Preferences of Patients with Non-Communicable Diseases for Primary Healthcare Facilities: A Discrete Choice Experiment in Wuhan, China

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design Development
2.1.1. Selection of Attributes
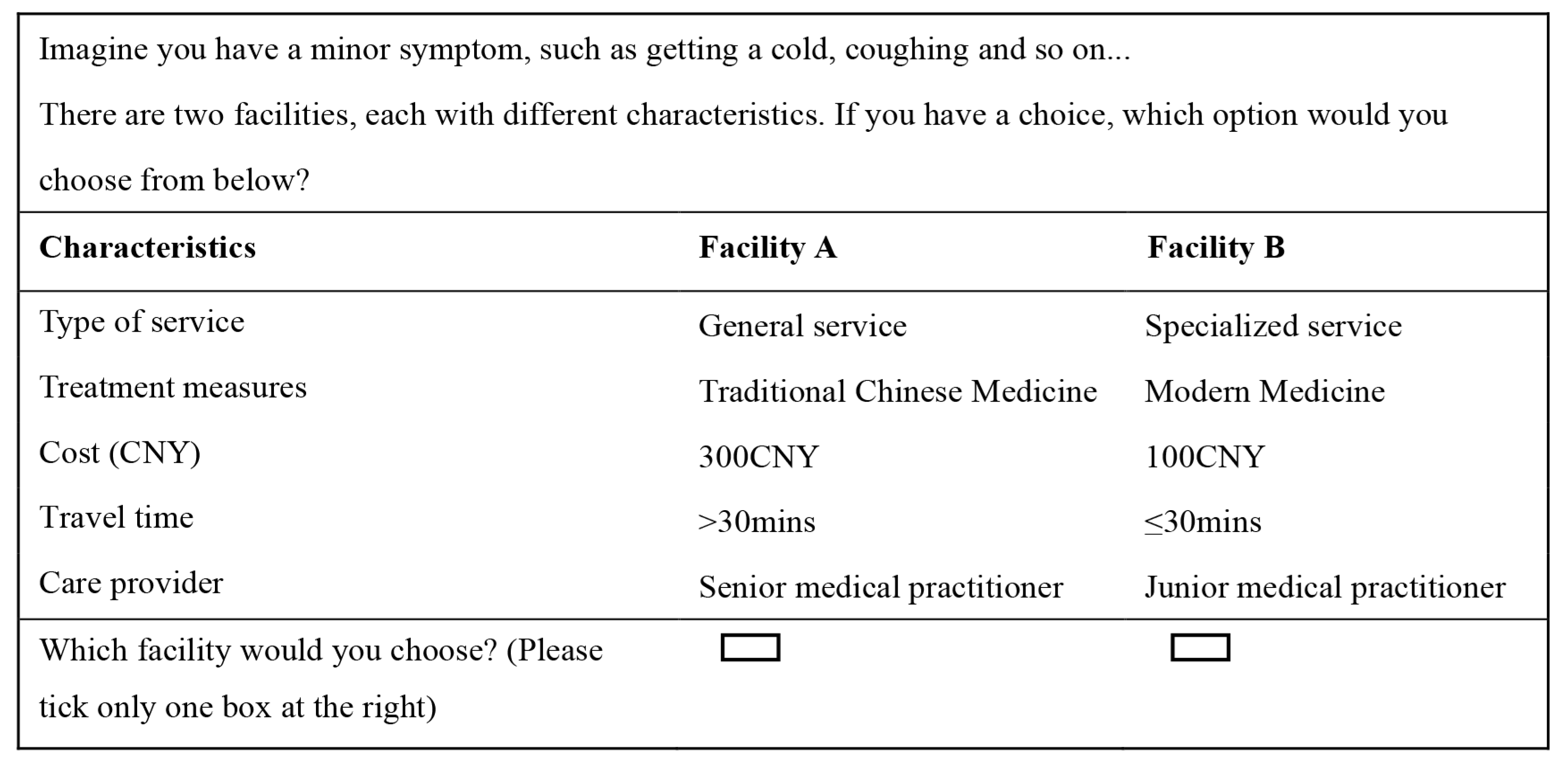
2.1.2. DCE Design
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. General Characteristics
3.2. Preferences under Different Hypothetical Disease Severities
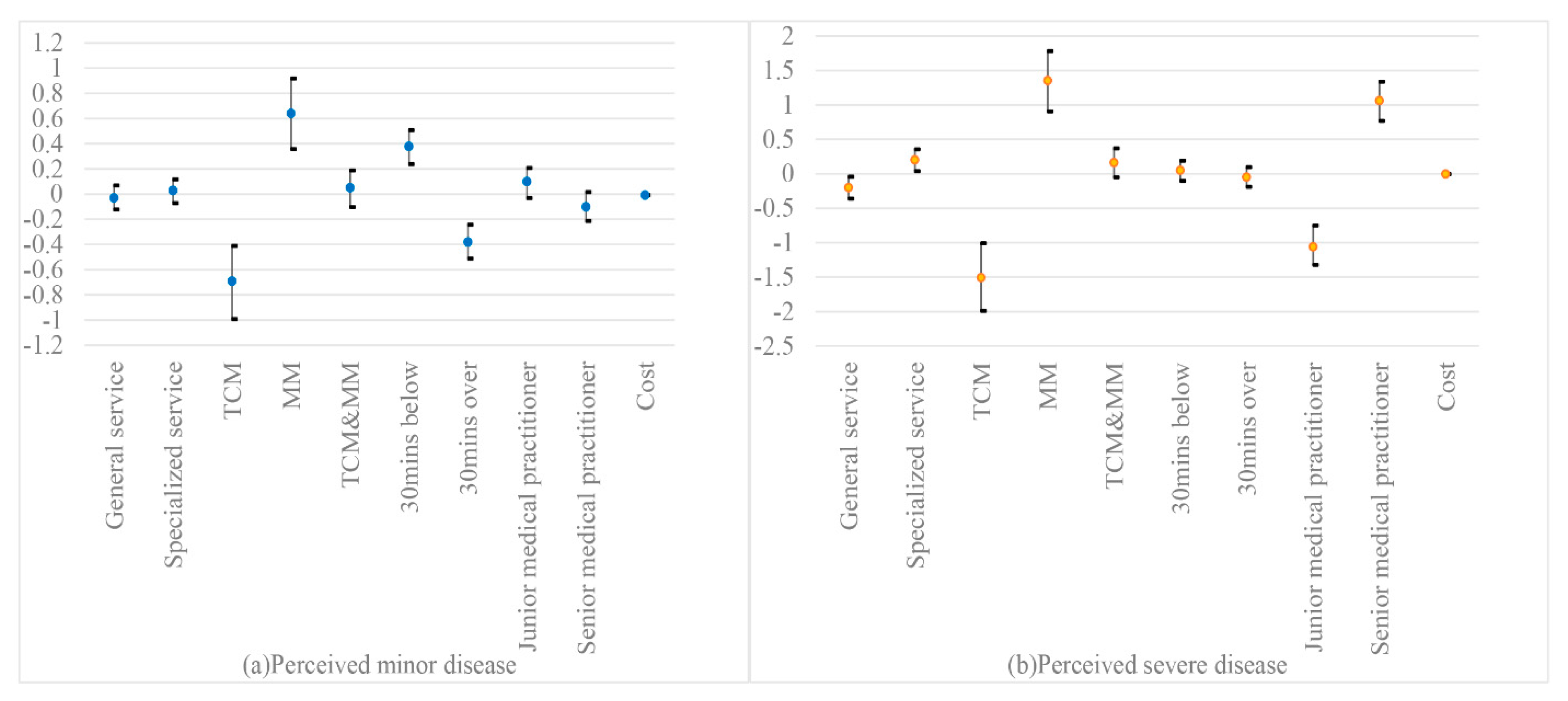
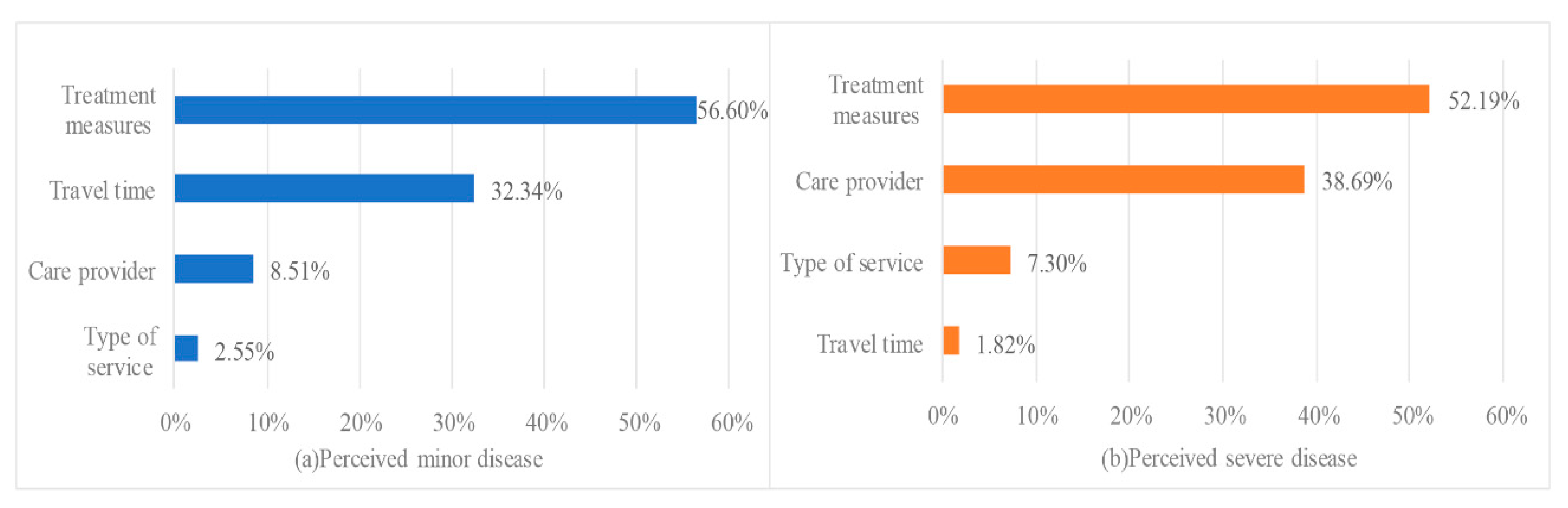
3.3. Preference Weights and Relative Importance of Attributes and Levels
3.4. Preference Heterogeneity
3.5. WTP Estimates
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data Availability
Abbreviations
| PHC | Primary healthcare |
| DCE | Discrete choice experiment |
| WTP | Willingness-to-pay |
| NCDs | Non-communicable diseases |
| MM | Modern Medicine |
| TCM | Traditional Chinese Medicine |
| Integration of TCM & MM | Integration of Traditional Chinese Medicine & Modern Medicine |
| GP | General practitioner |
| DALYs | Disability-adjusted life years |
| AIC | Akaike information criterion |
