Evaluating the Implementation and Effectiveness of the SWITCH–MS: An Ecological, Multi-Component Adolescent Obesity Prevention Intervention


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
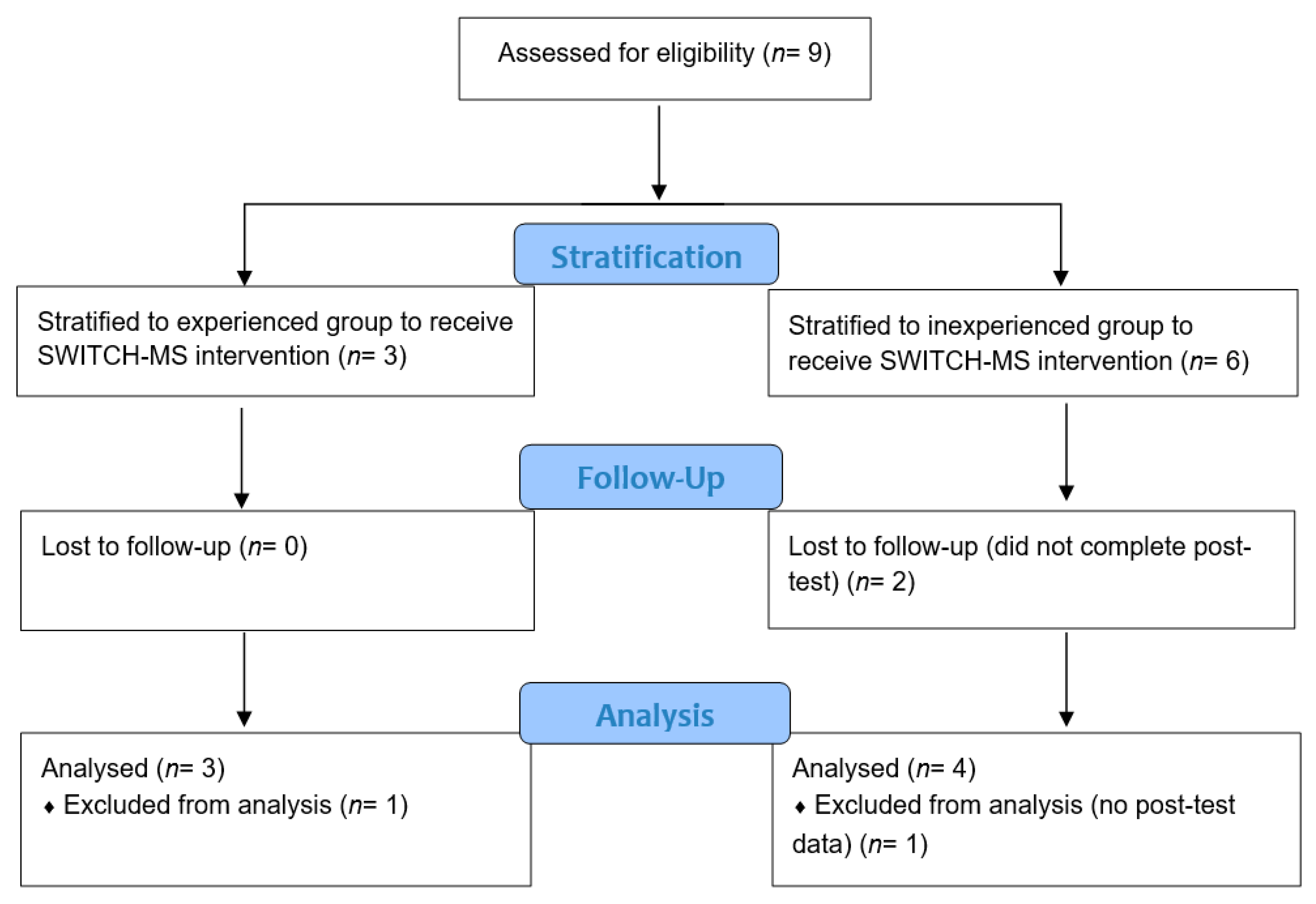
2.1. Design, Settings and Participants
