Emotional Intelligence and Mental Health in the Family: The Influence of Emotional Intelligence Perceived by Parents and Children

 , , and
, , and
Abstract
:1. Introduction
Emotional Intelligence in the Family and Mental Health
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Statistical Analysis
3. Results
Multivariate Analysis
4. Discussion
4.1. Hypothesis 1
4.2. Hypothesis 2
4.3. Hypothesis 3
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mayer, J.D.; Salovey, P. What is emotional intelligence? In Emotional Development and Emotional Intelligence: Implications for Educators; Salovey, P., Sluyter, D., Eds.; Basic Books: New York, NY, USA, 1997; pp. 3–31. [Google Scholar]
- Salovey, P.; Mayer, J.D.; Goldman, S.L.; Turvey, C.; Palfai, T.P. Emotional attention, clarity, and repair: Exploring Emotional Intelligence using Trait Meta-Mood Scale. In Emotion, Disclosure and Health; Pennebaker, J.W., Ed.; APA: Washington, DC, USA, 1995; pp. 125–154. [Google Scholar]
- Mayer, J.D.; Salovey, P.; Caruso, D.R.; Sitarenios, G. Measuring emotional intelligence with the MSCEIT V2.0. Emotion 2003, 3, 97–105. [Google Scholar] [PubMed] [Green Version]
- Mayer, J.D.; Caruso, D.R.; Salovey, P. The ability model of emotional intelligence: Principles and updates. Emot. Rev. 2016, 8, 290–300. [Google Scholar]
- Domínguez-García, E.; Fernández-Berrocal, P. The Association Between Emotional Intelligence and Suicidal Behavior: A Systematic Review. Front. Psychol. 2018, 9, 2380. [Google Scholar] [PubMed] [Green Version]
- Fernández-Berrocal, P.; Extremera, N. A review of trait meta-mood research. In Advances in Psychology Research; Columbus, A.M., Ed.; Nova Publishers: New York, NY, USA, 2008; Volume 55, pp. 17–55. [Google Scholar]
- Lischetzke1, T.; Eid, M.; Diener, E. Perceiving One’s Own and Others’ Feelings around the World: The Relations of Attention to and Clarity of Feelings with Subjective Well-Being Across Nations. J. Cross. Cult. Psychol. 2012, 43, 1249–1267. [Google Scholar]
- Sánchez-Alvarez, N.; Extremera, N.; Fernández-Berrocal, P. The relation between emotional intelligence and subjective well-being: A meta-analytic investigation. J. Posit. Psychol. 2016, 11, 276–285. [Google Scholar]
- Salovey, P.; Stroud, L.R.; Woolery, A.; Epel, E.S. Perceived emotional intelligence, stress reactivity, and symptom reports: Further explorations using the Trait Meta-Mood Scale. Psychol. Health 2002, 17, 611–627. [Google Scholar]
- Fernández-Berrocal, P.; Extremera, N.; Ramos, N. Validity and reliability of the Spanish modified version of the Trait Meta-Mood Scale. Psychol. Rep. 2004, 94, 751–755. [Google Scholar]