| BIC | Bayesian information criterion |
| SE | Standard errors |
| SD | Standard deviation |
| CI | Confidence intervals |
Appendix A

{kind=link}
{kind=link}
{kind=link}
| District | Gross Domestic Product (100 Million CNY) |
|---|---|
| Jiangan | 1073.60 |
| Jianghan | 1142.58 |
| Qiaokou | 668.07 |
| Hanyang | 948.31 |
| Wuchang | 1102.50 |
| Qingshan | 521.88 |
| Hongshan | 957.73 |
| Wuhan Airport Economic Development Zone | 730.63 |
| Caidian | 397.65 |
| Jiangxia | 770.98 |
| Huangpi | 702.49 |
| Xinzhou | 676.32 |
Appendix B
| Demographic Attribute | Variables |
|---|---|
| Age | Continuous |
| Region | Urban a |
| Suburban | |
| Gender | Male a |
| Female | |
| Marital status | Single a |
| Married | |
| Education | Middle school and below a |
| High school or higher | |
| Employment | Working a |
| Not working | |
| Family per capita monthly income (CNY) | ≤3000 a |
| >3000 |
References
- Hua, Y. Building a healthy china: Strategic significance, challenge, key measures. J. Chin. Acad. Gov. 2017, 20, 105–111. [Google Scholar]
