Physical Activity, Screen Time, and Emotional Well-Being during the 2019 Novel Coronavirus Outbreak in China

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Procedures
2.3. Statistical Analysis
3. Results
3.1. Survey Respondents
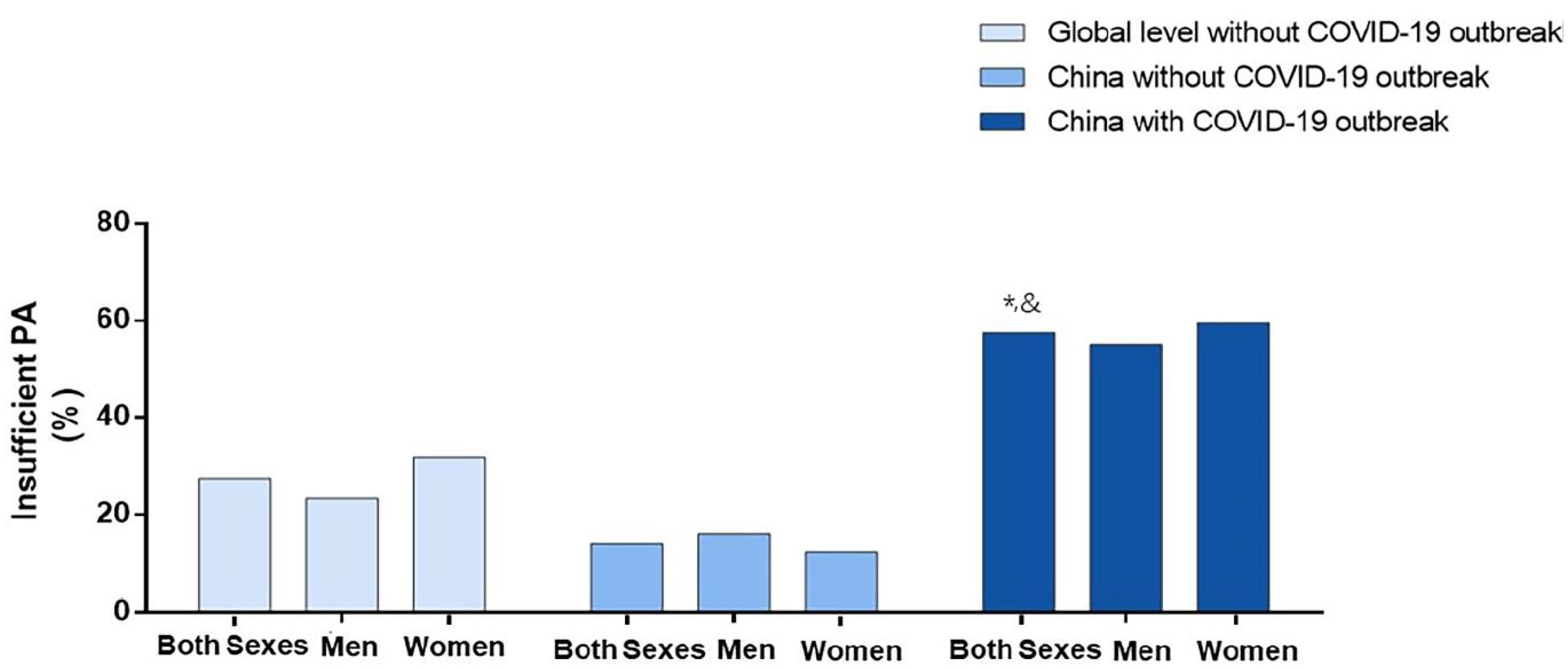
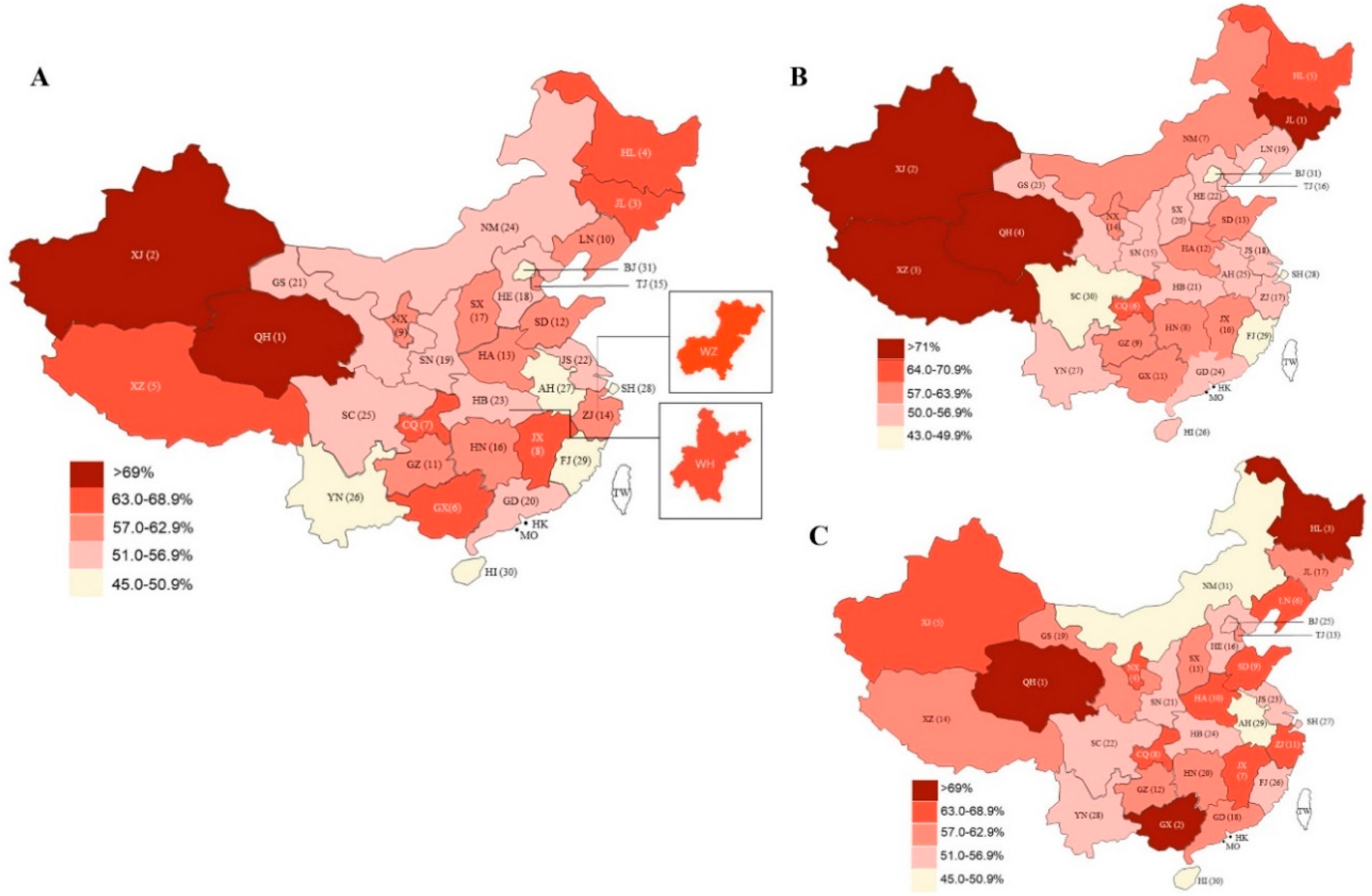
3.2. Physical Activity Impact
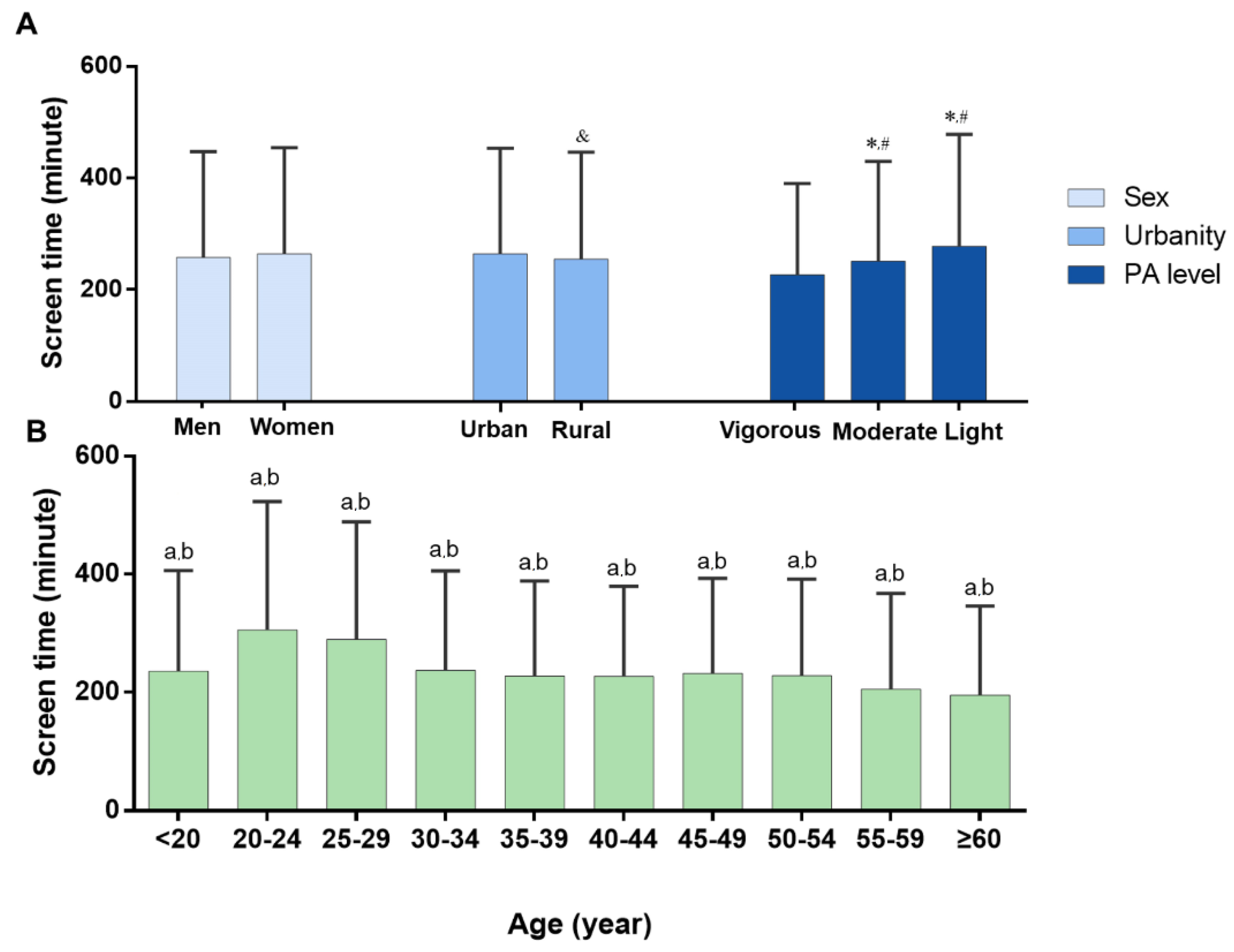
3.3. Screen Time Impact
3.4. Emotional Well-Being Impact
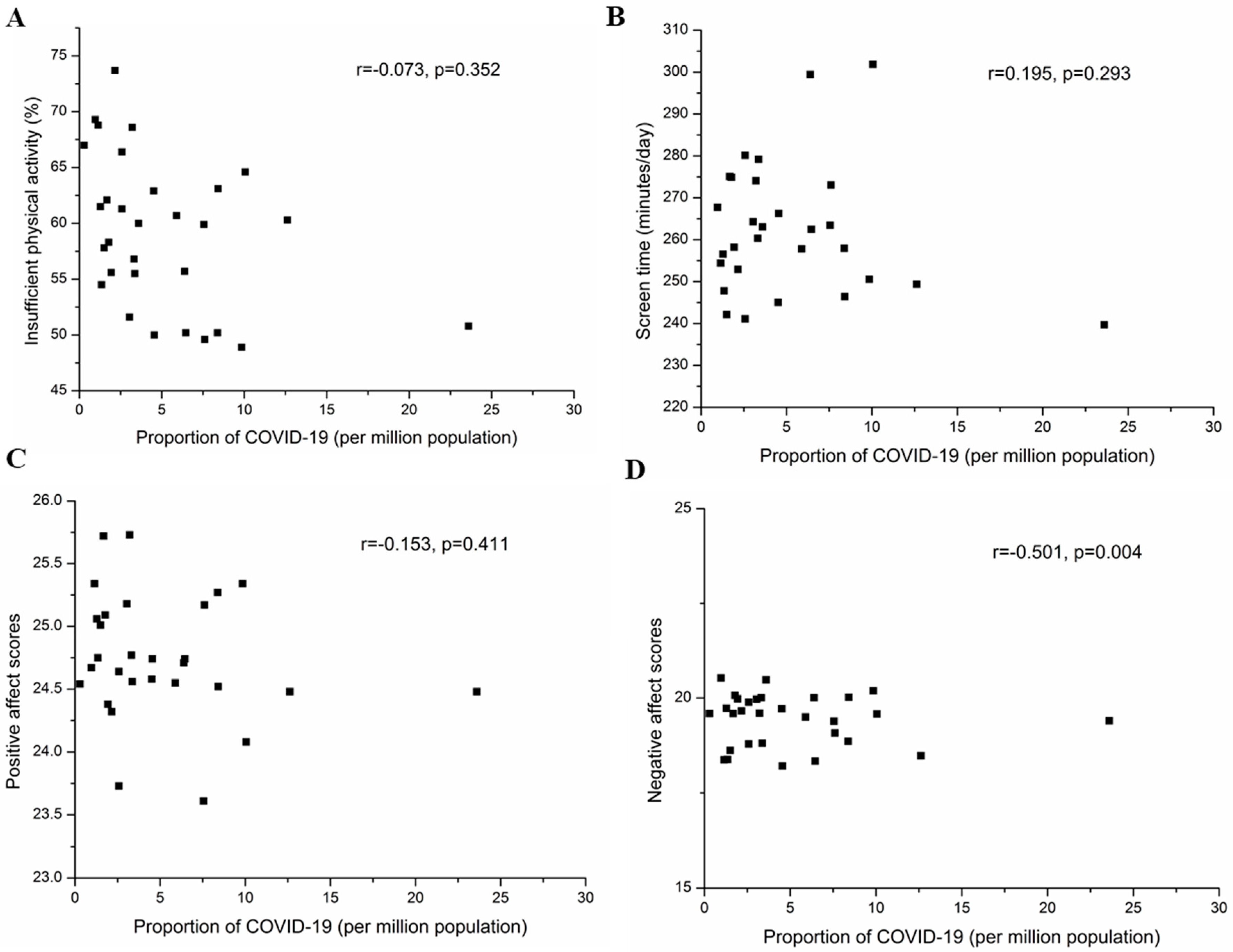
3.5. Correlations of Provincial Levels of Lifestyle and Emotional State with Proportion of Confirmed COVID-19 Cases in 31 Provinces of Mainland China
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Province | Targeted Survey Sampling Number | Total Population Size |
|---|---|---|
| Guangdong | 600 ± 200 | Large sample |
| Shandong | 600 ± 200 | Large sample |
| Henan | 600 ± 200 | Large sample |
| Sichuan | 600 ± 200 | Large sample |
| Jiangsu | 600 ± 200 | Large sample |
| Hebei | 600 ± 200 | Large sample |
| Hunan | 600 ± 200 | Large sample |
| Anhui | 600 ± 200 | Large sample |
| Hubei | 600 ± 200 | Large sample |
| Zhejiang | 600 ± 200 | Large sample |
| Beijing | 600 ± 200 | Large sample |
| Shanghai | 600 ± 200 | Large sample |
| Guangxi | 350 ± 100 | Medium sample |
| Yunnan | 350 ± 100 | Medium sample |
| Jiangxi | 350 ± 100 | Medium sample |
| Liaoning | 350 ± 100 | Medium sample |
| Heilongjiang | 350 ± 100 | Medium sample |
| Shananxi | 350 ± 100 | Medium sample |
| Fujian | 350 ± 100 | Medium sample |
| Shanxi | 350 ± 100 | Medium sample |
| Guizhou | 350 ± 100 | Medium sample |
| Chongqing | 200 ± 50 | Small sample |
