Benefits of Brief Group Cognitive Behavioral Therapy in Reducing Diabetes-Related Distress and HbA1c in Uncontrolled Type 2 Diabetes Mellitus Patients in Thailand

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
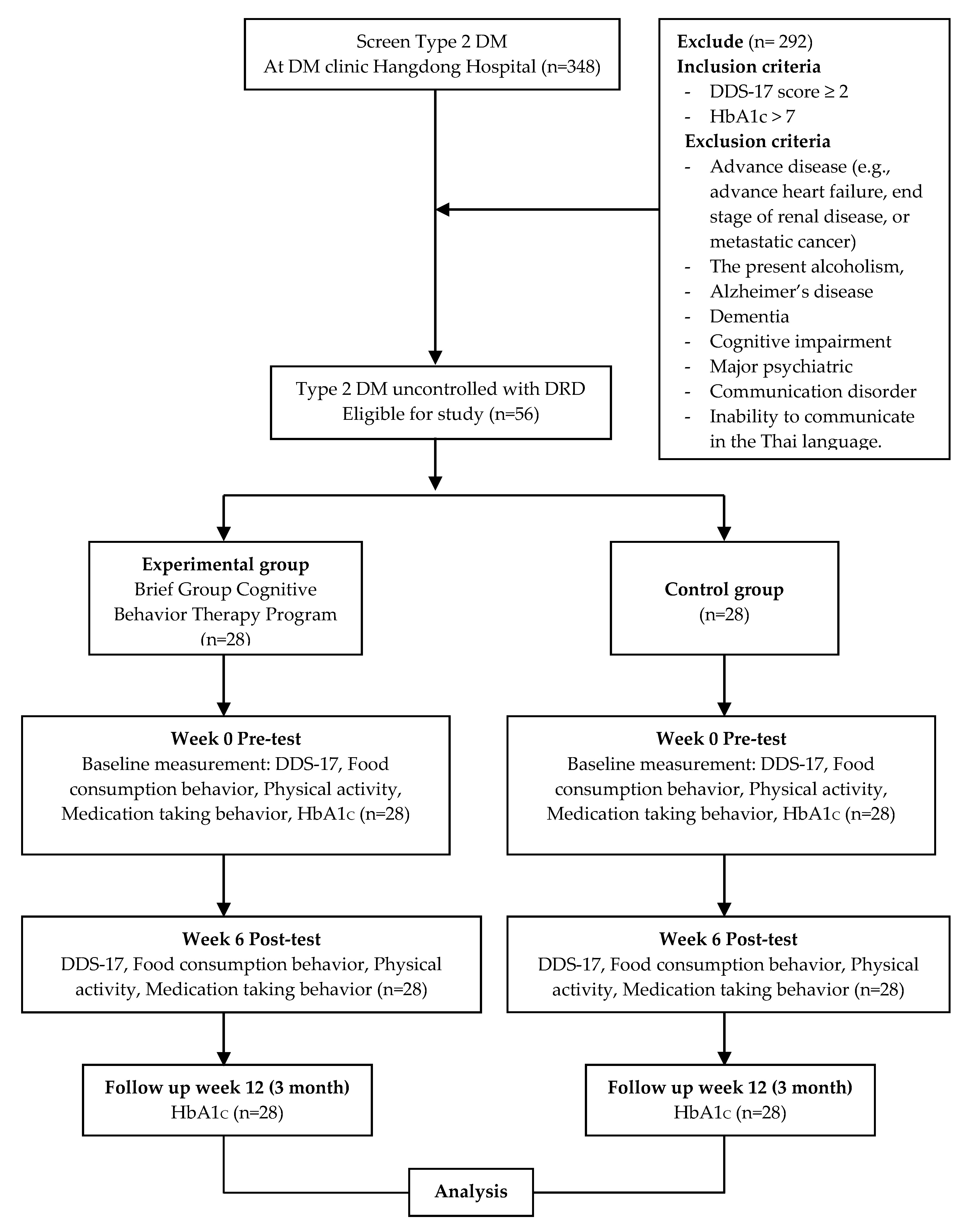
2.1. Study Design
2.2. Participants
2.3. Brief Group Cognitive Behavior Therapy (BG-CBT) Intervention Program
2.4. Outcomes and Measurement
2.4.1. Primary Outcomes
2.4.2. Secondary Outcome
2.5. Ethical Considerations
2.6. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and Regional Diabetes Prevalence Estimates for 2019 and Projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas. Diabetes Res. Clin. Pr. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aekplakorn, W.; Chariyalertsak, S.; Kessomboon, P.; Assanangkornchai, S.; Taneepanichskul, S.; Putwatana, P. Prevalence of Diabetes and Relationship with Socioeconomic Status in the Thai Population: National Health Examination Survey, 2004–2014. J. Diabetes Res. 2018, 2018, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Chew, B.H.; Vos, R.C.; Metzendorf, M.-I.; Scholten, R.J.; Rutten, G.E. Psychological Interventions for Diabetes-Related Distress in Adults with Type 2 Diabetes Mellitus. Cochrane Database Syst. Rev. 2017, 2017. [Google Scholar] [CrossRef]
- Polonsky, W.H.; Anderson, B.J.; A Lohrer, P.; Welch, G.; Jacobson, A.M.; E Aponte, J.; Schwartz, C.E. Assessment of Diabetes-Related Distress. Diabetes Care 1995, 18, 754–760. [Google Scholar] [CrossRef] [PubMed]
- Thanakwang, K.; Thinganjana, W.; Konggumnerd, R. Psychometric Properties of the Thai Version of the Diabetes Distress Scale in Diabetic Seniors. Clin. Interv. Aging 2014, 1353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young-Hyman, D.; De Groot, M.; Hill-Briggs, F.; Gonzalez, J.S.; Hood, K.; Peyrot, M. Psychosocial Care for People With Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2126–2140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, L.; Hessler, D.M.; Polonsky, W.H.; Mullan, J. When Is Diabetes Distress Clinically Meaningful? Diabetes Care 2012, 35, 259–264. [Google Scholar] [CrossRef] [Green Version]
- Aikens, J.E. Prospective Associations Between Emotional Distress and Poor Outcomes in Type 2 Diabetes. Diabetes Care 2012, 35, 2472–2478. [Google Scholar] [CrossRef] [Green Version]
- Fisher, L.; Hessler, D.; Glasgow, R.E.; Arean, P.A.; Masharani, U.; Naranjo, D.; Strycker, L.A. REDEEM: A Pragmatic Trial to Reduce Diabetes Distress. Diabetes Care 2013, 36, 2551–2558. [Google Scholar] [CrossRef] [Green Version]
- Tunsuchart, K.; Lerttrakarnnon, P.; Srithanaviboonchai, K.; Likhitsathian, S.; Skulphan, S. Type 2 Diabetes Mellitus Related Distress in Thailand. Int. J. Environ. Res. Public Health 2020, 17, 2329. [Google Scholar] [CrossRef] [Green Version]
