Assessment of the Economic and Health-Care Impact of COVID-19 (SARS-CoV-2) on Public and Private Dental Surgeries in Spain: A Pilot Study


 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed on 8 May 2020).
- Abramovitz, I.; Palmon, A.; Levy, D.; Karabucak, B.; Kot-Limon, N.; Shay, B.; Kolokythas, A.; Almoznino, G. Dental care during the coronavirus disease 2019 (COVID-19) outbreak: Operatory considerations and clinical aspects. Quintessence Int. 2020, 51, 418–429. [Google Scholar]
- Spagnuolo, G.; De Vito, D.; Rengo, S.; Tatullo, M. COVID-19 Outbreak: An Overview on Dentistry. Int. J. Environ. Res. Public Health 2020, 17, 2094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo Giudice, R. The Severe Acute Respiratory Syndrome Coronavirus-2 (SARS CoV-2) in Dentistry. Management of Biological Risk in Dental Practice. Int. J. Environ. Res. Public Health 2020, 17, 3067. [Google Scholar] [CrossRef] [PubMed]
- Hua, C.; Liu, Z.; Wang, Q.; Yang, Z.; Xu, Q.H.; Zhang, J. Strategy of dental clinics to cope with the epidemic period of infectious diseases based on the experience of corona virus disease outbreak. Hua Xi Kou Qiang Yi Xue Za Zhi 2020, 38, 117. [Google Scholar]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coulthard, P. Dentistry and coronavirus (COVID-19)—Moral decision-making. Br. Dent. J. 2020, 228, 503–505. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Practices for Disease Prevention in Dental Settings: Basic Expectations for Safe Care; Department of Health and United States Human Services, National Center for Chronic Disease Prevention and Health Promotion, Oral Health Division: Atlanta, GA, USA, 2017.
- Zhang, Y.; Holmes, E.C. A Genomic Perspective on the Origin and Emergence of SARS-CoV-2. Cell 2020, 181, 223–227. [Google Scholar] [CrossRef]
- Cevik, M.; Bamford, C.; Ho, A. COVID-19 pandemic—A focused review for clinicians. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef]
- Modi, P.D.; Nair, G.; Uppe, A.; Modi, J.; Tuppekar, B.; Gharpure, A.S.; Langade, D. COVID-19 Awareness Among Healthcare Students and Professionals in Mumbai Metropolitan Region: A Questionnaire-Based Survey. Cureus 2020, 12, e7514. [Google Scholar] [CrossRef] [Green Version]
- Kamate, S.K.; Sharma, S.; Thakar, S.; Srivastava, D.; Sengupta, K.; Hadi, A.J.; Chaudhary, A.; Joshi, R.; Dhanker, K. Assessing Knowledge, Attitudes and Practices of dental practitioners regarding the COVID-19 pandemic: A multinational study. Dent. Med. Probl. 2020, 57, 11–17. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission routes of 2019-nCoV and controls in dental practice. Int. J. Oral Sci. 2020, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef]
