Association between Shift Work and Neurocognitive Function among Firefighters in South Korea: A Prospective before–after Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
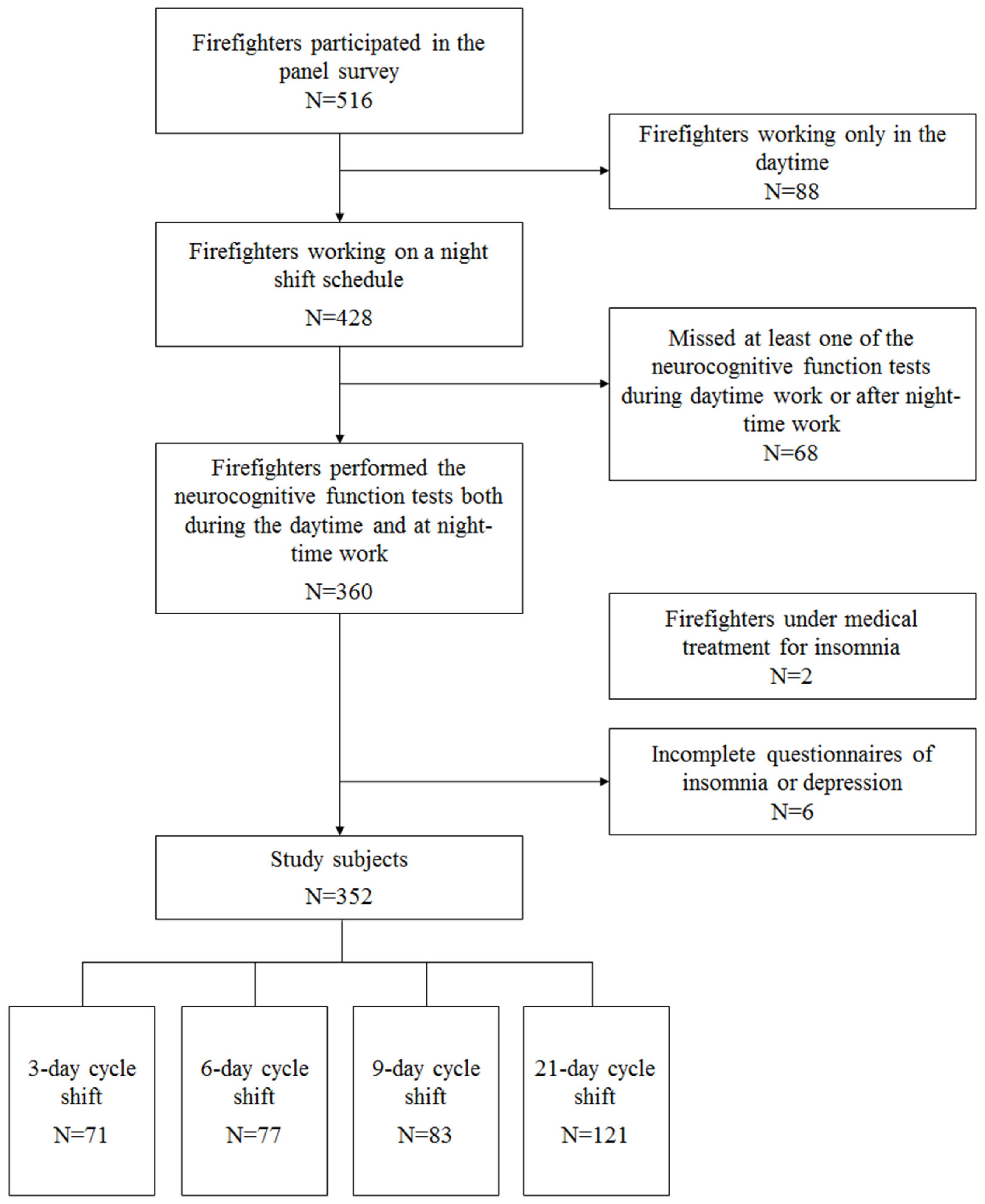
2.1. Study Subjects
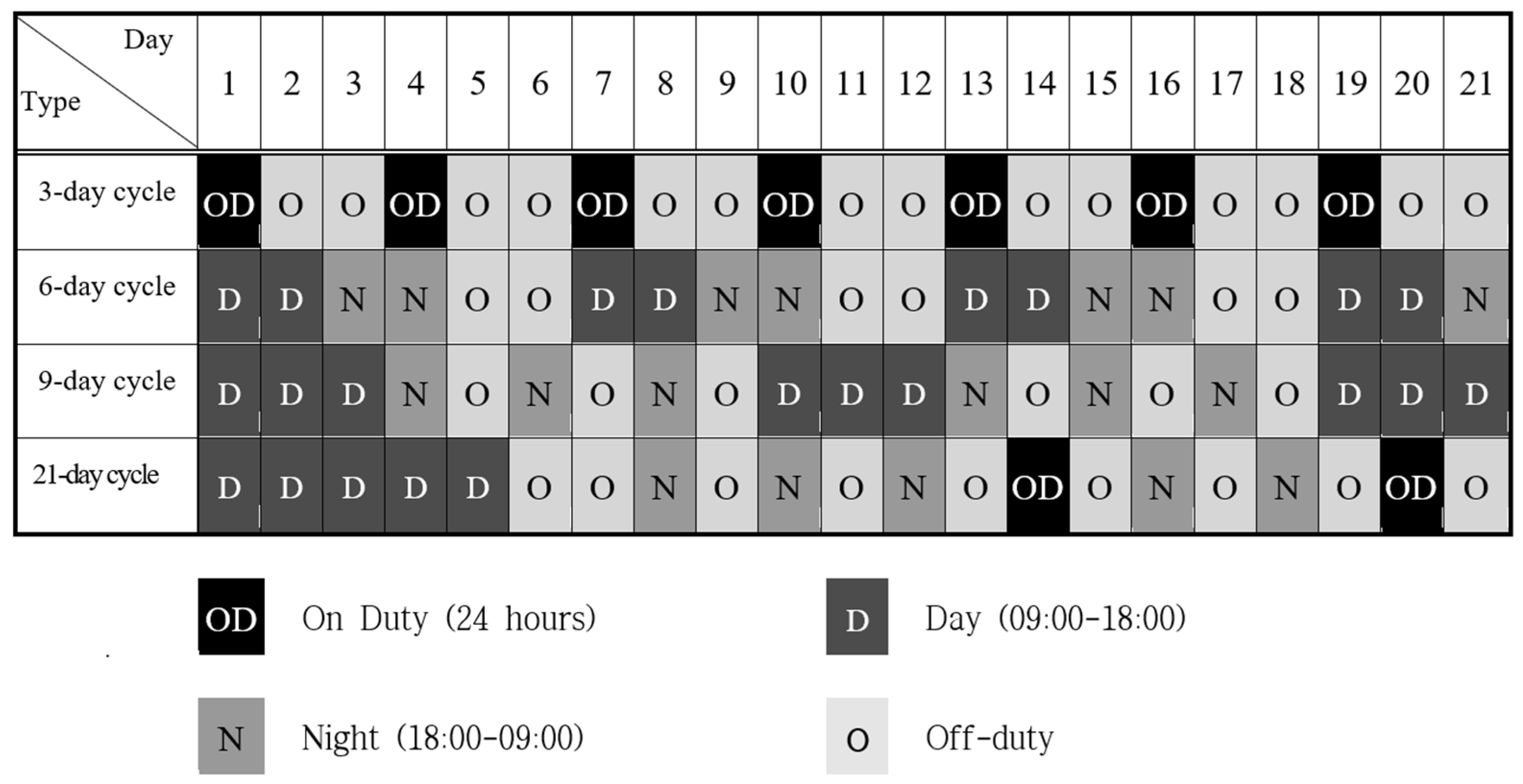
2.2. Type of Shift Work
2.3. Questionnaire
2.4. Sleep Disorder and Depression Evaluation Tools
2.5. Neurocognitive Function Testing
2.6. Study Endpoints
2.7. Statistical Analysis
2.8. Ethics Statement
3. Results
3.1. General Characteristics of Subjects
3.2. Neurocognitive Function
3.3. Stratifying Analysis Based on the ISI
3.4. Stratifying Analysis Based on the PHQ-9
3.5. Multivariate Analysis for the Changes of Neurocognitive Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lee, N.; Kim, J.H.; Kim, J.Y.; Kim, S.S. Association between workplace discrimination and depressive symptoms among firefighters in South Korea. Am. J. Ind. Med. 2018, 61, 741–750. [Google Scholar] [CrossRef]
- Guidotti, T.L.; Clough, V.M. Occupational health concerns of firefighting. Annu. Rev. Public Health 1992, 13, 151–171. [Google Scholar] [CrossRef]
- An, S.J.; Chung, Y.K.; Kim, B.H.; Kwak, K.M.; Son, J.S.; Koo, J.; Ju, Y.S.; Kwon, Y.J. The effect of organisational system on self-rated depression in a panel of male municipal firefighters. Ann. Occup. Envrion. Med. 2015, 27, 1. [Google Scholar] [CrossRef] [Green Version]
- Sakuma, A.; Takahashi, Y.; Ueda, I.; Sato, H.; Katsura, M.; Abe, M.; Nagao, A.; Suzuki, Y.; Kakizaki, M.; Tsuji, I.; et al. Post-traumatic stress disorder and depression prevalence and associated risk factors among local disaster relief and reconstruction workers fourteen months after the Great East Japan Earthquake: A cross-sectional study. BMC Psychiatry 2015, 15, 58. [Google Scholar] [CrossRef] [Green Version]
- Berninger, A.; Webber, M.P.; Niles, J.K.; Gustave, J.; Lee, R.; Cohen, H.W.; Kelly, K.; Corrigan, M.; Prezant, D.J. Longitudinal study of probable post-traumatic stress disorder in firefighters exposed to the World Trade Center disaster. Am. J. Ind. Med. 2010, 53, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- Del Ben, K.S.; Scotti, J.R.; Chen, Y.C.; Fortson, B.L. Prevalence of posttraumatic stress disorder symptoms in firefighters. Work Stress 2006, 20, 37–48. [Google Scholar] [CrossRef]
- Carey, M.G.; Al-Zaiti, S.S.; Dean, G.E.; Sessanna, L.; Finnell, D.S. Sleep problems, depression, substance use, social bonding, and quality of life in professional firefighters. J. Occup. Environ. Med. 2011, 53, 928–933. [Google Scholar] [CrossRef] [Green Version]
- Lim, D.K.; Baek, K.O.; Chung, I.S.; Lee, M.Y. Factors related to sleep disorders among male firefighters. Ann. Occup. Environ. Med. 2014, 26, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazloumi, A.; Golbabaei, F.; Khani, S.M.; Kazemi, Z.; Hosseini, M.; Abbasinia, M.; Dehghan, S.F. Evaluating effects of heat stress on cognitive function among workers in a hot industry. Health Promot. Perspect. 2014, 4, 240–246. [Google Scholar] [PubMed]
