Acute Physical Activity, Executive Function, and Attention Performance in Children with Attention-Deficit Hyperactivity Disorder and Typically Developing Children: An Experimental Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
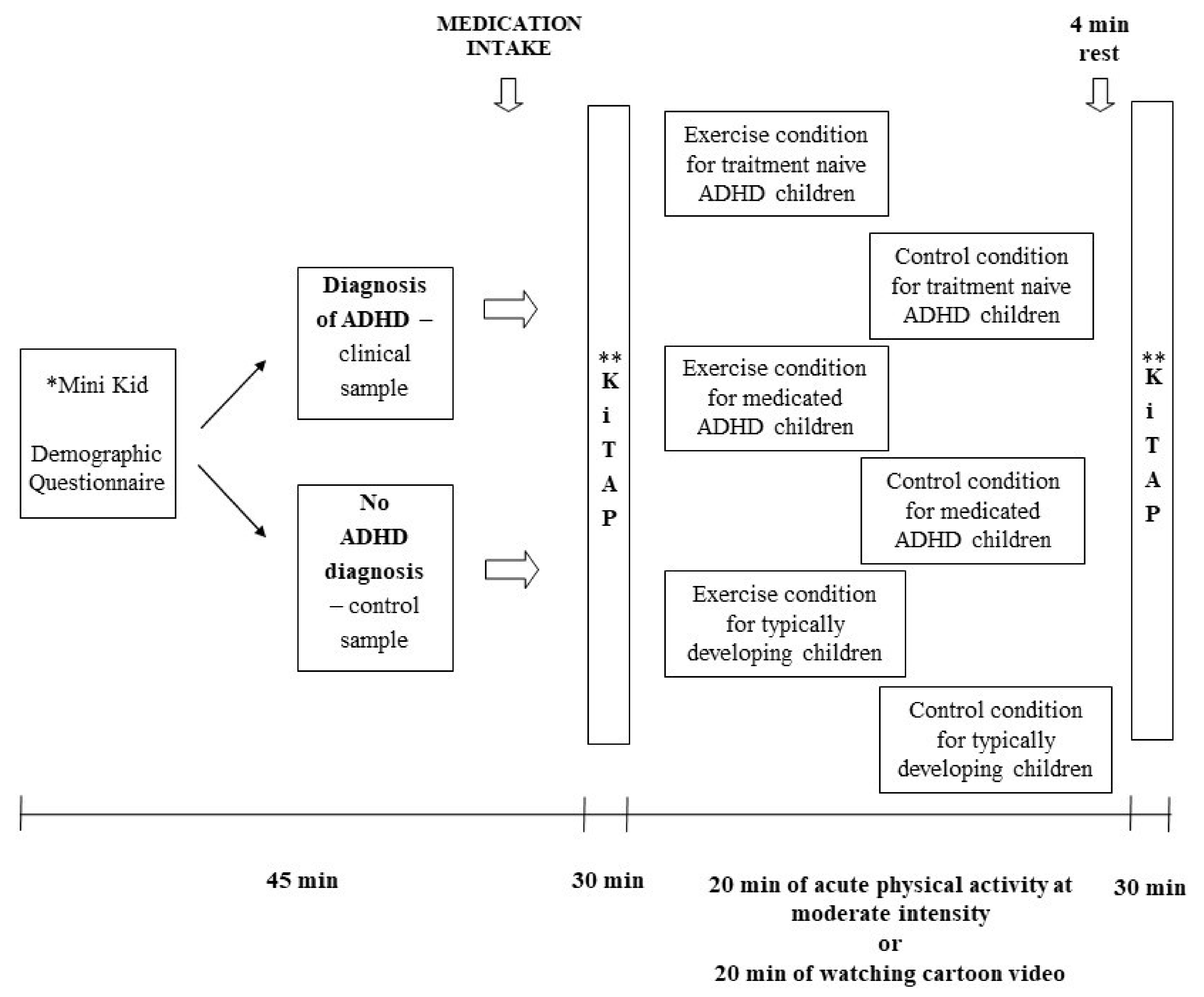
2.2. Experimental Protocols and Procedures
2.3. Measures
2.3.1. Mini International Neuropsychiatric Interview for Children and Adolescents (MINI Kid)
2.3.2. Demographic Questionnaire
2.3.3. KiTAP
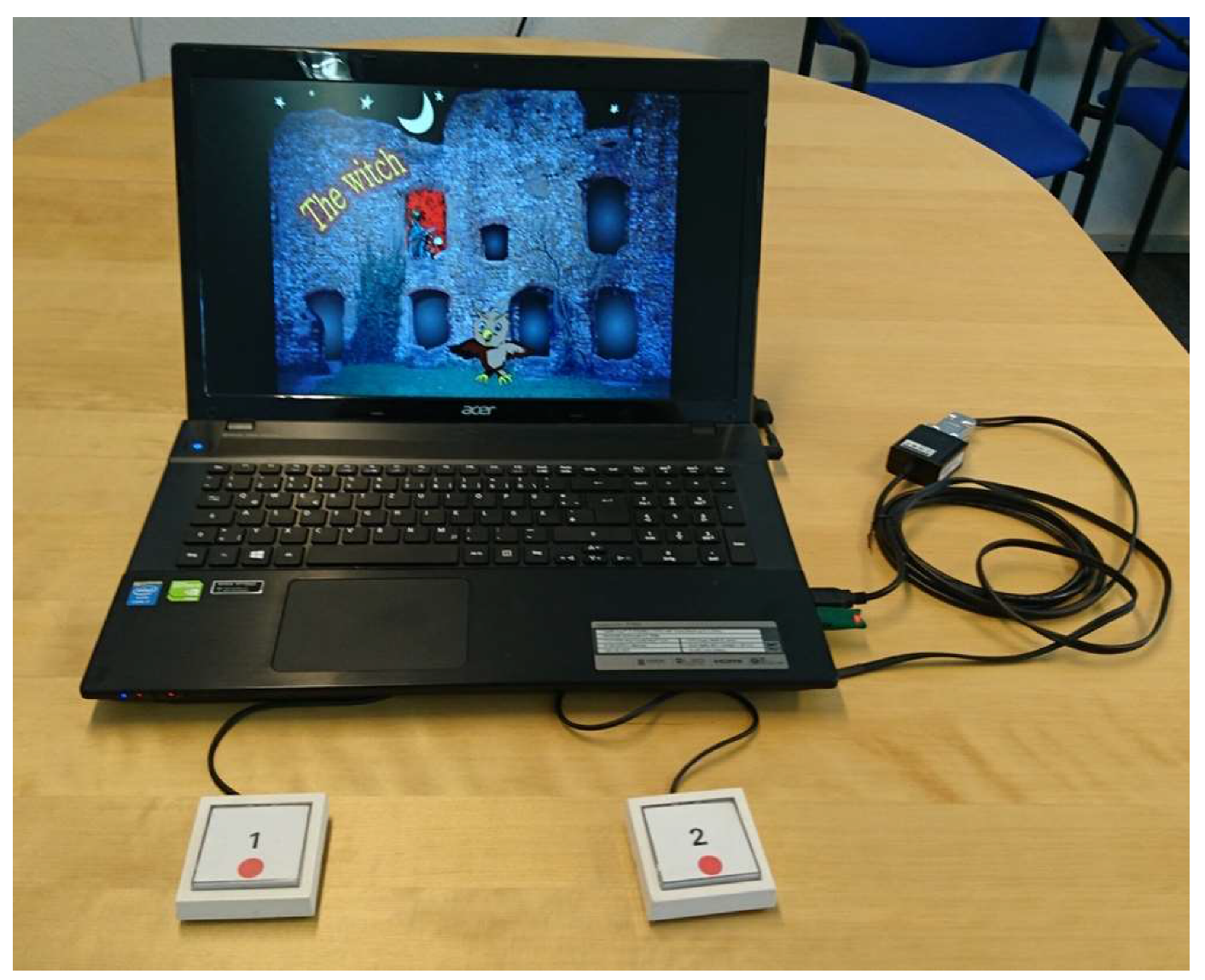
2.3.4. Equipment Used in the Exercise and Control Condition
2.4. Statistical Analysis
3. Results
3.1. Sample
3.2. KiTAP Parameters
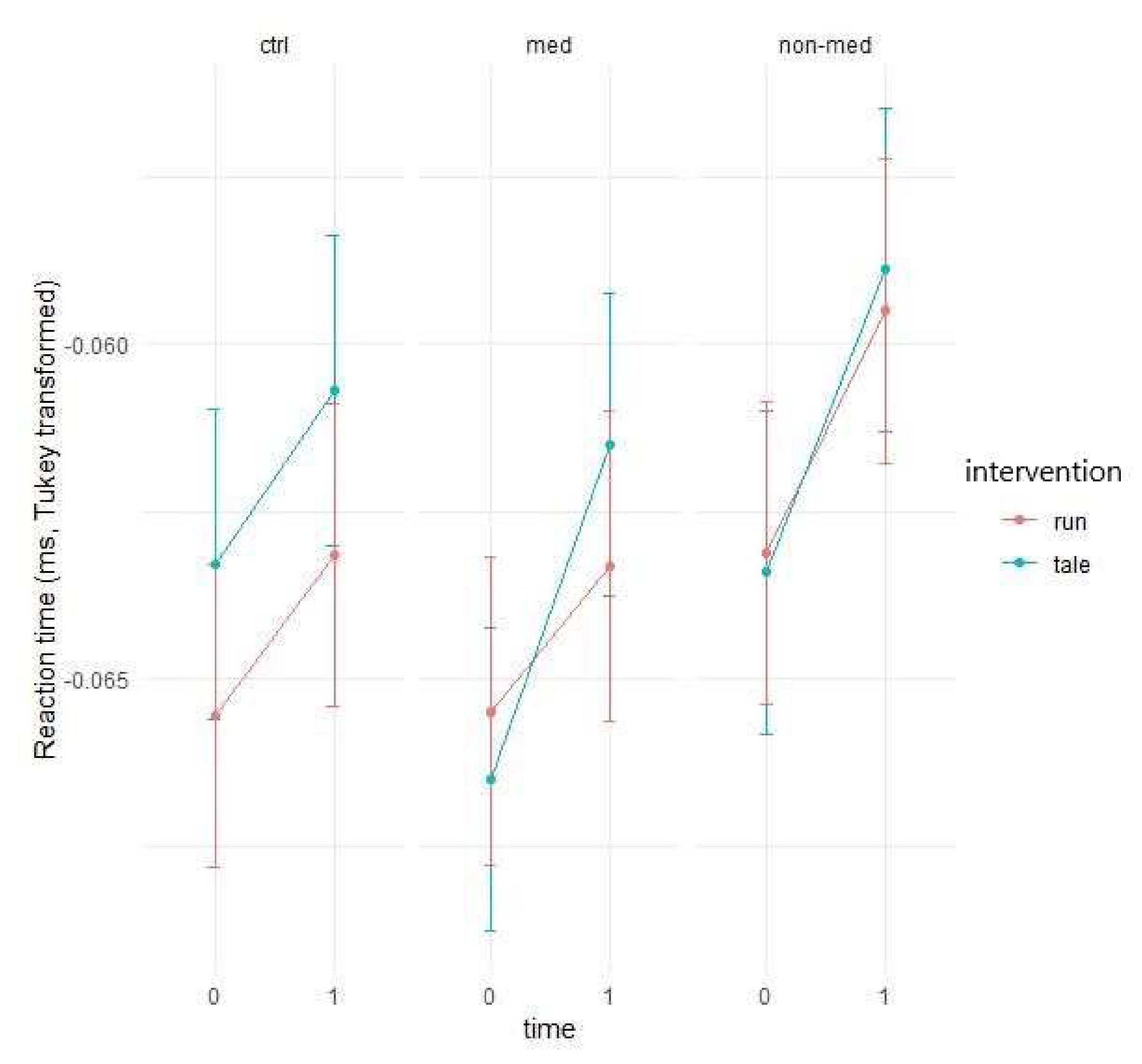
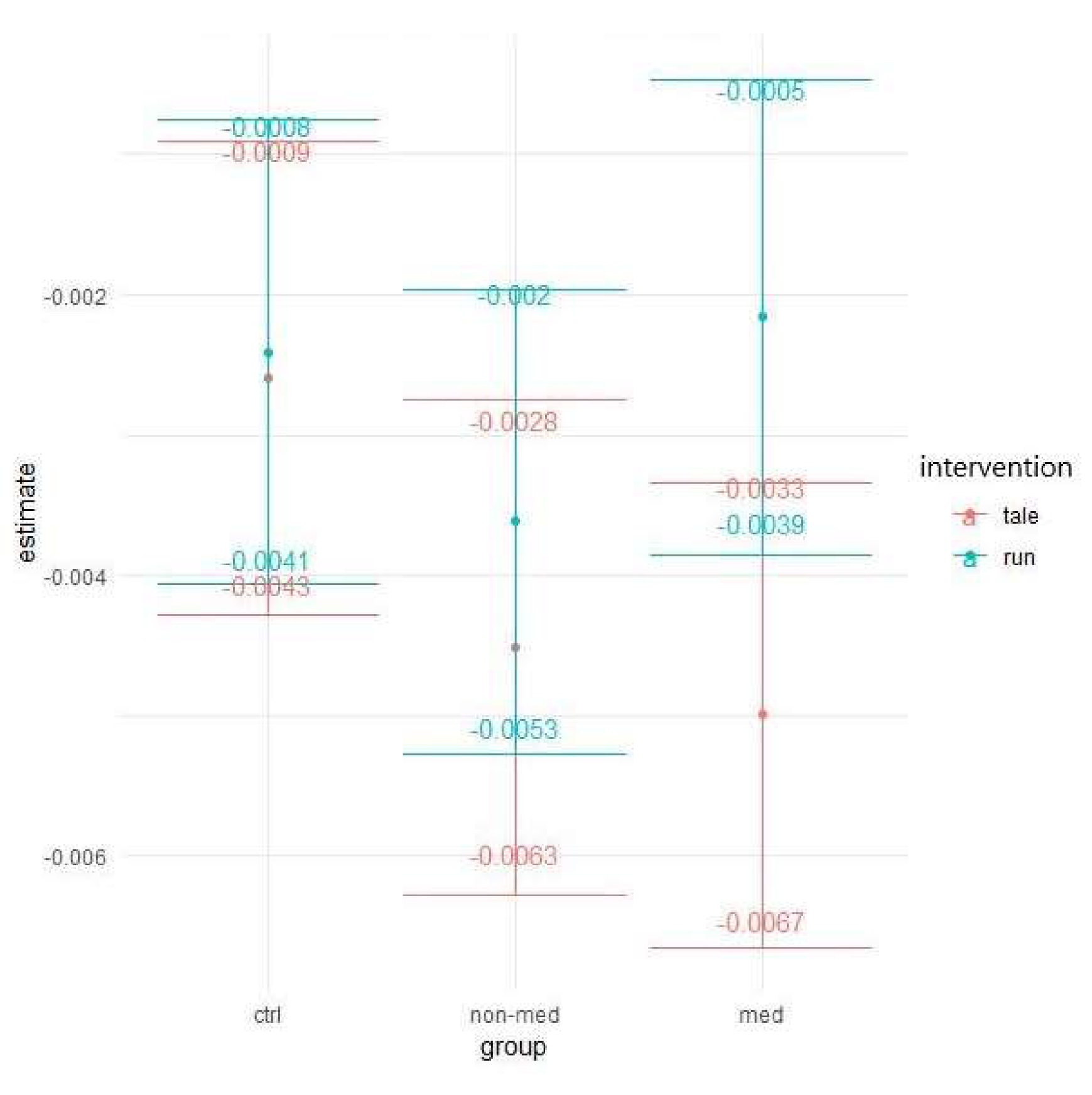
3.2.1. Alertness
Median of Reaction Time
Variability of Reaction Time
3.2.2. Distractibility
Total Omissions
Omissions with Distractor
Omissions without Distractor
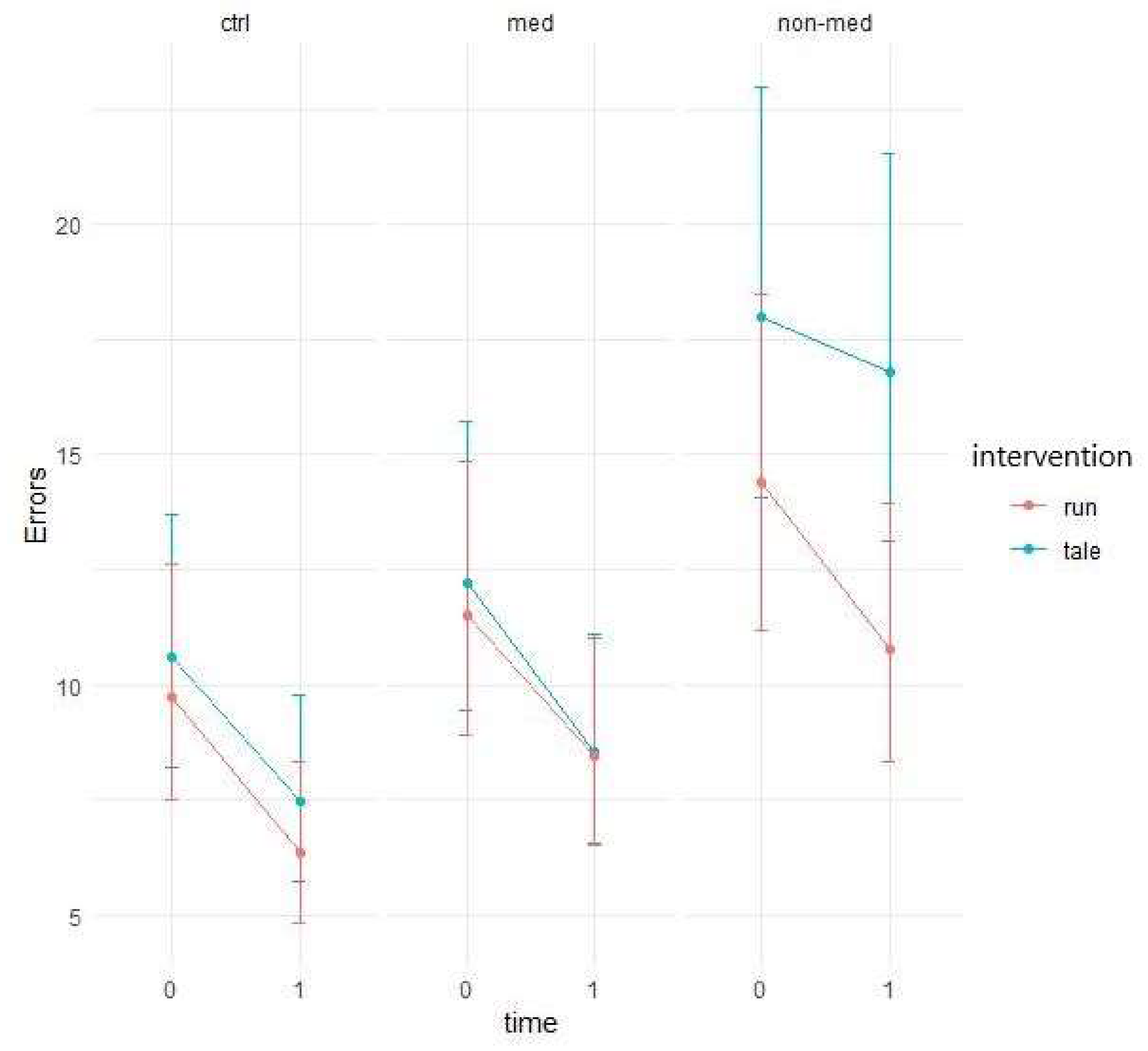
Total Error
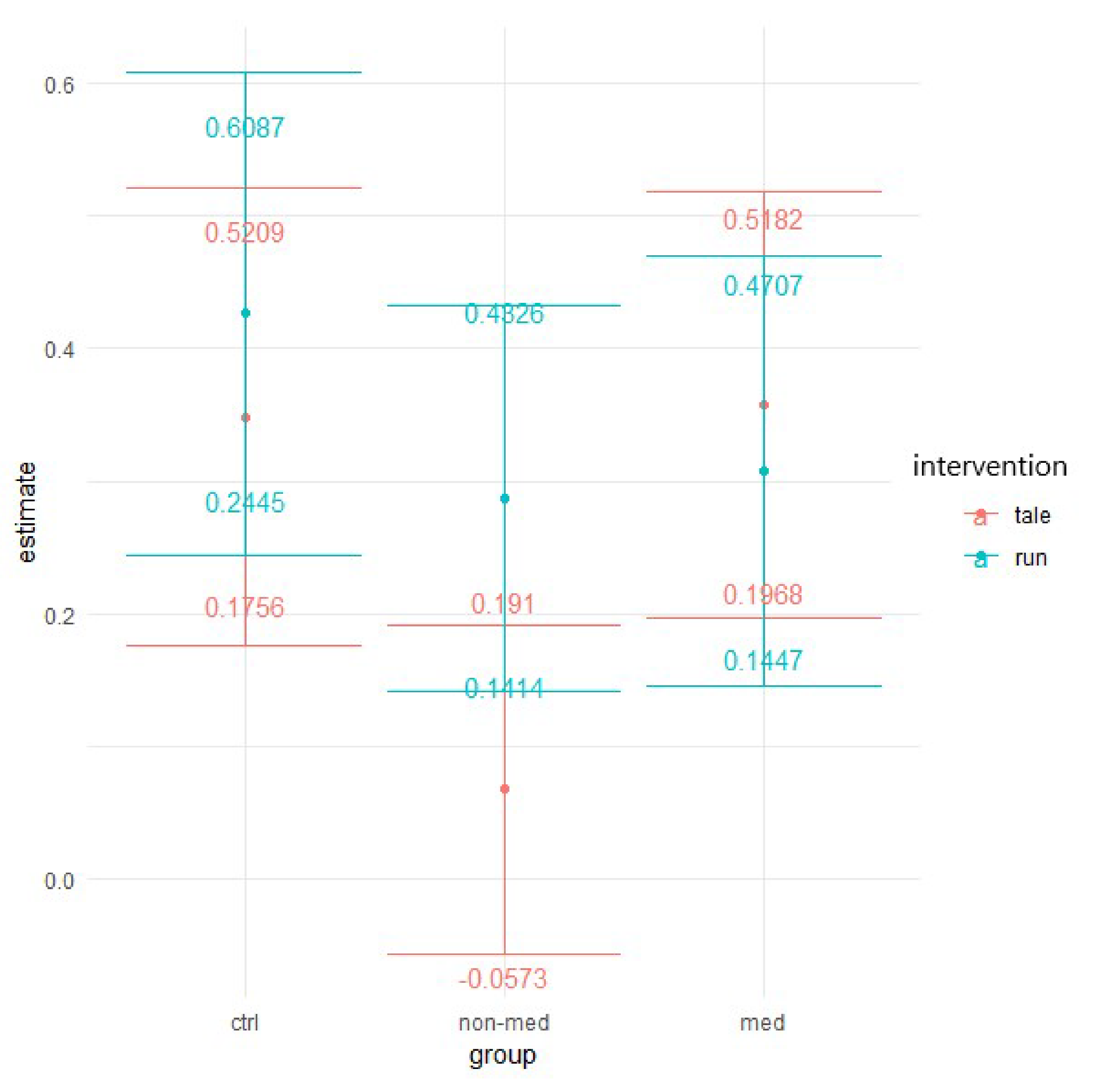
Errors with Distractor
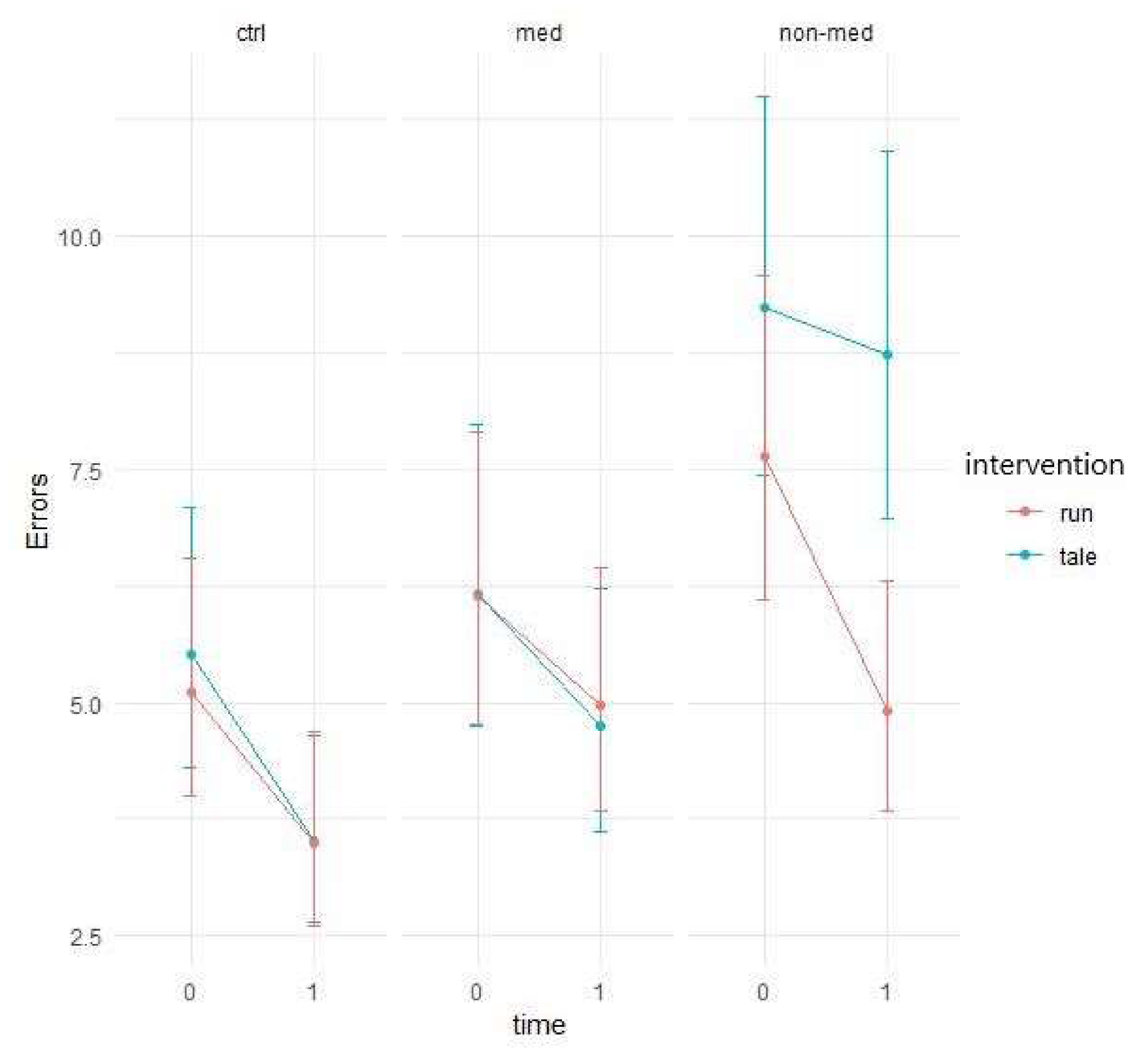
Errors without Distractor
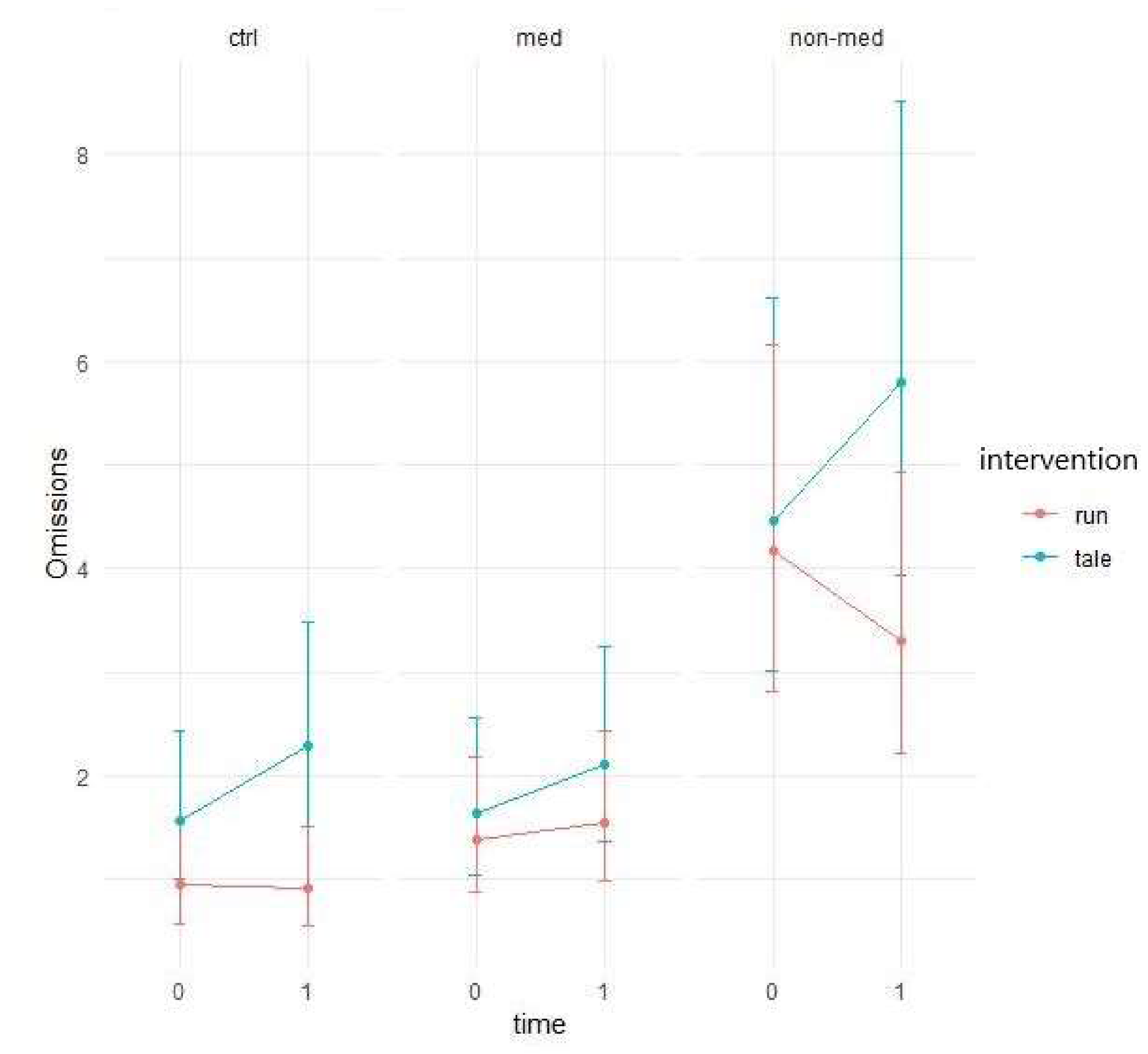
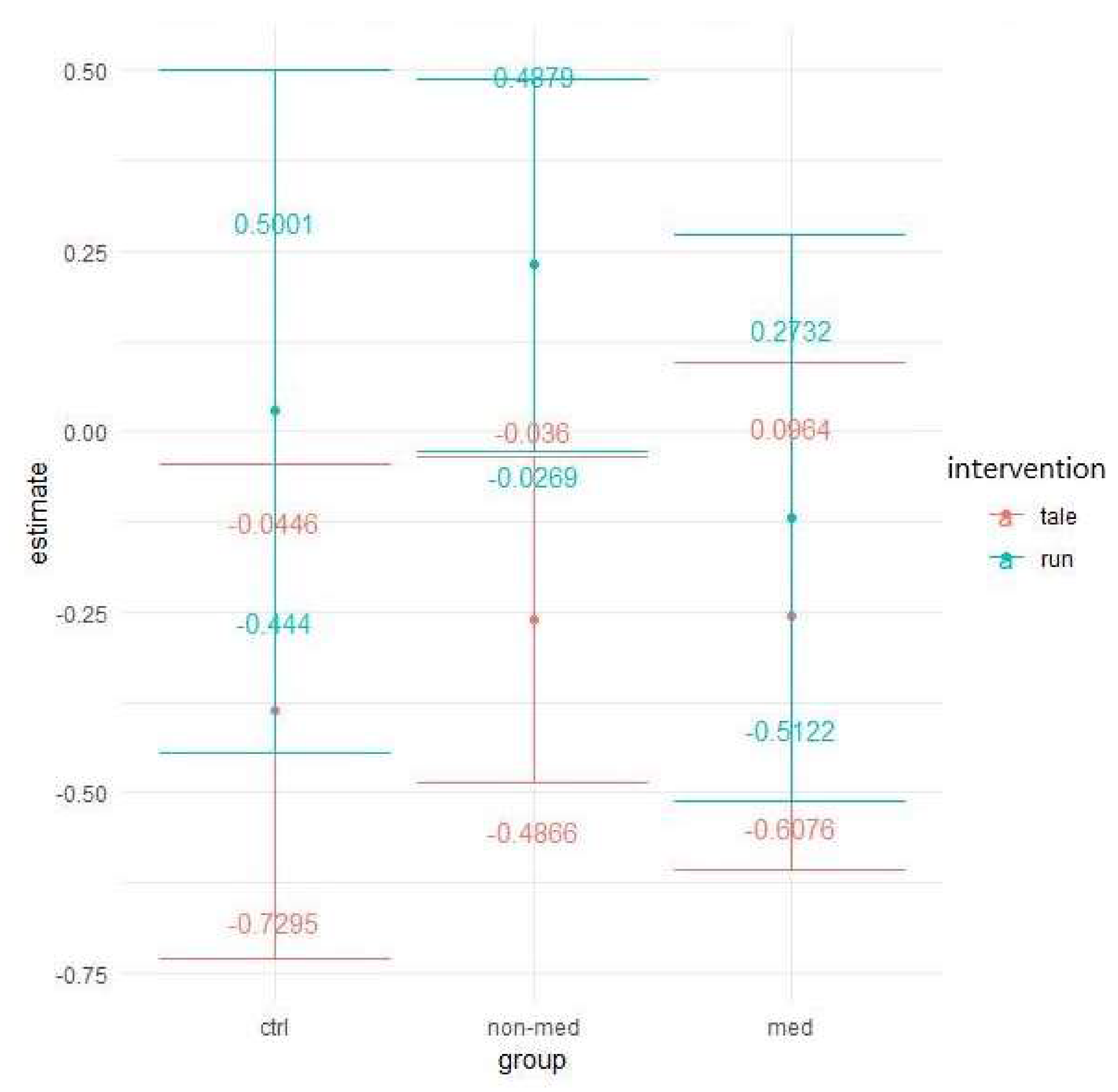
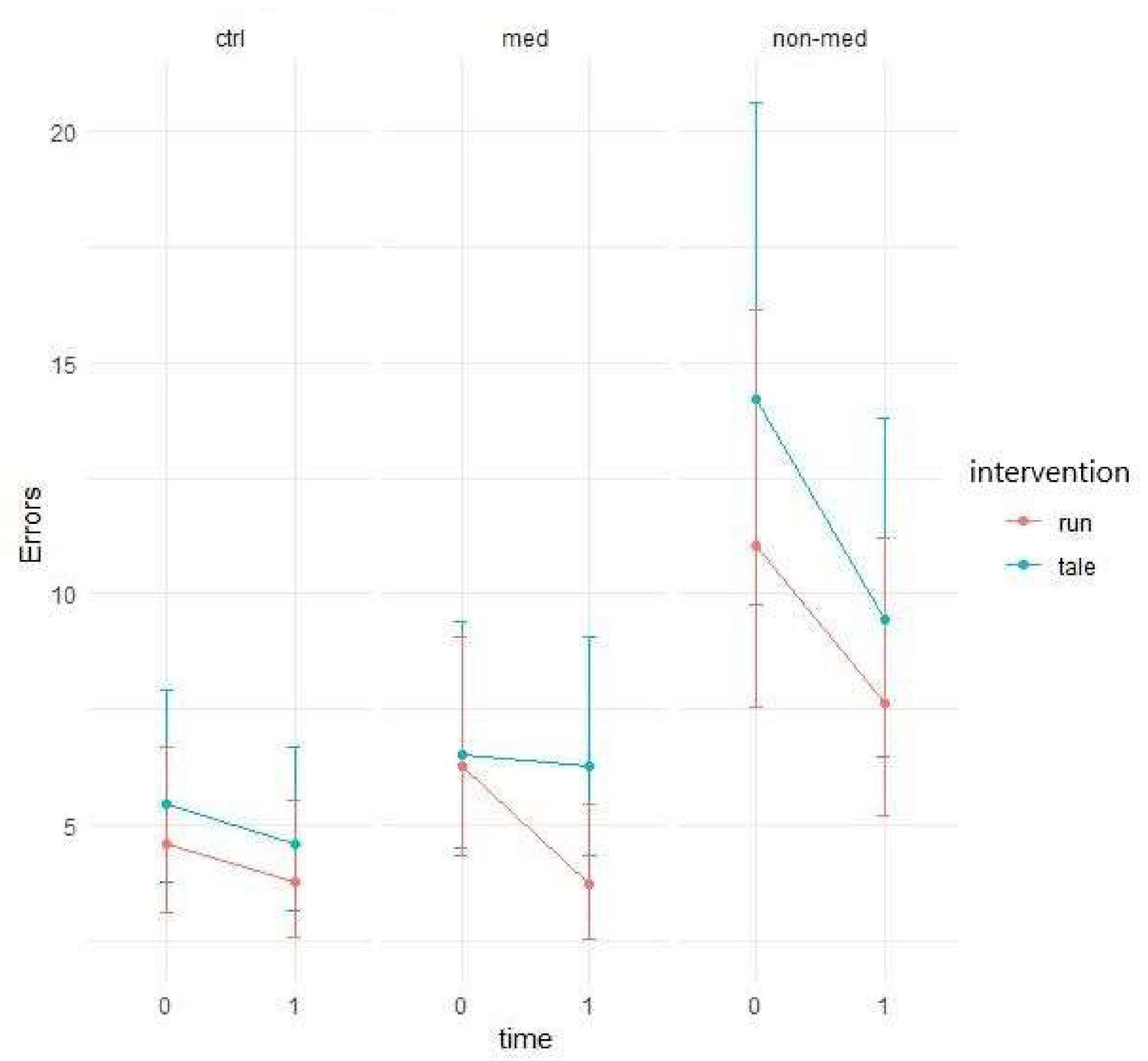
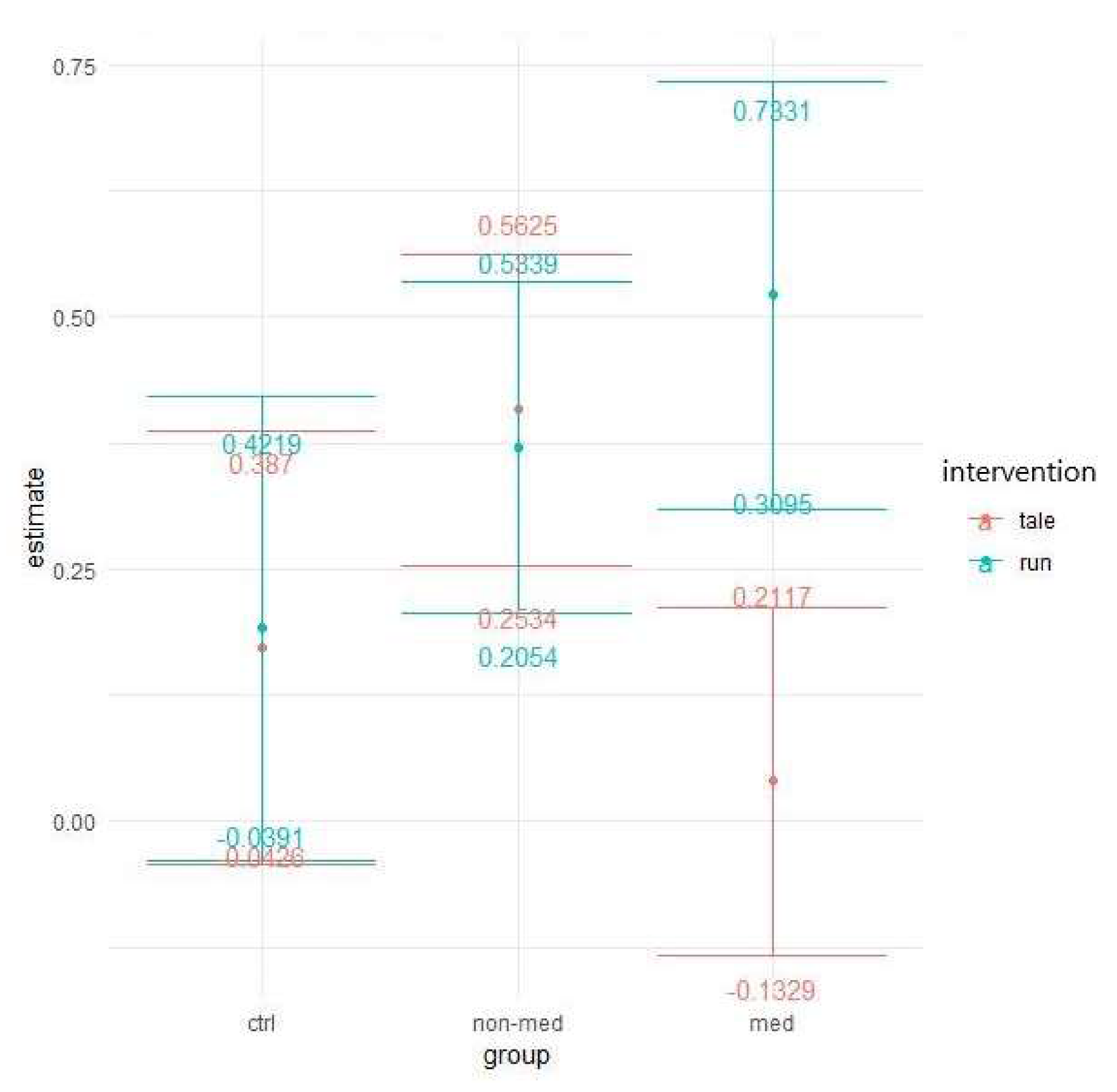
3.2.3. Divided Attention
Median of Reaction Time
Total Omissions
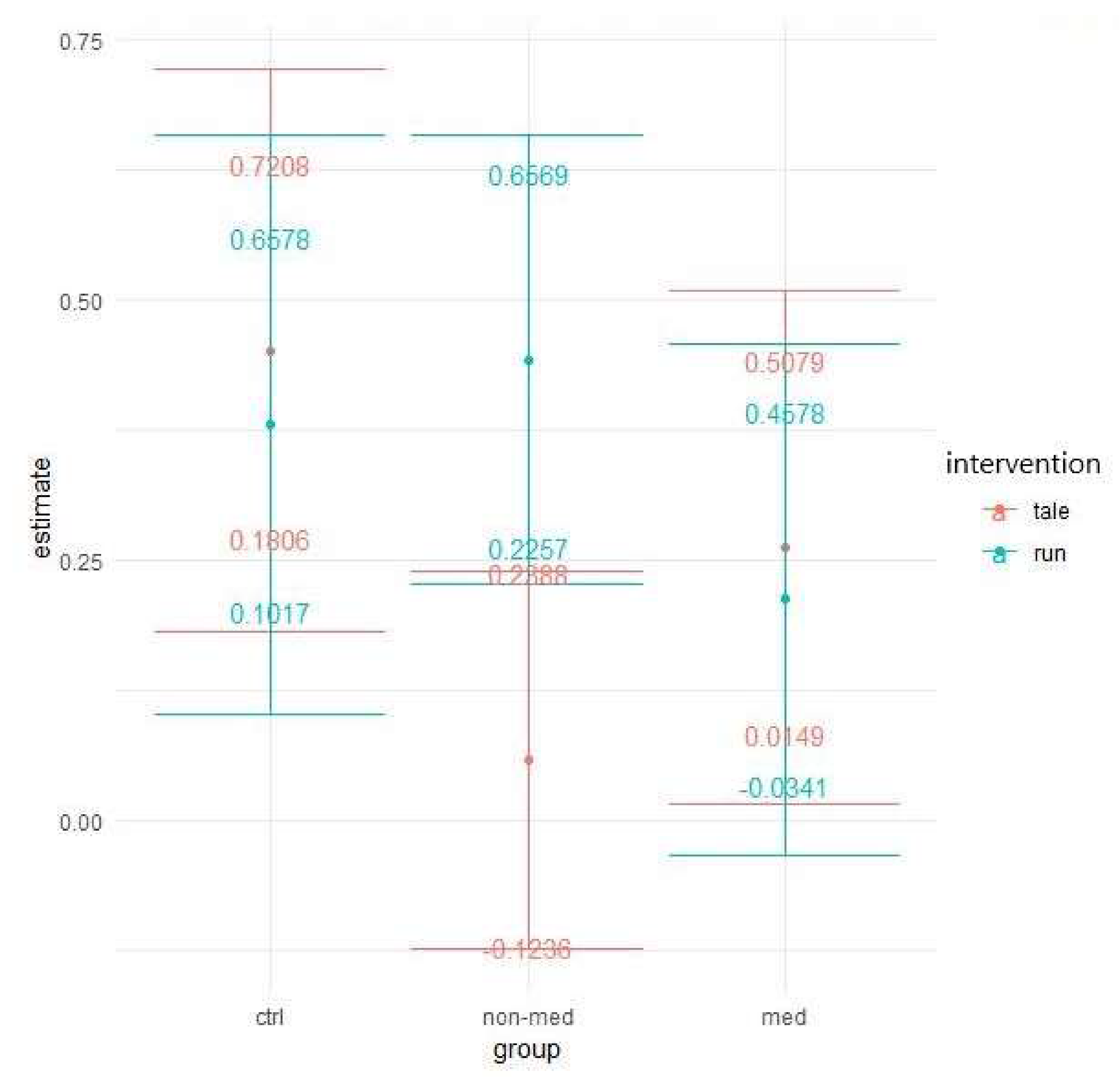
Total Error
3.2.4. Flexibility
Median of Reaction Time
Total Error
3.2.5. Go/No-Go
Median of Reaction Time
Total Error
4. Discussions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Greenhill, L.L. Diagnosing attention-deficit/hyperactivity disorder in children. J. Clin. Psychiatry 1998, 59, 31–41. [Google Scholar]
- Goldman, L.S.; Genel, M.; Bezman, R.J.; Slanetz, P.J. Diagnosis and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Council on Scientific Affairs, American Medical Association. JAMA 1998, 279, 1100–1107. [Google Scholar] [CrossRef]
- Brown, R.T.; Freeman, W.S.; Perrin, J.M.; Stein, M.T.; Amler, R.W.; Feldman, H.M.; Pierce, K.; Wolraich, M.L. Prevalence and Assessment of Attention-Deficit/Hyperactivity Disorder in Primary Care Setting. Pediatrics 2001, 107, E43. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; APA: Arlington, VA, USA, 2013. [Google Scholar]