2.2. SWITCH–MS Intervention Process
2.3. Implementation and Effectiveness Outcomes
2.3.1. Whole-of-School Implementation Outcomes
2.3.2. Classroom Implementation Outcomes
2.3.3. Effectiveness Healthy-Living Behavior Outcomes
2.4. Data Collection
2.5. Data Analysis
3. Results
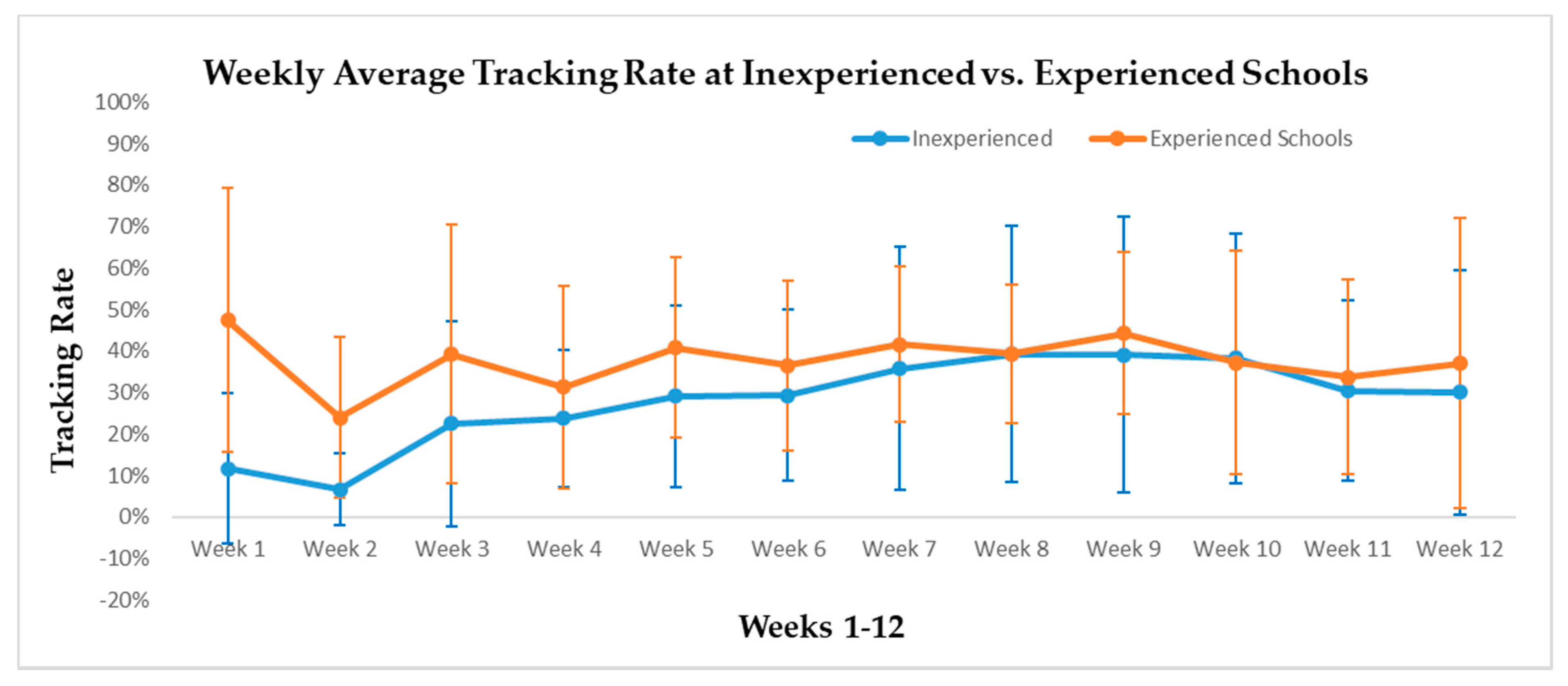
3.1. Implementation Outcomes
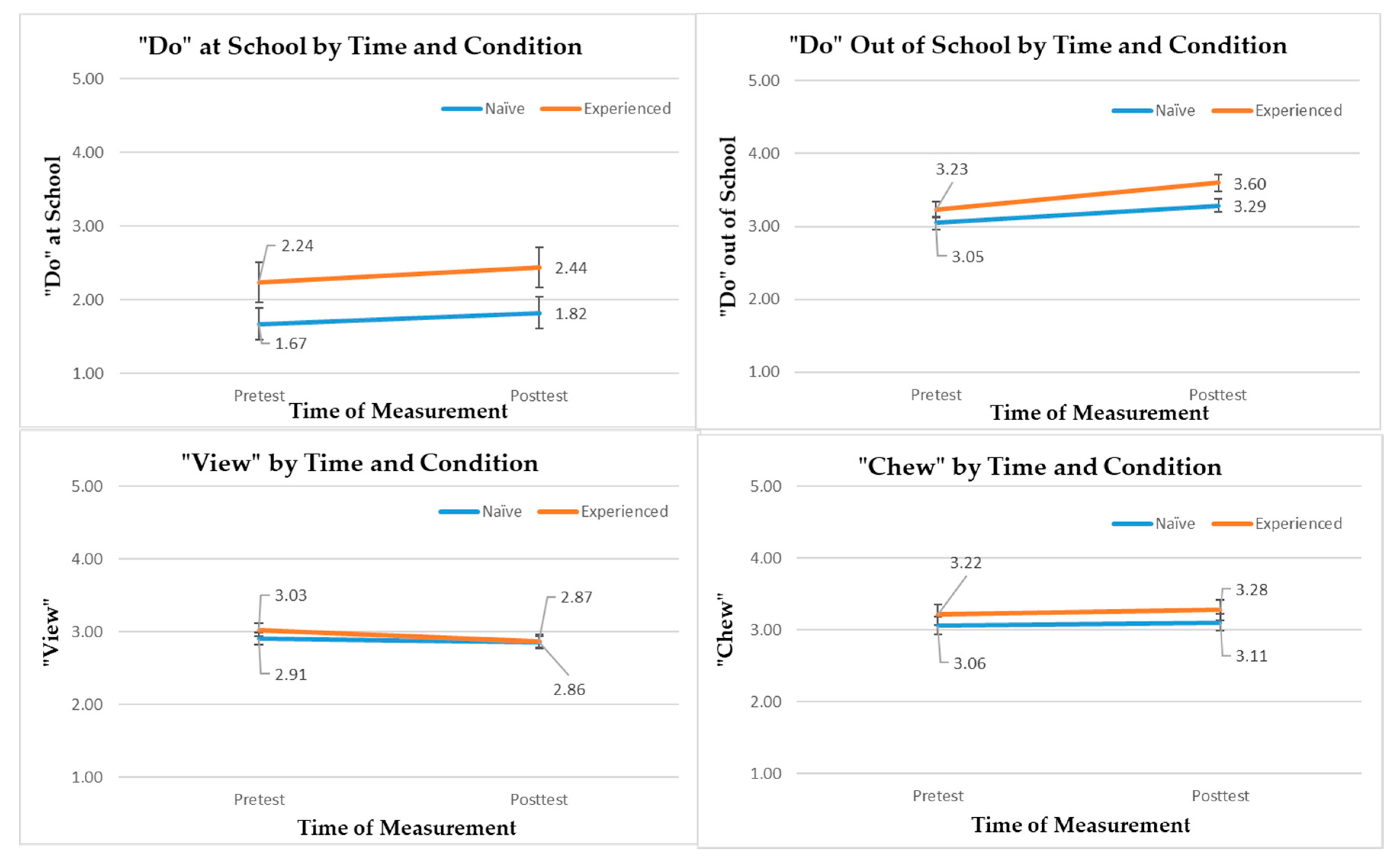
3.2. Effectiveness Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight Key Facts. 2020. Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 19 May 2020).