- Salovey, P.; Bedell, B.; Detweiler, J.B.; Mayer, J.D. Coping intelligently: Emotional intelligence and the coping process. In Coping: The Psychology of what Works; Snyder, C.R., Ed.; Oxford University Press: New York, NY, USA, 1999; pp. 141–164. [Google Scholar]
- Extremera, N.; Fernández-Berrocal, P. Emotional Intelligence as Predictor of Mental, Social and Physical Health in University Students. Span. J. Psychol. 2006, 9, 45–51. [Google Scholar]
- Fernández-Berrocal, P.; Alcaide, R.; Extremera, N.; Pizarro, D. The role of emotional intelligence in anxiety and depression among adolescents. Individ. Differ. Res. 2006, 4, 16–27. [Google Scholar]
- Fernández-Berrocal, P.; Salovey, P.; Vera, A.; Extremera, N.; Ramos, N. Cultural influences on the relation between perceived emotional intelligence and depression. Revue Internationale Psychologie Sociale 2005, 18, 91–107. [Google Scholar]
- Thayer, J.F.; Rossy, L.A.; Ruiz-Padial, E.; Johnsen, B.H. Gender differences in the relationship between emotional regulation and depressive symptoms. Cognit. Ther. Res. 2003, 27, 349–364. [Google Scholar] [CrossRef]
- Salovey, P. Applied emotional intelligence: Regulating emotions to become healthy, wealthy, and wise. In Emotional Intelligence in Every Life; Ciarrochi, J., Forgas, J., Mayer, J.D., Eds.; Psychology Press: Philadelphia, PA, USA, 2001; pp. 123–135. [Google Scholar]
- Martins, A.; Ramalho, N.; Morin, E. A comprehensive meta-analysis of the relationship between emotional intelligence and health. Pers. Individ. Dif. 2010, 49, 554–564. [Google Scholar] [CrossRef]
- Schutte, N.S.; Malouff, J.M.; Thorsteinsson, E.B.; Bhullar, N.; Rooke, S.E. A meta-analytic investigation of the relationship between emotional intelligence and health. Pers. Individ. Dif. 2007, 42, 921–933. [Google Scholar] [CrossRef]
- Fernández-Berrocal, P.; Extremera, N. Ability emotional intelligence, depression, and well-being. Emot. Rev. 2016, 8, 311–315. [Google Scholar] [CrossRef]
- Ciarrochi, J.V.; Deane, F.P.; Anderson, F. Emotional intelligence moderates the relationship between stress and mental health. Pers. Individ. Dif. 2002, 32, 197–209. [Google Scholar] [CrossRef]
- Salguero, J.M.; Palomera, R.; Fernández-Berrocal, P. Perceived emotional intelligence as predictor of psychological adjustment in adolescents: A 1-year prospective study. Eur. J. Psychol. Educ. 2012, 27, 21–34. [Google Scholar] [CrossRef]
- Mihalca, A.M.; Tarnavska, Y. Cognitive Emotion Regulation Strategies and Social Functioning in Adolescents. Procedia Soc. Behav. Sci. 2013, 82, 574–579. [Google Scholar] [CrossRef] [Green Version]
- Ortuño-Sierra, J.; Aritio-Solana, R.; Fonseca-Pedrero, E. Mental health difficulties in children and adolescents: The study of the SDQ in the Spanish National Health Survey 2011–2012. Psychiatry Res. 2018, 259, 236–242. [Google Scholar] [CrossRef]