- Cubillo, A.; Halari, R.; Smith, A.; Taylor, E.; Rubia, K. A review of fronto-striatal and fronto-cortical brain abnormalities in children and adults with Attention Deficit Hyperactivity Disorder (ADHD) and new evidence for dysfunction in adults with ADHD during motivation and attention. Cortex 2012, 48, 194–215. [Google Scholar] [CrossRef]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: A latent variable analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [Green Version]
- Lehto, J.E.; Juujärvi, P.; Kooistra, L.; Pulkkinen, L. Dimensions of executive functioning: Evidence from children. Br. J. Dev. Psychol. 2003, 21, 59–80. [Google Scholar] [CrossRef]
- Collins, A.; Koechlin, E. Reasoning, learning, and creativity: Frontal lobe function and human decision-making. PLoS Biol. 2012, 10, e1001293. [Google Scholar] [CrossRef]
- Lunt, L.; Bramham, J.; Morris, R.G.; Bullock, P.R.; Selway, R.P.; Xenitidis, K.; Davis, A.S. Prefrontal cortex dysfunction and “jumping to conclusions”: Bias or deficit? J. Neuropsychol. 2012, 6, 65–78. [Google Scholar] [CrossRef]
- Douglas, V.I. Cognitive control processes in Attention-Deficit/Hyperactivity Disorder. In Handbook of Disruptive Behavior Disorders; Quay, H.C., Hogan, A.E., Eds.; Kluwer Academic/Plenum Publishers: New York, NY, USA, 1991; pp. 105–138. [Google Scholar]
- Pennington, B.F.; Ozonoff, S. Executive functions and developmental psychopathology. J. Child Psychol. Psychiatry 1996, 37, 51–87. [Google Scholar] [CrossRef]
- Barkley, R.A. Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychol. Bull. 1997, 121, 65–94. [Google Scholar] [CrossRef] [Green Version]
- Levy, F. The dopamine theory of attention deficit hyperactivity disorder (ADHD). Aust. N. Z. J. Psychiatry 1991, 25, 277–283. [Google Scholar] [CrossRef]
- Sharma, A.; Couture, J. A review of the pathophysiology, etiology, and treatment of attention-deficit hyperactivity disorder (ADHD). Ann. Pharmacother. 2014, 48, 209–225. [Google Scholar] [CrossRef]
- Zuvekas, S.H.; Vitiello, B.; Norquist, G.S. Recent trends in stimulant medication use among U.S. children. Am. J. Psychiatry 2006, 163, 579–585. [Google Scholar] [CrossRef]
- Markowitz, J.S.; Straughn, A.B.; Patrick, K.S. Advances in the pharmacotherapy of attention-deficit-hyperactivity disorder: Focus on methylphenidate formulations. Pharmacotherapy 2003, 23, 1281–1299. [Google Scholar] [CrossRef]
- Greenhill, L.; Kollins, S.; Abikoff, H.; McCracken, J.; Riddle, M.; Swanson, J.; McGough, J.; Wigal, S.; Wigal, T.; Vitiello, B.; et al. Efficacy and safety of immediate-release methylphenidate treatment for preschoolers with ADHD. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 1284–1293. [Google Scholar] [CrossRef] [Green Version]