- Hancock, P.A.; Vasmatzidis, I. Effects of heat stress on cognitive performance: The current state of knowledge. Int. J. Hyperthermia 2003, 19, 355. [Google Scholar] [CrossRef]
- Gaoua, A. Cognitive function in hot environments: A question of methodology. Scand. J. Med. Sci. Sports 2010, 20, 60–70. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S.; Sapolsky, R.M. Stress and cognitive function. Curr. Opin. Neurobiol. 1995, 5, 205–216. [Google Scholar] [CrossRef]
- Marin, M.F.; Lord, C.; Andrews, J.; Juster, R.P.; Sindi, S.; Arsenault-Lapierre, G.; Fiocco, A.J.; Lupien, S.J. Chronic stress, cognitive functioning and mental health. Neurobiol. Learn. Mem. 2011, 96, 583–595. [Google Scholar] [CrossRef] [PubMed]
- Barrett, D.H.; Green, M.L.; Morris, R.; Giles, W.H.; Croft, J.B. Cognitive functioning and posttraumatic stress disorder. Am. J. Psychiatry 1996, 153, 1492–1494. [Google Scholar]
- Austin, M.P.; Ross, M.; Murray, C.; O’Caŕroll, R.E.; Ebmeier, K.P.; Goodwin, G.M. Cognitive function in major depression. J. Affect. Disord. 1992, 25, 21–29. [Google Scholar] [CrossRef]
- McDermott, L.M.; Ebmeier, K.P. A meta-analysis of depression severity and cognitive function. J. Affect. Disord. 2009, 119, 1–8. [Google Scholar] [CrossRef]
- Rock, P.L.; Roiser, J.P.; Riedel, W.J.; Blackwell, A.D. Cognitive impairment in depression: A systematic review and meta-analysis. Psychol. Med. 2014, 44, 2029–2040. [Google Scholar] [CrossRef] [Green Version]
- Titova, O.E.; Lindberg, E.; Elmståhl, S.; Lind, L.; Schiöth, H.B.; Benedict, C. Association between shift work history and performance on the trail making test in middle-aged and elderly humans: The EpiHealth study. Neurobiol. Aging 2016, 45, 23–29. [Google Scholar] [CrossRef]
- Ansiau, D.; Wild, P.; Niezborala, M.; Rouch, I.; Marquie, J.C. Effects of working conditions and sleep of the previous day on cognitive performance. Appl. Ergon. 2008, 39, 99–106. [Google Scholar] [CrossRef]
- Machi, M.S.; Staum, M.; Callaway, C.W.; Moore, C.; Jeong, K.; Suyama, J.; Patterson, P.D.; Hostler, D. The relationship between shift work, sleep, and cognition in career emergency physician. Acad. Emerg. Med. 2012, 19, 85–91. [Google Scholar] [CrossRef]
- Marquie, J.C.; Tucker, P.; Folkard, S.; Gentil, C.; Ansiau, D. Chronic effects of shift work on cognition: Findings from the VISAT longitudinal study. Occup. Environ. Med. 2015, 72, 258–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondratova, A.A.; Kondratov, R.V. The circadian clock and pathology of the ageing brain. Nat. Rev. Neurosci. 2012, 13, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Wulff, K.; Gatti, S.; Wettstein, J.G.; Foster, R.G. Sleep and circadian rhythm disruption in psychiatric and neurodegenerative disease. Nat. Rev. Neurosci. 2010, 11, 589–599. [Google Scholar] [CrossRef] [PubMed]
