The Burden of Endometriosis on Women’s Lifespan: A Narrative Overview on Quality of Life and Psychosocial Wellbeing

 ,
,  , ,
, ,
Abstract
:1. Introduction
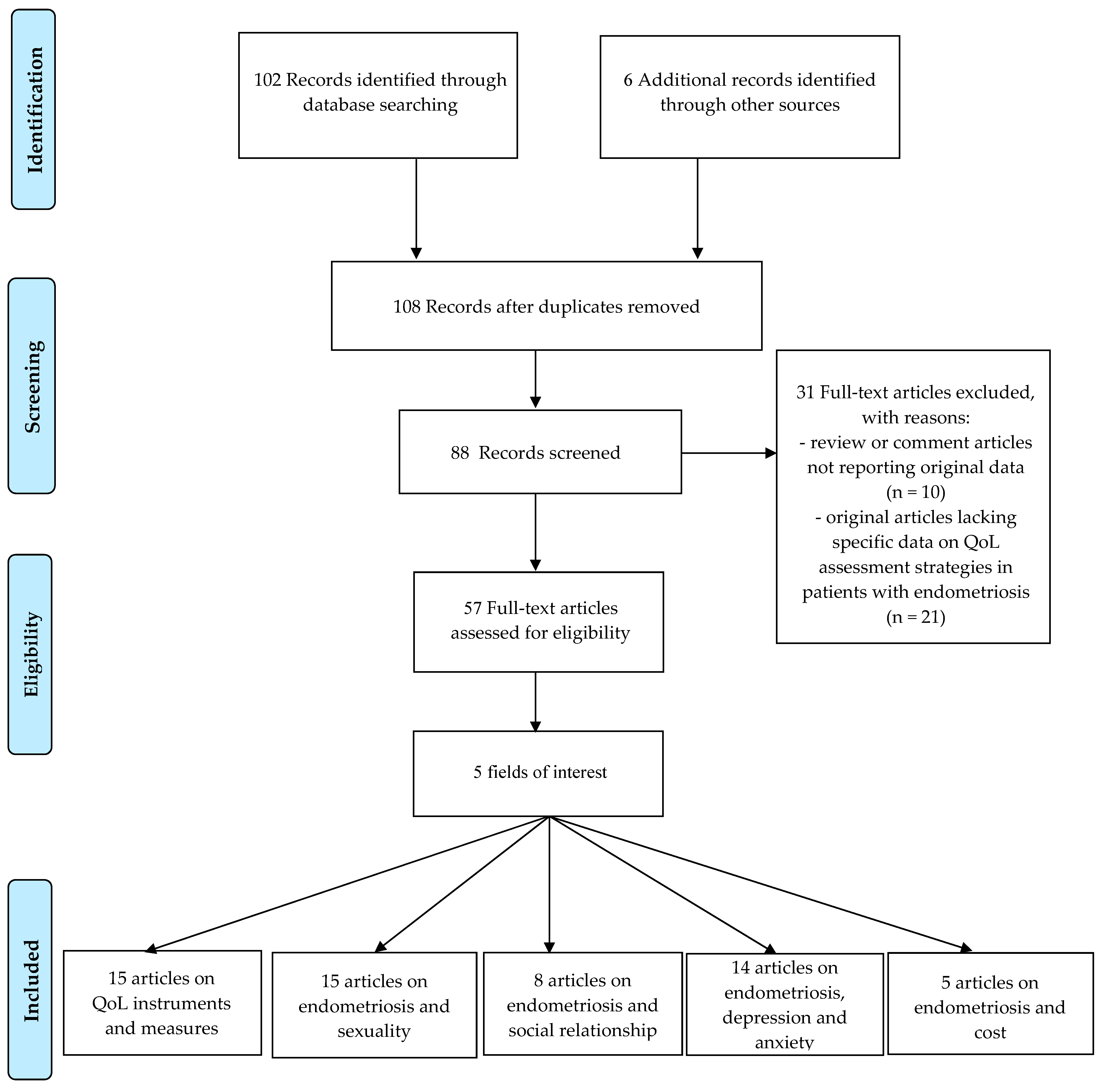
2. Materials and Methods
3. QoL Instruments
3.1. QoL Instruments and Measures for Endometriosis
3.2. Endometriosis and Sexuality
3.3. Endometriosis and Social Relationships
3.4. Endometriosis, Depression and Anxiety
3.5. “Costs” of Endometriosis
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Vitale, S.G.; Capriglione, S.; Peterlunger, I.; La Rosa, V.L.; Vitagliano, A.; Noventa, M.; Valenti, G.; Sapia, F.; Angioli, R.; Lopez, S.; et al. The Role of Oxidative Stress and Membrane Transport Systems during Endometriosis: A Fresh Look at a Busy Corner. Oxid. Med. Cell. Longev. 2018, 2018, 7924021. [Google Scholar] [CrossRef]
- Giudice, L.C. Clinical Practice. Endometriosis. N. Engl. J. Med. 2010, 362, 2389–2398. [Google Scholar] [CrossRef] [PubMed]
- Maniglio, P.; Ricciardi, E.; Meli, F.; Vitale, S.G.; Noventa, M.; Vitagliano, A.; Valenti, G.; La Rosa, V.L.; Lagana, A.S.; Caserta, D. Catamenial pneumothorax caused by thoracic endometriosis. Radiol. Case Rep. 2018, 13, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Tsakiridis, K.; Triantafilopoulou, K.; Minadakis, G.; Zatagias, A.; Sapalidis, K.; Kosmidis, C.; Ioannidis, A.; Romanidis, K.; Oikonomou, P.; Sevva, C.; et al. Catamenial Pneumothorax Recurrence due to Endometriosis. Respir. Med. Case Rep. 2020, 30, 101036. [Google Scholar] [CrossRef] [PubMed]
- Hickey, M.; Ballard, K.; Farquhar, C. Endometriosis. BMJ 2014, 348, g1752. [Google Scholar] [CrossRef] [PubMed]
- Falcone, T.; Flyckt, R. Clinical Management of Endometriosis. Obstet. Gynecol. 2018, 131, 557–571. [Google Scholar] [CrossRef] [Green Version]
- Burney, R.O.; Giudice, L.C. Pathogenesis and Pathophysiology of Endometriosis. Fertil. Steril. 2012, 98, 511–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagana, A.S.; Vitale, S.G.; Salmeri, F.M.; Triolo, O.; Ban Frangez, H.; Vrtacnik-Bokal, E.; Stojanovska, L.; Apostolopoulos, V.; Granese, R.; Sofo, V. Unus pro omnibus, omnes pro uno: A novel, evidence-based, unifying theory for the pathogenesis of endometriosis. Med. Hypotheses 2017, 103, 10–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giampaolino, P.; Della Corte, L.; Foreste, V.; Barra, F.; Ferrero, S.; Bifulco, G. Dioxin and endometriosis: A new possible relation based on epigenetic theory. Gynecol. Endocrinol. 2019, 1–6. [Google Scholar] [CrossRef]
- Cramer, D.W.; Missmer, S.A. The epidemiology of endometriosis. Ann. N. Y. Acad. Sci. 2002, 955, 11–22; discussion 34–41, 396–406. [Google Scholar] [CrossRef] [PubMed]
- Fichera, M.; Torok, P.; Tesarik, J.; Della Corte, L.; Rizzo, G.; Garzon, S.; Carlea, A.; Di Angelo Antonio, S.; Zito, G.; Panella, M.M.; et al. Reproductive Disorders and assisted reproduction: Evidences and perspectives. Int. J. Food Sci. Nutr. 2020, 71, 276–285. [Google Scholar] [CrossRef] [PubMed]
- Karadadaş, E.; Hortu, İ.; Ak, H.; Mete Ergenoğlu, A.; Karadadaş, N.; Hakan Aydın, H. Evaluation of complement system proteins C3a, C5a, and C6 in patients of endometriosis. Clin. Biochem 2020, 20, 15–19. [Google Scholar] [CrossRef]
- Seracchioli, R.; Poggioli, G.; Pierangeli, F.; Manuzzi, L.; Gualerzi, B.; Savelli, L.; Remorgida, V.; Mabrouk, M.; Venturoli, S. Surgical outcome and long-term follow up after laparoscopic rectosigmoid resection in women with deep infiltrating endometriosis. BJOG 2007, 114, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Vitale, S.G.; La Rosa, V.L.; Vitagliano, A.; Noventa, M.; Laganà, F.M.; Ardizzone, A.; Rapisarda, A.M.C.; Terzic, M.M.; Terzic, S.; Laganà, A.S. Sexual Function and Quality of Life in Patients Affected by Deep Infiltrating Endometriosis: Current Evidence and Future Perspectives. J. Endometr. Pelvic. Pain. Disord. 2018, 9, 270–274. [Google Scholar] [CrossRef]