- Coghill, D.R.; Seth, S.; Pedroso, S.; Usala, T.; Currie, J.; Gagliano, A. Effects of methylphenidate on cognitive functions in children and adolescents with attention-deficit/hyperactivity disorder: Evidence from a systematic review and meta-analysis. Biol. Psychiatry 2014, 76, 603–615. [Google Scholar] [CrossRef]
- Kratochvil, C.J.; Milton, D.R.; Vaughan, B.S.; Greenhill, L.L. Acute Atomoxetine Treatment of Younger and Older Children With ADHD: A Meta-Analysis of Tolerability and Efficacy. Child Adolesc. Psychiatry Ment. Health 2008, 2, 25. [Google Scholar] [CrossRef] [Green Version]
- Ledbetter, M. Atomoxetine: A novel treatment for child and adult ADHD. Neuropsychiatr. Dis. Treat. 2006, 2, 455–466. [Google Scholar] [CrossRef] [Green Version]
- Wilens, T.E.; Newcorn, J.H.; Kratochvil, C.J.; Gao, H.; Thomason, C.K.; Rogers, A.K.; Feldman, P.D.; Levine, L.R. Long-Term Atomoxetine Treatment in Adolescents With Attention-Deficit/Hyperactivity Disorder. J. Pediatrics 2006, 149, 112–119. [Google Scholar] [CrossRef]
- Antshel, K.M.; Olszewski, A.K. Cognitive Behavioral Therapy for Adolescents with ADHD. Child Adolesc. Psychiatr. Clin. N. Am. 2014, 23, 825–842. [Google Scholar] [CrossRef]
- Xue, J.; Zhang, Y.; Huang, Y. A Meta-Analytic Investigation of the Impact of Mindfulness-Based Interventions on ADHD Symptoms. Medicine (Baltimore) 2019, 98, e15957. [Google Scholar] [CrossRef]
- Antshel, K.M.; Remer, R. Social Skills Training in Children With Attention Deficit Hyperactivity Disorder: A Randomized-Controlled Clinical Trial. J. Clin. Child Adolesc. Psychol. 2003, 32, 153–165. [Google Scholar] [CrossRef]
- Zwi, M.; Jones, H.; Thorgaard, C.; York, A.; Dennis, J.A. Parent Training Interventions for Attention Deficit Hyperactivity Disorder (ADHD) in Children Aged 5 to 18 Years. Cochrane Database Syst. Rev. 2011, 12, CD003018. [Google Scholar] [CrossRef]
- Jensen, P.S.; Hinshaw, S.P.; Swanson, J.M.; Greenhill, L.L.; Conners, C.K.; Arnold, L.E.; Abikoff, H.B.; Elliott, G.; Hechtman, L.; Hoza, B.; et al. Findings from the NIMH multimodal treatment study of ADHD (MTA): Implications and applications for primary care providers. J. Dev. Behav. Pediatrics 2001, 22, 60–73. [Google Scholar] [CrossRef]
- Pelham, W.E.; Fabiano, G.A. Evidence-based psychosocial treatments for attention deficit/hyperactivity disorder. J. Clin. Child Adolesc. Psychol. 2008, 37, 184–214. [Google Scholar] [CrossRef]