- Musiek, E.S.; Lim, M.M.; Yang, G.; Bauer, A.Q.; Qi, L.; Lee, Y.; Roh, J.H.; Gonzalez, X.O.; Dearborn, J.T.; Culver, J.P.; et al. Circadian clock proteins regulate neuronal redox homeostasis and neurodegeneration. J. Clin. Investig. 2013, 123, 5389–5400. [Google Scholar] [CrossRef]
- Rodrigues, S.; Paiva, J.S.; Dias, D.; Pimentel, G.; Kaiseler, M.; Cunha, J.P.S. Wearable Biomonitoring Platform for the Assessment of Stress and its Impact on Cognitive Performance of Firefighters: An Experimental Study. Clin. Pract. Epidemiol. Ment. Health 2018, 14, 250–262. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Ensrud, K.E.; Joffe, H.; Guthrie, K.A.; Larson, J.C.; Reed, S.D.; Newton, K.M.; Sternfeld, B.; LaCroix, A.Z.; Landis, C.A.; Woods, N.F.; et al. Effect of escitalopram on insomnia symptoms and subjective sleep quality in healthy menopausal women with hot flashes: A randomized controlled trial. Menopause 2012, 19, 848–855. [Google Scholar] [CrossRef] [Green Version]
- Kwak, K.M.; Ju, Y.S.; Kwon, Y.J.; Chung, Y.K.; Kim, B.K.; Kim, H.; Youn, K. The effect of aircraft noise on sleep disturbance among the residents near a civilian airport: A cross-sectional study. Ann. Occup. Environ. Med. 2016, 28, 38. [Google Scholar] [CrossRef] [Green Version]
- Morin, C.M.; Colecchi, C.; Stone, J.; Sood, R.M.; Brink, D. Behavioral and pharmacological therapies for late-life insomnia: A randomised controlled trial. JAMA 1999, 281, 991–999. [Google Scholar] [CrossRef] [Green Version]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W. Patient Health Questionnaire Study Group. Validity and utility of a self-report version of PRIME-MD: The PHQ Primary Care Study. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.W.; Song, M.L.; Morin, C.M. Validation of a Korean Version of the Insomnia Severity Index. J. Clin. Neurol. 2014, 10, 210–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, C.; Jo, S.A.; Kwak, J.H.; Pae, C.U.; Steffens, D.; Jo, I.; Park, M.H. Validation of the Patient Health Questionnaire-9 Korean version in the elderly population: The Ansan Geriatric study. Compr. Psychiatry 2008, 49, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Gualtieri, C.T.; Johnson, L.G. Reliability and validity of a computerized neurocognitive test battery, CNS Vital Signs. Arch. Clin. Neuropsychol. 2006, 21, 623–643. [Google Scholar] [CrossRef] [Green Version]
- CNS Vital Signs. CNS Vital Signs Brief Interpretation Guide. Available online: https://www.cnsvs.com/WhitePapers/CNSVS-BriefInterpretationGuide.pdf (accessed on 19 July 2019).