- Fisher, L.; Skaff, M.M.; Mullan, J.T.; Arean, P.; Glasgow, R.; Masharani, U. A Longitudinal Study of Affective and Anxiety Disorders, Depressive Affect and Diabetes Distress in Adults with Type 2 Diabetes. Diabet. Med. 2008, 25, 1096–1101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, C.-P.; Zhang, J.; Li, Y.; Liu, Q.-Z.; Wu, H.-X.; Xu, Z.-J.; Xue, X.-J.; Gao, Q. Comparative Study of the Influence of Diabetes Distress and Depression on Treatment Adherence in Chinese Patients with Type 2 Diabetes: A Cross-Sectional Survey in the People’s Republic of China. Neuropsychiatr. Dis. Treat. 2013, 9, 1289–1294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, W.; Gao, X.; Pang, C.; Hou, X.; Bao, Y.; Liu, W.; Wang, W.; Zuo, Y.; Gu, H.; Xiang, K. Prevalence and Risk Factors of Albuminuria and Chronic Kidney Disease in Chinese Population with Type 2 Diabetes and Impaired Glucose Regulation: Shanghai Diabetic Complications Study (SHDCS). Nephrol. Dial. Transplant. 2009, 24, 3724–3731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ting, R.Z.; Nan, H.; Yu, M.W.; Kong, A.P.; Ma, R.C.; Wong, R.Y.; Loo, K.; So, W.-Y.; Chow, C.-C.; Ko, G.T.; et al. Diabetes-Related Distress and Physical and Psychological Health in Chinese Type 2 Diabetic Patients. Diabetes Care 2011, 34, 1094–1096. [Google Scholar] [CrossRef] [Green Version]
- Fisher, L.; Mullan, J.T.; Skaff, M.M.; Glasgow, R.E.; Arean, P.; Hessler, D. Predicting Diabetes Distress in Patients with Type 2 Diabetes: A Longitudinal Study. Diabet. Med. 2009, 26, 622–627. [Google Scholar] [CrossRef]
- Gonzalez, J.S.; Shreck, E.; Psaros, C.; Safren, S.A. Distress and Type 2 Diabetes-Treatment Adherence: A Mediating Role for Perceived Control. Heal. Psychol. 2015, 34, 505. [Google Scholar] [CrossRef] [Green Version]
- Fisher, L.; Gonzalez, J.S.; Polonsky, W.H. The Confusing Tale of Depression and Distress in Patients with Diabetes: A Call for Greater Clarity and Precision. Diabet. Med. 2014, 31, 764–772. [Google Scholar] [CrossRef]
- Peyrot, M.; Rubin, R.R. Behavioral and Psychosocial Interventions in Diabetes: A Conceptual Review. Diabetes Care 2007, 30, 2433–2440. [Google Scholar] [CrossRef] [Green Version]
- Beck, J.S. Cognitive Behavior Therapy: Basics and Beyond; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Halford, J.; Brown, T. Cognitive–Behavioural Therapy as an Adjunctive Treatment in Chronic Physical Illness. Adv. Psychiatr. Treat. 2009, 15, 306–317. [Google Scholar] [CrossRef] [Green Version]
- Safren, S.A.; Gonzalez, J.S.; Wexler, D.J.; Psaros, C.; Delahanty, L.M.; Blashill, A.J.; Margolina, A.I.; Cagliero, E. A Randomized Controlled Trial of Cognitive Behavioral Therapy for Adherence and Depression (CBT-AD) in Patients with Uncontrolled Type 2 Diabetes. Diabetes Care 2014, 37, 625–633. [Google Scholar] [CrossRef] [Green Version]
