Neurodevelopmental Trajectories of Preterm Infants of Italian Native-Born and Migrant Mothers and Role of Neonatal Feeding

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedures
2.2. Outcome Measures
2.3. Socio-Demographic and Clinical Variables
2.4. Statistical Analyses
3. Results
3.1. Characteristics of the Study Sample
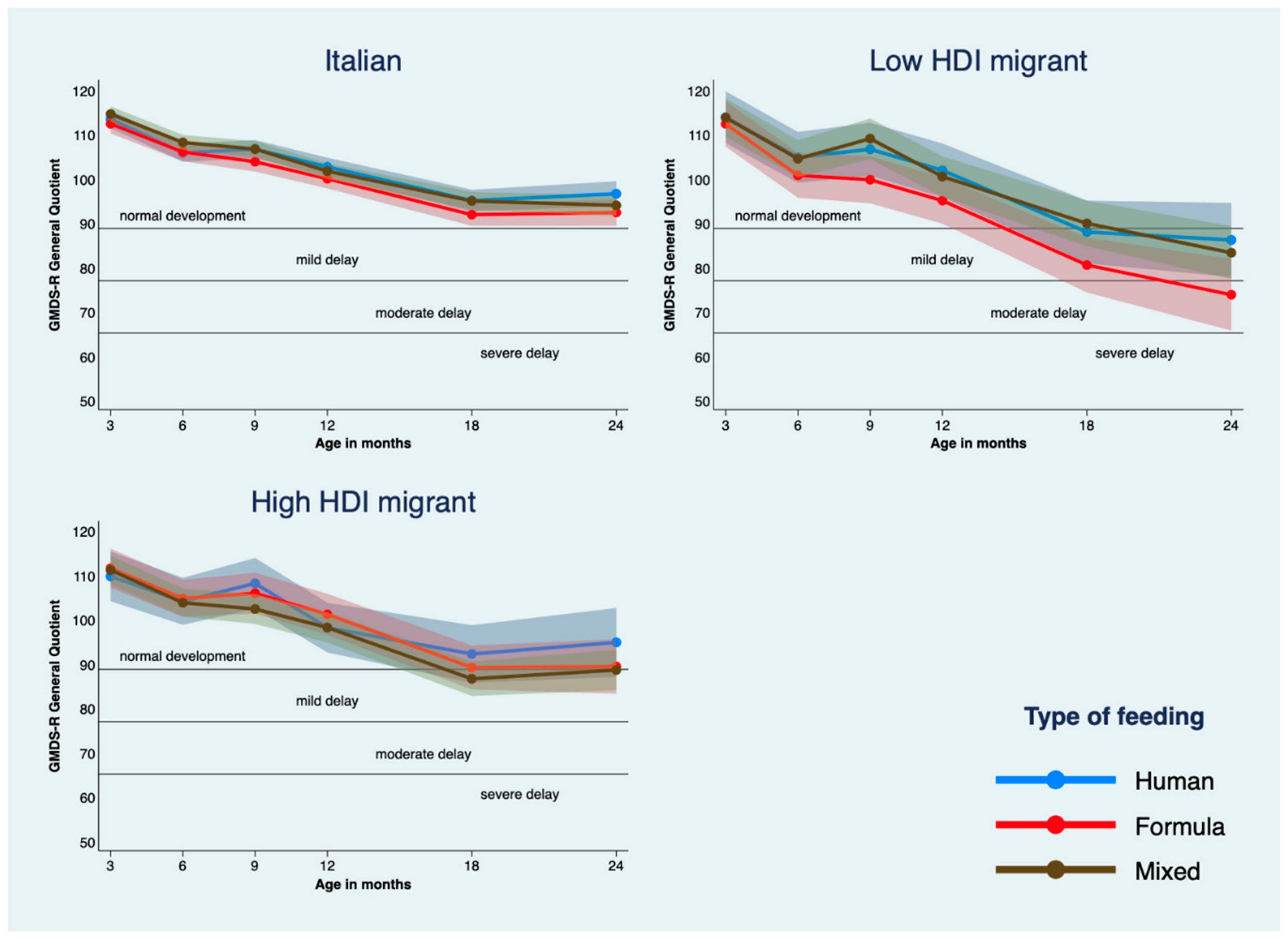
3.2. Empirical Neurodevelopmental Trajectories According to HDI and Diet
3.3. Estimated Neurodevelopmental Trajectories According to HDI and Diet
4. Discussion
Limitations and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Sansavini, A.; Guarini, A.; Caselli, M.C. Preterm birth: Neuropsychological profiles and atypical developmental pathways. Dev. Disabil. Res. Rev. 2011, 17, 102–113. [Google Scholar] [CrossRef] [PubMed]
- Limperopoulos, C.; Soul, J.S.; Gauvreau, K.; Huppi, P.S.; Warfield, S.K.; Bassan, H.; Robertson, R.L.; Volpe, J.J.; du Plessis, A.J. Late gestation cerebellar growth is rapid and impeded by premature birth. Pediatrics 2005, 115, 688–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibertoni, D.; Corvaglia, L.; Vandini, S.; Rucci, P.; Savini, S.; Alessandroni, R.; Sansavini, A.; Fantini, M.P.; Faldella, G. Positive effect of human milk feeding during NICU hospitalization on 24 month neurodevelopment of Very Low Birth Weight infants: An Italian cohort study. PLoS ONE 2015, 10, e0116552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Academy of Pediatrics. Breastfeeding and the Use of Human Milk. Pediatrics 2012, 129, e827–e841. [Google Scholar] [CrossRef] [Green Version]
- Lechner, B.E.; Vohr, B.R. Neurodevelopmental outcomes of preterm infants fed human milk. Clin. Perinatol. 2017, 44, 69–83. [Google Scholar] [CrossRef]
- Gu, H.; Wang, L.; Liu, L.; Luo, X.; Wang, J.; Hou, F.; Nkomola, P.D.; Li, J.; Liu, G.; Meng, H.; et al. A gradient relationship between low birth weight and IQ: A meta-analysis. Sci. Rep. 2017, 7, 18035. [Google Scholar] [CrossRef] [Green Version]
- Anstey, E.H.; Chen, J.; Elam-Evans, L.D.; Perrine, C.G. Racial and Geographic Differences in Breastfeeding —United States, 2011–2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 723–727. [Google Scholar] [CrossRef]
- Zakarija-Grković, I.; Šegvić, O.; Vučković Vukušić, A.; Lozančić, T.; Božinović, T.; Ćuže, A.; Burmaz, T. Predictors of suboptimal breastfeeding: An opportunity for public health interventions. Eur. J. Public Health 2016, 26, 282–289. [Google Scholar] [CrossRef] [Green Version]