- Bonnet, M.; Arand, D. Clinical effects of sleep fragmentation versus sleep deprivation. Sleep Med. Rev. 2003, 7, 297–310. [Google Scholar] [CrossRef] [Green Version]
- Chee, M.W.L.; Chuah, L.Y.M. Functional neuroimaging insights into how sleep and sleep deprivation affect memory and cognition. Curr. Opin. Neurol. 2008, 21, 417–423. [Google Scholar] [CrossRef]
- Williamson, A.M.; Feyer, A.M. Moderate sleep deprivation produces impairments in cognitive and motor performance equivalent to legally prescribed levels of alcohol intoxication. Occup. Environ. Med. 2000, 57, 649–655. [Google Scholar] [CrossRef] [Green Version]
- Van Dongen, H.; Maislin, G.; Mullington, J.M.; Dinges, D.F. The cumulative cost of additional wakefulness: Dose-response effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation. Sleep 2003, 26, 117–126. [Google Scholar] [CrossRef]
- Basner, M.; Rao, H.; Goel, N.; Dinges, D.F. Sleep deprivation and neurobehavioral dynamics. Curr. Opin. Neurobiol. 2013, 23, 854–863. [Google Scholar] [CrossRef] [Green Version]
- Melamed, S.; Oksenberg, A. Excessive daytime sleepiness and risk of occupational injuries in non-shift daytime workers. Sleep 2002, 25, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Geerlings, M.I.; Bouter, L.M.; Schoevers, R.A.; Beekman, A.T.F.; Jonker, C.; Deeg, D.J.H.; Van Tilburg, W.; Adèr, H.J.; Schmand, B. Depression and risk of cognitive decline and Alzheimer’s disease: Results of two prospective community-based studies in The Netherlands. Br. J. Psychiatry 2000, 176, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Lammers-van der Holst, H.M.; Kerkhof, G.A. Individual differences in the cortisol-awakening response during the first two years of shift work: A longitudinal study in novice police officers. Chronobiol. Int. 2015, 32, 1162–1167. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Bidlingmaier, M.; Petru, R.; Gil, F.P.; Loerbroks, A.; Angerer, P. Impact of shift work on the diurnal cortisol rhythm: A one-year longitudinal study in junior physicians. J. Occup. Med. Toxicol. 2018, 13, 23. [Google Scholar] [CrossRef] [PubMed]
- Chida, Y.; Steptoe, A. Cortisol awakening response and psychosocial factors: A systematic review and meta-analysis. Biol. Psychol. 2009, 80, 265–278. [Google Scholar] [CrossRef]
- Clow, A.; Hucklebridge, F.; Stalder, T.; Evans, P.; Thorn, L. The cortisol awakening response: More than a measure of HPA axis function. Neurosci. Biobehav. Rev. 2010, 35, 97–103. [Google Scholar] [CrossRef]
- Bottaccioli, A.G.; Bottaccioli, F.; Minelli, A. Stress and the psyche-brain-immune network in psychiatric diseases based on psychoneuroendocrineimmunology: A concise review. Ann. N. Y. Acad. Sci. 2018, 1437, 31–42. [Google Scholar] [CrossRef]
- Williams-Bell, F.M.; Aisbett, B.; Murphy, B.A.; Larsen, B. The Effects of Simulated Wildland Firefighting Tasks on Core Temperature and Cognitive Function under Very Hot Conditions. Front. Physiol. 2017, 8, 815. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.; Beauchamp, G.; Suyama, J.; Guyette, F.X.; Reis, S.E.; Clifton, W.; Callaway, C.W.; Hostler, D. Cognitive function following treadmill exercise in thermal protective clothing. Eur. J. Appl. Physiol. 2012, 112, 1733–1740. [Google Scholar] [CrossRef]
- Christensen, H.; Griffiths, K.; Mackinnon, A.; Jacomb, P.A. A quantitative review of cognitive deficits in depression and Alzheimer-type dementia. J. Int. Neuropsychol. Soc. 1997, 3, 631–651. [Google Scholar] [CrossRef]