- Koninckx, P.R.; Martin, D. Treatment of deeply infiltrating endometriosis. Curr. Opin. Obstet. Gynecol. 1994, 6, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Gordts, S.; Koninckx, P.; Brosens, I. Pathogenesis of deep endometriosis. Fertil. Steril. 2017, 108, 872–885.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butticè, S.; Laganà, A.S.A.S.; Mucciardi, G.; Marson, F.; Tefik, T.; Netsch, C.; Vitale, S.G.S.G.; Sener, E.; Pappalardo, R.; Magno, C. Different patterns of pelvic ureteral endometriosis. What is the best treatment? Results of a retrospective analysis. Arch. Ital. Urol. Androl. 2016, 88, 266–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laganà, A.S.; Vitale, S.G.; Trovato, M.A.; Palmara, V.I.; Rapisarda, A.M.C.; Granese, R.; Sturlese, E.; De Dominici, R.; Alecci, S.; Padula, F.; et al. Full-Thickness Excision versus Shaving by Laparoscopy for Intestinal Deep Infiltrating Endometriosis: Rationale and Potential Treatment Options. BioMed Res. Int. 2016, 2016, 3617179. [Google Scholar] [CrossRef] [Green Version]
- Giampaolino, P.; Della Corte, L.; Saccone, G.; Vitagliano, A.; Bifulco, G.; Calagna, G.; Carugno, J.; Di Spiezio Sardo, A. Role of Ovarian Suspension in Preventing Postsurgical Ovarian Adhesions in Patients with Stage III-IV Pelvic Endometriosis: A Systematic Review. J. Minim. Invasive Gynecol. 2019, 26, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Caruso, S.; Iraci, M.; Cianci, S.; Vitale, S.G.; Fava, V.; Cianci, A. Effects of long-term treatment with Dienogest on the quality of life and sexual function of women affected by endometriosis-associated pelvic pain. J. Pain Res. 2019, 12, 2371–2378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darai, E.; Ploteau, S.; Ballester, M.; Bendifallah, S. Pathogenesis, Genetics and Diagnosis of Endometriosis. Presse Med. 2017, 46, 1156–1165. [Google Scholar] [CrossRef]
- Bazot, M.; Bornier, C.; Dubernard, G.; Roseau, G.; Cortez, A.; Darai, E. Accuracy of magnetic resonance imaging and rectal endoscopic sonography for the prediction of location of deep pelvic endometriosis. Hum. Reprod. 2007, 22, 1457–1463. [Google Scholar] [CrossRef] [Green Version]
- Noventa, M.; Scioscia, M.; Schincariol, M.; Cavallin, F.; Pontrelli, G.; Virgilio, B.; Vitale, S.G.; Lagana, A.S.; Dessole, F.; Cosmi, E.; et al. Imaging Modalities for Diagnosis of Deep Pelvic Endometriosis: Comparison between Trans-Vaginal Sonography, Rectal Endoscopy Sonography and Magnetic Resonance Imaging. A Head-to-Head Meta-Analysis. Diagnostics (Basel) 2019, 9, 225. [Google Scholar] [CrossRef] [Green Version]
- Elgafor El Sharkwy, I.A. Combination of non-invasive and semi-invasive tests for diagnosis of minimal to mild endometriosis. Arch. Gynecol. Obstet. 2013, 288, 793–797. [Google Scholar] [CrossRef]
- Johnson, N.P.; Hummelshoj, L. Consensus on current management of endometriosis. Hum. Reprod. 2013, 28, 1552–1568. [Google Scholar] [CrossRef]
- Taylor, H.S.; Giudice, L.C.; Lessey, B.A.; Abrao, M.S.; Kotarski, J.; Archer, D.F.; Diamond, M.P.; Surrey, E.; Johnson, N.P.; Watts, N.B.; et al. Treatment of Endometriosis-Associated Pain with Elagolix, an Oral GnRH Antagonist. N. Engl. J. Med. 2017, 377, 28–40. [Google Scholar] [CrossRef]
- Laganà, A.S.; Vitale, S.G.; Granese, R.; Palmara, V.; Ban Frangež, H.; Vrtačnik-Bokal, E.; Chiofalo, B.; Triolo, O. Clinical dynamics of Dienogest for the treatment of endometriosis: From bench to bedside. Expert Opin. Drug Metab. Toxicol. 2017, 13, 593–596. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, C. ACOG updates guideline on diagnosis and treatment of endometriosis. Am. Fam. Physician 2011, 83, 84–85. [Google Scholar]