| Jilin | 200 ± 50 | Small sample |
| Gansu | 200 ± 50 | Small sample |
| Inner mongolia | 200 ± 50 | Small sample |
| Xinjiang | 200 ± 50 | Small sample |
| Tianjin | 200 ± 50 | Small sample |
| Hainan | 150 ± 50 | Tiny sample |
| Ningxia | 150 ± 50 | Tiny sample |
| Qinghai | 150 ± 50 | Tiny sample |
| Tibet | 150 ± 50 | Tiny sample |
| Category | Criteria |
|---|---|
| Vigorous | meeting at least one of the following criteria (a) vigorous–intensity activity on at least 3 days achieving a minimum of at least 1500 MET–min/week OR (b) 7 or more days of any combination of walking, moderate–intensity or vigorous intensity activities achieving a minimum of at least 3000 MET–min/week |
| Moderate | (a) 3 or more days of vigorous activity of at least 25 min per day OR (b) 5 or more days of moderate–intensity activity or walking of at least 30 min per day OR (c) 5 or more days of any combination of walking, moderate–intensity or vigorous intensity activities achieving a minimum of at least 600 MET–min/week. |
| Light | Those individuals who not meet criteria for Categories 1 or 2 |
| Men and Women | Men | Women | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Sample Size | Number of Insufficient Physical Activity | The Prevalence of Insufficient Physical Activity % (95% CI) | Rank | Total Sample Size | Number of Insufficient Physical Activity | The Prevalence of Insufficient Physical Activity % (95% CI) | Rank | Total Sample Size | Number of Insufficient Physical Activity | The Prevalence of Insufficient Physical Activity % (95% CI) | Rank | |