- Jorm, A.F. Is depression a risk factor for dementia or cognitive decline? Gerontology 2000, 46, 219–227. [Google Scholar] [CrossRef]
- Saijo, Y.; Ueno, T.; Hashimoto, Y. Twenty-four-hour shift work, depressive symptoms, and job dissatisfaction among Japanese firefighters. Am. J. Ind. Med. 2008, 51, 380–391. [Google Scholar] [CrossRef] [PubMed]
- Saijo, Y.; Ueno, T.; Hashimoto, Y. Job stress and depressive symptoms among Japanese fire fighters. Am. J. Ind. Med. 2007, 50, 470–480. [Google Scholar] [CrossRef] [PubMed]
- Brzezinski, A.; Vangel, M.G.; Wurtman, R.J.; Norrie, G.; Zhdanova, I.; Ben-Shushan, A.; Ford, I. Effects of exogenous melatonin on sleep: A meta-analysis. Sleep Med. Rev. 2005, 9, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Ferracioli-Oda, E.; Qawasmi, A.; Bloch, M.H. Meta-analysis: Melatonin for the treatment of primary sleep disorders. PLoS ONE 2013, 8, e63773. [Google Scholar] [CrossRef] [Green Version]
- van der Zweerde, T.; Bisdounis, L.; Kyle, S.D.; Lancee, J.; van Straten, A. Cognitive behavioral therapy for insomnia: A meta-analysis of long-term effects in controlled studies. Sleep Med. Rev. 2019, 48, 101208. [Google Scholar] [CrossRef]
- Eidelman, P.; Talbot, L.; Ivers, H.; Bélanger, L.; Morin, C.M.; Harvey, A.G. Change in dysfunctional beliefs about sleep in behavior therapy, cognitive therapy, and cognitive-behavioral therapy for insomnia. Behav. Ther. 2016, 47, 102–115. [Google Scholar] [CrossRef]
- Small, G.W. Detection and prevention of cognitive decline. Am. J. Geriatr. Psychiat. 2016, 24, 1142–1150. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristics | Shift Work Schedule | All Subjects N = 352 | p-Value | |||
|---|---|---|---|---|---|---|
| 3-Day Cycle N = 71 | 6-Day Cycle N = 77 | 9-Day Cycle N = 83 | 21-Day Cycle N = 121 | |||
| Age (years) | 0.043 3–6 | |||||
| 20–29 | 4 (5.6%) | 11 (14.3%) | 11 (13.3%) | 14 (11.6%) | 40 (11.4%) | |
| 30–39 | 21 (29.6%) | 35 (45.5%) | 29 (34.9%) | 47 (38.8%) | 132 (37.5%) | |
| 40–49 | 30 (42.3%) | 19 (24.7%) | 24 (28.9%) | 48 (39.7%) | 121 (34.4%) | |
| 50–59 | 16 (22.5%) | 12 (15.6%) | 19 (22.9%) | 12 (9.9%) | 59 (16.8%) | |
| Mean ± SD | 42.5 ± 8.1 | 38.4 ± 9.3 | 41.2 ± 9.0 | 39.1 ± 8.0 | 40.1 ± 8.7 | 0.012 3–6,3–21 |
| Sex | 0.051 | |||||
| Men | 61 (85.9%) | 73 (94.8%) | 80 (96.4%) | 114 (94.2%) | 328 (93.2%) | |
| Women | 10 (14.1%) | 4 (5.2%) | 3 (3.6%) | 7 (5.8%) | 24 (6.8%) | |
| Job | 0.009 3–21,6–21 | |||||
| Fire suppression | 14 (19.7%) | 21 (27.3%) | 25 (30.1%) | 51 (42.1%) | 111 (31.5%) | |
| Others | 57 (80.3%) | 56 (72.7%) | 58 (69.9%) | 70 (57.9%) | 241 (68.5%) | |
| Education | 0.046 3–6,6–21 | |||||
| High school | 10 (14.1%) | 24 (31.2%) | 18 (21.7%) | 18 (14.9%) | 70 (19.9%) | |
| 2-year degree | 23 (32.4%) | 23 (29.9%) | 18 (21.7%) | 36 (29.7%) | 100 (28.4%) | |
| 4-year degree | 38 (53.5%) | 30 (39.0%) | 47 (56.6%) | 67 (55.4%) | 182 (51.7%) | |
| Monthly income | <0.001 3–6,3–21,6–9,9–21 | |||||
| Missing | 0 | 0 | 2 | 0 | 2 | |
| Low | 11 (15.5%) | 33 (42.9%) | 12 (14.8%) | 37 (30.6%) | 93 (26.6%) | |
| Middle | 32 (45.1%) | 32 (41.6%) | 42 (51.9%) | 62 (51.2%) | 168 (48.0%) | |
| High | 28 (39.4%) | 12 (15.6%) | 27 (33.3%) | 22 (18.2%) | 89 (25.4%) | |
| Smoking | 0.576 | |||||
| Missing | 0 | 0 | 0 | 1 | 1 | |
| Never | 29 (40.8%) | 37 (48.0%) | 33 (39.8%) | 40 (33.3%) | 139 (39.6%) | |