- Peiris, A.N.; Chaljub, E.; Medlock, D. Endometriosis. JAMA 2018, 320, 2608. [Google Scholar] [CrossRef] [Green Version]
- Setälä, M.; Härkki, P.; Matomäki, J.; Mäkinen, J.; Kössi, J. Sexual functioning, quality of life and pelvic pain 12 months after endometriosis surgery including vaginal resection. Acta Obstet. Gynecol. Scand. 2012, 91, 692–698. [Google Scholar] [CrossRef]
- Vitale, S.G. The Biopsy Snake Grasper Sec. VITALE: A New Tool for Office Hysteroscopy. J. Minim. Invasive Gynecol. 2019. [Google Scholar] [CrossRef]
- Di Spiezio Sardo, A.; Calagna, G.; Santangelo, F.; Zizolfi, B.; Tanos, V.; Perino, A.; De Wilde, R.L. The Role of Hysteroscopy in the Diagnosis and Treatment of Adenomyosis. BioMed Res. Int. 2017, 2017, 2518396. [Google Scholar] [CrossRef]
- Young, K.; Fisher, J.; Kirkman, M. Women’s experiences of endometriosis: A systematic review and synthesis of qualitative research. J. Fam. Plann. Reprod. Health Care 2015, 41, 225–234. [Google Scholar] [CrossRef]
- Culley, L.; Law, C.; Hudson, N.; Denny, E.; Mitchell, H.; Baumgarten, M.; Raine-Fenning, N. The social and psychological impact of endometriosis on women’s lives: A critical narrative review. Hum. Reprod. Update 2013, 19, 625–639. [Google Scholar] [CrossRef] [Green Version]
- Laganà, A.S.; La Rosa, V.L.; Rapisarda, A.M.C.; Valenti, G.; Sapia, F.; Chiofalo, B.; Rossetti, D.; Ban Frangež, H.; Vrtačnik Bokal, E.; Giovanni Vitale, S. Anxiety and depression in patients with endometriosis: Impact and management challenges. Int. J. Womens Health 2017, 9, 323–330. [Google Scholar] [CrossRef] [Green Version]
- Rush, G.; Misajon, R. Examining subjective wellbeing and health-related quality of life in women with endometriosis. Health Care Women Int. 2018, 39, 303–321. [Google Scholar] [CrossRef]
- Gilmour, J.A.; Huntington, A.; Wilson, H.V. The impact of endometriosis on work and social participation. Int. J. Nurs. Pract. 2008, 14, 443–448. [Google Scholar] [CrossRef]
- Carr, A.; Higginson, I.; Robinson, P.G. Quality of Life; BMJ: London, UK, 2003; p. vii. 133p. [Google Scholar]
- Moradi, M.; Parker, M.; Sneddon, A.; Lopez, V.; Ellwood, D. Impact of endometriosis on women’s lives: A qualitative study. BMC Womens Health 2014, 14, 123. [Google Scholar] [CrossRef] [Green Version]
- Marinho, M.C.P.; Magalhaes, T.F.; Fernandes, L.F.C.; Augusto, K.L.; Brilhante, A.V.M.; Bezerra, L. Quality of Life in Women with Endometriosis: An Integrative Review. J. Womens Health (Larchmt) 2018, 27, 399–408. [Google Scholar] [CrossRef]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Lovkvist, L.; Bostrom, P.; Edlund, M.; Olovsson, M. Age-Related Differences in Quality of Life in Swedish Women with Endometriosis. J. Womens Health (Larchmt) 2016, 25, 646–653. [Google Scholar] [CrossRef]
- Gandek, B.; Ware, J.E.; Aaronson, N.K.; Apolone, G.; Bjorner, J.B.; Brazier, J.E.; Bullinger, M.; Kaasa, S.; Leplege, A.; Prieto, L.; et al. Cross-validation of item selection and scoring for the SF-12 Health Survey in nine countries: Results from the IQOLA Project. International Quality of Life Assessment. J. Clin. Epidemiol. 1998, 51, 1171–1178. [Google Scholar] [CrossRef]
- The WHOQOL Group. Development of the World Health Organization WHOQOL-BREF Quality of Life Assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef] [Green Version]
- Bourdel, N.; Chauvet, P.; Billone, V.; Douridas, G.; Fauconnier, A.; Gerbaud, L.; Canis, M. Systematic review of quality of life measures in patients with endometriosis. PLoS ONE 2019, 14, e0208464. [Google Scholar] [CrossRef] [PubMed]
- Parkerson, G.R., Jr.; Broadhead, W.E.; Tse, C.K. The Duke Health Profile. A 17-item measure of health and dysfunction. Med. Care 1990, 28, 1056–1072. [Google Scholar] [CrossRef]