- Gapin, J.I.; Labban, J.D.; Bohall, S.C.; Wooten, J.S.; Chang, Y.K. Acute exercise is associated with specific executive functions in college students with ADHD: A preliminary study. J. Sport Health. Sci. 2015, 4, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Tsai, S.J. Attention-deficit hyperactivity disorder may be associated with decreased central brain-derived neurotrophic factor activity: Clinical and therapeutic implications. Med. Hypotheses 2007, 68, 896–899. [Google Scholar] [CrossRef]
- Arnsten, A.F. Fundamentals of attention-deficit/hyperactivity disorder: Circuits and pathways. J. Clin. Psychiatry 2006, 67, 7–12. [Google Scholar]
- Knaepen, K.; Goekint, M.; Heyman, E.M.; Meeusen, R. Neuroplasticity-exercise-induced response of peripherial brain-derived neurotrophic factor: A systematic review of experimental studies in human subjects. Sports Med. 2010, 40, 765–801. [Google Scholar] [CrossRef]
- Etnier, J.L.; Salazar, W.; Landers, D.M.; Petruzzello, S.J.; Han, M.; Nowell, P. The influence of physical fitness and exercise upon cognitive functioning: A meta-analysis. J. Sport Exerc. Psychol. 1997, 19, 249–277. [Google Scholar] [CrossRef] [Green Version]
- Brisswalter, J.; Collardeau, M.; René, A. Effects of acute physical exercise characteristics on cognitive performance. Sports Med. 2002, 32, 555–566. [Google Scholar] [CrossRef] [PubMed]
- Sibley, B.A.; Etnier, J.L. The relationship between physical activity and cognition in children: A meta-analysis. Pediatric Exerc. Sci. 2003, 15, 243–256. [Google Scholar] [CrossRef] [Green Version]
- Tomporowski, P.D. Effects of acute bouts of exercise on cognition. Acta Psychol. 2003, 112, 297–324. [Google Scholar] [CrossRef]
- Lambourne, K.; Tomporowski, P.D. The effect of exercise-induced arousal on cognitive task performance: A meta-regression analysis. Brain Res. 2010, 1341, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.K.; Labban, J.D.; Gapin, J.I.; Etnier, J.L. The effects of acute exercise on cognitive performance: A meta-analysis. Brain Res. 2012, 1453, 87–101. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.K.; Chu, I.H.; Chen, F.T.; Wang, C.C. Dose-response effect of acute resistance exercise on Tower of London in middle-aged adults. J. Sport Exerc. Psychol. 2011, 33, 866–883. [Google Scholar] [CrossRef]
- Chang, Y.K.; Tsai, C.L.; Hung, T.M.; So, E.C.; Chen, F.T.; Etnier, J.L. Effects of acute exercise on executive function: A study with a tower of london task. J. Sport Exerc. Psychol. 2011, 33, 847–865. [Google Scholar] [CrossRef] [Green Version]