| Qinghai | 133 | 98 | 73.7% (66.2–81.2) | 1 | 60 | 44 | 73.3% (61.7–83.3) | 4 | 73 | 54 | 74.0% (64.4–83.6) | 1 |
| Xinjiang | 137 | 95 | 69.3% (61.3–76.6) | 2 | 48 | 36 | 75.0% (60.4–85.4) | 2 | 89 | 59 | 66.3% (56.2–75.3) | 5 |
| Jilin | 160 | 110 | 68.8% (61.3–75.6) | 3 | 87 | 66 | 75.9% (66.7–85.1) | 1 | 73 | 44 | 60.3% (49.3–71.2) | 17 |
| Heilongjiang | 220 | 151 | 68.6% (62.7–74.5) | 4 | 77 | 52 | 67.5% (57.1–77.9) | 5 | 143 | 99 | 69.2% (61.5–76.2) | 3 |
| Tibet | 91 | 61 | 67.0% (57.1–75.8) | 5 | 39 | 29 | 74.4% (59.0–87.2) | 3 | 52 | 32 | 61.5% (48.1–73.1) | 14 |
| Guangxi | 330 | 219 | 66.4% (61.5–71.2) | 6 | 124 | 73 | 58.9% (50.0–67.7) | 11 | 146 | 206 | 70.9% (64.1–76.2) | 2 |
| Chongqing | 178 | 115 | 64.6% (57.9–71.9) | 7 | 99 | 64 | 64.6% (54.5–73.7) | 6 | 79 | 51 | 64.6% (54.5–74.7) | 8 |
| Jiangxi | 358 | 226 | 63.1% (57.8–68.2) | 8 | 161 | 97 | 60.2% (52.8–67.7) | 10 | 197 | 129 | 65.5% (58.9–72.1) | 7 |
| Ningxia | 240 | 151 | 62.9% (56.3–69.2) | 9 | 119 | 68 | 57.1% (47.9–65.5) | 14 | 121 | 83 | 68.6% (60.3–76.9) | 4 |
| Liaoning | 314 | 195 | 62.1% (56.7–67.2) | 10 | 120 | 67 | 55.8% (46.7–64.2) | 19 | 194 | 128 | 66.0% (59.3–72.7) | 6 |
| Guizhou | 161 | 99 | 61.5% (53.4–68.3) | 11 | 81 | 49 | 60.5% (49.4–71.6) | 9 | 80 | 50 | 62.5% (51.3–72.5) | 12 |
| Shandong | 952 | 584 | 61.3% (58.4–64.4) | 12 | 460 | 266 | 57.8% (53.5–62.2) | 13 | 492 | 318 | 64.6% (60.6–68.9) | 9 |
| Henan | 685 | 416 | 60.7% (57.1–64.5) | 13 | 350 | 203 | 58.0% (52.3–62.9) | 12 | 335 | 213 | 63.6% (58.5–68.7) | 10 |
| Zhejiang | 860 | 519 | 60.3% (57.2–63.7) | 14 | 349 | 195 | 55.9% (50.4–60.7) | 17 | 511 | 324 | 63.4% (59.3–67.7) | 11 |