- Kramer, M.R.; Hogue, C.R. What causes racial disparities in very preterm birth? A biosocial perspective. Epidemiol. Rev. 2009, 31, 84–98. [Google Scholar] [CrossRef]
- Anderson, F.M.; Hatch, S.L.; Comacchio, C.; Howard, L.M. Prevalence and risk of mental disorders in the perinatal period among migrant women: A systematic review and meta-analysis. Arch. Womens Ment. Health 2017, 20, 449–462. [Google Scholar] [CrossRef] [Green Version]
- Lehti, V.; Chudal, R.; Suominen, A.; Gissler, M.; Sourander, A. Association between immigrant background and ADHD: A nationwide population-based case-control study. J. Child Psychol. Psychiatry 2016, 57, 967–975. [Google Scholar] [CrossRef] [PubMed]
- Vohr, B.R.; Davis, E.P.; Wanke, C.A.; Krebs, N.F. Neurodevelopment: The impact of nutrition and inflammation during preconception and pregnancy in low-resource settings. Pediatrics 2017, 139 (Suppl. 1), S38–S49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mwaniki, M.K.; Atieno, M.; Lawn, J.E.; Newton, C.R.J.C. Long-term neurodevelopmental outcomes after intrauterine and neonatal insults: A systematic review. Lancet 2012, 379, 445–452. [Google Scholar] [CrossRef] [Green Version]
- Linsell, L.; Malouf, R.; Morris, J.; Kurinczuk, J.J.; Marlow, N. Prognostic factors for poor cognitive development in children born very preterm or with very low birth weight. JAMA Pediatr. 2015, 169, 1162–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyle, L.W.; Cheong, J.L.Y.; Burnett, A.; Roberts, G.; Lee, K.J.; Anderson, P.J. Biological and Social Influences on Outcomes of Extreme-Preterm/Low-Birth Weight Adolescents. Pediatrics 2015, 136, e1513–e1520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sansavini, A.; Savini, S.; Guarini, A.; Broccoli, S.; Alessandroni, R.; Faldella, G. The effect of gestational age on developmental outcomes: A longitudinal study in the first 2 years of life. Child Care Health Dev. 2011, 37, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Marlow, N.; Wolke, D.; Bracewell, M.A.; Samara, M. Neurologic and developmental disability at six years of age after extremely preterm birth. N. Engl. J. Med. 2005, 352, 9–19. [Google Scholar] [CrossRef]
- Putnick, D.L.; Bornstein, M.H.; Eryigit-Madzwamuse, S.; Wolke, D. Long-term stability of language performance in very preterm, moderate-late preterm, and term children. J. Pediatr. 2017, 181, 74–79. [Google Scholar] [CrossRef] [Green Version]