- Aguilera, A.; Bruehlman-Senecal, E.; Liu, N.; Bravin, J. Implementing Group CBT for Depression Among Latinos in a Primary Care Clinic. Cogn. Behav. Pr. 2018, 25, 135–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amsberg, S.; Anderbro, T.; Wredling, R.; Lisspers, J.; Lins, P.-E.; Adamson, U.; Johansson, U.-B. A Cognitive Behavior Therapy-Based Intervention among Poorly Controlled Adult Type 1 Diabetes Patients—A Randomized Controlled Trial. Patient Educ. Couns. 2009, 77, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Cummings, D.M.; Lutes, L.D.; Littlewood, K.; Solar, C.; Carraway, M.; Kirian, K.; Patil, S.; Adams, A.; Ciszewski, S.; Edwards, S.; et al. Randomized Trial of a Tailored Cognitive Behavioral Intervention in Type 2 Diabetes With Comorbid Depressive and/or Regimen-Related Distress Symptoms: 12-Month Outcomes From COMRADE. Diabetes Care 2019, 42, 841–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seyed-Reza, A.; Norzarina, M.Z.; Kimura, L. The Benefits of Cognitive Behavioral Therapy (CBT) on Diabetes Distress and Glycemic Control in Type 2 Diabetes. Available online: https://www.mjpsychiatry.org/index.php/mjp/article/view/362/266 (accessed on 31 July 2020).
- Hill, R. What Sample Size is “Enough” in Internet Survey Research. Interpers. Comput. Technol. Electron. J. 21st Century 1998, 6, 1–12. [Google Scholar]
- Polonsky, W.H.; Fisher, L.; Earles, J.; Dudl, R.J.; Lees, J.; Mullan, J.; Jackson, R.A. Assessing Psychosocial Distress in Diabetes: Development of the Diabetes Distress Scale. Diabetes Care 2005, 28, 626–631. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, T.; Bull, F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J. Public Heal. 2006, 14, 66–70. [Google Scholar] [CrossRef]
- Visuthipanich, V. Psychometric Testing of GPAQ among the Thai Population. Thai Pharm. Health Sci. J. 2016, 11, 144–152. [Google Scholar]
- Sakthong, P.; Sonsa-Ardjit, N.; Sukarnjanaset, P.; Munpan, W.; Suksanga, P. Development and Psychometric Testing of the Medication Taking Behavior Tool in Thai Patients. Int. J. Clin. Pharm. 2016, 38, 438–445. [Google Scholar] [CrossRef]
- Rapoport, L.; Clark, M.; Wardle, J. Evaluation of a Modified Cognitive–Behavioural Programme for Weight Management. Int. J. Obes. 2000, 24, 1726–1737. [Google Scholar] [CrossRef] [Green Version]
- Ismail, K.; Winkley, K.; Rabe-Hesketh, S. Systematic Review and Meta-Analysis of Randomised Controlled Trials of Psychological Interventions to Improve Glycaemic Control in Patients with Type 2 Diabetes. Lancet 2004, 363, 1589–1597. [Google Scholar] [CrossRef]
- Van Der Ven, N.C.; Lubach, C.H.; Hogenelst, M.H.; Van Iperen, A.; Tromp-Wever, A.M.; Vriend, A.; Van Der Ploeg, H.M.; Heine, R.J.; Snoek, F.J. Cognitive Behavioural Group Training (CBGT) for Patients with Type 1 Diabetes in Persistent Poor Glycaemic Control: Who do We Reach? Patient Educ. Couns. 2005, 56, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Welschen, L.M.; Van Oppen, P.; Bot, S.D.M.; Kostense, P.J.; Dekker, J.M.; Nijpels, G. Effects of a Cognitive Behavioural Treatment in Patients with Type 2 Diabetes when Added to Managed Care; a Randomised Controlled Trial. J. Behav. Med. 2013, 36, 556–566. [Google Scholar] [CrossRef] [PubMed]