- Shabani, J.; Hassan, S.A.; Ahmad, A.; Baba, M. Exploring the relationship of emotional intelligence with mental health among early adolescents. Int. J. Psychol. Stud. 2010, 2, 209. [Google Scholar] [CrossRef] [Green Version]
- Shabani, J.; Damavandi, A.J. The importance of gender as a moderator for the relationship between emotional intelligence and mental health of adolescents. Asian Soc. Sci. 2011, 7, 142. [Google Scholar] [CrossRef] [Green Version]
- Ruckmani, V.S.; Balachandra, A. A Study on Emotional Intelligence, Family Environment, Mental Health Problems & Pro-Social Behavior. J. Psychosoc. Res. 2015, 10, 2. [Google Scholar]
- Zeidner, M.; Matthews, G.; Roberts, R.D.; MacCann, C. Development of Emotional Intelligence: Towards a multi-level investment model. Hum. Dev. 2003, 46, 69–96. [Google Scholar] [CrossRef]
- Vernon, P.A.; Petrides, K.V.; Bratko, D.; Schermer, J.A. A behavioral genetic study of trait emotional intelligence. Emotion 2008, 8, 635–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markus, H.R.; Kitayama, S. Cultures and selves: A cycle of mutual constitution. Pers. Psychol. Sci. 2010, 5, 420–430. [Google Scholar] [CrossRef]
- Halberstadt, A.G.; Lozada, F.T. Emotion development in infancy through the lens of culture. Emot. Rev. 2011, 3, 158–168. [Google Scholar] [CrossRef]
- Sung, H.Y. The influence of culture on parenting practices of east Asian families and emotional intelligence of older adolescents: A qualitative study. Sch. Psych. Int. 2010, 31, 199–214. [Google Scholar] [CrossRef]
- Field, J.; Kolbert, J. Enhancing Emotional Intelligence in Parents: The Professional School Counselor’s Role. In Emotionally Intelligent School Counselling; Pellitteri, J., Stern, R., Shelton, C., Muller-Ackerman, B., Eds.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2006. [Google Scholar]
- Marsland, K.W.; Likavec, S.C. Maternal emotional intelligence, infant attachment and child socio-emotional competence. In Proceedings of the 15th Annual Meeting of the American Psychological Society, Atlanta, GA, USA, 29 May–1 June 2003. [Google Scholar]
- Alavi, M.; Mehrinezhad, S.A.; Amini, M.; Singh, M.K.P. Family functioning and trait emotional intelligence among youth. Health Psych. Open. 2017, 4, 1–5. [Google Scholar] [CrossRef]
- Sánchez-Núñez, M.T.; Fernández-Berrocal, P.; Latorre, J.M. Assessment of emotional intelligence in the family: Influences between parents and children on their own perception and that of others. Fam. J. 2013, 21, 65–73. [Google Scholar] [CrossRef]
- Guastello, D.D.; Guastello, S.J. Androgyny, gender role behavior, and emotional intelligence among college students and their parents. Sex Roles 2003, 49, 663–673. [Google Scholar] [CrossRef]
