossRef]
- Asai, K.; Nakase, J.; Shimozaki, K.; Toyooka, K.; Kitaoka, K.; Tsuchiya, H. Incidence of injury in young handball players during national competition: A 6-year survey. J. Orthop. Sci. 2019. [Google Scholar] [CrossRef] [PubMed]
- López-Valenciano, A.; Ruiz-Pérez, I.; Garcia-Gómez, A.; Vera-Garcia, F.J.; De Ste Croix, M.; Myer, G.D.; Ayala, F. Epidemiology of injuries in professional football: A systematic review and meta-analysis. Br. J. Sport. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Perera, N.K.; Joseph, C.; Kemp, J.L.; Finch, C.F. Epidemiology of injuries in women playing competitive team bat-or-stick sports: A systematic review and a meta-analysis. Sports Med. 2018, 48, 617–640. [Google Scholar] [CrossRef] [PubMed]
- King, D.; Hume, P.; Cummins, C.; Pearce, A.; Clark, T.; Foskett, A.; Barnes, M. Match and training injuries in women’s rugby union: A systematic review of published studies. Sports Med. 2019, 49, 1559–1574. [Google Scholar] [CrossRef] [PubMed]
- Andreoli, C.V.; Chiaramonti, B.C.; Buriel, E.; Pochini, A.D.C.; Ejnisman, B.; Cohen, M. Epidemiology of sports injuries in basketball: Integrative systematic review. BMJ Open Sport Exerc. Med. 2018, 4, e000468. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA group preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Pfirrmann, D.; Herbst, M.; Ingelfinger, P.; Simon, P.; Tug, S. Analysis of injury incidences in male professional adult and elite youth soccer players: A systematic review. J. Athl. Train. 2016, 51, 410–424. [Google Scholar] [CrossRef] [Green Version]
- Mónaco, M.; Gutiérrez Rincón, J.A.; Montoro Ronsano, J.B.; Til, L.; Drobnic, F.; Nardi Vilardaga, J.; Puigdellivol Grifell, J.; Pedret Carballido, C.; Rodas, G. Epidemiología lesional del balonmano de elite: Estudio retrospectivo en equipos profesional y formativo de un mismo club. Apunt. Med. L’esport 2013, 49, 11–19. [Google Scholar]
- Petersen, W.; Braun, C.; Bock, W.; Schmidt, K.; Weimann, A.; Drescher, W.; Eiling, E.; Stange, R.; Fuchs, T.; Hedderich, J.; et al. A controlled prospective case control study of a prevention training program in female team handball players: The German experience. Arch. Orthop. Trauma Surg. 2005, 125, 614–621. [Google Scholar] [CrossRef]
- Piry, H.; Fallahi, A.; Kordi, R.; Rajabi, R.; Rahimi, M.; Yosefi, M. Handball injuries in elite Asian players. World Appl. Sci. J. 2011, 14, 1559–1564. [Google Scholar]
- Tabben, M.; Landreau, P.; Chamari, K.; Juin, G.; Ahmed, H.; Farooq, A.; Bahr, R.; Popovic, N. Age, player position and 2 min suspensions were associated with match injuries during the 2017 Men’s Handball World Championship (France). Br. J. Sport. Med. 2019, 53, 436–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wedderkopp, N.; Kaltoft, M.; Lundgaard, B.; Rosendahl, M.; Froberg, K. Prevention of injuries in young female players in European team handball. A prospective intervention study. Scand. J. Med. Sci. Sports 1999, 9, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Junge, A.; Langevoort, G.; Pipe, A.; Peytavin, A.; Wong, F.; Mountjoy, M.; Beltrami, G.; Terrell, R.; Holzgraefe, M.; Charles, R.; et al. Injuries in team sport tournaments during the 2004 Olympic Games. Am. J. Sport. Med. 2006, 34, 565–576. [Google Scholar] [CrossRef] [PubMed]
- Van der Horst, N.; Smits, D.W.; Petersen, J.; Goedhart, E.A.; Backx, F.J.G. The preventive effect of the Nordic hamstring exercise on hamstring injuries in amateur soccer players: Study protocol for a randomised controlled trial. Inj. Prev. 2014, 20, e8. [Google Scholar] [CrossRef]
- Hägglund, M.; Waldén, M.; Bahr, R.; Ekstrand, J. Methods for epidemiological study of injuries to professional football players: Developing the UEFA model. Br. J. Sport. Med. 2005, 39, 340–346. [Google Scholar] [CrossRef] [Green Version]