- Hales, C.M.; Fryar, C.D.; Carroll, M.D.; Freedman, D.S.; Ogden, C.L. Trends in obesity and severe obesity prevalence in US youth and adults by sex and age, 2007–2008 to 2015–2016. JAMA 2018, 319, 1723–1725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogden, C.L.; Fryar, C.D.; Hales, C.M.; Carroll, M.D.; Aoki, Y.; Freedman, D.S. Differences in obesity prevalence by demographics and urbanization in US children and adolescents, 2013–2016. JAMA 2018, 319, 2410–2418. [Google Scholar] [CrossRef]
- Manore, M.M.; Brown, K.; Houtkooper, L.; Jakicic, J.M.; Peters, J.C.; Edge, M.S.; Steiber, A.; Going, S.; Gable, L.G.; Krautheim, A.M. Energy balance at a crossroads: Translating the science into action. Med. Sci. Sport Exerc. 2014, 46, 2466–2473. [Google Scholar] [CrossRef] [PubMed]
- Sobol-Goldberg, S.; Rabinowitz, J.; Gross, R. School-based obesity prevention programs: A meta-analysis of randomized controlled trials. Obesity (Silver Spring) 2013, 21, 2422–2428. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Cai, L.; Wu, Y.; Wilson, R.F.; Weston, C.; Fawole, O.; Bleich, S.N.; Cheskin, L.J.; Showell, N.N.; Lau, B.D.; et al. What childhood obesity prevention programmes work? A systematic review and meta-analysis. Obes. Rev. 2015, 16, 547–565. [Google Scholar] [CrossRef]
- Knowlden, A.P.; Sharma, M. Systematic review of family and home-based interventions targeting paediatric overweight and obesity. Obes. Rev. 2012, 13, 499–508. [Google Scholar] [CrossRef]
- Sevil, J.; García-González, L.; Abós, Á.; Generelo, E.; Aibar, A. Can high schools be an effective setting to promote healthy lifestyles? effects of a multiple behavior change intervention in adolescents. J. Adolesc. Health 2019, 64, 478–486. [Google Scholar] [CrossRef]
- Sevil-Serrano, J.; Aibar, A.; Abós, Á.; Generelo, E.; García-González, L. Improving motivation for physical activity and physical education through a school-based intervention. J. Exp. Educ. 2020, 1–21. [Google Scholar] [CrossRef]
- Gentile, D.A.; Welk, G.; Eisenmann, J.C.; Reimer, R.A.; Walsh, D.A.; Russell, D.W.; Callahan, R.; Walsh, M.; Strickland, S.; Fritz, K. Evaluation of a multiple ecological level child obesity prevention program: Switch what you Do, View, and Chew. BMC Med. 2009, 7, 49. [Google Scholar] [CrossRef] [Green Version]
- Welk, G.J.; Chen, S.; Nam, Y.H.; Weber, T.E. A formative evaluation of the SWITCH(R) obesity prevention program: Print versus online programming. BMC Obes. 2015, 2, 20. [Google Scholar] [CrossRef]
- Chen, S.; Dzewaltowski, D.A.; Rosenkranz, R.R.; Lanningham-Foster, L.; Vazou, S.; Gentile, D.A.; Lee, J.A.; Braun, K.J.; Wolff, M.M.; Welk, G.J. Feasibility study of the SWITCH implementation process for enhancing school wellness. BMC Public Health 2018, 18, 1119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dzewaltowski, D.A.; Estabrooks, P.A.; Johnston, J.A. Healthy youth places promoting nutrition and physical activity. Health Educ. Res. 2002, 17, 541–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dzewaltowski, D.A.; Estabrooks, P.A.; Welk, G.; Hill, J.; Milliken, G.; Karteroliotis, K.; Johnston, J.A. Healthy youth places: A randomized controlled trial to determine the effectiveness of facilitating adult and youth leaders to promote physical activity and fruit and vegetable consumption in middle schools. Health Educ. Behav. 2009, 36, 583–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewallen, T.C.; Hunt, H.; Potts-Datema, W.; Zaza, S.; Giles, W. The Whole School, Whole Community, Whole Child model: A new approach for improving educational attainment and healthy development for students. J. Sch. Health 2015, 85, 729–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rooney, L.E.; Videto, D.M.; Birch, D.A. Using the whole school, whole community, whole child model: Implications for practice. J. Sch. Health 2015, 85, 817–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Educating the Student Body Taking Physical Activity and Physical Education to School; Institute of Medicine: Washington, DC, USA, 2013.