- Verburgh, L.; Königs, M.; Scherder, E.J.; Oosterlaan, J. Physical exercise and executive functions in preadolescent children, adolescents and young adults: A meta-analysis. Br. J. Sports Med. 2013, 48, 973–979. [Google Scholar] [CrossRef] [Green Version]
- Best, J.R. Effects of Physical Activity on Children’s Executive Function: Contributions of Experimental Research on Aerobic Exercise. Dev. Rev. 2010, 30, 331–551. [Google Scholar] [CrossRef]
- Gapin, J.I.; Labban, J.D.; Etnier, J.L. The effects of physical activity on attention deficit hyperactivity disorder symptoms: The evidence. Prev. Med. 2011, 52, S70–S74. [Google Scholar] [CrossRef] [Green Version]
- Berwid, O.G.; Halperin, J.M. Emerging Support for a Role of Exercise in Attention-Deficit/Hyperactivity Disorder Intervention Planning. Curr. Psychiatry Rep. 2012, 14, 543–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halperin, J.M.; Berwid, O.G.; O’Neill, S. Healthy Body, Healthy Mind? The Effectiveness of Physical Activity to Treat ADHD in Children. Child Adolesc. Psychiatr. Clin. N. Am. 2014, 23, 899–936. [Google Scholar] [CrossRef] [PubMed]
- Grassman, V.; Alves, M.V.; Santos-Galduróz, R.F.; Galduróz, J.C.F. Possible Cognitive Benefits of Acute Physical Exercise in Children With ADHD: A Systematic Review. J. Atten. Disord. 2017, 21, 367–371. [Google Scholar] [CrossRef]
- Christiansen, L.; Beck, M.M.; Bilenberg, N.; Wienecke, J.; Astrup, A.; Lundbye-Jensen, J. Effects of Exercise on Cognitive Performance in Children and Adolescents with ADHD: Potential Mechanisms and Evidence-based Recommendations. J. Clin. Med. 2019, 8, 841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neudecker, C.; Mewes, N.; Reimers, A.K.; Woll, A. Exercise Interventions in Children and Adolescents With ADHD: A Systematic Review. J. Atten. Disord. 2019, 23, 307–324. [Google Scholar] [CrossRef] [PubMed]
- Craft, D.H. Effect of prior exercise on cognitive performance tasks by hyperactive and normal young boys. Percept. Mot. Ski. 1983, 56, 979–982. [Google Scholar] [CrossRef] [PubMed]
- Medina, J.A.; Netto, T.L.; Muszkat, M.; Medina, A.C.; Botter, D.; Orbetelli, R.; Scaramuzza, L.F.; Sinnes, E.G.; Vilela, M.; Miranda, M.C. Exercise impact on sustained attention of ADHD children, methylphenidate effects. Atten. Defic. Hyperact. Disord. 2010, 2, 49–58. [Google Scholar] [CrossRef]