- Castillo, D.; Raya-González, J.; Weston, M.; Yanci, J. Distribution of external load during acquisition training sessions and match play of a professional soccer team. J. Strength Cond. Res. 2019. [Google Scholar] [CrossRef]
- Cardinale, M.; Whiteley, R.; Hosny, A.A.; Popovic, N. Activity profiles and positional differences of handball players during the World Championships in Qatar 2015. Int. J. Sport. Physiol. Perform. 2017, 12, 908–915. [Google Scholar] [CrossRef]
- Gabbett, T.J. The training—injury prevention paradox: Should athletes be training smarter and harder? Br. J. Sport. Med. 2016, 50, 273–280. [Google Scholar] [CrossRef] [Green Version]
- Raya-González, J.; García-Esteban, S.; Hume, P.; Castillo, D. Effects of gluteal muscles strengthening on lower- limb injuries in male professional handball players : A preliminary study. J. Strength Cond. Res. 2020. [Google Scholar] [CrossRef]
- Degen, N.; Sass, J.; Jalali, J.; Kovacs, L.; Euler, E.; Prall, W.C.; Böcker, W.; Thaller, P.H.; Fürmetz, J. Three-dimensional assessment of lower limb alignment: Reference values and sex-related differences. Knee 2019, 27, 428–435. [Google Scholar] [CrossRef]
- Sakaguchi, M.; Ogawa, H.; Shimizu, N.; Kanehisa, H.; Yanai, T.; Kawakami, Y. Gender differences in hip and ankle joint kinematics on knee abduction during running. Eur. J. Sport Sci. 2014, 14 (Suppl. 1), S302–S309. [Google Scholar] [CrossRef] [PubMed]
- Mendiguchia, J.; Ford, K.R.; Quatman, C.E.; Alentorn-Geli, E.; Hewett, T.E. Sex differences in proximal control of the knee joint. Sports Med. 2011, 41, 541–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price, R.J.; Hawkins, R.D.; Hulse, M.A.; Hodson, A. The Football Association medical research programme: An audit of injuries in academy youth football. Br. J. Sport. Med. 2004, 38, 466–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raya-González, J.; de Ste Croix, M.; Read, P.; Castillo, D. A Longitudinal Investigation of muscle injuries in an elite spanish male academy soccer club: A hamstring injuries approach. Appl. Sci. 2020, 10, 1610. [Google Scholar] [CrossRef] [Green Version]
- Mallo, J.; González, P.; Veiga, S.; Navarro, E. Injury incidence in a spanish sub-elite professional football team: A prospective study during four consecutive seasons. J. Sports Sci. Med. 2011, 10, 731–736. [Google Scholar]
- Clemente, F.M.; Oliveira, H.; Vaz, T.; Carriço, S.; Calvete, F.; Mendes, B. Variations of perceived load and well-being between normal and congested weeks in elite case study handball team. Res. Sport. Med. 2019, 27, 412–423. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Age Range | Number of Participants (N) | Region | Status | Duration |
|---|---|---|---|---|---|---|
| Bere et al. (2015) [19] | Prospective cohort study | N/D | 384 | International | Elite | World championship |
| Giroto et al. (2015) [22] | Prospective cohort study | 24.1 y | 156 | Brazil | Elite | One season |
| Junge et al. (2006) [43] | Prospective cohort study | N/D | 168 | International | Elite | Olympic games |
| Langevoort et al. (2006) [30] | Prospective cohort study | N/D | 384 | International | Elite | World championship |
| Langevoort et al. (2006) [30] | Prospective cohort study | N/D | 384 | International | Elite | World championship |
| Luig et al. (2018) [1] | Retrospective cohort study | 25.8 y | 549 | Germany | Elite | Three seasons (First division) |
| Luig et al. (2018) [1] | Retrospective cohort study | 24.8 y | 828 | Germany | Elite | Three seasons (Second division) |
| Moller et al. (2012) [3] | Prospective cohort study | 24.9 y | 56 | Denmark | National level | 31 weeks |
| Mónaco et al. (2013) [38] | Prospective cohort study | 28.3 y | 89 | Spain | National level (First team) | Three seasons |
| Mónaco et al. (2013) [38] | Prospective cohort study | 20.1 y | 79 | Spain | National level (Second team) | Three seasons |
