Impact of the Burden of COVID-19 in Italy: Results of Disability-Adjusted Life Years (DALYs) and Productivity Loss

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Data
2.2. Models Parameters
2.3. Method of Estimating YLL and YLD
2.4. Method of Estimating DALY
2.5. Productivity Losses
3. Results
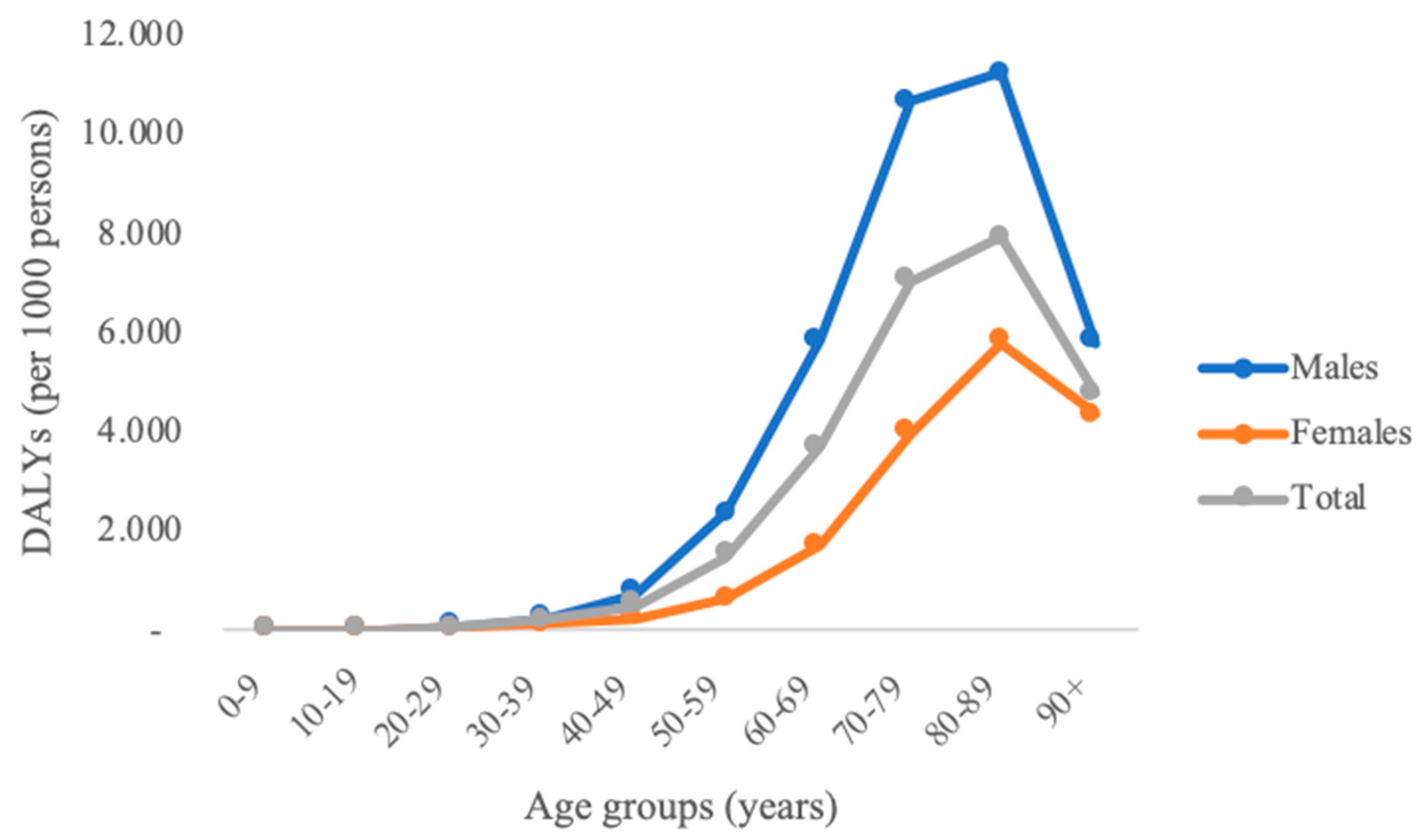
3.1. DALYs
3.2. Productivity Losses
4. Discussion
4.1. Main Implication
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ministero Della Salute. FAQ—Covid-19. Available online: http://www.salute.gov.it/portale/malattieInfettive/dettaglioFaqMalattieInfettive.jsp?lingua=italiano&id=228 (accessed on 4 May 2020).