- McLoughlin, G.M.; Rosenkranz, R.R.; Lee, J.A.; Wolff, M.M.; Chen, S.; Dzewaltowski, D.A.; Vazou, S.; Lanningham-Foster, L.; Gentile, D.A.; Rosen, M.S.; et al. The Importance of self-monitoring for behavior change in youth: Findings from the SWITCH® school wellness feasibility study. Int. J. Environ. Res. Public Health 2019, 16, 3806. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Liu, Y.; Welk, G.J. Using a hybrid design to analyze effectiveness and implementation of a refined energy-balance education module for upper elementary physical education. J. Rech. Interv. Educ. Phys. Sport 2019, 3, 108–124. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Zhu, X.; Androzzi, J.; Nam, Y.H. Evaluation of a concept-based physical education unit for energy balance education. J. Sport Health Sci. 2018, 7, 353–362. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.A.; McLoughlin, G.; Dzewaltowski, D.A.; Rosenkranz, R.R.; Lanningham-Foster, L.; Vazou, S.; Chen, S.; Gentile, D.; Liechty, L.; Welk, G.J. Evaluation of the implementation process and outcomes in the school wellness integration targeting child health (SWITCH®). Proj. Eval. Progr. Plan. under review.
- McLoughlin, G.M.; Candal, P.; Vazou, S.; Lee, J.A.; Dzewaltowski, D.A.; Rosenkranz, R.R.; Lanningham-Foster, L.; Gentile, D.A.; Liechty, L.; Chen, S.; et al. Evaluating the implementation of the SWITCH® school wellness intervention through mixed methods. Int. J. Behav. Nutr. Phys. Act. under review.
- Colditz, G.A. The promises and challenges of dissemination and implementation research. In Dissemination and Implementation Research in Health; Brownson, R.C., Colditz, G.A., Proctor, E.K., Eds.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Curran, G.M.; Bauer, M.; Mittman, B.; Pyne, J.M.; Stetler, C. Effectiveness-implementation hybrid designs: Combining elements of clinical effectiveness and implementation research to enhance public health impact. Med. Care 2012, 50, 217–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durlak, J.A.; DuPre, E.P. Implementation matters: A review of research on the influence of implementation on program outcomes and the factors affecting implementation. Am. J. Community Psychol. 2008, 41, 327–350. [Google Scholar] [CrossRef]
- McLoughlin, G.M.; Vazou, S.; Liechty, L.; Torbert, A.; Lanningham-Foster, L.; Rosenkranz, R.R.; Welk, G.J. Transdisciplinary approaches for the dissemination of the SWITCH school wellness initiative through a distributed 4-H/extension network. Child. Youth Care Forum 2020. [Google Scholar] [CrossRef]
- Saint-Maurice, P.F.; Kim, Y.; Hibbing, P.; Oh, A.Y.; Perna, F.M.; Welk, G.J. Calibration and validation of the youth activity profile: The FLASHE study. Am. J. Prev. Med. 2017, 52, 880–887. [Google Scholar] [CrossRef] [PubMed]