| Past smoker | 24 (33.8%) | 22 (28.6%) | 21 (25.3%) | 45 (37.5%) | 112 (31.9%) | |
| Current light smoker | 10 (14.1%) | 10 (13.0%) | 17 (20.5%) | 21 (17.5%) | 58 (16.5%) | |
| Current heavy smoker | 8 (11.3%) | 8 (10.4%) | 12 (14.5%) | 14 (11.7%) | 42 (12.0%) | |
| Alcohol | 0.996 | |||||
| Missing | 2 | 3 | 1 | 2 | 8 | |
| No | 15 (21.7%) | 17 (23.0%) | 16 (19.5%) | 24 (20.2%) | 72 (20.9%) | |
| Normal drinking | 41 (59.4%) | 41 (55.4%) | 48 (58.5%) | 69 (58.0%) | 199 (57.9%) | |
| Heavy drinking | 13 (18.8%) | 16 (21.6%) | 18 (22.0%) | 26 (21.8%) | 73 (21.2%) | |
| Regular exercise | 0.636 | |||||
| No | 33 (46.5%) | 36 (46.8%) | 44 (53.0%) | 53 (43.8%) | 166 (47.2%) | |
| Yes | 38 (53.5%) | 41 (53.2%) | 39 (47.0%) | 68 (56.2%) | 186 (52.8%) | |
| Caffeine | 0.045 3–6,3–9 | |||||
| Missing | 5 | 7 | 2 | 4 | 18 | |
| No | 8 (12.1%) | 16 (22.9%) | 15 (18.5%) | 18 (15.4%) | 57 (17.1%) | |
| Light coffee drinking | 25 (37.9%) | 35 (50.0%) | 45 (55.6%) | 61 (52.1%) | 166 (49.7%) | |
| Moderate to heavy coffee drinking | 33 (50.0%) | 19 (27.1%) | 21 (25.9%) | 38 (32.5%) | 111 (33.2%) | |
| Insomnia | 0.148 | |||||
| Normal (≤ 7) | 43 (60.6%) | 31 (40.3%) | 44 (53.0%) | 68 (56.2%) | 186 (52.8%) | |
| Mild Insomnia (8–14) | 21 (29.6%) | 40 (51.9%) | 32 (38.6%) | 41 (33.9%) | 134 (38.1%) | |
| Insomnia (≥ 15) | 7 (9.9%) | 6 (7.8%) | 7 (8.4%) | 12 (9.9%) | 32 (9.1%) | |
| Mean ± SD | 7.3 ± 2.2 | 8.8 ± 2.4 | 7.7 ± 4.7 | 7.2 ± 5.3 | 7.7 ± 5.0 | 0.151 |
| Depression | 0.896 | |||||
| Normal (≤ 4) | 60 (84.5%) | 64 (83.1%) | 71 (85.5%) | 103 (85.1%) | 298 (84.7%) | |
| Mild depression (5–9) | 9 (12.7%) | 9 (11.7%) | 11 (13.3%) | 14 (11.6%) | 43 (12.2%) | |
| Depression (≥ 10) | 2 (2.8%) | 4 (5.2%) | 1 (1.2%) | 4 (3.3%) | 11 (3.1%) | |
| Mean ± SD | 2.2 ± 2.8 | 2.4 ± 3.1 | 2.1 ± 2.3 | 2.0 ± 2.9 | 2.1 ± 2.8 | 0.771 |
| Domain | Mean ± SD (N = 352) | p-Value | |
|---|---|---|---|
| During Day Work | After Night Work | ||
| Composite memory | 90.6 ± 19.1 | 84.7 ± 19.7 | <0.001 |
| Verbal memory | 87.7 ± 20.0 | 81.3 ± 21.9 | <0.001 |
| Visual memory | 97.1 ± 16.3 | 94.0 ± 16.6 | 0.001 |
| Complex attention | 97.8 ± 18.2 | 93.3 ± 32.4 | 0.007 |
| Psychomotor speed | 112.4 ± 15.4 | 110.1 ± 15.2 | <0.001 |
| Motor speed | 111.0 ± 15.1 | 108.7 ± 14.1 | <0.001 |
| Processing speed | 107.6 ± 15.7 | 107.4 ± 17.1 | 0.860 |
| Reaction time | 92.4 ± 15.0 | 92.7 ± 17.1 | 0.711 |
| Cognitive flexibility | 106.2 ± 16.9 | 105.8 ± 19.1 | 0.671 |
| Executive functioning | 107.0 ± 16.5 | 107.2 ± 18.5 | 0.799 |
| Neurocognitive index | 99.9 ± 11.6 | 97.4 ± 13.4 | <0.001 |
| Domain | ISI Category | N | Mean ± SD (n = 352) | p-Value | |
|---|---|---|---|---|---|
| During Daytime Work | Post Nighttime Work | ||||
| Composite memory | Normal | 186 | 90.2 ± 20.1 | 84.8 ± 19.5 | <0.001 |
| Mild insomnia | 134 | 90.6 ± 17.2 | 85.4 ± 19.4 | 0.002 | |
| Insomnia | 32 | 92.8 ± 21.6 | 81.5 ± 21.9 | 0.012 | |
| Verbal memory | Normal | 186 | 87.7 ± 20.6 | 82.7 ± 22.5 | <0.001 |
| Mild insomnia | 134 | 87.4 ± 19.1 | 80.4 ± 20.3 | <0.001 | |
| Insomnia | 32 | 89.7 ± 20.1 | 77.2 ± 24.6 | 0.001 | |
| Visual memory | Normal | 186 | 96.6 ± 16.8 | 92.8 ± 15.8 | 0.006 |
| Mild insomnia | 134 | 97.6 ± 14.9 | 95.8 ± 17.1 | 0.269 | |
| Insomnia | 32 | 98.3 ± 18.9 | 92.8 ± 18.6 | 0.110 | |
| Complex attention | Normal | 186 | 96.1 ± 20.3 | 94.3 ± 23.7 | 0.260 |