- National Health Commission of the people’s republic of China. China Health and Family Planning Statistical Yearbook 2017; China Xie-he Medical University Press: Beijing, China, 2017.
- Zeng, X.Y.; Qi, J.L.; Yin, P.; Wang, L.J.; Liu, Y.N.; Liu, J.M.; Zhou, M.G. Report on the burden of disease in China and provincial administrative regions from 1990 to 2016. Chin. Circ. J. 2018, 33, 1147–1158. [Google Scholar]
- GBD 2013 DALYs and HALE Collaborators; Murray, C.J.; Barber, R.M.; Foreman, K.J.; Abbasoqlu Ozqoren, A.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Abraham, J.P.; Abubakar, I.; et al. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: Quantifying the epidemiological transition. Lancet 2015, 386, 2145–2191. [Google Scholar]
- Bodenheimer, T.; Wagner, E.H.; Grumbach, K. Improving primary care for patients with chronic illness. JAMA 2002, 288, 1775–1779. [Google Scholar] [CrossRef]
- Qiao, G.H.; Liao, P.; Jia, J.Z.; Li, W.Z.; Chen, T.Z.; Wang, Z.F. Equity of general practitioner distribution in China. Chin. Gen. Prac. 2020, 23, 1606–1610. [Google Scholar]
- Commission National Health. China Health Statistical Yearbook 2018; Peking Union Medical College Press: Beijing, China, 2018.