- Chang, Y.K.; Liu, S.; Yu, H.H.; Lee, Y.H. Effect of acute exercise on executive function in children with attention deficit hyperactivity disorder. Arch. Clin. Neuropsychol. 2012, 27, 225–237. [Google Scholar] [CrossRef] [Green Version]
- Mahon, A.D.; Dean, R.S.; McIntosh, D.E.; Marjerrison, A.D.; Cole, A.S.; Woodruff, M.E.; Lee, M.P. Acute Exercise Effects on Measures of Attention and Impulsivity in Children with Attention Deficit/Hyperactivity Disorder. J. Educ. Dev. Psychol. 2013, 3, 65–73. [Google Scholar] [CrossRef]
- Pontifex, M.B.; Saliba, B.J.; Raine, L.B.; Picchietti, D.L.; Hillman, C.H. Exercise improves behavioral, neurocognitive, and schlastic performance in children with attention-deficit/hyperactivity disorder. J. Pediatrics 2013, 162, 543–551. [Google Scholar] [CrossRef] [Green Version]
- Piepmeier, A.T.; Shih, C.H.; Whedon, M.; Williams, L.M.; Davis, M.E.; Henning, D.A.; Park, S.; Calkins, S.D.; Etnier, J.L. The effect of acute exercise on cognitive performance in children with and without ADHD. J. Sport Health Sci. 2015, 4, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Hung, C.L.; Huang, C.J.; Tsai, Y.J.; Chang, Y.K.; Hung, T.M. Neuroelectric and Behavioral Effects of Acute Exercise on Task Switching in Children with Attention-Deficit/Hyperactivity Disorder. Front. Psychol. 2016, 7, 1589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ludyga, S.; Brand, S.; Gerber, M.; Weber, P.; Brotzmann, M.; Habibifar, F.; Pühse, U. An event-related potential investigation of the acute effects of aerobic and coordinative exercise on inhibitory control in children with ADHD. Dev. Cogn. Neurosci. 2017, 28, 21–28. [Google Scholar] [CrossRef]
- Ludyga, S.; Gerber, M.; Mücke, M.; Brand, S.; Weber, P.; Brotzmann, M.; Pühse, U. The Acute Effects of Aerobic Exercise on Cognitive Flexibility and Task-Related Heart Rate Variability in Children with ADHD and Healthy Controls. J. Atten. Disord. 2020, 24, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Miklós, M.; Futó, J.; Balázs, J. How Do Parents See? The Relationship between Sport Participation and Quality of Life among Boys with ADHD: A Cross-Sectional Study. Psychol. Behav. Sci. Int. J. 2019, 10, 555796. [Google Scholar] [CrossRef] [Green Version]
- Miklós, M.; Futó, J.; Komáromy, D.; Balázs, J. Executive function and Attention Performance in Children with ADHD: Effects of Medication and Comparison with Typically Developing Children. Int. J. Environ. Res. Public Health 2019, 16, 3822. [Google Scholar] [CrossRef] [Green Version]