- EuroQol, G. EuroQol--A new facility for the measurement of health-related quality of life. Health Policy (Amst. Neth.) 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Sintonen, H. The 15D instrument of health-related quality of life: Properties and applications. Ann. Med. 2001, 33, 328–336. [Google Scholar] [CrossRef] [PubMed]
- Soliman, A.M.; Coyne, K.S.; Gries, K.S.; Castelli-Haley, J.; Snabes, M.C.; Surrey, E.S. The Effect of Endometriosis Symptoms on Absenteeism and Presenteeism in the Workplace and at Home. J. Manag. Care Spec. Pharm. 2017, 23, 745–754. [Google Scholar] [CrossRef]
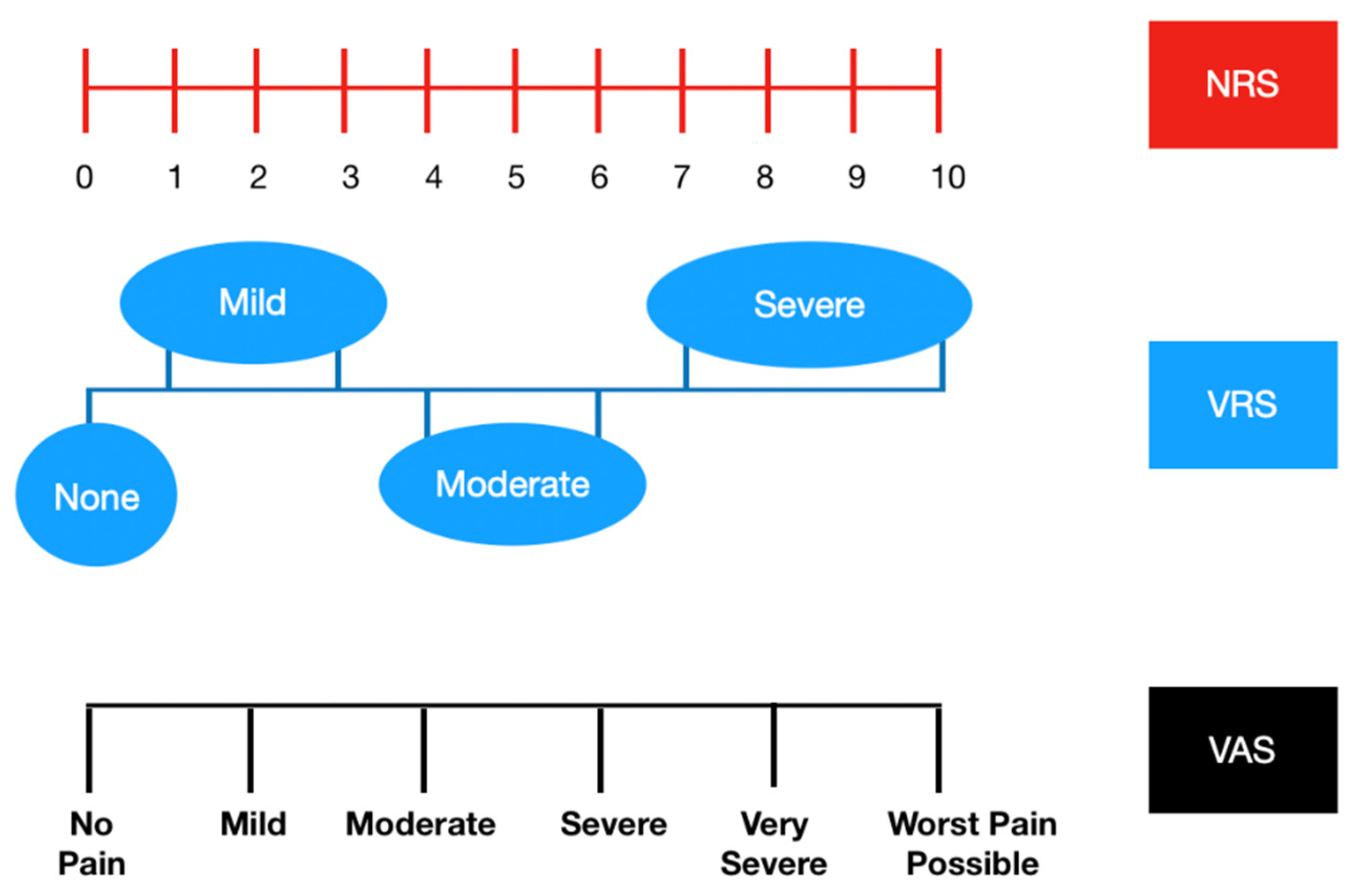
- Gerlinger, C.; Schumacher, U.; Wentzeck, R.; Uhl-Hochgräber, K.; Solomayer, E.F.; Schmitz, H.; Faustmann, T.; Seitz, C. How can we measure endometriosis-associated pelvic pain? J. Endometr. 2012, 4, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Thong, I.S.K.; Jensen, M.P.; Miro, J.; Tan, G. The validity of pain intensity measures: What do the NRS, VAS, VRS, and FPS-R measure? Scand. J. Pain 2018, 18, 99–107. [Google Scholar] [CrossRef]
- Pokrzywinski, R.; Soliman, A.M.; Chen, J.; Snabes, M.C.; Taylor, H.S.; Coyne, K.S. Responsiveness Evaluation and Recommendation for Responder Thresholds for Endometriosis Health Profile-30: Analysis of Two Phase III Clinical Trials. J. Womens Health (Larchmt) 2019. [Google Scholar] [CrossRef] [PubMed]
- Learman, L.A.; Huang, A.J.; Nakagawa, S.; Gregorich, S.E.; Kuppermann, M. Development and validation of a sexual functioning measure for use in diverse women’s health outcome studies. Am. J. Obstet. Gynecol. 2008, 198, 710.e1–710.e8; discussion 710.e8–710.e9. [Google Scholar] [CrossRef] [PubMed]
- ter Kuile, M.M.; Brauer, M.; Laan, E. The Female Sexual Function Index (FSFI) and the Female Sexual Distress Scale (FSDS): Psychometric properties within a Dutch population. J. Sex Marital Ther. 2006, 32, 289–304. [Google Scholar] [CrossRef]
- Derogatis, L.; Clayton, A.; Lewis-D’Agostino, D.; Wunderlich, G.; Fu, Y. Validation of the female sexual distress scale-revised for assessing distress in women with hypoactive sexual desire disorder. J. Sex. Med. 2008, 5, 357–364. [Google Scholar] [CrossRef]
- Jones, G.; Jenkinson, C.; Kennedy, S. Evaluating the responsiveness of the Endometriosis Health Profile Questionnaire: The EHP-30. Qual. Life Res. 2004, 13, 705–713. [Google Scholar] [CrossRef]
- Jones, G.; Jenkinson, C.; Kennedy, S. Development of the Short Form Endometriosis Health Profile Questionnaire: The EHP-5. Qual. Life Res. 2004, 13, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Mabrouk, M.; Del Forno, S.; Spezzano, A.; Raimondo, D.; Arena, A.; Zanello, M.; Leonardi, D.; Paradisi, R.; Seracchioli, R. Painful Love: Superficial Dyspareunia and Three Dimensional Transperineal Ultrasound Evaluation of Pelvic Floor Muscle in Women with Endometriosis. J. Sex Marital. Ther. 2019, 1–10. [Google Scholar] [CrossRef]
- Bernuit, D.; Ebert, A.D.; Halis, G.; Strothmann, A.; Gerlinger, C.; Geppert, K.; Faustmann, T. Female perspectives on endometriosis: Findings from the uterine bleeding and pain women’s research study. J. Endometr. 2011, 3, 73–85. [Google Scholar] [CrossRef]
- La Rosa, V.L.; De Franciscis, P.; Barra, F.; Schiattarella, A.; Tropea, A.; Tesarik, J.; Shah, M.; Kahramanoglu, I.; Marques Cerentini, T.; Ponta, M.; et al. Sexuality in women with endometriosis: A critical narrative review. Minerva Med. 2019. [Google Scholar] [CrossRef]
- La Rosa, V.L.; Barra, F.; Chiofalo, B.; Platania, A.; Di Guardo, F.; Conway, F.; Di Angelo Antonio, S.; Lin, L.T. An overview on the relationship between endometriosis and infertility: The impact on sexuality and psychological well-being. J. Psychosom. Obstet. Gynaecol. 2019, 1–5. [Google Scholar] [CrossRef]