- Yomogida, J.; Inouye, J.; Li, D.; Davis, J. The Effect of a Cognitive–Behavioral Intervention on Diet and Exercise among Asian Americans and Pacific Islanders with Type 2 Diabetes. Asian Pac. Isl. Nurs. J. 2015, 1, 7. [Google Scholar] [CrossRef]
- Ahmad, N.S.; Ramli, A.; Islahudin, F.; Paraidathathu, T. Medication Adherence in Patients with Type 2 Diabetes Mellitus Treated at Primary Health Clinics in Malaysia. Patient Prefer. Adher. 2013, 7, 525. [Google Scholar]
- Polonsky, W.H.; Henry, R.R. Poor Medication Adherence in Type 2 Diabetes: Recognizing the Scope of the Problem and its Key Contributors. Patient Prefer. Adher. 2016, 10, 1299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denison, E.; Underland, V.; Mosdøl, A.; Vist, G.E. Cognitive Therapies for Increasing Physical Activity. Knowledge Centre for the Health Services at the Norwegian Institute of Public Health (NIPH). 2016. Available online: https://fhi.brage.unit.no/fhi-xmlui/bitstream/handle/11250/2436234/Denison_2016_Cog.pdf?sequence=1 (accessed on 30 July 2020).
- Bond, F.W.; Dryden, W. Handbook of Brief Cognitive Behaviour Therapy; Wiley: Hoboken, NJ, USA, 2002. [Google Scholar]
- Whitfield, G. Group Cognitive–Behavioural Therapy for Anxiety and Depression. Adv. Psychiatr. Treat. 2010, 16, 219–227. [Google Scholar] [CrossRef]
- Guo, M.; Mi, J.; Jiang, Q.-M.; Xu, J.-M.; Tang, Y.-Y.; Tian, G.; Wang, B. Metformin may Produce Antidepressant Effects through Improvement of Cognitive Function among Depressed Patients with Diabetes Mellitus. Clin. Exp. Pharmacol. Physiol. 2014, 41, 650–656. [Google Scholar] [CrossRef]
- Zemdegs, J.; Martin, H.; Pintana, H.; Bullich, S.; Manta, S.; Marqués, M.A.; Moro, C.; Layé, S.; Ducrocq, F.; Chattipakorn, N.; et al. Metformin Promotes Anxiolytic and Antidepressant-Like Responses in Insulin-Resistant Mice by Decreasing Circulating Branched-Chain Amino Acids. J. Neurosci. 2019, 39, 5935–5948. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Parameter | Experimental Group (n = 28) | Control Group (n = 28) | Total (n = 56) | p-Value |
|---|---|---|---|---|
| Age (years) mean ± SD | 58.18 ± 8.83 | 53.89 ± 7.34 | 56.04 ± 8.33 | 0.093 |
| Gender (% female) | 57.10% | 60.70% | 58.90% | 0.813 |
| DM complications (% present) | 32.10% | 60.70% | 46.40% | 0.326 |
| Comorbidities (% present) | 85.70% | 60.70% | 73.20% | 0.713 |
| Duration of diabetes (years) mean ± SD | 10.34 ± 7.77 | 7.39 ± 5.40 | 8.87 ± 6.79 | 0.077 |
| HbA1c% mean ± SD | 9.44 ± 1.63 | 9.68 ± 2.09 | 9.56 ± 1.86 | 0.575 |
| DDS-17 scores mean ± SD | 2.46 ± 0.41 | 2.46 ± 0.47 | 2.46 ± 0.44 | 0.915 |
| Physical activity mean ± SD | 69.90 ± 57.43 | 83.56 ± 92.92 | 76.73 ± 76.85 | 0.511 |
| Food consumption behavior score mean ± SD | 45.14 ± 7.37 | 52.86 ± 6.81 | 49.00 ± 8.04 | 0.000 |