- National Bureau of Disease Control and Prevention. Interpretation of China’s medium—Long-Term Plan for the Prevention and Treatment of Chronic Diseases (2017–2025). Available online: http://www.nhc.gov.cn/jkj/s3586/201702/34a1fff908274ef8b776b5a3fa4d364b.shtml (accessed on 9 May 2020).
- Yip, W.; Hsiao, W. Harnessing the privatisation of China’s fragmented health-care delivery. Lancet 2014, 384, 805–818. [Google Scholar] [CrossRef]
- Wu, D.; Lam, T.P. Underuse of primary care in china: The scale, causes, and solutions. J. Am. Board Fam. Med. 2016, 29, 240–247. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Lu, J.P.; Hu, S.; Hu, S.; Cheng, K.K.; Maeseneer, J.D.; Meng, Q.Y.; Mossialso, E.; Dong Roman Xu, M.P.P.; Winnie, Y.; et al. The primary health-care system in China. Lancet 2017, 390, 2584–2594. [Google Scholar] [CrossRef]
- National Health Commission of the people’s republic of China. China Health and Family Planning Statistical Yearbook 2013; China Xie-he Medical University Press: Beijing, China, 2013.
- Yu, W.; Li, M.; Nong, X.; Ding, T.; Ye, F.; Liu, J.; Dai, Z.; Zhang, L. Practices and attitudes of doctors and patients to downward referral in Shanghai, China. BMJ Open 2017, 7, e012565. [Google Scholar] [CrossRef] [Green Version]
- De Bekker-Grob, E.W.; Essink-Bot, M.L.; Meerding, W.J.; Pols, H.A.; Koes, B.W.; Steyerberq, E.W. Patients’ preferences for osteoporosis drug treatment: A discrete choice experiment. Osteoporos Int. 2008, 19, 1029–1037. [Google Scholar] [CrossRef] [Green Version]
- Feehan, M.; Walsh, M.; Godin, J.; Sundwall, D.; Munqer, M.A. Patient preferences for healthcare delivery through community pharmacy settings in the USA: A discrete choice study. J. Clin. Pharm. Ther. 2017, 42, 738–749. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhong, L.; Yuan, S.; van de Klundert, J. Why patients prefer high-level healthcare facilities: A qualitative study using focus groups in rural and urban China. BMJ Glob. Health 2018, 3, e000854. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Yin, H.; Zheng, T.; llia, B.; Wang, X.; Chen, R.; Hao, Y.; Sun, H.; Jiao, M.; Kang, Z.; et al. Primary health institutions preference by hypertensive patients: Effect of distance, trust and quality of management in the rural Heilongjiang province of China. BMC Health Serv. Res. 2019, 19, 852. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Zhang, H.; Sun, X.; Gu, Y.; Zhen, X.; Gu, S.; Li, Y.; Huang, M.; Wei, J.; Dong, H. Older adults’ choices of first-contact care and related factors in Zhejiang and Qinghai Province, China. Geriatr. Gerontol. Int. 2019, 19, 938–944. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Kong, Q.; de Bekker-Grob, E.W. Public preferences for health care facilities in rural China: A discrete choice experiment. Soc. Sci. Med. 2019, 237, 112396. [Google Scholar] [CrossRef]
- Liu, T.; Li, S.; Yang, R.; Liu, S.; Chen, G. Job preferences of undergraduate nursing students in eastern China: A discrete choice experiment. Hum. Resour. Health 2019, 17, 1. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Li, S.; Li, Y.; Wang, H.; Zhao, J.; Chen, G. Job preferences for healthcare administration students in China: A discrete choice experiment. PLoS ONE 2019, 14, e0211345. [Google Scholar] [CrossRef] [Green Version]
- Muehlbacher, A.C.; Bridges, J.F.; Bethge, S.; Dintsios, C.M.; Schwalm, A.; Gerber-Grote, A.; Nubling, M. Preferences for antiviral therapy of chronic hepatitis C: A discrete choice experiment. Eur. J. Health Econ. 2017, 18, 155–165. [Google Scholar] [CrossRef]
- Patil, R.; Cotler, S.J.; Banaad-Omiotek, G.; McNutt, R.A.; Brown, M.D.; Cotler, S.; Jensen, D.M. Physicians’ preference values for hepatitis C health states and antiviral therapy: A survey. BMC Gastroenterol. 2001, 1, 6. [Google Scholar] [CrossRef] [Green Version]