- Mayo Clinic. Coronavirus Disease 2019 (COVID-19). Available online: https://www.mayoclinic.org/diseases-conditions/coronavirus/symptoms-causes/syc-20479963 (accessed on 4 May 2020).
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Situation Report—51. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_10 (accessed on 4 May 2020).
- Center for Systems Science and Engineering (CSSE) JHU (JHU). COVID-19 Dashboard. Available online: https://0-coronavirus-jhu-edu.brum.beds.ac.uk/map.html (accessed on 5 May 2020).
- Istituto Superiore di Sanità. ISS per COVID-19. Available online: https://www.iss.it/en/coronavirus (accessed on 5 May 2020).
- Decreto del Presidente del Consiglio dei Ministri 9 Marzo 2020. Ulteriori Disposizioni Attuative del Decreto-Legge 23 Febbraio 2020, n. 6, Recante Misure Urgenti in Materia di Contenimento e Gestione Dell’emergenza Epidemiologica da COVID-19, Applicabili Sull’intero Territorio Nazionale (20A01558). Available online: https://www.gazzettaufficiale.it/eli/id/2020/04/27/20A02352/sg (accessed on 5 May 2020).
- World Health Organization. Global Health Risks. 2009. Available online: http://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_full.pdf (accessed on 5 May 2020).
- Ungar, W.J.; Coyte, P.C. The pharmacy medication monitoring. Measuring productivity loss days in asthma patients. Health Econ. 2000, 9, 37–46. [Google Scholar] [CrossRef]
- Cancer Research Economics Support Team. Productivity Losses and How They are Calculated. 2016. Available online: http://www.crest.uts.edu.au/pdfs/Factsheet_ProductivityLoss_Nov2016.pdf (accessed on 6 May 2020).
- Murray, C.J.L.; Lopez, A.D.; World Health Organization; World Bank; Harvard School of Public Health. The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020, 1st ed.; Christopher, J.L., Alan, M., Lopez, D., Eds.; World Health Organization: Geneva, Switzerland, 1996; Available online: https://apps.who.int/iris/handle/10665/41864 (accessed on 6 May 2020).
- Gaunt, E.R.; Harvala, H.; McIntyre, C.; Templeton, K.E.; Simmonds, P. Disease burden of the most commonly detected respiratory viruses in hospitalized patients calculated using the disability adjusted life year (DALY) model. J. Clin. Virol. 2011, 52, 215–221. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Lopez, A.D. Quantifying disability: Data, methods and results. Bull. World Health Organ. 1994, 72, 481–494. [Google Scholar]
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2017 (GBD 2017) Disability Weights. 2018. Available online: http://ghdx.healthdata.org/record/ihme-data/gbd-2017-disability-weights (accessed on 6 May 2020).
- Pearce, A.M.; Hanly, P.; Timmons, A.; Walsh, P.M.; O’Neill, C.; O’Sullivan, E.; Gooberman-Hill, R.; Thomas, A.A.; Gallagher, P.; Sharp, L. Productivity losses associated with head and neck cancer using the human capital and friction cost approaches. Appl. Health Econ. Health Policy 2015, 13, 359–367. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 6 May 2020).
- Istituto Nazionale di Statistica (ISTAT). Condizioni di Vita, Reddito e Carico Fiscale Delle Famiglie. Available online: https://www.istat.it/it/archivio/236432 (accessed on 2 June 2020).
- Pearce, A.; Sharp, L.; Hanly, P.; Barchuk, A.; Bray, F.; de Camargo Cancela, M.; Gupta, P.; Meheus, F.; Qiao, Y.L.; Sitas, F.; et al. Productivity losses due to premature mortality from cancer in Brazil, Russia, India, China, and South Africa (BRICS): A population-based comparison. Cancer Epidemiol. 2018, 53, 27–34. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Italy—Old-Age Benefits. 2020. Available online: https://ec.europa.eu/social/main.jsp?catId=1116&langId=en&intPageId=4625 (accessed on 2 June 2020).