- Rogers, R.G.; Pauls, R.N.; Thakar, R.; Morin, M.; Kuhn, A.; Petri, E.; Fatton, B.; Whitmore, K.; Kingsberg, S.A.; Lee, J. An international Urogynecological association (IUGA)/international continence society (ICS) joint report on the terminology for the assessment of sexual health of women with pelvic floor dysfunction. Int. Urogynecol. J. 2018, 29, 647–666. [Google Scholar] [CrossRef] [PubMed]
- Yong, P.J.; Williams, C.; Yosef, A.; Wong, F.; Bedaiwy, M.A.; Lisonkova, S.; Allaire, C. Anatomic Sites and Associated Clinical Factors for Deep Dyspareunia. Sex Med. 2017, 5, e184–e195. [Google Scholar] [CrossRef] [Green Version]
- Vercellini, P.; Somigliana, E.; Buggio, L.; Barbara, G.; Frattaruolo, M.P.; Fedele, L. “I can’t get no satisfaction”: Deep dyspareunia and sexual functioning in women with rectovaginal endometriosis. Fertil. Steril. 2012, 98, 1503–1511.e1. [Google Scholar] [CrossRef]
- Ferrero, S.; Esposito, F.; Abbamonte, L.H.; Anserini, P.; Remorgida, V.; Ragni, N. Quality of sex life in women with endometriosis and deep dyspareunia. Fertil. Steril. 2005, 83, 573–579. [Google Scholar] [CrossRef]
- Shum, L.K.; Bedaiwy, M.A.; Allaire, C.; Williams, C.; Noga, H.; Albert, A.; Lisonkova, S.; Yong, P.J. Deep Dyspareunia and Sexual Quality of Life in Women With Endometriosis. Sex Med. 2018, 6, 224–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cyranowski, J.M.; Frank, E.; Cherry, C.; Houck, P.; Kupfer, D.J. Prospective assessment of sexual function in women treated for recurrent major depression. J. Psychiatr. Res. 2004, 38, 267–273. [Google Scholar] [CrossRef]
- Bernays, V.; Schwartz, A.K.; Geraedts, K.; Rauchfuss, M.; Wolfler, M.M.; Haeberlin, F.; von Orelli, S.; Eberhard, M.; Imthurn, B.; Fink, D.; et al. Qualitative and quantitative aspects of sex life in the context of endometriosis: A multicentre case control study. Reprod. BioMed. Online 2020, 40, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Montanari, G.; Di Donato, N.; Benfenati, A.; Giovanardi, G.; Zannoni, L.; Vicenzi, C.; Solfrini, S.; Mignemi, G.; Villa, G.; Mabrouk, M.; et al. Women with deep infiltrating endometriosis: Sexual satisfaction, desire, orgasm, and pelvic problem interference with sex. J. Sex Med. 2013, 10, 1559–1566. [Google Scholar] [CrossRef]
- Simonsen, S.M.; Stromberg, C.; Zoffmann, V.; Hartwell, D.; Olesen, M.L. About me as a person not only the disease—piloting Guided Self-Determination in an outpatient endometriosis setting. Scand. J. Caring Sci. 2019. [Google Scholar] [CrossRef]
- Fritzer, N.; Hudelist, G. Love is a pain? Quality of sex life after surgical resection of endometriosis: A review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 209, 72–76. [Google Scholar] [CrossRef]
- Vercellini, P.; Somigliana, E.; Consonni, D.; Frattaruolo, M.P.; De Giorgi, O.; Fedele, L. Surgical versus medical treatment for endometriosis-associated severe deep dyspareunia: I. Effect on pain during intercourse and patient satisfaction. Hum. Reprod. 2012, 27, 3450–3459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Graaff, A.A.; D’Hooghe, T.M.; Dunselman, G.A.; Dirksen, C.D.; Hummelshoj, L.; Simoens, S. The significant effect of endometriosis on physical, mental and social wellbeing: Results from an international cross-sectional survey. Hum. Reprod. 2013, 28, 2677–2685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seear, K. The etiquette of endometriosis: Stigmatisation, menstrual concealment and the diagnostic delay. Soc. Sci. Med. 2009, 69, 1220–1227. [Google Scholar] [CrossRef] [PubMed]