- Robyn, P.J.; Baernighausen, T.; Souares, A.; Savadogo, G.; Bicaba, B.; Sie, A.; Sauerborn, R. Health worker preferences for community-based health insurance payment mechanisms: A discrete choice experiment. BMC Health Serv. Res. 2012, 12, 159. [Google Scholar] [CrossRef] [Green Version]
- Barber, S.; Bekker, H.; Marti, J.; Pavitt, S.; Khambay, B.; Meads, D. Development of a Discrete-Choice Experiment (DCE) to elicit adolescent and parent preferences for hypodontia treatment. Patient 2019, 12, 137–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lancsar, E.; Louviere, J. Conducting discrete choice experiments to inform healthcare decision making: A user guide. Pharmacoeconomics 2008, 26, 661–677. [Google Scholar] [CrossRef] [PubMed]
- Coast, J.; Al-Janabi, H.; Sutton, E.J.; Horrocks, S.A.; Vosper, A.J.; Swancutt, D.R.; Flynn, T.N. Using qualitative methods for attribute development for discrete choice experiments: Issues and recommendations. Health Econ. 2012, 21, 730–741. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Li, M.; Ye, F.; Xue, C.; Zhang, L. Patient preference and choice of healthcare providers in Shanghai, China: A cross-sectional study. BMJ Open 2017, 7, e016418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Light, D.W. The real ethics of rationing. BMJ 1997, 315, 112–115. [Google Scholar] [CrossRef] [PubMed]
- Kleij, K.S.; Tangermann, U.; Amelung, V.E.; Krauth, C. Patients’ preferences for primary health care—A systematic literature review of discrete choice experiments. BMC Health Serv. Res. 2017, 17, 476. [Google Scholar] [CrossRef] [Green Version]
- Groenewoud, S.; Van Exel, N.J.; Bobinac, A.; Berq, M.; Huijsman, R.; Stolk, E.A. What influences patients’ decisions when choosing a health care provider? Measuring preferences of patients with knee Arthrosis, chronic depression, or Alzheimer’s disease, using discrete choice experiments. Health Serv. Res. 2015, 50, 1941–1972. [Google Scholar] [CrossRef]
- Niu, Y.; Ye, T.; Zhang, Y.; Zhang, L. Can primary medical institutions lead to worse health status for patients with noncommunicable diseases compared with high-level hospitals? A follow-up observation study in China. Int. J. Environ. Res. Public Health 2019, 16, 1336. [Google Scholar] [CrossRef] [Green Version]
- Hesketh, T.; Zhu, W.X. Health in China—Traditional Chinese medicine: One country, two systems. BMJ 1997, 315, 115–117. [Google Scholar] [CrossRef] [Green Version]
- United States Agency for International Development; World Health Organization; World Bank. How to Conduct a Discrete Choice Experiment for Health Workforce Recruitment and Retention in Remote and Rural Areas: A User Guider with Case Studies; World Health Organization Press: Geneva, Switzerland, 2012.
- Ryan, M.; Skatun, D. Modelling non-demanders in choice experiments. Health Econ. 2004, 13, 397–402. [Google Scholar] [CrossRef]
- Orme, B. Sample Size Issues for Conjoint Analysis; Sawtooth Software Research paper series: Sequim, WA, USA, 1998. [Google Scholar]
- Johnson, R.; Orme, B. Getting the most from CBC; Sawtooth Software Research Paper Series: Sequim, WA, USA, 2003. [Google Scholar]
- Coast, J.; Horrocks, S. Developing attributes and levels for discrete choice experiments using qualitative methods. J. Health Serv. Res. Policy 2007, 12, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Marshall, D.; Bridges, J.F.; Hauber, B.; Cameron, R.; Donnalley, L.; Fyie, K.; Johnson, F.R. Conjoint analysis applications in health—How are studies being designed and reported? An update on current practice in the published literature between 2005 and 2008. Patient 2010, 3, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Wuhan Municipal Statistics Bureau, State Statistical Bureau Wuhan Investigation Team. Wuhan Statistical Yearbook 2018; China Statistics Press: Beijing, China, 2018. [Google Scholar]