- Mangin, K.S.; Horwood, L.J.; Woodward, L.J. Cognitive Development Trajectories of Very Preterm and Typically Developing Children. Child Dev. 2016, 88, 282–298. [Google Scholar] [CrossRef]
- Luu, T.M.; Vohr, B.R.; Allan, W.; Schneider, K.C.; Ment, L.R. Evidence for catch-up in cognition and receptive vocabulary among adolescents born very preterm. Pediatrics 2011, 128, 313–322. [Google Scholar] [CrossRef]
- Linsell, L.; Johnson, S.; Wolke, D.; O’Reilly, H.; Morris, J.K.; Kurinczuk, J.J.; Marlow, N. Cognitive trajectories from infancy to early adulthood following birth before 26 weeks of gestation: A prospective, population-based cohort study. Arch. Dis. Child. 2018, 103, 363–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herich, L.C.; Cuttini, M.; Croci, I.; Franco, F.; Di Lallo, D.; Baronciani, D.; Fares, K.; Gargano, G.; Raponi, M.; Zeitlin, J. Maternal Education Is Associated with Disparities in Breastfeeding at Time of Discharge but Not at Initiation of Enteral Feeding in the Neonatal Intensive Care Unit. J. Pediatr. 2017, 182, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, R. The Griffiths Mental Development Scales from Birth to Two Years, Manual; Association for Research in Infant and Child Development, Test Agency: Henley-on-Thames, UK, 1996. [Google Scholar]
- Juárez, S.P.; Hjern, A. The weight of inequalities: Duration of residence and offspring’s birthweight among migrant mothers in Sweden. Soc. Sci. Med. 2017, 175, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Bertino, E.; Spada, E.; Occhi, L.; Coscia, A.; Giuliani, F.; Gagliardi, L.; Gilli, G.; Bona, G.; Fabris, C.; De Curtis, M.; et al. Neonatal anthropometric charts: The Italian neonatal study compared with other European studies. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 353–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papile, L.A.; Burstein, J.; Burstein, R.; Koffler, H. Incidence and evolution of subependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1500 gm. J. Pediatr. 1978, 92, 529–534. [Google Scholar] [CrossRef]
- Klein, D. MIMRGNS: Stata Module to Run Margins after mi Estimate. Available online: https://ideas.repec.org/c/boc/bocode/s457795.html (accessed on 22 June 2020).
- Jann, B. COEFPLOT: Stata Module to Plot Regression Coefficients and Other Results. Available online: https://ideas.repec.org/c/boc/bocode/s457686.html (accessed on 22 June 2020).