| Tianjin | 130 | 78 | 60.0% (51.5–68.5) | 15 | 53 | 30 | 56.6% (43.4–69.8) | 16 | 77 | 48 | 62.3% (51.9–74.0) | 13 |
| Hunan | 544 | 326 | 59.9% (55.5–64.0) | 16 | 258 | 158 | 61.2% (55.4–67.1) | 8 | 286 | 168 | 58.7% (53.1–64.3) | 20 |
| Shanxi | 290 | 169 | 58.3% (52.4–64.1) | 17 | 142 | 79 | 55.6 (47.2–64.1) | 20 | 148 | 90 | 60.8% (52.7–68.9) | 15 |
| Hebei | 561 | 324 | 57.8% (53.8–61.5) | 18 | 258 | 140 | 54.3 (48.1–60.5) | 22 | 303 | 184 | 60.7% (55.1–66.3) | 16 |
| Shananxi | 243 | 138 | 56.8% (49.8–63.0) | 19 | 120 | 68 | 56.7% (48.3–65.8) | 15 | 123 | 70 | 56.9% (48.8–65.9) | 21 |
| Guangdong | 672 | 374 | 55.7% (51.9–59.5) | 20 | 314 | 161 | 51.3% (45.5–56.7) | 24 | 358 | 213 | 59.5% (54.7–64.8) | 18 |
| Gansu | 178 | 99 | 55.6% (48.3–62.4) | 21 | 74 | 38 | 51.4% (39.2–62.2) | 23 | 104 | 61 | 58.7% (49.0–67.3) | 19 |
| Jiangsu | 809 | 449 | 55.5% (52.2–58.7) | 22 | 354 | 198 | 55.9% (50.8–60.7) | 18 | 455 | 251 | 55.2% (50.3–59.3) | 23 |
| Hubei | 361 | 198 | 54.8% (49.6–59.8) | 23 | 147 | 81 | 55.1% (46.9–62.6) | 21 | 214 | 117 | 54.7% (48.1–61.7) | 24 |
| Inner Mongolia | 165 | 90 | 54.5% (47.3–61.8) | 24 | 80 | 49 | 61.3% (51.3–72.5) | 7 | 85 | 41 | 48.2% (37.6–58.8) | 31 |
| Sichuan | 461 | 238 | 51.6% (47.1–56.0) | 25 | 219 | 101 | 46.1% (39.7–53.4) | 30 | 242 | 137 | 56.6% (50.4–62.8) | 22 |
| Yunnan | 264 | 134 | 50.8% (45.1–56.4) | 26 | 162 | 82 | 50.6% (42.6–58.6) | 27 | 102 | 52 | 51.0% (41.2–59.8) | 28 |
| Anhui | 629 | 316 | 50.2% (46.3–54.2) | 27 | 337 | 172 | 51.0% (45.4–57.0) | 25 | 292 | 144 | 49.3% (43.5–55.5) | 29 |