- Saint-Maurice, P.F.; Welk, G.J. Validity and calibration of the youth activity profile. PLoS ONE 2015, 10, e0143949. [Google Scholar] [CrossRef] [Green Version]
- Klimesh, K.A. Associations between the Family Nutrition and Physical Activity Screening Tool and the Youth Activity Profile; Department of Kinesiology, Iowa State University: Ames, IA, USA, 2015. [Google Scholar]
- Heck, R.H.; Thomas, S.L.; Tabata, L.N. Multilevel and Longitudinal Modeling with IBM SPSS, 2nd ed.; Routledge: New York, NY, USA, 2013. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| School # | Group | Locale | Enrollment | %White | %Male | %FARM |
|---|---|---|---|---|---|---|
| 1 | Inexperienced | Rural: Distant | 227 | 95% | 54% | 21% |
| 2 | Inexperienced | Rural: Distant | 97 | 99% | 46% | 22% |
| 3 | Inexperienced | City: Mid-size | 737 | 30% | 49% | 74% |
| 4 | Inexperienced | Rural: Distant | 189 | 93% | 49% | 28% |
| 5 * | Experienced | Town: Fringe | 30 | 92% | 45% | --- |
| 6 | Experienced | Rural: Distant | 270 | 89% | 54% | 34% |
| 7 | Experienced | Rural: Remote | 70 | 96% | 54% | 26% |
| Group | Implementation of the Best Practices | Awareness | Engagement | ||
|---|---|---|---|---|---|
| Health | PE | Lunchroom | |||
| Inexperienced (n = 3) | 1.9 ± 0.4 | 1.4 ± 0.2 | 2.2 ± 1.1 | 2.2 ± 0.2 | 1.9 ± 0.3 |
| Experienced (n = 3) | 1.8 ± 0.4 | 1.4 ± 0.5 | 1.7 ± 0.6 | 2.3 ± 0.3 | 2.3 ± 0.3 |
| Behavior Outcome | Predictors | B | s.e. | df | t | p | 95% CI | Variances Explained at Levels 1, 2, 3 | |
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| “Do” at School | Intercept | 2.04 | 0.41 | 4.83 | 4.96 | <0.01 | 0.97 | 3.11 | 33.5%, 45.7%, 20.8% |
| Time (T1) | −0.20 | 0.07 | 375.05 | −2.83 | <0.01 | −0.34 | −0.06 | ||
| Condition (inexp.) | −0.62 | 0.35 | 4.32 | −1.79 | 0.14 | −1.55 | 0.31 | ||
| Time×Condition (T1×inexp.) | 0.05 | 0.08 | 374.93 | 0.55 | 0.59 | −0.12 | 0.21 | ||
| Gender (boys) | 0.23 | 0.08 | 383.42 | 3.09 | <0.01 | 0.08 | 0.38 | ||
| Grade (6th G) | 0.85 | 0.13 | 379.46 | 6.34 | <0.01 | 0.59 | 1.11 | ||
| Grade (7th G) | −0.10 | 0.14 | 394.64 | −0.73 | 0.46 | −0.37 | 0.17 | ||
| Tracking | 0.14 | 0.85 | 4.08 | 0.17 | 0.88 | −2.20 | 2.48 | ||
| “Do” out of School | Intercept | 2.99 | 0.20 | 16.25 | 15.03 | <0.01 | 2.57 | 3.41 | 45.7%, 53.6%, 0.7% |
| Time (T1) | −0.37 | 0.09 | 375.08 | −4.12 | <0.01 | −0.54 | −0.19 | ||
| Condition (inexp.) | −0.31 | 0.14 | 5.43 | −2.29 | 0.07 | −0.65 | 0.03 | ||
| Time×Condition (T1×inexp.) | 0.13 | 0.11 | 374.98 | 1.21 | 0.23 | −0.08 | 0.34 | ||
| Gender (boys) | 0.20 | 0.09 | 384.25 | 2.17 | 0.03 | 0.02 | 0.37 | ||