| medication taking behavior score mean ± SD | 21.50 ± 2.03 | 22.00 ± 1.94 | 21.75 ± 1.98 | 0.350 |
| Parameter | Experimental Group (n = 28), Mean (± SD) | p-Value | Control Group (n = 28), Mean (± SD) | p-Value | ||
|---|---|---|---|---|---|---|
| Baseline | Post Intervention | Baseline | Post Intervention | |||
| DDS score | 2.47 ± 0.41 | 2.08 ± 0.49 | <0.001 | 2.46 ± 0.47 | 2.48 ± 0.80 | 0.817 |
| Food consumption behaviors score | 45.14 ± 7.37 | 50.21 ± 7.03 | <0.001 | 52.86 ± 6.81 | 52.50 ± 5.07 | 0.777 |
| Physical activity | 69.90 ± 57.43 | 76.89 ± 61.39 | 0.176 | 83.56 ± 92.92 | 92.43 ± 109.88 | 0.372 |
| Medication taking behaviors score | 21.50 ± 2.03 | 21.89 ± 1.97 | 0.110 | 22.00 ± 1.94 | 21.46 ± 2.91 | 0.216 |
| HbA1c% | 9.44 ± 1.63 | 7.34 ± 1.10 | <0.001 | 9.68 ± 2.09 | 8.97 ± 2.38 | 0.101 |
| Parameter | Experimental Group (n = 28) Mean (± SD) | Control Group (n = 28) Mean (± SD) | p-Value Change | ||||
|---|---|---|---|---|---|---|---|
| Baseline | Follow-up | Mean Change | Baseline | Follow-up | Mean Change | ||
| DDS score | 2.47 ± 0.41 | 2.08 ± 0.49 | −0.39 ± 0.47 | 2.46 ± 0.47 | 2.48 ± 0.80 | +0.02 ± 0.62 | 0.006 |
| Food consumption behaviors score | 45.14 ± 7.37 | 50.21 ± 7.03 | +5.07 ± 6.57 | 52.86 ± 6.81 | 52.50 ± 5.07 | −0.36 ± 6.60 | 0.003 |
| Physical Activity | 69.90 ± 57.43 | 76.89 ± 61.39 | +6.99 ± 26.64 | 83.56 ± 92.92 | 92.43 ± 109.88 | +8.87 ± 51.67 | 0.865 |
| Medication taking behaviors score | 21.50 ± 2.03 | 21.89 ± 1.97 | +0.39 ± 1.26 | 22.00 ± 1.94 | 21.46 ± 2.91 | −0.54 ± 2.24 | 0.062 |
| HbA1c% | 9.44 ± 1.63 | 7.34 ± 1.10 | −2.10 ± 1.53 | 9.68 ± 2.09 | 8.97 ± 2.38 | −0.71 ± 2.21 | 0.009 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tunsuchart, K.; Lerttrakarnnon, P.; Srithanaviboonchai, K.; Likhitsathian, S.; Skulphan, S. Benefits of Brief Group Cognitive Behavioral Therapy in Reducing Diabetes-Related Distress and HbA1c in Uncontrolled Type 2 Diabetes Mellitus Patients in Thailand. Int. J. Environ. Res. Public Health 2020, 17, 5564. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155564
Tunsuchart K, Lerttrakarnnon P, Srithanaviboonchai K, Likhitsathian S, Skulphan S. Benefits of Brief Group Cognitive Behavioral Therapy in Reducing Diabetes-Related Distress and HbA1c in Uncontrolled Type 2 Diabetes Mellitus Patients in Thailand. International Journal of Environmental Research and Public Health. 2020; 17(15):5564. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155564
Chicago/Turabian StyleTunsuchart, Kongprai, Peerasak Lerttrakarnnon, Kriengkrai Srithanaviboonchai, Surinporn Likhitsathian, and Sombat Skulphan. 2020. "Benefits of Brief Group Cognitive Behavioral Therapy in Reducing Diabetes-Related Distress and HbA1c in Uncontrolled Type 2 Diabetes Mellitus Patients in Thailand" International Journal of Environmental Research and Public Health 17, no. 15: 5564. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155564