- Sabino-Silva, R.; Jardim, A.C.G.; Siqueira, W.L. Coronavirus COVID-19 impacts to dentistry and potential salivary diagnosis. Clin. Oral. Investig. 2020, 24, 1619–1621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khader, Y.; Al Nsour, M.; Al-Batayneh, O.B.; Saadeh, R.; Bashier, H.; Alfaqih, M.; Al-Azzam, S. Dentists’ Awareness, Perception, and Attitude Regarding COVID-19 and Infection Control: Cross-Sectional Study among Jordanian Dentists. JMIR Public Health Surveill. 2020, 6, e18798. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.A.; Jouhar, R.; Ahmed, N.; Adnan, S.; Aftab, M.; Zafar, M.S.; Khurshid, Z. Fear and Practice Modifications among Dentists to Combat Novel Coronavirus Disease (COVID-19) Outbreak. Int. J. Environ. Res. Public Health 2020, 17, 2821. [Google Scholar] [CrossRef]
- Navarro-Mora, M.; Cartes-Velasques, R. Expectativas de especialización profesional en estudiantes de odontología. Revisión de literatura. Rev. Estomatol. Herediana 2015, 2, 158–166. [Google Scholar] [CrossRef]
- Moran, P.S.; Wuytack, F.; Turner, M.; Normand, C.; Brown, S.; Begley, C.; Daly, D. Economic burden of maternal morbidity—A systematic review of cost-of-illness studies. PLoS ONE 2020, 15, e0227377. [Google Scholar] [CrossRef]
- Pallavi, S.K.; Rajkumar, G.C. Professional practice among woman dentist. J. Int. Soc. Prev. Community Dent. 2011, 1, 14–19. [Google Scholar] [CrossRef]
- Panesar, K.; Dodson, T.; Lynch, J.; Bryson-Cahn, C.; Chew, L.; Dillon, J. Evolution of COVID-19 Guidelines for University of Washington Oral and Maxillofacial Surgery Patient Care. J. Oral Maxillofac. Surg. 2020, 78, 1136–1146. [Google Scholar] [CrossRef]
- Ather, A.; Patel, B.; Ruparel, N.B.; Diogenes, A.; Hargreaves, K.M. Coronavirus Disease 19 (COVID-19): Implications for Clinical Dental Care. J. Endod. 2020, 46, 584–595. [Google Scholar] [CrossRef] [PubMed]
- Baghizadeh Fini, M. What dentists need to know about COVID-19. Oral Oncol. 2020, 105, 104741. [Google Scholar] [CrossRef] [PubMed]
- SESPO. Available online: http://sespo.es/metodologia-de-investigacion-en-salud-publica-oral/ (accessed on 10 May 2020).
- Chang, H.; Huang, N.; Lee, C.H.; Hsu, Y.J.; Hsieh, C.J.; Chou, Y.J. The impact of the SARS epidemic on the utilization of medical services: SARS and the fear of SARS. Am. J. Public Health 2004, 94, 562–564. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Questionnaire Items | No. (%) |
|---|---|
| Sex | |
| Male | 142 (35.5) |
| Female | 258 (64.5) |
| Age | 4 (1) |
| Between 22–25 | 108 (27) |
| Between 26–35 | 138 (34.5) |
| Between 26–35 | 79 (19.8) |
| Between 56–65 | 67 (16.8) |
| 65 and older | 4 (1) |
| Type of surgery where you work: | |