| Mild insomnia | 134 | 100.1 ± 15.0 | 92.2 ± 43.3 | 0.027 | |
| Insomnia | 32 | 98.2 ± 17.0 | 92.7 ± 22.4 | 0.227 | |
| Psychomotor speed | Normal | 186 | 111.7 ± 16.5 | 110.2 ± 15.9 | 0.056 |
| Mild insomnia | 134 | 114.1 ± 14.5 | 111.5 ± 14.5 | 0.008 | |
| Insomnia | 32 | 109.3 ± 11.3 | 104.3 ± 13.5 | 0.069 | |
| Motor speed | Normal | 186 | 110.1 ± 15.8 | 108.6 ± 14.7 | 0.053 |
| Mild insomnia | 134 | 112.2 ± 14.8 | 108.3 ± 13.5 | 0.001 | |
| Insomnia | 32 | 111.4 ± 12.1 | 104.8 ± 13.6 | 0.007 | |
| Processing speed | Normal | 186 | 107.7 ± 15.9 | 106.5 ± 16.9 | 0.298 |
| Mild insomnia | 134 | 109.1 ± 15.9 | 110.2 ± 17.4 | 0.341 | |
| Insomnia | 32 | 100.8 ± 11.3 | 101.4 ± 15.0 | 0.845 | |
| Reaction time | Normal | 186 | 92.4 ± 15.2 | 92.3 ± 16.8 | 0.931 |
| Mild insomnia | 134 | 93.5 ± 15.2 | 93.3 ± 17.3 | 0.872 | |
| Insomnia | 32 | 88.5 ± 12.3 | 93.0 ± 19.2 | 0.190 | |
| Cognitive flexibility | Normal | 186 | 104.8 ± 18.8 | 105.1 ± 18.9 | 0.809 |
| Mild insomnia | 134 | 108.4 ± 14.0 | 106.8 ± 20.1 | 0.306 | |
| Insomnia | 32 | 105.3 ± 15.4 | 106.0 ± 15.8 | 0.821 | |
| Executive functioning | Normal | 186 | 105.6 ± 18.3 | 106.6 ± 18.3 | 0.426 |
| Mild insomnia | 134 | 109.2 ± 13.8 | 108.0 ± 19.8 | 0.414 | |
| Insomnia | 32 | 105.8 ± 15.2 | 108.0 ± 14.7 | 0.397 | |
| Neurocognitive index | Normal | 186 | 99.0 ± 13.0 | 97.3 ± 12.7 | 0.009 |
| Mild insomnia | 134 | 101.4 ± 9.6 | 97.9 ± 14.9 | 0.001 | |
| Insomnia | 32 | 98.9 ± 10.9 | 95.4 ± 10.3 | 0.089 | |
| Domain | PHQ-9 Category | N | Mean ± SD (n = 352) | p-Value | |
|---|---|---|---|---|---|
| During Daytime Work | Post Nighttime Work | ||||
| Composite memory | Normal | 298 | 90.1 ± 19.1 | 84.6 ± 19.7 | <0.001 |
| Depression | 54 | 93.3 ± 19.4 | 85.3 ± 19.7 | 0.003 | |
| Verbal memory | Normal | 298 | 87.3 ± 19.8 | 81.1 ± 22.0 | <0.001 |
| Depression | 54 | 90.1 ± 20.9 | 82.7 ± 21.3 | <0.001 | |
| Visual memory | Normal | 298 | 96.8 ± 16.3 | 94.0 ± 16.3 | 0.010 |
| Depression | 54 | 99.1 ± 16.4 | 93.8 ± 18.4 | 0.040 | |
| Complex attention | Normal | 298 | 97.2 ± 19.0 | 93.1 ± 34.0 | 0.030 |
| Depression | 54 | 101.0 ± 12.7 | 94.5 ± 22.1 | 0.017 | |
| Psychomotor speed | Normal | 298 | 112.3 ± 15.8 | 111.0 ± 15.0 | 0.035 |
| Depression | 54 | 112.9 ± 13.5 | 105.4 ± 15.9 | <0.001 | |
| Motor speed | Normal | 298 | 110.6 ± 15.5 | 108.6 ± 14.1 | 0.002 |
| Depression | 54 | 113.2 ± 12.7 | 105.8 ± 14.3 | <0.001 | |
| Processing speed | Normal | 298 | 108.1 ± 15.9 | 108.6 ± 16.9 | 0.626 |
| Depression | 54 | 104.5 ± 14.2 | 101.2 ± 16.8 | 0.143 | |
| Reaction time | Normal | 298 | 92.7 ± 15.1 | 92.5 ± 17.3 | 0.808 |
| Depression | 54 | 90.8 ± 14.5 | 93.7 ± 16.4 | 0.142 | |
| Cognitive flexibility | Normal | 298 | 106.0 ± 17.4 | 105.9 ± 19.0 | 0.921 |
| Depression | 54 | 107.6 ± 14.1 | 105.6 ± 19.7 | 0.471 | |
| Executive functioning | Normal | 298 | 106.8 ± 16.9 | 107.4 ± 18.4 | 0.545 |
| Depression | 54 | 108.2 ± 13.7 | 106.6 ± 19.4 | 0.544 | |
| Neurocognitive index | Normal | 298 | 99.7 ± 12.0 | 97.4 ± 13.6 | <0.001 |
| Depression | 54 | 101.1 ± 9.4 | 96.9 ± 12.1 | 0.003 | |
| Domain | Type of Shift Work | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|---|
| LSmeans | p-Value | LSmeans | p-Value | LSmeans | p-Value | ||
| Composite memory | 3-day cycle | 8.38 | 0.503 | 9.26 | 0.493 | 8.68 | 0.483 |
| 6-day cycle | 4.74 | 5.06 | 4.59 | ||||
| 9-day cycle | 3.81 | 4.82 | 4.18 | ||||
| 21-day cycle | 6.50 | 7.35 | 7.07 | ||||