- She, J.; Nakamura, H.; Makino, K.; Ohyama, Y.; Hashimoto, H. Selection of Suitable Maximum-heart-rate Formulas for Use with Karvonen Formula to Calculate Exercise Intensity. Int. J. Autom. Comput. 2015, 12, 62–69. [Google Scholar] [CrossRef]
- Riebe, D.; Ehrman, J.K.; Liguori, G.; Magal, M. Chapter 6 General Principles of Exercise Prescription. In ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; American College of Sports Medicine; Wolters Kluwer/Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2017; pp. 143–179. [Google Scholar]
- Lecrubier, Y.; Sheehan, D.V.; Weiller, E.; Amorim, P.; Bonora, I.; Sheehan, K.H.; Janavs, J.; Dunbar, G.C. The Mini International Neuropsychiatric Interview (MINI): A short diagnostic structured interview. Reliability and validity according to the CIDI. Eur. Psychiatry 1997, 12, 224–231. [Google Scholar] [CrossRef]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Janavs, J.; Weiller, E.; Keskiner, A.; Schinka, J.; Knapp, E.; Sheehan, M.F.; Dunbar, G.C. The validity of the Mini International Neuropsychiatric Interview (MINI) according to the SCID-P and its reliability. Eur. Psychiatry 1997, 12, 232–241. [Google Scholar] [CrossRef]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The MINI-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59, 22–33. [Google Scholar]
- Balázs, J.; Bíró, A.; Dálnoki, D.; Lefkovics, E.; Tamás, Z.; Nagy, P.; Gádoros, J. A gyermek M.I.N.I kérdőív magyar nyelvű változatának ismertetése [Introduction of the Hungarian version of the M.I.N.I Kid]. Psychiatr. Hung. 2004, 19, 358–364. [Google Scholar]
- Sheehan, D.V.; Sheehan, K.H.; Shytle, R.D.; Janavs, J.; Bannon, Y.; Rogers, J.E.; Milo, K.M.; Stock, S.L.; Wilkinson, B. Reliability and validity of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID). J. Clin. Psychiatry 2010, 71, 313–326. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR, 4th ed.; APA: Washington, DC, USA, 1994. [Google Scholar]
- Balázs, J.; Bitter, I.; Hideg, K.; Vitrai, J. A M.I.N.I. és a M.I.N.I. Plusz kérdőív magyar nyelvű változatának kidolgozása [The Hungarian version of the MINI and MINI Plus]. Psychiatr. Hung. 1998, 13, 160–168. [Google Scholar]
- Zimmermann, P.; Gondan, M.; Fimm, B. Test of Attentional Performance for Children, Version 1.5, Part 1—Description; Psychologische Testsysteme: Herzogenrath, Germany, 2005; Available online: http://www.psytest.net (accessed on 9 October 2019).