| Exclusively private practice | 359 (89.9) |
| Exclusively public practice | 13 (3.3) |
| Public and private practice | 28 (7) |
| Do you work in more than one surgery? | |
| No | 218 (54.5) |
| Yes | 182 (45.5) |
| How many? | |
| 2 | 98 (24.5) |
| 3-4 | 58 (14.5) |
| More than 4 | 24 (6) |
| Are any of these surgeries franchises or dental insurance companies? | |
| No | 351 (37.8) |
| Yes | 49 (12.3) |
| Average number of patients seen per week: | |
| 1–20 | 25 (6.3) |
| 21–40 | 98 (24.5) |
| 41–60 | 140 (35) |
| More than 60 patients | 137 (34.3) |
| Speciality: | |
| Oral Surgery and Implantology | 76 (19) |
| Endodontics | 24 (6) |
| General Dentistry | 241 (60.3) |
| Paedodontics | 12 (3) |
| Orthodontics | 37 (9.3) |
| Prosthodontics | 10 (2.5) |
| Before the State of Alarm was declared (14th March) did you use FFP2 masks in routine dental practice? | |
| No | 383 (95.8) |
| Yes | 17 (4.3) |
| Did you manage to procure PPE (Personal Protective Equipment) for yourself and your colleagues once the State of Alarm had been declared? | |
| I was unable to procure any PPE | 243 (60.8) |
| Yes, I managed to procure caps, FFP2 masks and disposable gowns | 44 (11) |
| Yes, I managed to procure caps and masks | 26 (6.5) |
| Yes, I managed to procure caps or masks | 38 (9.5) |
| Yes, I managed to procure caps, FFP2 masks and disposable gowns. | 49 (12.3) |
| Regarding COVID-19 test: | |
| I was not tested | 385 (96.3) |
| I tested negative | 11 (2.8) |
| I tested positive | 4 (1) |
| If you tested positive, what type of symptoms did you have? | |
| Mild symptoms | 8 (2) |
| Serious symptoms (required hospitalisation) | 0 |
| Did any of your employees or non-dentist colleagues (receptionists, dental hygienists or clinic assistants) test positive for COVID-19? | |
| Some of those who were tested came back positive | 9 (2.3) |
| No one tested positive | 18 (4.5) |
| No one was tested | 373 (93.3) |
| Do you know any dentist who tested positive for COVID19? | |
| No | 300 (75) |
| Yes | 100 (25) |
| Do you know any dentist who died from COVID19? No Yes | 390 (97.5) 10 (2.5) |
| What percentage of patients called to cancel or informed of their intention to cancel previously scheduled appointments after the State of Alarm was declared on the 14th of March? | |
| Less than 10% | 344 (86) |
| 10–40% | 41 (10.3) |
| 40–70% | 12 (3) |
| More than 70% | 3 (0.8) |
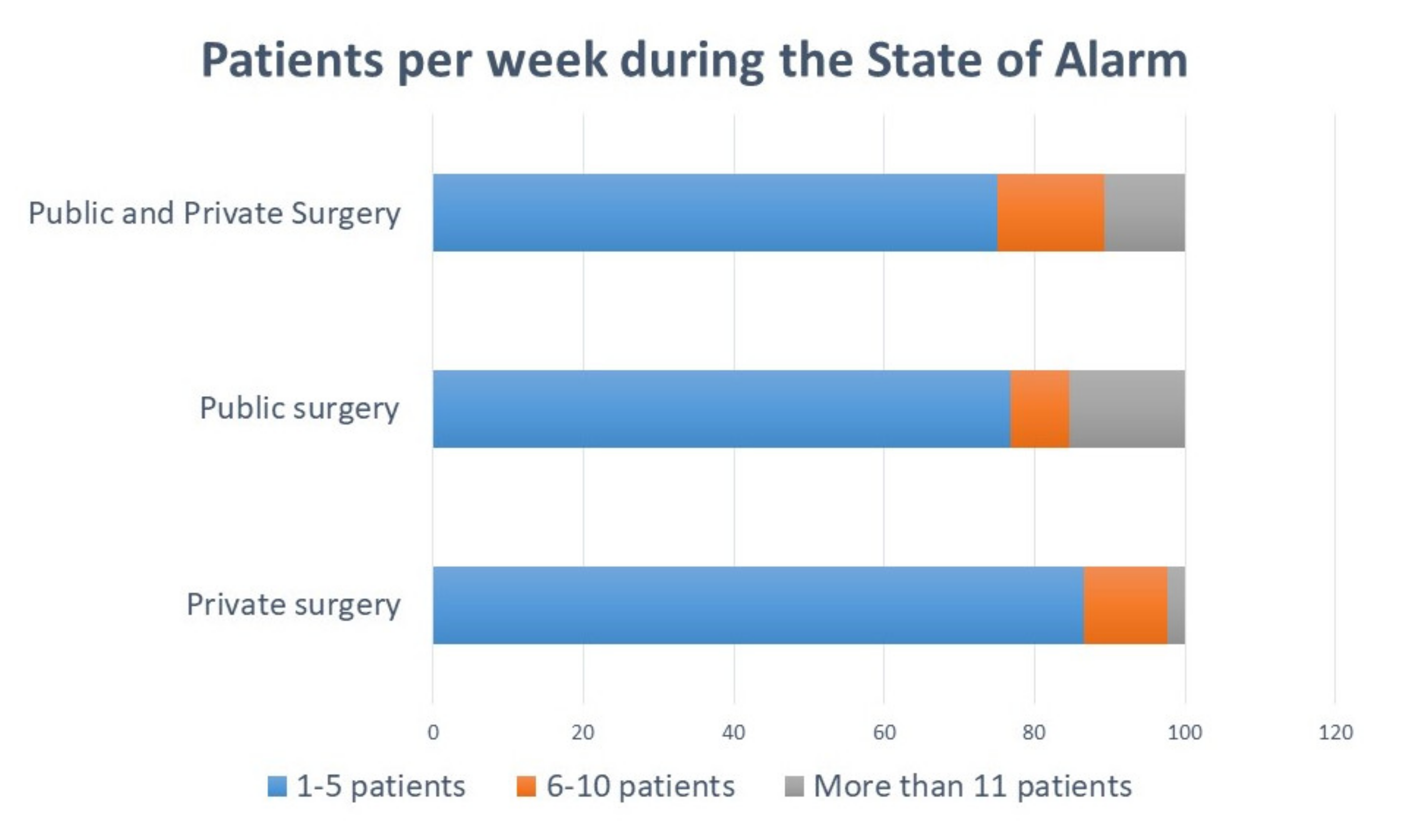
| How many patients did you see per week during the State of Alarm? | |
| 1–5 patients/week | 342 (85.5) |
| 6–10 patients/week | 45 (11.3) |
| More than 11 patients/week | 13 (3.3) |
| Did any of the patients request treatment for a situation which they considered to be a medical emergency but that you did not consider as such? | |