| Shanghai | 957 | 480 | 50.2% (47.1–53.5) | 28 | 465 | 225 | 48.4% (44.3–53.5) | 28 | 492 | 255 | 51.8% (47.6–56.1) | 27 |
| Fujian | 268 | 134 | 50.0% (44.0–56.0) | 29 | 123 | 57 | 46.3% (37.4–54.5) | 29 | 145 | 77 | 53.1% (44.8–60.7) | 26 |
| Hainan | 139 | 69 | 49.6% (41.0–57.6) | 30 | 65 | 33 | 50.8% (38.5–63.1) | 26 | 74 | 36 | 48.6% (36.5–59.5) | 30 |
| Beijing | 617 | 302 | 48.9% (45.1–52.7) | 31 | 288 | 125 | 43.4% (37.2–49.0) | 31 | 329 | 177 | 53.8% (48.3–59.3) | 25 |
| China (total) | 12107 | 6957 | 57.5% (56.6–58.3) | 5633 | 3106 | 55.1% (53.9–56.6) | 6474 | 3851 | 59.5% (58.2–60.7) | |||
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- WHO. Coronavirus Disease (COVID-19) Outbreak Situation. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 9 June 2020).
- Shih, G.; Denyer, S. Chinese Coronavirus Infections, Death Toll Soar as Fifth Case Is Confirmed in U.S. Available online: https://www.washingtonpost.com/world/asia_pacific/coronavirus-china-latest-updates/2020/2001/2026/4603266c-4603263fa4603268-4603211ea-afe4603262-4603090eb4603237b4603260b4603261_story.html (accessed on 1 March 2020).
- Fifield, A. Travel Ban Goes into Effect in Chinese City of Wuhan as Authorities Try to Stop Coronavirus Spread. Available online: https://www.washingtonpost.com/world/asia_pacific/nine-dead-as-chinese-coronavirus-spreads-despite-efforts-to-contain-it/2020/01/22/1eaade72-3c6d-11ea-afe2-090eb37b60b1_story.html. (accessed on 1 March 2020).
- Khaliq, R. China Prolongs School Closure Amid Coronavirus Outbreak. Available online: https://www.aa.com.tr/en/asia-pacific/china-prolongs-school-closure-amid-coronavirus-outbreak/1716100 (accessed on 1 March 2020).