- Alegre, A.; Benson, M.J. Parental behaviors and adolescent adjustment: Mediation via adolescent trait emotional intelligence. Individ. Differ. Res. 2010, 8, 83–96. [Google Scholar]
- Matthews, G.; Zeidner, M.; Roberts, R.D. Emotional Intelligence. Science & Myth; MIT Press: Cambridge, MA, USA, 2002. [Google Scholar]
- Salovey, P.; Bedell, B.; Detweiler, J.B.; Mayer, J.D. Current directions in emotional intelligence research. In Handbook of Emotions, 2nd ed.; Lewis, M., Haviland-Jones, J.M., Eds.; Guilford Press: New York, NY, USA, 2000. [Google Scholar]
- Cumberland-Li, A.; Eisenberg, N.; Champion, C.; Gershoff, E.; Fabes, R.A. The relation of parental emotionality and related dispositional traits to parental expression of emotion and children’s social functioning. Motiv. Emot. 2003, 27, 27–56. [Google Scholar] [CrossRef]
- Howe, D. Child Abuse and Neglect: Attachment, Development and Intervention; Red Globe Press: London, UK, 2005. [Google Scholar]
- Zhou, Q.; Eisenberg, N.; Losoya, S.H.; Fabes, R.A.; Reiser, M.; Guthrie, I.K.; Murphy, B.C.; Cumberland, A.J.; Shepard, S.A. The relations of parental warmth and positive expressiveness to children’s empathy-related responding and social functioning: A longitudinal study. Child Dev. 2002, 73, 893–915. [Google Scholar] [CrossRef] [PubMed]
- Valiente, C.; Eisenberg, N. Parenting and children’s adjustment: The role of children’s emotion regulation. In Emotion Regulation in Couples and Families: Pathways to Dysfunction and Health; Snyder, D.K., Simpson, J., Hughes, J.N., Eds.; American Psychological Association: Washington, DC, USA, 2006; pp. 123–142. [Google Scholar]
- Valiente, C.; Eisenberg, N.; Spinrad, T.L.; Reiser, M.; Cumberland, A.; Losoya, S.H.; Liew, J. Relations among mothers’ expressivity, children’s effortful control, and their problem behaviors: A four-year longitudinal study. Emotion 2006, 6, 459–472. [Google Scholar] [CrossRef] [Green Version]
- Furnham, A.; Rakow, T.; Mak, T. The determinants of parents’ beliefs about the intelligence of their children: A study from Hong Kong. Int. J. Psychol. 2002, 37, 343–352. [Google Scholar] [CrossRef]
- Kirkcaldy, B.; Noack, P.; Furnham, A.; Siefen, G. Parental Estimates of their own and their children’s intelligence. Eur. Psychol. 2007, 12, 173–180. [Google Scholar] [CrossRef]
- Furnham, A.; Bunclark, K. Sex differences in parents’ estimations of their own and their children’s intelligence. Intelligence 2006, 34, 1–14. [Google Scholar] [CrossRef]
- Cole, D.A.; Rehm, L.P. Family interaction patterns and childhood depression. J. Abnorm. Child Psychol. 1986, 14, 297–314. [Google Scholar] [CrossRef]
- Overall, N.C.; Hammond, M.D. Biased and accurate: Depressive symptoms and daily perceptions within intimate relationships. Pers. Soc. Psychol. Bull. 2013, 39, 636–650. [Google Scholar] [CrossRef]