- Patra, K.; Hamilton, M.; Johnson, T.J.; Greene, M.; Dabrowski, E.; Meier, P.P.; Patel, A.L. NICU Human Milk Dose and 20-Month Neurodevelopmental Outcome in Very Low Birth Weight Infants. Neonatology 2017, 112, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Belfort, M.B.; Anderson, P.J.; Nowak, V.A.; Lee, K.J.; Molesworth, C.; Thompson, D.K.; Doyle, L.W.; Inder, T.E. Breast Milk Feeding, Brain Development, and Neurocognitive Outcomes: A 7-Year Longitudinal Study in Infants Born at Less Than 30 Weeks’ Gestation. J. Pediatr. 2016, 177, 133–139. [Google Scholar] [CrossRef] [Green Version]
- Wong, H.S.; Edwards, P. Nature or nurture: A systematic review of the effect of socio-economic status on the developmental and cognitive outcomes of children born preterm. Matern. Child Health J. 2013, 17, 1689–1700. [Google Scholar] [CrossRef]
- van Veen, S.; Remmers, S.; Aarnoudse-Moens, C.S.; Oosterlaan, J.; van Kaam, A.H.; van Wassenaer-Leemhuis, A.G. Multilingualism was associated with lower cognitive outcomes in children who were born very and extremely preterm. Acta Paediatr. 2019, 108, 479–485. [Google Scholar] [CrossRef] [Green Version]
- Bornstein, M.H.; Hahn, C.-S.; Suwalsky, J.T.D. Physically developed and exploratory young infants contribute to their own long-term academic achievement. Psychol. Sci. 2013, 24, 1906–1917. [Google Scholar] [CrossRef] [Green Version]
- Zuccarini, M.; Guarini, A.; Savini, S.; Iverson, J.M.; Aureli, T.; Alessandroni, R.; Faldella, G.; Sansavini, A. Object exploration in extremely preterm infants between 6 and 9 months and relation to cognitive and language development at 24 months. Res. Dev. Disabil. 2017, 68, 140–152. [Google Scholar] [CrossRef] [PubMed]
- Keller, H. Cultures of Infancy; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2007. [Google Scholar]
- Paradis, J.; Genesee, F.; Crago, M.B. Dual Language Development & Disorders: A Handbook on Bilingualism & Second Language Learning, 2nd ed.; Brookes Publishing: Baltimore, MD, USA, 2011; ISBN 978-1-59857-058-8. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Italy (n = 384) | High HDI (n = 87) | Low HDI (n = 59) | Test (p-Value) | Significant Post-Hoc Comparisons at p = 0.017 |
|---|---|---|---|---|---|
| Maternal characteristics | |||||
| Age (n = 529) mean ± SD | 34.9 ± 5.2 | 31.9 ± 6.1 | 30.1 ± 5.8 | 27.3; <0.001 * | Italy > High HDI, Low HDI |
| Education (n = 527) | 27.1; <0.001 # | ||||
| Low n (%) | 57 (14.9) | 19 (22.1) | 23 (39.0) | Low HDI > Italy, High HDI | |
| Middle n (%) | 174 (45.6) | 45 (52.3) | 26 (44.1) | ||
| High n (%) | 151 (39.5) | 22 (25.6) | 10 (16.9) | Low HDI < Italy | |
| Working condition (n = 529) | <0.001 $ | ||||