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Coronavirus disease (COVID-19): The need to maintain regular physical activity while taking precautions. J. Sport Health Sci. 2020, 9, 103–104. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T.W. Sedentary behavior as a mediator of type 2 diabetes. Med. Sport Sci. 2014, 60, 11–26. [Google Scholar] [CrossRef] [Green Version]
- Owen, N.; Sparling, P.B.; Healy, G.N.; Dunstan, D.W.; Matthews, C.E. Sedentary behavior: Emerging evidence for a new health risk. Mayo Clin. Proc. 2010, 85, 1138–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.T.; Leung, K.; Leung, G.M. Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: A modelling study. Lancet 2020, 395, 689–697. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.H.; Yu, Y.Y.; McDowell, I.; Leung, G.M.; Lam, T.H.; Stewart, S.M. Performance of the international physical activity questionnaire (short form) in subgroups of the Hong Kong chinese population. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 81. [Google Scholar] [CrossRef] [Green Version]
- Sjostrom, M. Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire–IPAQ (GDPA-IPAQ). Available online: https://www.academia.edu/5346814/Guidelines_for_Data_Processing_and_Analysis_of_the_International_Physical_Activity_Questionnaire_IPAQ_Short_and_Long_Forms_Contents (accessed on 1 March 2020).
- WHO. How Much of Physical Activity Is Recommended? Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 1 March 2020).
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Bey, L.; Hamilton, M.T. Suppression of skeletal muscle lipoprotein lipase activity during physical inactivity: A molecular reason to maintain daily low-intensity activity. J. Physiol. 2003, 551, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Jeon, S.W.; Lee, M.Y.; Shin, D.W.; Lim, W.J.; Shin, Y.C.; Oh, K.S. The association between physical activity and anxiety symptoms for general adult populations: An analysis of the dose-response relationship. Psychiatry Investig. 2020, 17, 29–36. [Google Scholar] [CrossRef]
- Mielke, G.I.; da Silva, I.C.M.; Kolbe-Alexander, T.L.; Brown, W.J. Shifting the physical inactivity curve worldwide by closing the gender gap. Sports Med. 2018, 48, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Tu, H.; Liao, X.; Schuller, K.; Cook, A.; Fan, S.; Lan, G.; Lu, Y.; Yuan, Z.; Moore, J.B.; Maddock, J.E. Insights from an observational assessment of park-based physical activity in Nanchang, China. Prev. Med. Rep. 2015, 2, 930–934. [Google Scholar] [CrossRef] [Green Version]
- Kari, J.T.; Viinikainen, J.; Böckerman, P.; Tammelin, T.H.; Pitkänen, N.; Lehtimäki, T.; Pahkala, K.; Hirvensalo, M.; Raitakari, O.T.; Pehkonen, J. Education leads to a more physically active lifestyle: Evidence based on Mendelian randomization. Scand. J. Med. Sci. Sports 2020, 30, 1194–1204. [Google Scholar] [CrossRef]
- Ranasinghe, C.D.; Ranasinghe, P.; Jayawardena, R.; Misra, A. Physical activity patterns among South-Asian adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 116. [Google Scholar] [CrossRef] [Green Version]
- Hills, A.P.; Farpour-Lambert, N.J.; Byrne, N.M. Precision medicine and healthy living: The importance of the built environment. Prog. Cardiovasc. Dis. 2019, 62, 34–38. [Google Scholar] [CrossRef]
- Kondo, M.C.; Fluehr, J.M.; McKeon, T.; Branas, C.C. Urban green space and its impact on human health. Int. J. Environ. Res. Public Health 2018, 15, 445. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.C.; Maheswaran, R. The health benefits of urban green spaces: A review of the evidence. J. Public Health (Oxf.) 2011, 33, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Varela, A.R.; Pratt, M.; Harris, J.; Lecy, J.; Salvo, D.; Brownson, R.C.; Hallal, P.C. Mapping the historical development of physical activity and health research: A structured literature review and citation network analysis. Prev. Med. 2018, 111, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Yeh, H.P.; Stone, J.A.; Churchill, S.M.; Wheat, J.S.; Brymer, E.; Davids, K. Physical, psychological and emotional benefits of green physical activity: An ecological dynamics perspective. Sports Med. 2016, 46, 947–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahart, I.; Darcy, P.; Gidlow, C.; Calogiuri, G. The effects of green exercise on physical and mental wellbeing: A systematic review. Int. J. Environ. Res. Public Health 2019, 16, 1352. [Google Scholar] [CrossRef] [Green Version]