- Young, K.; Fisher, J.; Kirkman, M. Clinicians’ perceptions of women’s experiences of endometriosis and of psychosocial care for endometriosis. Aust. N. Z. J. Obstet. Gynaecol. 2017, 57, 87–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fagervold, B.; Jenssen, M.; Hummelshoj, L.; Moen, M.H. Life after a diagnosis with endometriosis—A 15 years follow-up study. Acta Obstet. Gynecol. Scand. 2009, 88, 914–919. [Google Scholar] [CrossRef]
- Culley, L.; Law, C.; Hudson, N.; Mitchell, H.; Denny, E.; Raine-Fenning, N. A qualitative study of the impact of endometriosis on male partners. Hum. Reprod. 2017, 32, 1667–1673. [Google Scholar] [CrossRef]
- La Rosa, V.L.; De Franciscis, P.; Barra, F.; Schiattarella, A.; Torok, P.; Shah, M.; Karaman, E.; Marques Cerentini, T.; Di Guardo, F.; Gullo, G.; et al. Quality of life in women with endometriosis: A narrative overview. Minerva Med. 2019. [Google Scholar] [CrossRef]
- Cavaggioni, G.; Lia, C.; Resta, S.; Antonielli, T.; Benedetti Panici, P.; Megiorni, F.; Porpora, M.G. Are mood and anxiety disorders and alexithymia associated with endometriosis? A preliminary study. BioMed Res. Int. 2014, 2014, 786830. [Google Scholar] [CrossRef]
- Chen, L.C.; Hsu, J.W.; Huang, K.L.; Bai, Y.M.; Su, T.P.; Li, C.T.; Yang, A.C.; Chang, W.H.; Chen, T.J.; Tsai, S.J.; et al. Risk of developing major depression and anxiety disorders among women with endometriosis: A longitudinal follow-up study. J. Affect. Disord. 2016, 190, 282–285. [Google Scholar] [CrossRef] [PubMed]
- Roth, R.S.; Punch, M.; Bachman, J.E. Psychological factors in chronic pelvic pain due to endometriosis: A comparative study. Gynecol. Obstet. Investig. 2011, 72, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Tripoli, T.M.; Sato, H.; Sartori, M.G.; de Araujo, F.F.; Girao, M.J.; Schor, E. Evaluation of quality of life and sexual satisfaction in women suffering from chronic pelvic pain with or without endometriosis. J. Sex Med. 2011, 8, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Sepulcri Rde, P.; do Amaral, V.F. Depressive symptoms, anxiety, and quality of life in women with pelvic endometriosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2009, 142, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Arion, K.; Orr, N.L.; Noga, H.; Allaire, C.; Williams, C.; Bedaiwy, M.A.; Yong, P.J. A Quantitative Analysis of Sleep Quality in Women with Endometriosis. J. Womens Health (Larchmt) 2020. [Google Scholar] [CrossRef] [PubMed]
- Finan, P.H.; Goodin, B.R.; Smith, M.T. The association of sleep and pain: An update and a path forward. J Pain 2013, 14, 1539–1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roehrs, T.; Hyde, M.; Blaisdell, B.; Greenwald, M.; Roth, T. Sleep loss and REM sleep loss are hyperalgesic. Sleep 2006, 29, 145–151. [Google Scholar] [CrossRef]
- Roehrs, T.A.; Harris, E.; Randall, S.; Roth, T. Pain sensitivity and recovery from mild chronic sleep loss. Sleep 2012, 35, 1667–1672. [Google Scholar] [CrossRef]
- Roberts, R.E.; Duong, H.T. The prospective association between sleep deprivation and depression among adolescents. Sleep 2014, 37, 239–244. [Google Scholar] [CrossRef] [Green Version]
- Gupta, R.; Dahiya, S.; Bhatia, M.S. Effect of depression on sleep: Qualitative or quantitative? Indian J. Psychiatry 2009, 51, 117–121. [Google Scholar] [CrossRef]
- Lagana, A.S.; Condemi, I.; Retto, G.; Muscatello, M.R.; Bruno, A.; Zoccali, R.A.; Triolo, O.; Cedro, C. Analysis of psychopathological comorbidity behind the common symptoms and signs of endometriosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 194, 30–33. [Google Scholar] [CrossRef]
- Simoens, S.; Dunselman, G.; Dirksen, C.; Hummelshoj, L.; Bokor, A.; Brandes, I.; Brodszky, V.; Canis, M.; Colombo, G.L.; DeLeire, T.; et al. The burden of endometriosis: Costs and quality of life of women with endometriosis and treated in referral centres. Hum. Reprod. 2012, 27, 1292–1299. [Google Scholar] [CrossRef] [Green Version]