| Employed n (%) | 350 (91.4) | 53 (60.9) | 26 (44.1) | Italy > High HDI, Low HDI | |
| Unemployed n (%) | 8 (2.1) | 6 (6.9) | 3 (5.1) | Italy < High HDI, Low HDI | |
| Student n (%) | 8 (2.1) | 5 (5.7) | 2 (3.4) | Italy < High HDI | |
| Housewife n (%) | 17 (4.4) | 23 (26.4) | 28 (47.5) | Italy < High HDI < Low HDI | |
| Smoker (n = 423) | 35 (11.7) | 13 (16.9) | 6 (13.0) | 1.50; 0.472 # | |
| Maternal social risk score (n = 529) mean ± SD | 0.37 ± 0.60 | 0.70 ± 0.82 | 1.05 ± 0.84 | 35.5; <0.001 § | Italy < High HDI < Low HDI |
| Neonatal characteristics | |||||
| Sex (females) n (%) | 191 (49.7) | 44 (50.6) | 35 (59.3) | 1.9; 0.390 # | |
| Weight at birth (gr.) mean ± SD | 1173 ± 340 | 1163 ± 329 | 1086 ± 305 | 1.7; 0.178 * | |
| Gestational age (weeks) mean ± SD | 29.2 ± 2.5 | 28.9 ± 2.6 | 28.4 ± 2.3 | 3.2; 0.042 * | |
| <28 weeks n (%) | 92 (24.0) | 22 (25.3) | 21 (35.6) | ||
| 28–31 weeks n (%) | 240 (62.5) | 58 (66.7) | 32 (54.2) | ||
| 32–35 weeks n (%) | 52 (13.5) | 7 (8.0) | 6 (10.2) | ||
| Born in 2010–2014 n (%) | 194 (50.5) | 56 (64.4) | 34 (57.6) | 5.9; 0.052 # | Italy < High HDI |
| SGA at birth n (%) | 76 (19.8) | 12 (13.8) | 11 (18.6) | 1.7; 0.432 # | |
| Firstborn n (%) | 308 (80.2) | 61 (70.1) | 31 (52.5) | 22.8; <0.001 # | Italy > Low HDI |
| Twins (n = 529) n (%) | 152 (39.7) | 29 (33.3) | 14 (23.7) | 6.2; 0.046 # | Italy > Low HDI |
| IVH or PVL (n = 527) n (%) | 22 (5.8) | 11 (12.6) | 7 (11.9) | 6.5; 0.039 # | Italy < Low HDI, High HDI |
| Mechanical ventilation n (%) | 107 (27.9) | 23 (26.4) | 24 (40.7) | 4.4; 0.110 # | |
| BPD (n = 527) n (%) | 78 (20.5) | 22 (25.3) | 18 (30.5) | 3.5; 0.177 # | |
| Sepsis (n = 526) n (%) | 53 (13.9) | 12 (13.8) | 11 (19.0) | 1.1; 0.584 # | |
| NEC req. surgery n (%) | 16 (4.2) | 3 (3.4) | 3 (5.1) | 0.2; 0.888 # | |
| Weight at discharge (n = 521) mean ± SD | 2094 ± 397 | 2085 ± 376 | 2206 ± 441 | 3.0; 0.223 § | |
| SGA at discharge (n = 521) n (%) | 274 (72.9) | 65 (74.7) | 37 (63.8) | 2.4, 0.301 # | |
| Length of stay (days) mean ± SD | 56.3 ± 33.4 | 59.4 ± 40.2 | 64.7 ± 37.7 | 3.7; 0.159 § | |
| Diet at discharge | 5.2; 0.270 # | ||||
| Human milk only n (%) | 112 (29.2) | 16 (18.4) | 14 (23.7) | ||
| Formula milk only n (%) | 106 (27.6) | 25 (28.7) | 19 (32.2) | ||
| Mixed n (%) | 166 (43.2) | 46 (52.9) | 26 (44.1) |
| Variables | Human Milk (n = 142) | Mixed (n = 238) | Formula Milk (n = 149) | Test (p-Value) | Significant Post-Hoc Comparisons at p = 0.017 |
|---|---|---|---|---|---|
| Maternal characteristics | |||||
| Age (n = 529) mean ± SD | 33.5 ± 5.5 | 34.3 ± 5.1 | 33.5 ± 6.5 | 1.4; 0.256 | |
| Education (n = 527) | 21.5; <0.001 # | ||||
| Low n (%) | 15 (10.6) | 49 (20.6) | 35 (23.6) | Human < Formula, Mixed | |