- World Health Organization. The Global Burden of Disease Concept. Quantifying Environ Health Impacts. 2002. Available online: https://www.who.int/quantifying_ehimpacts/publications/en/9241546204chap3.pdf (accessed on 7 May 2020).
- Mathers, C.D.; Salomon, J.A.; Ezzati, M.; Begg, S.; Vander Hoon, S.; Lopez, A.D. Sensitivity and uncertainty analyses for burden of disease and risk factor estimates. In Global Burden of Disease and Risk Factors; Intenernational Bank for Reconstruction and Development/The World Bank Group: Washington, DC, USA, 2006; pp. 399–426. [Google Scholar]
- Weisbrod, B.A. The valuation of human capital. J. Polit Econ. 1961, 69, 425–436. [Google Scholar] [CrossRef]
- Zhang, W.; Bansback, N.; Anis, A.H. Measuring and valuing productivity loss due to poor health: A critical review. Soc. Sci. Med. 2011, 72, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Istituto Superiore di Sanità. Epidemia COVID-19—Aggiornamento Nazionale 28 Aprile 2020. Available online: https://www.epicentro.iss.it/coronavirus/bollettino/Bollettino-sorveglianza-integrata-COVID-19_28-aprile-2020.pdf (accessed on 8 May 2020).
- Murray, C.J.L.; Lopez, A.D.; Jamison, D.T. The global burden of disease in 1990: Summary results, sensitivity analysis and future directions. Bull. World Health Organ. 1994, 72, 495–509. [Google Scholar] [PubMed]
- Troeger, C.; Forouzanfar, M.; Rao, P.C.; Khalil, I.; Brown, A.; Swartz, S.; Fullman, N.; Mosser, J.; Thompson, R.L.; Reiner, R.C., Jr.; et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect. Dis. 2017, 17, 1133–1161. [Google Scholar]
- Wenham, C.; Smith, J.; Morgan, R. COVID-19: The gendered impacts of the outbreak. Lancet 2020, 395, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Sharma, G.; Volgman, A.S.; Michos, E.D. Sex differences in mortality from COVID-19 pandemic: Are men vulnerable and women protected? JACC Case Rep. 2020, in press. [Google Scholar] [CrossRef]
- Wolff, J.L.; Starfield, B.; Anderson, G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch. Intern. Med. 2002, 162, 2269–2276. [Google Scholar] [CrossRef] [PubMed]
- Ssentongo, P.; Ssentongo, A.E.; Heilbrunn, E.S.; Chinchilli, V.M. The association of cardiovascular disease and other pre-existing comorbidities with COVID-19 mortality: A systematic review and meta-analysis. Medrxiv 2020, 6, 1–24. [Google Scholar]
- Istituto Superiore di Sanità. Caratteristiche dei Pazienti Deceduti Positivi All’infezione da SARS-CoV-2 in Italia. Available online: https://www.epicentro.iss.it/coronavirus/sars-cov-2-decessi-italia (accessed on 11 May 2020).
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Istituto Superiore di Sanità. Survey Nazionale sul Contagio COVID-19 Nelle Strutture Residenziali e Sociosanitarie TERZO REPORT. Available online: https://www.epicentro.iss.it/coronavirus/pdf/sars-cov-2-survey-rsa-rapporto-3.pdf (accessed on 11 May 2020).