- Fuldeore, M.; Yang, H.; Du, E.X.; Soliman, A.M.; Wu, E.Q.; Winkel, C. Healthcare utilization and costs in women diagnosed with endometriosis before and after diagnosis: A longitudinal analysis of claims databases. Fertil. Steril. 2015, 103, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Soliman, A.M.; Surrey, E.S.; Bonafede, M.; Nelson, J.K.; Vora, J.B.; Agarwal, S.K. Health Care Utilization and Costs Associated with Endometriosis Among Women with Medicaid Insurance. J. Manag. Care Spec. Pharm. 2019, 25, 566–572. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Questionnaires | Number of Questions | Domains | Scores | What Does it Assess? | References |
|---|---|---|---|---|---|
| Short Form 36 (SF-36) | 36 items | Eight domains: vitality, mental health, bodily pain, general health perceptions, physical, role-physical, social and role emotional functioning | Scores range from 0 to 100, with higher scores indicating better QoL | QoL | Ware JE Jr et al. [40] (1992) |
| Short Form 12 (SF-12) | 12 items | Eight domains: vitality, mental health, bodily pain, general health perceptions, physical, role-physical, social and role emotional functioning | Scores range from 0 to 100, with higher scores indicating better QoL | QoL | Gandek B et al. [41,42,43] (1998) |
| Nottingham Health Profile (NHP) | Part I: 38 items Part II: 7 items | Part I: six domains (physical abilities, pain, sleep, social isolation, emotional reactions and energy level) Part II: seven domains (problems on employment, jobs around the house, personal relationships, social and sex life, hobbies and holidays) | All questions have only yes/no answer options and each section score (maximum 100) is weighted. | QoL | Bourdel N et al. [44] (2019) |
| World Health Organization Quality of Life Assessment-BREF (WHOQOL-BREF) | 26 items | Four domains: physical, psychological, social, and environmental health | Scores for each item range from 1 to 5, with the highest score indicating the best QoL | QoL | The WHOQOL Group [45] (1998) |
| Duke Health Profile (DUKE) | 17 items | Six health measures (physical, mental, social, perceived health, and self-esteem) and four dysfunction measures (anxiety, depression, pain, and disability). | Scores for each measure range from 0 to 100. For health measures high score = good health; for dysfunction measures high score = poor health | QoL | Parkerson GR Jr et al. [46] (1990) |
| Euro QOL-5-dimension instrument (EQ-5D) | 5 items | Five dimensions: mobility, self-care, daily activities, pain, and emotional well-being (depression or anxiety) + EQ Visual Analog Scale (EQ-VAS) on health status | Scores expressed initially as a 5-digit number can be converted into a single weighted index score that describes the patient’s health state. + VAS with a grade ranging from 0 (the worst possible health status) to 100 (the best possible health status) | QoL | EuroQol Group [47] (1990) |
| 15-Dimensional (15D) | 15 items | Breathing, mental function, speech (communication), vision, mobility, usual activities, vitality, hearing, eating, elimination, sleeping, distress, discomfort and symptoms, sexual activity, and depression. | The single index score uses a 0–1 scale (1 corresponds to no problems on any dimension) | QoL | Sintonen H [48] (2001) |
| Health Related Productivity Questionnaire (HRPQ) | 9 items | Four sections evaluating also absenteeism (missed work hours at paid employment, in the home, or at educational activities) and presenteeism (reduced effectiveness during any work that is attempted) + an optional section for younger age-group patients and those pursuing education | Specific algorithm | Work productivity | Soliman AM et al. [49] (2017) |