- Fraser, M.; Munoz, S.A.; MacRury, S. What motivates participants to adhere to green exercise? Int. J. Environ. Res. Public Health 2019, 16, 1832. [Google Scholar] [CrossRef] [Green Version]
- Nie, M.J.; Fan, C.Q.; Sun, R.Z.; Wang, J.J.; Feng, Q.; Zhang, Y.F.; Yao, Z.; Wang, M. Accelerometer-measured physical activity in children and adolescents at altitudes over 3500 meters: A cross-sectional study in Tibet. Int. J. Environ. Res. Public Health 2019, 16, 686. [Google Scholar] [CrossRef] [Green Version]
- Stamatakis, E.; Hamer, M.; Dunstan, D.W. Screen-based entertainment time, all-cause mortality, and cardiovascular events: Population-based study with ongoing mortality and hospital events follow-up. J. Am. Coll. Cardiol. 2011, 57, 292–299. [Google Scholar] [CrossRef]
- Wang, X.; Li, Y.; Fan, H. The associations between screen time-based sedentary behavior and depression: A systematic review and meta-analysis. BMC Public Health 2019, 19, 1524. [Google Scholar] [CrossRef]
- Ding, E.L.; Mekary, R.A. Letter by Ding and Mekary regarding article, “television viewing time and mortality: The Australian diabetes, obesity and lifestyle study (AusDiab)”. Circulation 2010, 122, e472. [Google Scholar] [CrossRef] [Green Version]
- Gibbs, B.B.; Reis, J.P.; Schelbert, E.B.; Craft, L.L.; Sidney, S.; Lima, J.; Lewis, C.E. Sedentary screen time and left ventricular structure and function: The CARDIA study. Med. Sci. Sports Exerc. 2014, 46, 276–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celis-Morales, C.A.; Lyall, D.M.; Steell, L.; Gray, S.R.; Iliodromiti, S.; Anderson, J.; Mackay, D.F.; Welsh, P.; Yates, T.; Pell, J.P.; et al. Associations of discretionary screen time with mortality, cardiovascular disease and cancer are attenuated by strength, fitness and physical activity: Findings from the UK Biobank study. BMC Med. 2018, 16, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruine de Bruin, W. Age differences in COVID-19 risk perceptions and mental health:Evidence from a national US survey conducted in March 2020. J. Gerontol. B Psychol. Sci. Soc. Sci. 2020. [Google Scholar] [CrossRef] [PubMed]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, anxiety and stress during COVID-19: Associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.M.; Lai, J.H.; Huang, T.W. Mediating effects of depression on anxiety and leisure constraints in patients with breast cancer. BMC Womens Health 2019, 19, 141. [Google Scholar] [CrossRef] [PubMed]
- Cho, D.; Post, J.; Kim, S.K. Comparison of passive and active leisure activities and life satisfaction with aging. Geriatr. Gerontol. Int. 2018, 18, 380–386. [Google Scholar] [CrossRef]
- Asmundson, G.J.; Fetzner, M.G.; Deboer, L.B.; Powers, M.B.; Otto, M.W.; Smits, J.A. Let’s get physical: A contemporary review of the anxiolytic effects of exercise for anxiety and its disorders. Depress. Anxiety 2013, 30, 362–373. [Google Scholar] [CrossRef]
- Stubbs, B.; Vancampfort, D.; Rosenbaum, S.; Firth, J.; Cosco, T.; Veronese, N.; Salum, G.A.; Schuch, F.B. An examination of the anxiolytic effects of exercise for people with anxiety and stress-related disorders: A meta-analysis. Psychiatry Res. 2017, 249, 102–108. [Google Scholar] [CrossRef]




| Men | Women | Total | |
|---|---|---|---|
| Percentage n (%) | 5366 (46.5%) | 6474 (53.5%) | 12,107 (100%) |
| Age (years) | |||
| <20 | 464 (8.2%) | 390 (6.0%) | 854 (7.1%) |
| 20–24 | 1832 (32.5%) | 2064 (31.9%) | 3896 (32.2%) |
| 25–29 | 644 (11.4%) | 817 (12.6%) | 1461 (12.1%) |
| 30–34 | 568 (10.1%) | 860 (13.3%) | 1428 (11.8%) |
| 35–39 | 608 (10.8%) | 777 (12.0%) | 1385 (11.4%) |
| 40–44 | 570 (10.1%) | 658 (10.2%) | 1228 (10.1%) |
| 45–49 | 463 (8.2%) | 447 (6.9%) | 910 (7.5%) |
| 50–54 | 243 (4.3%) | 238 (3.7%) | 481 (4.0%) |
| 55–59 | 148 (2.6%) | 132 (2.0%) | 280 (2.3%) |
| ≥60 | 93 (1.7%) | 91 (1.4%) | 184 (1.5%) |
| Urbanity | |||