- Logar, S. Care home facilities as new COVID-19 hotspots: Lombardy Region (Italy) case study. Arch. Gerontol. Geriatr. 2020, 89, 104087. [Google Scholar] [CrossRef] [PubMed]
- Putri, W.C.W.S.; Muscatello, D.J.; Stockwell, M.S.; Newall, A.T. Economic burden of seasonal influenza in the United States. Vaccine 2018, 36, 3960–3966. [Google Scholar] [CrossRef]
- Krishnamoorthy, K.; Harichandrakumar, K.T.; Kumari, A.K.; Das, L.K. Burden of Chikungunya in India: Estimates of disability adjusted life years (DALY) lost in 2006 epidemic. J. Vector Borne Dis. 2009, 46, 26–35. [Google Scholar] [PubMed]
- Steel, N.; Ford, J.A.; Newton, J.N.; Davis, A.C.J.; Vos, T.; Naghavi, M.; Glenn, S.; Hughes, A.; Dalton, A.M.; Stockton, D.; et al. Changes in health in the countries of the UK and 150 english local authority areas 1990–2016: A systematic analysis for the global burden of disease study 2016. Lancet 2018, 392, 1647–1661. [Google Scholar] [CrossRef] [Green Version]
- Hyder, A.A.; Liu, L.; Morrow, R.H.; Ghaffar, A. The Global Forum For. Health Research. Application of Burden of Disease Analyses in Developing Countries Implication for policy, Planning and Management; Global Forum for Health Research: Geneva, Switzerland, 2006; pp. 1–63. [Google Scholar]
- Knapp, M. Hidden costs of mental illness. Br. J. Psychiatry 2003, 183, 477–478. [Google Scholar] [CrossRef] [Green Version]
- Istituto Superiore di Sanità (ISS). Available online: https://www.iss.it/en/home (accessed on 11 May 2020).
- Istituto Nazionale di Statistica (ISTAT). Available online: https://www.istat.it/it/ (accessed on 11 May 2020).
- Istituto Nazionale della Previdenza Sociale (INPS). Available online: https://www.inps.it/nuovoportaleinps/home.htm (accessed on 11 May 2020).
- Ministero della Salute. Available online: http://www.salute.gov.it/portale/home.html (accessed on 11 May 2020).
- Ministero della Salute. Documento Relativo ai Criteri Per Sottoporre Soggetti Clinicamente Asintomatici alla Ricerca D’infezione da SARS-CoV-2 Attraverso Tampone Rino-Faringeo e Test Diagnostico. Available online: http://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2020&codLeg=73444&parte=1%20&serie=nullhttp://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2020&codLeg=73444&parte=1%20&serie=null (accessed on 12 May 2020).
- World Health Organization. Laboratory Testing for Coronavirus Disease 2019 (COVID-19) in Suspected Human Cases. Available online: https://apps.who.int/iris/handle/10665/331329 (accessed on 12 May 2020).
- World Health Organization. Considerations in the Investigation of Cases and Clusters of COVID-19. Available online: https://www.who.int/publications-detail/considerations-in-the-investigation-of-cases-and-clusters-of-covid-19 (accessed on 12 May 2020).
- Istituto Nazionale di Statistica & Istituto Superiore di Sanità. Impact of the Covid-19 Epidemic on the Total Mortality of the Resident Population in the First Quarter of 2020. Available online: https://www.istat.it/it/files//2020/05/Istat-ISS_-eng.pdf (accessed on 6 June 2020).
- Galea, S.; Merchant, R.M.; Lurie, N. The mental health consequences of COVID-19 and physical distancing. JAMA Intern. Med. 2020, 180, 817–818. [Google Scholar] [CrossRef] [Green Version]
- Zhu, H.; Rhee, J.-W.; Cheng, P.; Waliany, S.; Chang, A.; Witteles, R.M.; Maecker, H.; Davis, M.M.; Nguyen, P.K.; Wu, S.M. Correction to: Cardiovascular complications in patients with COVID-19: Consequences of viral toxicities and host immune response. Curr. Cardiol. Rep. 2020, 22, 1–9. [Google Scholar]
- Oxley, T.J.; Mocco, J.; Majidi, S.; Kellner, C.P.; Shoirah, H.; Singh, I.P.; Leacy, R.A.D.; Shigematsu, T.; Ladner, T.R.; Yaeger, K.A.; et al. Large-vessel stroke as a presenting feature of covid-19 in the young. N. Engl. J. Med. 2020, 382, e60. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention. Guidance for Discharge and Ending Isolation in the Context of Widespread Community Transmission of COVID-19-First Update. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/covid-19-guidance-discharge-and-ending-isolation-first%20update.pdf (accessed on 12 May 2020).