- Piaget, J. The Construction of Reality in the Child; Ballantine: New York, NY, USA, 1954. [Google Scholar]
- Ohannessian, C.; Lerner, R.M.; Von Eye, A.; Lerner, J.V. Direct and indirect relations between perceived parental acceptance, perceptions of the self, and emotional adjustment during early adolescence. Fam. Consum. Sci. Res. J. 1996, 25, 159–183. [Google Scholar] [CrossRef]
- Schwartz, J.P.; Thigpen, S.E.; Montgomery, J.K. Examination of parenting styles of processing emotions and differentiation of self. Fam. J. 2006, 14, 41–48. [Google Scholar] [CrossRef]
- McCarthy, C.J.; Brack, G.; Brack, C.J. Relationship of cognitive appraisals and attachment to emotional events within the family of origin. Fam. J. 1996, 4, 316–326. [Google Scholar] [CrossRef]
- Tinajero, C.; Cadaveira, F.; Rodríguez, M.; Páramo, M. Perceived social support from significant others among binge drinking and polyconsuming Spanish university students. Int. J. Environ. Res. Public Health 2019, 16, 4506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chodorow, N. Mothering, object-relations, and the female oedipal configuration. Fem. Stud. 1978, 4, 137–158. [Google Scholar] [CrossRef]
- Gilligan, C.; Attanucci, J. Two moral orientations: Gender differences and similarities. Merrill Palmer Q. 1988, 34, 223–237. [Google Scholar]
- Erdmans, M. The Grasinski Girls: The Choices They Had and the Choices They Made; Ohio University Press: Athens, OH, USA, 2002. [Google Scholar]
- Rossi, A.S.; Rossi, P.H. Of Human Bonding: Parent-Child Relations Across the Life Course; Aldine de Gruyter: New York, NY, USA, 1990. [Google Scholar]
- Navarro-Bravo, B.; Latorre, J.M.; Jiménez, A.; Cabello, R.; Fernández-Berrocal, P. Ability emotional intelligence in young people and older adults with and without depressive symptoms, considering gender and educational level. PeerJ 2019, 7, e6595. [Google Scholar] [CrossRef]
- Sánchez-Núñez, M.T.; Fernández-Berrocal, P.; Montañés, J.; Latorre, J.M. Does emotional intelligence depend on gender? The socialization of emotional competencies in men and women and its implications. Rev. Electron. Investig. Psicoeduc. Psicoped. 2008, 6, 455–474. [Google Scholar]
- Sánchez-Núñez, M.T.; Medina, C.R.; Rubio, N.G. Gender differences in perceptive emotional adjustment of parents on their children’s emotional intelligence. Psychology 2018, 9, 124–143. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short form health survey (SF-36). Med. Care 1992, 20, 473–483. [Google Scholar] [CrossRef]
- Alonso, J.; Prieto, L.; Antó, J.M. La versión española del SF-36 Health Survey (Cuestionario de Salud SF-36): Un instrumento para la medida de los resultados clínicos. Med. Clin. 1995, 104, 771–776. [Google Scholar]