- Kaufmann, L.; Zieren, N.; Zotter, S.; Karall, D.; Scholl-Burgi, S.; Haberlandt, E.; Fimm, B. Predictive validity of attentional functions in differentiating children with and without ADHD: A componential analysis. Dev. Med. Child Neurol. 2010, 52, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 3rd ed.; Harper Collins College Publishers: New York, NY, USA, 1996. [Google Scholar]
- Benzing, V.; Chang, Y.; Schmidt, M. Acute Physical Activity Enhances Executive Functions in Children with ADHD. Sci. Rep. 2018, 8, 12382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Mourik, R.; Oosterlaan, J.; Heslenfeld, D.J.; Konig, C.E.; Sergeant, J.A. When distraction is not distracting: A behavioral and ERP study on distraction in ADHD. Clin. Neurophysiol. 2007, 118, 1855–1865. [Google Scholar] [CrossRef] [PubMed]
- Gumenyuk, V.; Korzyukov, O.; Escera, C.; Hämäläinen, M.; Huotilainen, M.; Häyrinen, T.; Oksanen, H.; Näätänen, R.; von Wendt, L.; Alho, K. Electrophysiological evidence of enhanced distractibility in ADHD children. Neurosci. Lett. 2005, 374, 212–217. [Google Scholar] [CrossRef]
- Adams, R.; Finn, P.; Moes, E.; Flannery, K.; Rizzo, A.S. Distractibility in Attention/Deficit/Hyperactivity Disorder (ADHD): The virtual reality classroom. Child Neuropsychol. 2009, 15, 120–135. [Google Scholar] [CrossRef]
- Fassbender, C.; Zhang, H.; Buzy, W.M.; Cortes, C.R.; Mizuiri, D.; Beckett, L.; Schweitzer, J.B. A lack of default network suppression is linked to increased distractibility in ADHD. Brain Res. 2009, 1273, 114–128. [Google Scholar] [CrossRef] [Green Version]
- Ross, P.; Randolph, J. Differences Between Students With and Without ADHD on Task Vigilance Under Conditions of Distraction. J. Educ. Res. Pract. 2014, 4, 1–10. [Google Scholar] [CrossRef]
- Elosúa, M.R.; Del Olmo, S.; Contreras, M.J. Differences in Executive Functioning in Children with Attention Deficit and Hyperactivity Disorder (ADHD). Front. Psychol. 2017, 8, 976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lajoie, G.; Anderson, V.; Anderson, P.; Tucker, A.R.; Robertson, I.H.; Manly, T. Effects of Methylphenidate on Attention Skills in Children with Attention Deficit/Hyperactivity disorder. Brain Impair. 2005, 6, 21–32. [Google Scholar] [CrossRef]
- Cepeda, N.J.; Cepeda, M.L.; Kramer, A.F. Task switching and attention deficit hyperactivity disorder. J. Abnorm. Child Psychol. 2000, 28, 213–226. [Google Scholar] [CrossRef] [PubMed]
- Willcutt, E.G.; Doyle, A.E.; Nigg, J.T.; Faraone, S.V.; Pennington, B.F. Validity of the Executive Function Theory of Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review. Biol. Psychiatry 2005, 57, 1336–1346. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lijffijt, M.; Kenemans, J.L.; Verbaten, M.N.; van Engeland, H. A meta-analytic review of stopping performance in attention-deficit/hyperactivity disorder: Deficient inhibitory motor control? J. Abnorm. Psychol. 2005, 114, 216–222. [Google Scholar] [CrossRef] [Green Version]
- Alderson, R.M.; Rapport, M.D.; Kofler, M.J. Attention-deficit/hyperactivity disorder and behavioral inhibition: A meta-analytic review of the stop-signal paradigm. J. Abnorm. Child Psychol. 2007, 35, 745–758. [Google Scholar] [CrossRef]
- Lipszyc, J.; Schachar, R. Inhibitory control and psychopathology: A meta-analysis of studies using the stop signal task. J. Int. Nerupsychol. Soc. 2010, 16, 1064–1076. [Google Scholar] [CrossRef]
- Skogan, A.H.; Zeiner, P.; Egeland, J.; Rohrer-Baumgartner, N.; Urnes, A.G.; Reichborn-Kjennerud, T.; Aase, H. Inhibition and working memory in young preschool children with symptoms of ADHD and/or oppositional-defiant disorder. Child Neuropsychol. 2014, 20, 607–624. [Google Scholar] [CrossRef]
- Wright, L.; Lipszyc, J.; Dupuis, A.; Thayapararajah, S.W.; Schachar, R. Response inhibition and psychopathology: A meta-analysis of go/no-go task performance. J. Abnorm. Psychol. 2014, 123, 429–439. [Google Scholar] [CrossRef]
- Rahmi, I.; Wimbarti, S. Inhibition in ADHD and non-ADHD children ages 6–12 years. Int. J. Res. Stud. Psychol. 2018, 7, 73–85. [Google Scholar] [CrossRef] [Green Version]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups Conditions | Non-Medicated Group (Number of Children) | Medicated Groups (Number of Children) | Control Group (Number of Children) |
|---|---|---|---|
| Exercise | 25 | 25 | 25 |
| Control | 25 | 25 | 25 |
| Sum | 50 | 50 | 50 |
| Variables | Non-Medicated Group n = 50 | Medicated Group n = 50 | Control Group n = 50 | F or Fischer’s Exact Test Value | p-Value |
|---|---|---|---|---|---|
| Age; mean (SD) | 8.26 (1.47) | 9.7 (1.78) | 8.68 (1.41) | F(2, 147) = 11.29 | p < 0.001 |
| Gender; persons (%) | 45 boys (90%) 5 girls (10%) | 47 boys (94%) 3 girls (6%) | 43 boys (86%) 7 girls (14%) | Fischer’s exact test = 1.75 | p > 0.05 (2-sided) |
| Residence; person (%) | Fischer’s exact test = 38.16 | p < 0.001 (2-sided) | |||
| Capital | 27 (54%) | 21 (42%) | 45 (90%) | ||
| Countryside city | 11 (22%) | 23 (46%) | 3 (6%) | ||
| Village | 12 (24%) | 6 (12%) | 1 (2%) | ||
| Countryside town | 0 (0%) | 0 (0%) | 1 (2%) | ||
| Accommodation; person (%) | Fischer’s exact test = 5.23 | p > 0.05 (2-sided) | |||
| Own parents | 46 (92%) | 47 (94%) | 50 (100%) | ||
| Adopted | 3 (6%) | 3 (6%) | 0 (0%) | ||
| Foster parents | 1 (2%) | 0 (0%) | 0 (0%) |
| KiTAP Subtests | Main Effects and Interactions | Df | F/χ2 Value | p-Value |
|---|---|---|---|---|
| Alertness | Median of reaction time | |||
| group | 2 | 3.76 | p < 0.05 | |
| time | 1 | 94.29 | p < 0.001 | |
| intervention: time | 1 | 3.51 | p > 0.05 (marginally) | |
| Variability of reaction time | ||||
| group | 2 | 14.17 | p < 0.001 | |
| time | 1 | 84.42 | p < 0.001 | |
| Distractibility | Total omissions | |||
| group | 2 | 20.03 | p < 0.001 | |
| Omissions with distractor | ||||
| group | 2 | 15.17 | p < 0.001 | |
| intervention | 1 | 3.66 | p > 0.05 (marginally) | |
| Omissions without distractor | ||||
| group | 2 | 16.88 | p < 0.001 | |
| Total error | ||||
| group | 2 | 20.86 | p < 0.001 | |
| time | 1 | 69.31 | p < 0.001 | |
| group: time | 2 | 8.87 | p < 0.05 | |
| Errors with distractor | ||||
| group | 2 | 10.64 | p < 0.01 | |
| time | 1 | 10.79 | p < 0.01 | |
| group: time | 2 | 5.97 | p > 0.05 (marginally) | |
| group: intervention: time | 2 | 5.18 | p > 0.05 (marginally) | |
| Errors without distractor | ||||
| group | 2 | 17.85 | p < 0.001 | |
| time | 1 | 33.62 | p < 0.001 | |
| group: time | 2 | 11.33 | p < 0.01 | |
| Divided attention | Median of reaction time | |||
| group | 2 | 12.8 | p < 0.001 | |
| time | 1 | 28.88 | p < 0.001 | |
| Total omissions | ||||
| group | 2 | 40.02 | p < 0.001 | |
| intervention | 1 | 6.34 | p < 0.05 | |
| time | 1 | 3.63 | p > 0.05 (marginally) | |
| intervention: time | 1 | 8.91 | p < 0.01 | |
| Total error | ||||
| group | 2 | 14.37 | p < 0.001 | |
| group: time | 2 | 10.07 | p < 0.01 | |
| group: intervention: time | 2 | 9 | p < 0.05 | |
| Flexibility | Median of reaction time | |||
| group | 2 | 4.56 | p < 0.05 | |
| time | 1 | 89.32 | p < 0.001 | |
| group: intervention | 2 | 2.93 | p > 0.05 (marginally) | |
| Total error | ||||
| group | 2 | 8.62 | p < 0.05 | |
| time | 1 | 16.5 | p < 0.001 | |
| Go/no-go | Median of reaction time | |||
| group | 2 | 2.73 | p > 0.05 (marginally) | |
| time | 1 | 6.06 | p < 0.05 | |
| group: time | 2 | 3.26 | p < 0.05 | |
| intervention: time | 1 | 3.86 | p > 0.05 (marginally) | |
| Total error | ||||
| group | 2 | 25.49 | p < 0.001 | |
| intervention | 1 | 4.98 | p < 0.05 | |
| time | 1 | 3.99 | p < 0.05 | |
| intervention: time | 1 | 3.6 | p > 0.05 (marginally) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miklós, M.; Komáromy, D.; Futó, J.; Balázs, J. Acute Physical Activity, Executive Function, and Attention Performance in Children with Attention-Deficit Hyperactivity Disorder and Typically Developing Children: An Experimental Study. Int. J. Environ. Res. Public Health 2020, 17, 4071. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114071
Miklós M, Komáromy D, Futó J, Balázs J. Acute Physical Activity, Executive Function, and Attention Performance in Children with Attention-Deficit Hyperactivity Disorder and Typically Developing Children: An Experimental Study. International Journal of Environmental Research and Public Health. 2020; 17(11):4071. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114071
Chicago/Turabian StyleMiklós, Martina, Dániel Komáromy, Judit Futó, and Judit Balázs. 2020. "Acute Physical Activity, Executive Function, and Attention Performance in Children with Attention-Deficit Hyperactivity Disorder and Typically Developing Children: An Experimental Study" International Journal of Environmental Research and Public Health 17, no. 11: 4071. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114071