- Marshall, H.S.; Chen, G.; Clarke, M.; Ratcliffe, J. Adolescent, parent and societal preferences and willingness to pay for meningococcal B vaccine: A discrete choice experiment. Vaccine 2016, 34, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Bech, M.; Gyrd-Hansen, D. Effects coding in discrete choice experiments. Health Econ. 2005, 14, 1079–1083. [Google Scholar] [CrossRef] [PubMed]
- Bliemer, M.C.J.; Rose, J.M. Confidence intervals of willingness-to-pay for random coefficient logit models. Transp. Res. Part B Methodol. 2013, 58, 199–214. [Google Scholar] [CrossRef] [Green Version]
- Goett, A.A.; Hudson, K.; Train, K.E. Customers’ choice among retail energy suppliers: The willingness-to-pay for service attributes. Energy J. 2000, 21, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Hole, A.R. A comparison of approaches to estimating confidence intervals for willingness to pay measures. Health Econ. 2007, 16, 827–840. [Google Scholar] [CrossRef] [Green Version]
- Liao, Q.Y.; Tiffany, W.Y.N. Benjamin J cowling. What influenza vaccination programmes are preferred by healthcare personnel? A discrete choice experiment. Vaccine 2020, 38, 4557–4563. [Google Scholar] [CrossRef]
- Hauber, A.B.; Gonzalez, J.; Groothuis-Oudshoorn, C.; Prior, T.; Marshall, D.A.; Cunningham, C.; Bridges, J.F. Statistical methods for the analysis of discrete choice experiments: A report of the ISPOR conjoint analysis good research practices task force. Value Health 2016, 19, 300–315. [Google Scholar] [CrossRef] [Green Version]
- Lancsar, E.; Louviere, J.; Flynn, T. Several methods to investigate relative attribute impact in stated preference experiments. Soc. Sci. Med. 2007, 64, 1738–1753. [Google Scholar] [CrossRef] [Green Version]
- Goossens, A.J.M.; Cheung, K.L.; Sijstermans, E.; Conde, R.; Gonzalez, J.G.R.; Hiligsmann, M. A discrete choice experiment to assess patients’ preferences for HIV treatment in the rural population in Colombia. J. Med. Econ. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Li, C.X.; Xu, Q.; Huang, P.X. Analysis on the utilization of traditional Chinese medicine and influencing factors for community residents in the Pudong new area. Chin. Prim. Health Care 2017, 31, 19–21. [Google Scholar]
- Wei, B.; Bai, L.; Bai, J.Q.; Tian, C.Y. Current situation of Chinese medicine services in community health service centers in Hebei Province. Chin. Gen. Prac. 2014, 17, 3150–3152. [Google Scholar]
- Jiang, Y.; Xu, Y.; Hong, B.L.; Zhao, X.; Bai, B.N.; Cheng, W. Research on the utilization of traditional Chinese medicine service in Beijing based on the provider distribution method. Chin Health Econ. 2017, 36, 60–62. [Google Scholar]
- Health Statistics and Information Center. An Analysis Report of National Health Services Survey in China 2013; Health Statistics and Information Center: Beijing, China, 2015.
- Wang, L.; Wang, Z.; Ma, Q.; Fang, G.; Yang, J. The development and reform of public health in China from 1949 to 2019. Glob. Health 2019, 15, 45. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Shi, Y.W.; Wang, H.X.; Sun, B.Y. The impacts of medical facility accessibility on patients’ medical treatment space: A case study in shanghai. Urban Development Studies. 2019, 26, 46–52, 61. [Google Scholar]
- Qian, D.; Pong, R.W.; Yin, A.; Naqurajan, K.V.; Meng, Q. Determinants of health care demand in poor, rural China: The case of Gansu Province. Health Policy Plan 2009, 24, 324–334. [Google Scholar] [CrossRef] [Green Version]
- Manthiram, K.; Blood, E.A.; Kuppuswamy, V.; Martins, Y.; Narayan, A.; Burmeister, K.; Parvathy, K.; Hassan, A. Predictors of optional immunization uptake in an urban south Indian population. Vaccine 2014, 32, 3417–3423. [Google Scholar] [CrossRef]
- Zhu, J.; Li, J.; Zhang, Z.; Li, H.; Cai, L. Exploring determinants of health provider choice and heterogeneity in preference among outpatients in Beijing: A labelled discrete choice experiment. BMJ Open 2019, 9, e023363. [Google Scholar] [CrossRef] [Green Version]