- Vilagut, G.; Ferrer, M.; Rajmil, L.; Rebollo, P.; Permanyer-Miralda, G.; Quintana, J.M.; Santed, R.; Valderas, J.M.; Ribera, A.; Salvany, A.D.; et al. El cuestionario de salud SF-36 español: Una década de experiencia y nuevos desarrollos. Gac. Sanit. 2005, 19, 135–150. [Google Scholar] [CrossRef] [Green Version]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis. A Regression-Based Approach, 2nd ed.; The Guildford Press: New York, NY, USA, 2018. [Google Scholar]
- Faltýnková, A.; Blinka, L.; Ševčíková, A.; Husarova, D. The Associations between Family-Related Factors and Excessive Internet Use in Adolescents. Int. J. Environ. Res. Public. Health. 2020, 17, 1754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenthal, R. Expectancy effects. In Encyclopedia of Psychology; Kazdin, A.E., Ed.; American Psychological Association: Washington, DC, USA, 2000; pp. 294–296. [Google Scholar]



{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. MH5 C | --- | |||||||||||||||
| 2. Attention C | −0.21 ** | --- | ||||||||||||||
| 3. Clarity C | 0.14 | 0.19 * | --- | |||||||||||||
| 4. Repair C | 0.33 ** | 0.06 | 0.24 ** | --- | ||||||||||||
| 5. Attention F/C | −0.07 | 0.34 ** | 0.23 ** | −0.06 | --- | |||||||||||
| 6. Attention M/C | −0.17 * | 0.29 ** | 0.13 | −0.05 | 0.37 ** | --- | ||||||||||
| 7. Clarity F/C | −0.01 | 0.12 | 0.16 * | −0.06 | 0.48 ** | 0.21 ** | --- | |||||||||
| 8. Clarity M/C | −0.00 | 0.19 * | 0.23 ** | 0.10 | 0.27 ** | 0.51 ** | 0.38 ** | --- | ||||||||
| 9. Repair F/C | 0.13 | 0.15 * | 0.06 | −0.06 | 0.32 ** | 0.16 * | 0.60 ** | 0.28 ** | --- | |||||||
| 10. Repair M/C | 0.07 | 0.07 | 0.07 | 0.16 * | 0.08 | 0.31 ** | 0.12 | 0.49 ** | 0.28 ** | --- | ||||||
| 11. Attention C/F | 0.08 | 0.35 ** | 0.33 ** | 0.17 * | 0.24 ** | 0.11 | 0.12 | 0.15 | 0.15 * | −0.01 | --- | |||||
| 12. Attention C/M | −0.04 | 0.42 ** | 0.20 ** | 0.16 * | 0.24 ** | 0.23 ** | 0.18 * | 0.17 * | 0.11 | 0.08 | 0.09 | --- | ||||
| 13. Clarity C/F | 0.23 ** | 0.16 * | 0.38 ** | 0.20 ** | 0.05 | −0.04 | 0.08 | 0.20 ** | 0.16 * | 0.13 | 0.28 ** | 0.15 * | --- | |||
| 14. Clarity C/M | −0.03 | 0.33 ** | 0.46 ** | 0.09 | 0.21 ** | 0.21 ** | 0.13 | 0.27 ** | 0.17 * | 0.15 | 0.29 ** | 0.27 ** | 0.51 ** | --- | ||
| 15. Repair C/F | 0.34 ** | 0.14 | 0.17 * | 0.27 ** | −0.10 | −0.09 | 0.07 | 0.11 | 0.20 ** | 0.18 * | 0.19 * | 0.17 * | 0.60 ** | 0.23 ** | --- | |
| 16. Repair C/M | 0.10 | 0.18 * | 0.14 | 0.35 ** | −0.08 | 0.05 | −0.09 | 0.03 | −0.18 * | 0.18 * | 0.17 * | 0.07 | 0.17 * | 0.36 ** | 0.25 ** | --- |
| Mean | 4.22 | 3.43 | 3.28 | 3.27 | 3.44 | 3.40 | 3.37 | 3.36 | 3.43 | 3.28 | 2.87 | 3.45 | 3.28 | 3.56 | 3.12 | 3.20 |