| Middle n (%) | 66 (46.8) | 98 (41.2) | 81 (54.7) | ||
| High n (%) | 60 (42.6) | 91 (38.2) | 32 (21.6) | Formula< Human, Mixed | |
| Working condition (n = 529) | 0.197 $ | ||||
| Employed n (%) | 122 (85.9) | 194 (81.5) | 113 (75.8) | ||
| Unemployed n (%) | 2 (1.4) | 11 (4.6) | 4 (2.7) | ||
| Student n (%) | 3 (2.1) | 5 (2.1) | 7 (4.7) | ||
| Housewife n (%) | 15 (10.6) | 28 (11.8) | 25 (16.8) | ||
| Smoker (n = 423) | 5 (5.3) | 26 (12.4) | 23 (19.3) | 0.42; 0.009 # | Human < Formula |
| Maternal social risk score (n = 529) mean ± SD | 0.35 ± 0.58 | 0.50 ± 0.69 | 0.64 ± 0.81 | 8.2; 0.016 § | Human < Formula |
| Neonatal characteristics | |||||
| Sex (females) n (%) | 71 (50.0) | 125 (52.5) | 74 (49.3) | 0.4; 0.801 # | |
| Birthweight (g) mean ± SD | 1173 ± 339 | 1234 ± 308 | 1035 ± 340 | 17.3; <0.001 * | Formula < Human, Mixed |
| Gestational age mean ± SD | 29.1 ± 2.3 | 29.7 ± 2.3 | 28.1 ± 2.6 | 19.7; <0.001* | Formula < Human, Mixed |
| <28 weeks n (%) | 33 (23.2) | 43 (18.1) | 59 (39.3) | ||
| 28–31 weeks n (%) | 95 (66.9) | 153 (64.3) | 82 (54.7) | ||
| 32–35 weeks n (%) | 14 (9.9) | 42 (17.6) | 9 (6.0) | ||
| Born in 2010–2014 n (%) | 36 (25.3) | 176 (73.9) | 72 (48.0) | 87.1; <0.001 # | Human < Formula < Mixed |
| SGA at birth n (%) | 24 (16.9) | 43 (18.1) | 32 (21.3) | 1.0; 0.592 # | |
| Firstborn n (%) | 115 (81.0) | 177 (74.4) | 108 (72.0) | 3.5; 0.177 # | |
| Twins (n = 529) n (%) | 57 (40.1) | 98 (41.2) | 40 (26.8) | 9.0; 0.011 # | Formula < Human, Mixed |
| IVH or PVL (n = 527) n (%) | 7 (4.9) | 15 (6.4) | 18 (12.0) | 6.1; 0.048 # | |
| Mechanical ventilation n (%) | 39 (27.5) | 49 (20.6) | 66 (44.0) | 24.7; <0.001 # | Formula > Human > Mixed |
| BPD (n = 527) n (%) | 78 (20.5) | 18 (30.5) | 22 (25.3) | 3.5; 0.177 # | |
| Sepsis (n = 526) n (%) | 53 (13.9) | 11 (19.0) | 12 (13.8) | 1.1; 0.584 # | |
| NEC requiring surgery n (%) | 16 (4.2) | 3 (5.1) | 3 (3.4) | 0.2; 0.888 # | |
| Weight at discharge (n = 521) mean ± SD | 2094 ± 397 | 2206 ± 441 | 2085 ± 376 | 3.0; 0.223 § | |
| SGA at discharge (n = 521) n (%) | 274 (72.9) | 37 (63.8) | 65 (74.7) | 2.4, 0.301 # | |
| Length of stay (days) mean ± SD | 56.3 ± 33.4 | 64.7 ± 37.7 | 59.4 ± 40.2 | 3.7; 0.159 § |
| Variables | Mothers’ Origin | Type of Feeding | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Italy (n = 384) | High HDI (n = 87) | Low HDI (n = 59) | ANOVA Test (F; p) | Significant Post-Hoc Comparisons at p = 0.017 | Human M. (n = 142) | Mixed (n = 238) | Formula (n = 150) | ANOVA Test (F; p-value) | Significant Post-Hoc Comparisons at p = 0.017 | |
| 3-months | 114.3 ± 9.4 | 111.1 ± 9.6 | 112.6 ± 9.6 | 3.7, 0.024 | Italy > High HDI | 114.6 ± 8.0 | 115.3 ± 8.0 | 110.0 ± 11.9 | 13.8, <0.001 | Formula < Human, Mixed |