| Urban regions | 1751 (31.1%) | 1949 (30.1%) | 3700 (30.6%) |
| Rural regions | 3882 (68.9%) | 4525 (69.9%) | 8407 (69.4%) |
| Education | |||
| Primary school or lower | 187 (3.3%) | 161 (2.5%) | 348 (2.9%) |
| Middle school | 272 (4.8%) | 413 (6.4%) | 685 (5.7%) |
| High school | 504 (8.9%) | 700 (10.8%) | 1204 (9.9%) |
| College | 3260 (57.9%) | 3707 (57.2%) | 6963 (57.5%) |
| Graduate | 1410 (25.0%) | 1497 (23.1%) | 2907 (24.0%) |
| Occupation | |||
| Full-time student | 2211 (39.3%) | 2249 (34.7%) | 4460 (36.8%) |
| Labor | 458 (8.1%) | 504 (7.8%) | 962 (7.9%) |
| Professional | 2280 (40.4%) | 2476 (38.2%) | 4756 (39.3%) |
| Unemployed and freelance | 684 (12.1%) | 1245 (19.2%) | 1929 (15.9%) |
| Vigorous | Moderate | Light | p for Difference * | |
|---|---|---|---|---|
| Sex | <0.0001 | |||
| Men | 23.0% (21.9–24.2) | 21.9% (20.8–23.0) | 55.1% (53.8–56.4) | |
| Women | 19.4% (18.4–20.3) | 21.2% (20.2–22.2) | 59.5% (58.2–60.7) | |
| Age | <0.0001 | |||
| <20 | 28.9% (25.8–32.0) | 20.7% (18.0–23.5) | 50.4% (47.0–53.7) | |
| 20–24 | 17.1% (15.9–18.4) | 18.7% (17.5–19.9) | 64.2% (62.7–65.8) | |
| 25–29 | 17.1% (15.0–19.1) | 19.4% (17.4–21.5) | 63.4% (61.0–65.9) | |
| 30–34 | 17.9% (15.8–19.7) | 22.1% (20.0–24.4) | 60.0% (57.6–62.5) | |
| 35–39 | 23.3% (21.1–25.7) | 22.2% (19.9–24.3) | 54.5% (51.8–57.0) | |
| 40–44 | 24.2% (21.7–26.6) | 23.9% (21.3–26.3) | 51.9% (49.2–54.8) | |
| 45–49 | 24.8% (22.1–27.6) | 27.8% (24.9–30.8) | 47.4% (44.2–50.4) | |
| 50–54 | 28.1% (23.9–32.2) | 24.5% (20.6–28.7) | 47.4% (42.8–52.0) | |
| 55–59 | 33.2% (27.9–38.9) | 25.7% (20.7–30.7) | 41.1% (35.4–46.8) | |
| ≥60 | 30.4% (23.9–37.0) | 28.3% (21.7–34.8) | 41.3% (34.2–48.9) | |
| Urbanity | <0.0001 | |||
| Urban | 20.5% (19.6–21.3) | 22.1% (21.2–23.0) | 57.5% (56.4–58.5) | |
| Rural | 22.4% (21.1–23.8) | 20.1% (18.8–21.4) | 57.5% (55.9–59.1) |
| PANAS Positive Affect | PANAS Negative Affect | |
|---|---|---|
| Total | ||
| n = 12107 | 24.78 ± 6.88 | 19.34 ± 7.05 |
| Sex | ||
| Male (n = 5633) | 25.09 ± 7.06 | 19.04 ± 7.00 |
| Female (n = 6474) | 24.51 ± 6.70 | 19.61 ± 7.08 |
| p for difference | <0.0001 | <0.0001 |
| Urbanity | ||
| Urban (n = 8407) | 24.81 ± 6.85 | 19.46 ± 7.13 |
| Rural (n = 3700) | 24.70 ± 6.95 | 19.08 ± 6.86 |
| p for difference | 0.420 | 0.006 |
| Age | ||
| <20 (n = 854) | 26.26 ± 7.61 ab | 17.35 ± 6.68 ab |
| 20–24 (n = 3896) | 24.14 ± 7.17 | 19.69 ± 7.20 |
| 25–29 (n = 1461) | 24.21 ± 6.86 | 20.43 ± 7.20 |
| 30–34 (n = 1428) | 24.41 ± 6.66 | 19.86 ± 7.15 b |
| 35–39 (n = 1385) | 25.21 ± 6.38 ab | 19.93 ± 6.84 |
| 40–44 (n = 1228) | 25.52 ± 6.46 ab | 19.21 ± 6.98 ab |
| 45–49 (n = 910) | 25.05 ± 6.12 ab | 18.45 ± 6.42 ab |
| 50–54 (n = 481) | 25.35 ± 6.56 ab | 17.48 ± 6.15 ab |
| 55–59 (n = 280) | 25.90 ± 6.93 ab | 17.32 ± 6.47 ab |
| ≥60 (n = 184) | 25.97 ± 7.15 ab | 17.18 ± 7.46 ab |
| p for difference | <0.0001 | <0.0001 |
| Physical activity level | ||
| Vigorous (n = 2548) | 27.54 ± 6.44 | 18.41 ± 6.49 |
| Moderate (n = 2602) | 25.53 ± 6.37 * | 18.93 ± 6.51 * |
| Light (n = 6957) | 23.48 ± 6.88 *# | 19.34 ± 7.39 *# |
| p for difference | <0.0001 | <0.0001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qin, F.; Song, Y.; Nassis, G.P.; Zhao, L.; Dong, Y.; Zhao, C.; Feng, Y.; Zhao, J. Physical Activity, Screen Time, and Emotional Well-Being during the 2019 Novel Coronavirus Outbreak in China. Int. J. Environ. Res. Public Health 2020, 17, 5170. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145170
Qin F, Song Y, Nassis GP, Zhao L, Dong Y, Zhao C, Feng Y, Zhao J. Physical Activity, Screen Time, and Emotional Well-Being during the 2019 Novel Coronavirus Outbreak in China. International Journal of Environmental Research and Public Health. 2020; 17(14):5170. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145170
Chicago/Turabian StyleQin, Fei, Yiqing Song, George P Nassis, Lina Zhao, Yanan Dong, Cuicui Zhao, Yiwei Feng, and Jiexiu Zhao. 2020. "Physical Activity, Screen Time, and Emotional Well-Being during the 2019 Novel Coronavirus Outbreak in China" International Journal of Environmental Research and Public Health 17, no. 14: 5170. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145170