| Mónaco et al. (2019) [20] | Prospective cohort study | 20.4 y | 31 | Spain | National level (Second team) | Two seasons |
| Piry et al. (2011) [40] | Retrospective cohort study | N/D | 40 | Asia | Asian level | One year |
| Rafnsson et al. (2017) [23] | Prospective cohort study | 23.6 | 109 | Iceland | National level | One season |
| Tabben et al. (2019) [41] | Prospective cohort study | N/D | 387 | International | Elite | World championship |
| Study | Study Design | Age Range | Number of Participants (N) | Region | Status | Duration |
|---|---|---|---|---|---|---|
| Giroto et al. (2015) [22] | Prospective cohort study | 22.8 y | 183 | Brazil | Elite | One season |
| Junge et al. (2006) [43] | Prospective cohort study | N/D | 168 | International | Elite | Olympic games |
| Langevoort et al. (2006) [30] | Prospective cohort study | N/D | 384 | International | Elite | World championship |
| Langevoort et al. (2006) [30] | Prospective cohort study | N/D | 256 | Europe | Elite | Europe Cup |
| Moller et al. (2012) [3] | Prospective cohort study | 23.2 | 75 | Denmark | National level | 31 weeks |
| Petersen et al. (2005) [39] | Prospective cohort study | N/D | 142 | Germany | National level | One season |
| Study | Study Design | Age Range | Number of Participants (N) | Region | Status | Duration |
|---|---|---|---|---|---|---|
| Asai et al. (2019) [31] | Retrospective cohort study | 13–14 y | 3780 | Japan | National level | Six seasons |
| Moller et al. (2012) [3] | Prospective cohort study | 17.6 y (U18) | 41 | Denmark | National level | 31 weeks |
| Moller et al. (2012) [3] | Prospective cohort study | 15.7 y (U16) | 28 | Denmark | National level | 31 weeks |
| Mónaco et al. (2013) [38] | Prospective cohort study | 16.1 (U17) | 85 | Spain | National level | Three seasons |
| Mónaco et al. (2013) [38] | Prospective cohort study | 14.7 y (U15) | 87 | Spain | National level | Three seasons |
| Mónaco et al. (2013) [38] | Prospective cohort study | 12.7 y (U13) | 69 | Spain | National level | Three seasons |
| Mónaco et al. (2019) [20] | Prospective cohort study | 14.4 y (U15) | 133 | Spain | National level | Two seasons |
| Olsen et al. (2006) [21] | Prospective cohort study | U17 | 107 | Norway | National level | Seven months |
| Study | Study Design | Age Range | Number of Participants (N) | Region | Status | Duration |
|---|---|---|---|---|---|---|
| Asai et al. (2019) [31] | Retrospective cohort study | 13–14 y | 3300 | Japan | National level | Six seasons |
| Moller et al. (2012) [3] | Prospective cohort study | 17.5 y (U18) | 53 | Denmark | National level | 31 weeks |
| Moller et al. (2012) [3] | Prospective cohort study | 15.7 y (U16) | 89 | Denmark | National level | 31 weeks |
| Olsen et al. (2006) [21] | Prospective cohort study | U17 | 321 | Norway | National level | Seven months |
| Wedderkopp et al. (1999) [42] | Prospective cohort study | 16–18 y | 126 | Europe | Elite | One season |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raya-González, J.; Clemente, F.M.; Beato, M.; Castillo, D. Injury Profile of Male and Female Senior and Youth Handball Players: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 3925. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113925
Raya-González J, Clemente FM, Beato M, Castillo D. Injury Profile of Male and Female Senior and Youth Handball Players: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(11):3925. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113925
Chicago/Turabian StyleRaya-González, Javier, Filipe Manuel Clemente, Marco Beato, and Daniel Castillo. 2020. "Injury Profile of Male and Female Senior and Youth Handball Players: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 11: 3925. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113925