| 6-months | 107.3 ± 12.1 | 103.1 ± 14.1 | 101.5 ± 13.8 | 7.3, 0.001 | Italy > High HDI, Low HDI | 106.0 ± 13.0 | 107.9 ± 11.4 | 102.9 ± 14.0 | 6.6, 0.002 | Formula < Mixed |
| 9-months | 106.8 ± 12.8 | 105.1 ± 13.9 | 105.2 ± 14.8 | 0.7, 0.514 | 107.9 ± 11.1 | 108.0 ± 12.5 | 102.4 ± 15.4 | 7.6, 0.001 | Formula < Human, Mixed | |
| 12-months | 101.7 ± 13.1 | 98.2 ± 14.1 | 98.5 ± 11.5 | 3.1, 0.045 | 102.3 ± 12.8 | 101.9 ± 12.4 | 97.7 ± 14.1 | 5.6, 0.004 | Formula < Human, Mixed | |
| 18-months | 94.7 ± 13.7 | 87.6 ± 13.7 | 83.5 ± 16.6 | 18.4, <0.001 | Italy > High HDI, Low HDI | 94.8 ± 13.0 | 94.1 ± 13.6 | 87.5 ± 16.2 | 11.0, <0.001 | Formula < Human, Mixed |
| 24-months | 94.5 ± 14.4 | 90.9 ± 14.4 | 79.8 ± 19.9 | 19.4, <0.001 | Low HDI < Italy, High HDI | 95.9 ± 13.6 | 93.2 ± 15.3 | 87.8 ± 17.1 | 9.0, <0.001 | Formula < Human, Mixed |
| Delayed impairment at 24-months, n (%) | 56.6, <0.001 * | 18.9, 0.004 * | ||||||||
| Severe | 18 (5.3) | 5 (6.9) | 12 (27.3) | Low HDI > High HDI, Italy | 4 (3.1) | 15 (7.2) | 16 (13.2) | Formula > Human, Mixed | ||
| Moderate | 11 (3.2) | 3 (4.2) | 9 (20.4) | Low HDI > High HDI, Italy | 8 (6.3) | 9 (4.4) | 6 (5.0) | |||
| Mild | 65 (19.1) | 18 (25.0) | 7 (15.9) | 17 (13.3) | 41 (19.8) | 32 (26.4) | ||||
| Normal development | 246 (72.4) | 46 (63.9) | 16 (36.4) | Low HDI < High HDI, Italy | 99 (77.3) | 142 (68.6) | 67 (55.4) | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gibertoni, D.; Sansavini, A.; Savini, S.; Locatelli, C.; Ancora, G.; Perrone, E.; Ialonardi, M.; Rucci, P.; Fantini, M.P.; Faldella, G.; et al. Neurodevelopmental Trajectories of Preterm Infants of Italian Native-Born and Migrant Mothers and Role of Neonatal Feeding. Int. J. Environ. Res. Public Health 2020, 17, 4588. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124588
Gibertoni D, Sansavini A, Savini S, Locatelli C, Ancora G, Perrone E, Ialonardi M, Rucci P, Fantini MP, Faldella G, et al. Neurodevelopmental Trajectories of Preterm Infants of Italian Native-Born and Migrant Mothers and Role of Neonatal Feeding. International Journal of Environmental Research and Public Health. 2020; 17(12):4588. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124588
Chicago/Turabian StyleGibertoni, Dino, Alessandra Sansavini, Silvia Savini, Chiara Locatelli, Gina Ancora, Enrica Perrone, Magda Ialonardi, Paola Rucci, Maria Pia Fantini, Giacomo Faldella, and et al. 2020. "Neurodevelopmental Trajectories of Preterm Infants of Italian Native-Born and Migrant Mothers and Role of Neonatal Feeding" International Journal of Environmental Research and Public Health 17, no. 12: 4588. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124588