- Lu, R.Y.; Lian, D.Q.; Li, Y.P.; Liu, X.M.; Ruan, J.J. Job preferences of doctors at township health center for choosing a job in depresses area based on Mixed Logit Model. Chin. J. Health Policy 2018, 11, 45–48. [Google Scholar]
- Yip, W.; Fu, H.; Chen, A.T.; Zhai, T.; Jian, W.; Xu, R.; Pan, J.; Hu, M.; Zhou, Z.; Chen, Q.; et al. 10 years of health-care reform in China: Progress and gaps in Universal Health Coverage. Lancet 2019, 394, 1192–1204. [Google Scholar] [CrossRef]
- Jia, X.X.; Xu, L.; Zhang, Y.G.; Hu, H.Y.; Wang, X.X.; Zhuo, L.; Chen, J.Y. Prevalence of common chronic diseases and its influences on health-related quality of life among general population aged 15 years and over in China. Chin. J. Publ. Health 2017, 33, 1567–1570. [Google Scholar]
- Wang, X.H.; Lin, J.N.; Liu, G.Z.; Fan, H.M.; Huang, Y.P.; Li, C.J.; Yan, H.Y. Women are at a higher risk of chronic metabolic diseases compared to men with increasing body mass index in China. Front. Endocrinol. 2020, 11, 127. [Google Scholar] [CrossRef] [PubMed]



| Hypothetical Scenarios | Explanation | |
|---|---|---|
| Disease severity | Minor | Suppose that you are getting a cold, cough and so on |
| Severe | Suppose that health status seriously affects your daily life over a long period of time and makes you worry and anxious | |
| Attributes | Levels | Explanation |
| 1. Type of service | General service a Specialized service | Type of service refers to different modes of services consisting of differing skill sets. |
| 2. Treatment measures | Traditional Chinese Medicine (TCM) a Modern Medicine (MM) Integration of Traditional Chinese Medicine & Modern Medicine (Integration of TCM & MM) | Treatment measurements are different approaches (usually stand for differing medicine system) of diagnosis and treatment of diseases. |
| 3. Cost (CNY) b | 100 a 200 300 | Cost is average expense of each visit for healthcare seeking, which was set according to China Statistical Yearbook in 2017. |
| 4. Travel time (min) | ≤30 a >30 | Travel time stands for the time taken to go to healthcare facilities from home (one-way travel). |
| 5. Care provider | Senior medical practitioner a Junior medical practitioner | Care provider is the healthcare provider with differing seniority. |
| Characteristic | N (%) |
|---|---|
| Gender | |
| Female | 132 (67.4) (pre-defined quota: 49%) |
| Male | 64 (32.6) (pre-defined quota: 51%) |
| Region | |
| Urban area | 115 (58.7) (pre-defined quota: 69.1%) |
| Suburban area | 81 (41.3) (pre-defined quota: 30.9%) |
| Age | |
| 45–65 | 78 (39.8) |
| ≥65 | 118 (60.2) |
| Marital status | |
| Single | 26 (13.3) |
| Married | 170 (86.7) |
| Education | |
| Elementary school and below | 31 (15.8) |
| Middle school | 100 (51.0) |
| High school and above | 65 (33.2) |
| Employment | |
| Employed/Working | 36 (18.4) |
| Retiree/Pensioner | 118 (60.2) |
| Not working | 42 (21.4) |
| Family per capita monthly income (CNY) | |
| ≤1500 | 18 (9.2) |
| 1500–4000 | 117 (59.7) |
| >4000 | 61 (31.1) |
| Minor Disease Scenario | Severe Disease Scenario | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Attributes and Levels | Mean | SE | SD | SE | WTP/95%CI | Mean | SE | SD | SE | WTP/95%CI | |
| Type of service: | |||||||||||
| General service a | −0.03 | 0.05 | 0.03 | 0.28 | −3.45 (−16.51, 9.61) | −0.20 | 0.08 * | 0.64 | 0.11 ** | −53.65 (−107.53, 0.24) | |
| Specialized service | 0.03 | 0.05 | 0.03 | 0.28 | 3.45 (−9.61, 16.51) | 0.20 | 0.08 * | 0.64 | 0.11 ** | 53.65 (−0.24, 107.53) | |
| Treatment measures: | |||||||||||
| TCM a | −0.69 | 0.15 ** | 1.62 | 0.17 ** | −94.15 (−135.91, −53.45) | −1.51 | 0.25 ** | 2.19 | 0.27 ** | −400.71 (−610.50, −190.91) | |