| S.D. | 0.90 | 0.80 | 0.74 | 0.77 | 0.81 | 0.83 | 0.82 | 0.78 | 0.81 | 0.73 | 0.79 | 0.79 | 0.79 | 0.72 | 0.92 | 0.84 |
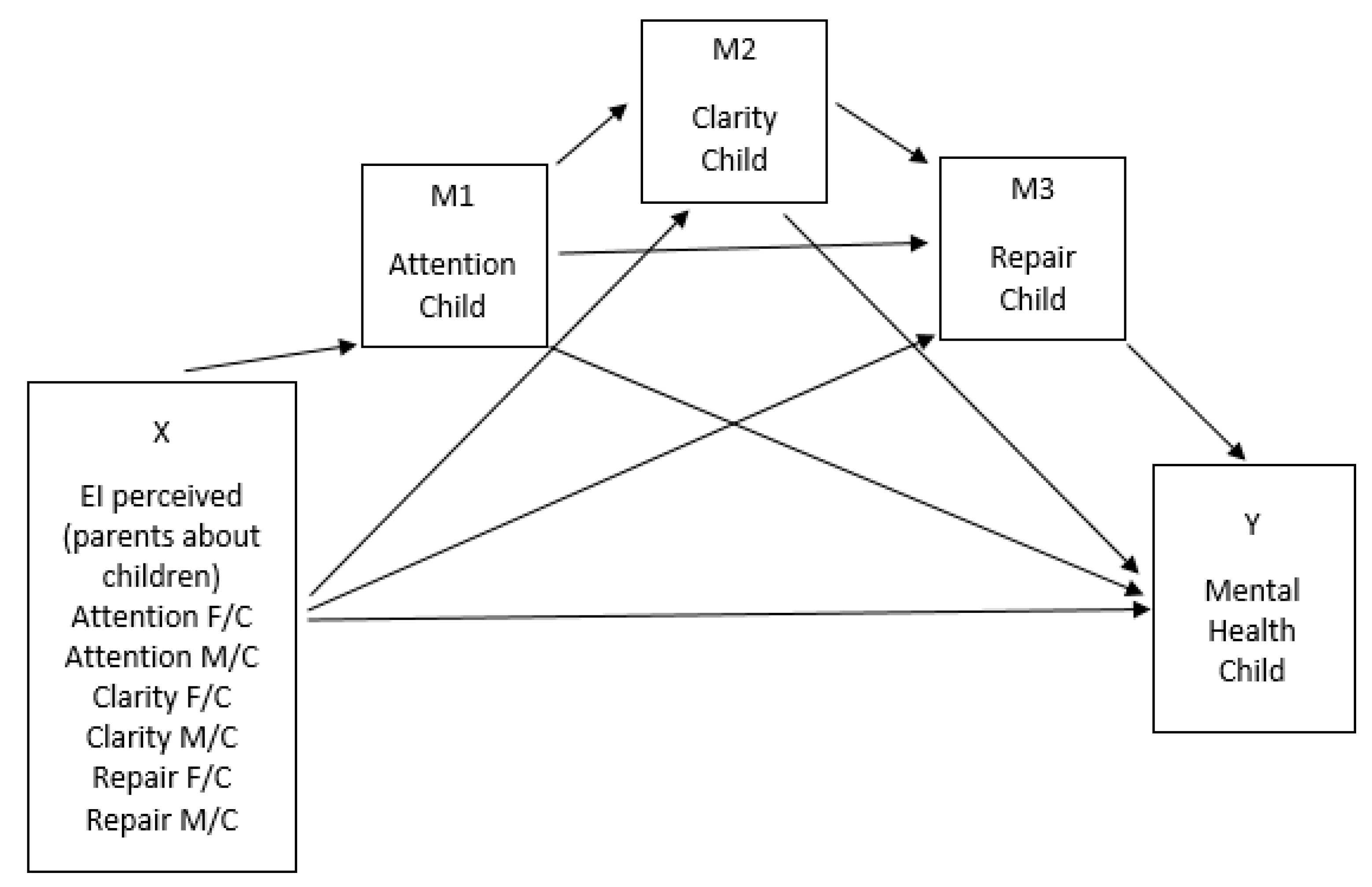
| Consequent | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M1 (Attention Child) | M2 (Clarity Child) | M3 (Repair Child) | Y (MH5) | |||||||||
| Antecedent | Coeff. | SE | p | Coeff. | SE | p | Coeff. | SE | p | Coeff. | SE | p |
| Constant | 1.9170 | 0.3801 | 0.0000 | 2.0795 | 0.3923 | 0.0000 | 2.4394 | 0.4411 | 0.0000 | 3.2815 | 0.5270 | 0.0000 |
| Attention F/C | 0.2936 | 0.0852 | 0.0007 | 0.1448 | 0.0847 | 0.0894 | −0.0655 | 0.0887 | 0.4545 | 0.0271 | 0.0973 | 0.7808 |
| Attention M/C | 0.1619 | 0.0842 | 0.0564 | −0.0556 | 0.0818 | 0.4978 | −0.1341 | 0.0850 | 0.1166 | −0.1386 | 0.0938 | 0.1416 |
| Clarity F/C | −0.1391 | 0.0991 | 0.1624 | 0.0054 | 0.0957 | 0.5704 | −0.0361 | 0.0994 | 0.7170 | −0.1447 | 0.1089 | 0.1860 |
| Clarity M/C | 0.0780 | 0.0995 | 0.4343 | 0.1972 | 0.0957 | 0.0409 | 0.0767 | 0.1006 | 0.4473 | 0.0206 | 0.1104 | 0.8525 |
| Repair F/C | 0.1048 | 0.0917 | 0.2548 | −0.0862 | 0.0883 | 0.3304 | −0.0832 | 0.0920 | 0.3669 | 0.2976 | 0.1010 | 0.0037 |
| Repair M/C | −0.0603 | 0.0941 | 0.5228 | −0.0121 | 0.0905 | 0.8942 | 0.1840 | 0.0939 | 0.0519 | −0.0017 | 0.1041 | 0.9870 |
| M1 | --- | --- | --- | 0.1108 | 0.0752 | 0.1424 | 0.2530 | 0.0920 | 0.1166 | −0.2851 | 0.0862 | 0.0012 |
| M2 | --- | --- | --- | --- | --- | --- | 0.2530 | 0.0816 | 0.0023 | 0.1529 | 0.0920 | 0.0982 |
| M3 | --- | --- | --- | --- | --- | --- | --- | --- | --- | 0.3675 | 0.0863 | 0.0000 |
| R2 = 0.1610 F(6,163) = 5.2130; p = 0.0001 | R2 = 0.1026 F(7,162) = 2.6455; p = 0.0129 | R2 = 0.1158 F(8,161) = 2.6359; p = 0.0097 | R2 = 0.2299 F(9,162) = 5.3067; p = 0.0000 | |||||||||
| Y = MH5 Child | Specific Indirect Effects | Total Indirect Effect | Direct Effect | ||||||
|---|---|---|---|---|---|---|---|---|---|
| X | Mediator 1 (Attention Child) | Mediator 2 (Clarity Child) | Mediator 3 (Repair Child) | Mediator 4 (Att -> Cl) | Mediator 5 (Att -> Rep) | Mediator 6 (Cl -> Rep) | Mediator 7 (Att -> Cl -> Rep) | ||
| Attention F/C | −0.0837 (−0.1726; −0.0199) | 0.0221 (−0.0153; 0.0739) | −0.0244 (−0.1149; 0.0348) | 0.0050 (−0.0030; 0.0243) | 0.0071 (−0.0089; 0.0323) | 0.0135 (−0.0035; 0.0448) | 0.0030 (−0.0010; 0.0120) | −0.0574 (−0.1726; 0.0483) | 0.0271 (−0.1651; 0.2194) (p = 0.7808) |
| Attention M/C | −0.0461 (−0.1099; 0.0003) | −0.0085 (−0.0528; 0.0208) | −0.0493 (−0.1390; 0.0150) | 0.0027 (−0.0018; 0.0136) | 0.0039 (−0.0052; 0.0199) | −0.0052 (−0.0303; 0.0105) | 0.0017 (−0.0006; 0.0075) | −0.1008 (−0.2164; −0.0091) | −0.1386 (−0.3238; 0.0467) (p = 0.1416) |