| No, or less than 10% | 254 (63.5) |
| Yes, between 10–30% | 112 (28) |
| Yes, between 31 and 60% | 22 (5.5) |
| More than 60% | 12 (3) |
| What percentage of patients expressed their dissatisfaction regarding the provision of dental care exclusively for emergency cases? | |
| Less than 10% | 344 (86) |
| 10–40% | 41 (10.3) |
| 40–70% | 12 (3) |
| More than 70% | 3 (0.8) |
| If you are the owner of the dental surgery, did you apply for a TERF (temporary employment regulation file) for any of the dental surgery’s staff? | |
| No | 43 (10.8) |
| Yes | 219 (54.8) |
| I am not the owner | 138 (34.4) |
| If you applied for a TERF, was it approved by the government? | |
| No | 19 (4.8) |
| Yes | 225 (56.3) |
| I did not apply for it | 156 (39) |
| If you work at a private surgery, what economic losses have been caused by the COVID-19 pandemic in terms of monthly income? | |
| 1,000–4,999 € | 108 (27) |
| 5,000-9,999 € | 102 (25.5) |
| 10,000–14,999 € | 79 (19.8) |
| More than 15,000 € | 97 (24.3) |
| I do not work at a private surgery | 14 (3.5) |
| Have any of the surgeries where you work closed down? | |
| No | 348 (87) |
| Yes | 52 (13) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chamorro-Petronacci, C.; Martin Carreras-Presas, C.; Sanz-Marchena, A.; A Rodríguez-Fernández, M.; María Suárez-Quintanilla, J.; Rivas-Mundiña, B.; Suárez-Quintanilla, J.; Pérez-Sayáns, M. Assessment of the Economic and Health-Care Impact of COVID-19 (SARS-CoV-2) on Public and Private Dental Surgeries in Spain: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 5139. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145139
Chamorro-Petronacci C, Martin Carreras-Presas C, Sanz-Marchena A, A Rodríguez-Fernández M, María Suárez-Quintanilla J, Rivas-Mundiña B, Suárez-Quintanilla J, Pérez-Sayáns M. Assessment of the Economic and Health-Care Impact of COVID-19 (SARS-CoV-2) on Public and Private Dental Surgeries in Spain: A Pilot Study. International Journal of Environmental Research and Public Health. 2020; 17(14):5139. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145139
Chicago/Turabian StyleChamorro-Petronacci, Cintia, Carmen Martin Carreras-Presas, Adriana Sanz-Marchena, María A Rodríguez-Fernández, José María Suárez-Quintanilla, Berta Rivas-Mundiña, Juan Suárez-Quintanilla, and Mario Pérez-Sayáns. 2020. "Assessment of the Economic and Health-Care Impact of COVID-19 (SARS-CoV-2) on Public and Private Dental Surgeries in Spain: A Pilot Study" International Journal of Environmental Research and Public Health 17, no. 14: 5139. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145139