| Grade (6th G) | 0.60 | 0.15 | 148.25 | 3.98 | <0.01 | 0.30 | 0.89 | ||
| Grade (7th G) | 0.23 | 0.16 | 379.02 | 1.44 | 0.15 | −0.09 | 0.55 | ||
| Tracking | 0.94 | 0.30 | 4.31 | 3.09 | 0.03 | 0.12 | 1.76 | ||
| “View” Behavior | Intercept | 3.14 | 0.16 | 9.89 | 19.48 | <0.01 | 2.78 | 3.50 | 46.5%, 52.4%, 1.1% |
| Time (T1) | 0.16 | 0.07 | 374.98 | 2.25 | 0.03 | 0.02 | 0.30 | ||
| Condition (inexp.) | −0.01 | 0.11 | 3.74 | −0.08 | 0.94 | −0.33 | 0.31 | ||
| Time×Condition (T1×inexp.) | −0.11 | 0.08 | 374.88 | −1.35 | 0.18 | −0.28 | 0.05 | ||
| Gender (boys) | 0.21 | 0.07 | 384.16 | 2.98 | <0.01 | 0.07 | 0.35 | ||
| Grade (6th G) | −0.46 | 0.12 | 139.81 | −3.90 | <0.01 | −0.69 | −0.23 | ||
| Grade (7th G) | −0.22 | 0.13 | 379.96 | −1.73 | 0.08 | −0.47 | 0.03 | ||
| Tracking | −0.60 | 0.25 | 2.96 | −2.35 | 0.10 | −1.42 | 0.22 | ||
| “Chew” Behavior | Intercept | 2.86 | 0.23 | 6.75 | 12.33 | <0.01 | 2.31 | 3.42 | 31.7%, 61.9%, 6.5% |
| Time (T1) | −0.05 | 0.06 | 375.30 | −0.90 | 0.37 | −0.17 | 0.06 | ||
| Condition (inexp.) | −0.16 | 0.18 | 4.61 | −0.90 | 0.41 | −0.65 | 0.32 | ||
| Time×Condition (T1×inexp.) | 0.01 | 0.07 | 375.15 | 0.11 | 0.91 | −0.13 | 0.14 | ||
| Gender (boys) | −0.10 | 0.07 | 390.33 | −1.44 | 0.15 | −0.24 | 0.04 | ||
| Grade (6th G) | 0.64 | 0.12 | 333.44 | 5.17 | <0.01 | 0.40 | 0.89 | ||
| Grade (7th G) | 0.26 | 0.13 | 405.07 | 2.02 | 0.04 | 0.01 | 0.51 | ||
| Tracking | 0.65 | 0.44 | 4.09 | 1.48 | 0.21 | −0.56 | 1.87 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, S.; Rosenkranz, R.R.; McLoughlin, G.M.; Vazou, S.; Lanningham-Foster, L.; Gentile, D.A.; Dzewaltowski, D.A. Evaluating the Implementation and Effectiveness of the SWITCH–MS: An Ecological, Multi-Component Adolescent Obesity Prevention Intervention. Int. J. Environ. Res. Public Health 2020, 17, 5401. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155401
Chen S, Rosenkranz RR, McLoughlin GM, Vazou S, Lanningham-Foster L, Gentile DA, Dzewaltowski DA. Evaluating the Implementation and Effectiveness of the SWITCH–MS: An Ecological, Multi-Component Adolescent Obesity Prevention Intervention. International Journal of Environmental Research and Public Health. 2020; 17(15):5401. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155401
Chicago/Turabian StyleChen, Senlin, Richard R. Rosenkranz, Gabriella M. McLoughlin, Spyridoula Vazou, Lorraine Lanningham-Foster, Douglas A. Gentile, and David A. Dzewaltowski. 2020. "Evaluating the Implementation and Effectiveness of the SWITCH–MS: An Ecological, Multi-Component Adolescent Obesity Prevention Intervention" International Journal of Environmental Research and Public Health 17, no. 15: 5401. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155401