| MM | 0.64 | 0.14 ** | 1.60 | 0.16 ** | 87.60 (47.73, 127.47) | 1.35 | 0.22 ** | 2.18 | 0.26 ** | 361.02 (168.12, 553.93) | |
| Integration of TCM&MM | 0.05 | 0.07 | 0.01 | 0.32 | 6.55 (−13.47, 26.57) | 0.16 | 0.11 | 0.18 | 0.30 | 42.75 (−14.35, 99.84) | |
| Travel time: | |||||||||||
| ≤30 min a | 0.38 | 0.07 ** | 0.62 | 0.09 ** | 51.42 (32.09, 69.34) | 0.05 | 0.07 | 0.45 | 0.11 ** | 12.16 (−26.37, 50.68) | |
| >30 min | −0.38 | 0.07 ** | 0.62 | 0.08 ** | −51.42 (−70.21, −32.64) | −0.05 | 0.07 | 0.45 | 0.11 ** | −12.16 (−50.68, 26.37) | |
| Care provider: | |||||||||||
| Junior medical practitioner a | 0.10 | 0.06 | 0.55 | 0.09 ** | 13.14 (−3.70, 28.41) | −1.06 | 0.14 ** | 1.15 | 0.15 ** | −282.90 (−439.37, −141.69) | |
| Senior medical practitioner | −0.10 | 0.06 | 0.52 | 0.08 ** | −13.14 (−29.40, 3.12) | 1.06 | 0.14 ** | 1.10 | 0.14 ** | 282.90 (144.77,421.04) | |
| Cost (CNY) | −0.007 | 0.001 ** | −0.004 | 0.001 ** | |||||||
| Model fit | AIC | 1650.13 | 1395.14 | ||||||||
| BIC | 1716.68 | 1461.68 | |||||||||
| Log likelihood | −814.07 | −686.57 | |||||||||
| Respondents, n | 196 | ||||||||||
| Observations, n | 3136 | ||||||||||
| Attributes and Levels | Minor Disease Scenario | Severe Disease Scenario | ||
|---|---|---|---|---|
| Mean | 95%CI | Mean | 95%CI | |
| Type of service: | ||||
| General service a | ||||
| Specialized service | 0.0002 | (−0.71, 0.71) | −0.35 | (−1.64, 0.93) |
| Treatment measures: | ||||
| TCM a | ||||
| MM | 1.28 | (−0.82, 3.39) | 2.49 | (−0.79, 5.77) |
| Integration of TCM&MM | 0.07 | (−1.03, 1.17) | 1.04 | (−0.56, 2.64) |
| Travel time: | ||||
| ≤30 min a | ||||
| >30 min | −0.06 | (−1.02, 0.90) | −0.65 | (−1.92, 0.62) |
| Care provider: | ||||
| Junior medical practitioner a | ||||
| Senior medical practitioner | 0.58 | (−0.31, 1.47) | 0.72 | (−0.83,2.27) |
| Cost (CNY) | 0.01 | (−0.003, 0.02) | 0.01 | (−0.004, 0.02) |
| Interaction: attribute * demographic attributes | ||||
| Cost * region | −0.005 ** | (−0.008, −0.001) | ||
| Cost * marital status | −0.01 ** | (−0.020, −0.003) | ||
| Cost * family per capita monthly income | 0.006 ** | (0.002, 0.010) | ||
| >30 min * region | −0.64 ** | (−0.94, −0.33) | ||
| Senior medical practitioner * gender | −0.28 * | (−0.560, −0.002) | ||
| Senior medical practitioner * region | 0.57 * | (0.06, 1.08) | ||
| Senior medical practitioner * marital status | 0.92 * | (0.15, 1.68) | ||
| Specialized service * education | 0.32 * | (0.05, 0.60) | ||
| Specialized service * region | 0.47 * | (0.07, 0.86) | ||
| MM * gender | −1.07 * | (−2.09, −0.06) | ||
| Integration of TCM&MM * employment | 0.87 * | (0.06, 1.67) | ||
| Model fit AIC | 1653.43 | 1411.46 | ||
| BIC | 1974.08 | 1732.08 | ||
| Log likelihood | −773.71 | −652.73 | ||
| Respondents, n | 196 | |||
| Observations, n | 3136 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jia, E.; Gu, Y.; Peng, Y.; Li, X.; Shen, X.; Jiang, M.; Xiong, J. Preferences of Patients with Non-Communicable Diseases for Primary Healthcare Facilities: A Discrete Choice Experiment in Wuhan, China. Int. J. Environ. Res. Public Health 2020, 17, 3987. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113987
Jia E, Gu Y, Peng Y, Li X, Shen X, Jiang M, Xiong J. Preferences of Patients with Non-Communicable Diseases for Primary Healthcare Facilities: A Discrete Choice Experiment in Wuhan, China. International Journal of Environmental Research and Public Health. 2020; 17(11):3987. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113987
Chicago/Turabian StyleJia, Erping, Yuanyuan Gu, Yingying Peng, Xianglin Li, Xiao Shen, Mingzhu Jiang, and Juyang Xiong. 2020. "Preferences of Patients with Non-Communicable Diseases for Primary Healthcare Facilities: A Discrete Choice Experiment in Wuhan, China" International Journal of Environmental Research and Public Health 17, no. 11: 3987. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113987