| Verbal memory | 3-day cycle | −20.17 | 0.030 | −15.78 | 0.060 | −15.92 | 0.071 |
| 6-day cycle | −15.49 9 | −12.13 | −12.07 | ||||
| 9-day cycle | −25.95 6,21 | −13.01 | −21.21 | ||||
| 21-day cycle | −17.19 9 | −15.78 | −12.68 | ||||
| Visual memory | 3-day cycle | 6.20 | 0.327 | 6.39 | 0.246 | 5.34 | 0.313 |
| 6-day cycle | 1.30 | 0.61 | 0.12 | ||||
| 9-day cycle | 1.49 | 1.30 | 0.69 | ||||
| 21-day cycle | 3.79 | 3.59 | 3.29 | ||||
| Complex attention | 3-day cycle | 0.21 | 0.563 | 0.29 | 0.499 | −0.15 | 0.547 |
| 6-day cycle | 7.03 | 7.75 | 6.86 | ||||
| 9-day cycle | 4.11 | 4.53 | 4.29 | ||||
| 21-day cycle | 5.63 | 6.50 | 6.32 | ||||
| Psychomotor speed † | 3-day cycle | 2.04 | 0.307 | 2.40 | 0.215 | 1.81 | 0.279 |
| 6-day cycle | 0.31 | 0.10 | −0.41 | ||||
| 9-day cycle | 3.66 | 3.96 | 3.15 | ||||
| 21-day cycle | 2.71 | 2.68 | 2.15 | ||||
| Motor speed ‡ | 3-day cycle | 4.21 | 0.131 | 3.25 | 0.075 | 3.20 | 0.112 |
| 6-day cycle | 3.14 | 1.92 | 1.69 | ||||
| 9-day cycle | 4.31 | 3.29 | 2.81 | ||||
| 21-day cycle | 1.00 | −0.39 | −0.50 | ||||
| Processing speed †† | 3-day cycle | −2.66 21 | <0.001 | −0.23 21 | <0.001 | −1.47 21 | <0.001 |
| 6-day cycle | −4.21 9,21 | −2.37 9,21 | −2.93 9,21 | ||||
| 9-day cycle | 1.12 6 | 3.60 6 | 2.64 6 | ||||
| 21-day cycle | 3.88 3,6 | 6.36 3,6 | 5.50 3,6 | ||||
| Reaction time | 3-day cycle | −0.69 | 0.986 | 1.64 | 0.907 | 2.52 | 0.860 |
| 6-day cycle | −0.56 | 0.71 | 1.47 | ||||
| 9-day cycle | 0.04 | 2.41 | 3.50 | ||||
| 21-day cycle | −0.09 | 1.57 | 2.41 | ||||
| Cognitive flexibility | 3-day cycle | −3.24 21 | <0.001 | −3.02 21 | <0.001 | −2.88 21 | <0.001 |
| 6-day cycle | −3.74 21 | −4.53 21 | −4.62 21 | ||||
| 9-day cycle | 0.20 21 | −0.36 21 | −0.05 21 | ||||
| 21-day cycle | 5.25 3,6,9 | 4.90 3,6,9 | 5.18 3,6,9 | ||||
| Executive functioning | 3-day cycle | −3.52 21 | <0.001 | −3.21 21 | <0.001 | −3.10 21 | <0.001 |
| 6-day cycle | −4.78 21 | −5.51 21 | −5.39 21 | ||||
| 9-day cycle | −0.46 21 | −0.83 21 | −0.59 21 | ||||
| 21-day cycle | 4.77 3,6,9 | 4.42 3,6,9 | 4.80 3,6,9 | ||||
| Neurocognitive index | 3-day cycle | 1.46 | 0.291 | 2.19 | 0.269 | 1.52 | 0.225 |
| 6-day cycle | 1.57 | 1.77 | 2.92 | ||||
| 9-day cycle | 2.35 | 3.00 | 4.55 | ||||
| 21-day cycle | 3.99 | 4.53 | 2.07 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwak, K.; Kim, B.-K.; Jang, T.-W.; Sim, C.S.; Ahn, Y.-S.; Choi, K.-S.; Jeong, K.S. Association between Shift Work and Neurocognitive Function among Firefighters in South Korea: A Prospective before–after Study. Int. J. Environ. Res. Public Health 2020, 17, 4647. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134647
Kwak K, Kim B-K, Jang T-W, Sim CS, Ahn Y-S, Choi K-S, Jeong KS. Association between Shift Work and Neurocognitive Function among Firefighters in South Korea: A Prospective before–after Study. International Journal of Environmental Research and Public Health. 2020; 17(13):4647. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134647
Chicago/Turabian StyleKwak, Kyeongmin, Bong-Kyu Kim, Tae-Won Jang, Chang Sun Sim, Yeon-Soon Ahn, Kyeong-Sook Choi, and Kyoung Sook Jeong. 2020. "Association between Shift Work and Neurocognitive Function among Firefighters in South Korea: A Prospective before–after Study" International Journal of Environmental Research and Public Health 17, no. 13: 4647. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134647