| Personal Wellbeing Index (PWI) | 8 items | Seven domains: standard of living, achievement in life, relationships, safety, connection with the community, future safety, overall life satisfaction | Score range from 0 (completely dissatisfied) to 10 (completely satisfied) | SWB | Rush G et al. [35] (2018) |
| DYSP diary | Single items | Intensity of dyspareunia during 24 h | Absent (no discomfort during SI), Mild (tolerable discomfort), Moderate (SI interrupted), Severe (SI avoided) | Dysp | Pokrzywinski R et al. [50,51,52] (2020) |
| Questionnaire on Sexual Health Outcomes in Women (SHOW-Q) | 12 items | Sexual satisfaction, orgasm, sexual desire, and pelvic problem interference with intercourse | All items were scored on a scale from 0 to 100; higher scores represent better sexual function except for the fourth domain. The overall score corresponds to an average of the 12 articles | SQoL | Learman LA et al. [53] (2008) |
| Female Sexual Function Index (FSFI) | 19 items | Six domains: desire, subjective arousal, lubrication, orgasm, satisfaction, and pain | Each domain is scored from 0 to 6: higher scores indicate better sexual function. Total score of the questionnaire ranges from 2 to 36. | SQoL | ter Kuile MM et al. [54] (2006) |
| Female Sexual Distress Scale-Revised (FSDS-R) | 13 items | Sexual distress | Every item requires an answer that is rated from 0 (never) to 4 (always). The total score, ranging from 0 to 48 | SQoL | Derogatis L et al. [55] (2008) |
| Endometriosis Health Profile-30 (EHP-30) | Core instrument: 30 items Modular section: 23 items | Core items: pain, control and powerlessness, emotional well-being, social support, and self-image. Modular items: work, relationship with children, sexual relationship, feelings about medical profession, feelings about treatment, feelings about infertility | Each scale is standardized on a score ranging from 0 to 100, where the lowest score represents the best health status. | QoL | Jones G et al. [56] (2004) |
| Endometriosis Health Profile-5 (EHP-5) | 11 items | Core questionnaires (pain, control and powerlessness, emotions, social support, self-image) and modular questionnaires (work-life, relation with children, sexual intercourse, medical profession, treatment and infertility | Total score ranging on a scale from 0 (indicating best possible health status) to 100 (indicating worst possible health status). | QoL | Jones G et al. [57] (2004) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Della Corte, L.; Di Filippo, C.; Gabrielli, O.; Reppuccia, S.; La Rosa, V.L.; Ragusa, R.; Fichera, M.; Commodari, E.; Bifulco, G.; Giampaolino, P. The Burden of Endometriosis on Women’s Lifespan: A Narrative Overview on Quality of Life and Psychosocial Wellbeing. Int. J. Environ. Res. Public Health 2020, 17, 4683. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134683
Della Corte L, Di Filippo C, Gabrielli O, Reppuccia S, La Rosa VL, Ragusa R, Fichera M, Commodari E, Bifulco G, Giampaolino P. The Burden of Endometriosis on Women’s Lifespan: A Narrative Overview on Quality of Life and Psychosocial Wellbeing. International Journal of Environmental Research and Public Health. 2020; 17(13):4683. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134683
Chicago/Turabian StyleDella Corte, Luigi, Claudia Di Filippo, Olimpia Gabrielli, Sabrina Reppuccia, Valentina Lucia La Rosa, Rosalia Ragusa, Michele Fichera, Elena Commodari, Giuseppe Bifulco, and Pierluigi Giampaolino. 2020. "The Burden of Endometriosis on Women’s Lifespan: A Narrative Overview on Quality of Life and Psychosocial Wellbeing" International Journal of Environmental Research and Public Health 17, no. 13: 4683. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134683