{kind=link}
{kind=link}
| Age Group | Total YLL, YLD, and DALY for Males | Total YLL, YLD, and DALY for Females | ||||
|---|---|---|---|---|---|---|
| YLL | YLD | DALY | YLL | YLD | DALY | |
| 0–9 | 36.28 | 1.78 | 38 | 36.48 | 1.55 | 38 |
| 10–19 | 0.00 | 6.13 | 6 | 0.00 | 6.15 | 6 |
| 20–29 | 197.39 | 24.86 | 222 | 66.49 | 32.36 | 99 |
| 30–39 | 863.04 | 35.18 | 898 | 466.14 | 42.66 | 509 |
| 40–49 | 3479.70 | 49.30 | 3529 | 1192.04 | 66.57 | 1259 |
| 50–59 | 10,749.30 | 63.52 | 10,813 | 3016.28 | 70.07 | 3086 |
| 60–69 | 20,507.93 | 50.13 | 20,558 | 6476.51 | 31.98 | 6508 |
| 70–79 | 29,000.47 | 40.32 | 29,041 | 12,894.20 | 28.48 | 12,923 |
| 80–89 | 15,671.33 | 25.95 | 15,697 | 12,497.19 | 35.21 | 12,532 |
| 90+ Total | 1212.48 81,718 | 5.00 302 | 1217 82,020 | 2450.85 39,096 | 17.52 333 | 2468 39,429 |
| Age Group | Number of Adjusted Cases * | Individual Cost of TPL | Total Cost of TPL |
|---|---|---|---|
| 20–29 | 10,369 | EUR 802.40 | EUR 8,320,085.60 |
| 30–39 | 14,858 | EUR 919.20 | EUR 13,657,473.60 |
| 40–49 | 25,420 | EUR 919.20 | EUR 23,366,064.00 |
| 50–59 | 35,068 | EUR 962.40 | EUR 33,749,443.20 |
| 60–69 | 25,153 | EUR 962.40 | EUR 24,207,247.20 |
| Total | 110,868 | EUR 103,300,313.60 |
| Age Group | Number of Deaths | Individual Cost of PPL | Total Cost of PPL | Total Cost of PPL as% of GDP |
|---|---|---|---|---|
| 20–29 | 8 | EUR 198,617.16 | EUR 1,588,937.30 | 0.0009 |
| 30–39 | 49 | EUR 200,515.55 | EUR 9,825,261.95 | 0.0055 |
| 40–49 | 224 | EUR 164,212.36 | EUR 36,783,568.10 | 0.0206 |
| 50–59 | 918 | EUR 120,848.52 | EUR 110,938,945.80 | 0.0621 |
| 60–69 | 2727 | EUR 52,199.42 | EUR 142,347,805.00 | 0.0796 |
| Total | 3926 | EUR 301,484,518.15 | 0.1686 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nurchis, M.C.; Pascucci, D.; Sapienza, M.; Villani, L.; D’Ambrosio, F.; Castrini, F.; Specchia, M.L.; Laurenti, P.; Damiani, G. Impact of the Burden of COVID-19 in Italy: Results of Disability-Adjusted Life Years (DALYs) and Productivity Loss. Int. J. Environ. Res. Public Health 2020, 17, 4233. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124233
Nurchis MC, Pascucci D, Sapienza M, Villani L, D’Ambrosio F, Castrini F, Specchia ML, Laurenti P, Damiani G. Impact of the Burden of COVID-19 in Italy: Results of Disability-Adjusted Life Years (DALYs) and Productivity Loss. International Journal of Environmental Research and Public Health. 2020; 17(12):4233. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124233
Chicago/Turabian StyleNurchis, Mario Cesare, Domenico Pascucci, Martina Sapienza, Leonardo Villani, Floriana D’Ambrosio, Francesco Castrini, Maria Lucia Specchia, Patrizia Laurenti, and Gianfranco Damiani. 2020. "Impact of the Burden of COVID-19 in Italy: Results of Disability-Adjusted Life Years (DALYs) and Productivity Loss" International Journal of Environmental Research and Public Health 17, no. 12: 4233. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124233