| Clarity F/C | 0.0396 (−0.0147; 0.0984) | 0.0083 (−0.0329; 0.0676) | −0.0133 (−0.0923; 0.0686) | −0.0024 (−0.0118; 0.0020) | −0.0034 (−0.0187; 0.0048) | 0.0051 (−0.0237; 0.0287) | −0.0014 (−0.0067; 0.0009) | 0.0326 (−0.0710; 0.1334) | −0.1447 (−0.3598; 0.0704) (p = 0.1860) |
| Clarity M/C | −0.0222 (−0.0864; 0.0330) | 0.0302 (−0.0158; 0.0971) | 0.0282 (−0.0505; 0.1105) | 0.0013 (−0.0029; 0.0090) | 0.0019 (−0.0051; 0.0145) | 0.0183 (−0.0017; 0.0570) | 0.0008 (−0.0015; 0.0050) | 0.0584 (−0.0454; 0.1674) | 0.0206 (−0.1975; 0.2386) (p = 0.8525) |
| Repair F/C | −0.0299 (−0.0927; 0.0271) | −0.0132 (−0.0665; 0.0194) | −0.0306 (−0.1013; 0.0389) | 0.0018 (−0.0027; 0.0098) | 0.0025 (−0.0065; 0.0143) | −0.0080 (−0.0298; 0.0123) | 0.0011 (−0.0013; 0.0054) | −0.0763 (−0.1793; 0.0299) | 0.2976 (0.0982; 0.4970) (p = 0.0037) |
| Repair M/C | 0.0172 (−0.0378; 0.0808) | −0.0018 (−0.0442; 0.0383) | 0.0676 (0.0007; 0.1508) | −0.0010 (−0.0082; 0.0034) | −0.0015 (−0.0123; 0.0064) | −0.0011 (−0.0234; 0.0214) | −0.0006 (−0.0049; 0.0017) | 0.0787 (−0.0224; 0.1923) | −0.0017 (−0.2073; 0.2039) (p = 0.9870) |
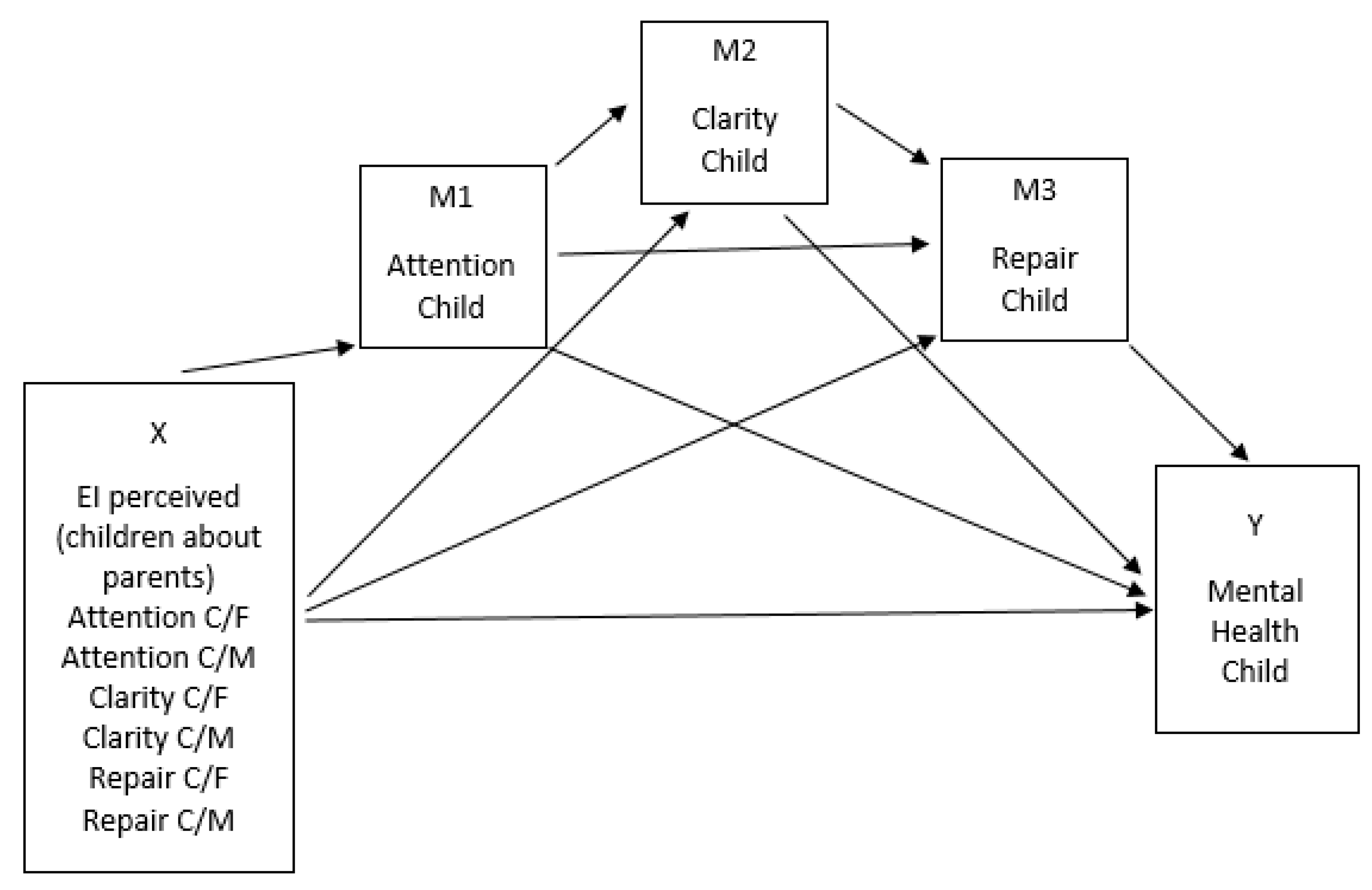
| Consequent | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M1 (Attention Child) | M2 (Clarity Child) | M3 (Repair Child) | Y (MH5) | |||||||||
| Antecedent | Coeff. | SE | p | Coeff. | SE | p | Coeff. | SE | p | Coeff. | SE | p |
| Constant | 0.7703 | 0.3590 | 0.0334 | 1.0373 | 0.3427 | 0.0029 | 1.3775 | 0.3800 | 0.0004 | 3.2603 | 0.4563 | 0.0000 |
| Attention C/F | 0.2795 | 0.0699 | 0.0001 | 0.1998 | 0.0690 | 0.0043 | 0.0811 | 0.0763 | 0.2891 | 0.0776 | 0.0884 | 0.3817 |
| Attention C/M | 0.3567 | 0.0687 | 0.0000 | 0.0942 | 0.0698 | 0.1793 | 0.1505 | 0.0758 | 0.0486 | −0.0149 | 0.0885 | 0.8669 |
| Clarity C/F | −0.0950 | 0.0954 | 0.3208 | 0.1763 | 0.0901 | 0.0520 | 0.0698 | 0.0983 | 0.4789 | 0.0789 | 0.1137 | 0.4887 |
| Clarity C/M | 0.2072 | 0.0945 | 0.0297 | 0.3283 | 0.0902 | 0.0004 | −0.2533 | 0.1012 | 0.0133 | −0.1580 | 0.1192 | 0.1867 |
| Repair C/F | 0.0233 | 0.0737 | 0.7521 | −0.0517 | 0.0694 | 0.4574 | 0.1117 | 0.0750 | 0.1384 | 0.2634 | 0.0872 | 0.0029 |
| Repair C/M | 0.0407 | 0.0686 | 0.5542 | −0.0249 | 0.0647 | 0.7009 | 0.3249 | 0.0698 | 0.0000 | 0.0104 | 0.0859 | 0.9033 |
| M1 | --- | --- | --- | −0.0472 | 0.0737 | 0.5229 | −0.0860 | 0.0796 | 0.2820 | −0.3047 | 0.0923 | 0.0012 |
| M2 | --- | --- | --- | --- | --- | --- | 0.2182 | 0.0848 | 0.0109 | 0.1248 | 0.0999 | 0.2133 |
| M3 | --- | --- | --- | --- | --- | --- | --- | --- | --- | 0.2678 | 0.0910 | 0.0037 |
| R2 = 0.3056 F(6,163) = 11.9543; p = 0.0000 | R2 = 0.2855 F(7,162)= 9.2488; p = 0.0000 | R2 = 0.2397 F(8,161) = 6.3453; p = 0.0000 | R2 = 0.2638 F(9,160) = 6.3706; p = 0.0000 | |||||||||
| Y = MH5 Child | Specific Indirect Effects | Total Indirect Effect | Direct Effect | ||||||
|---|---|---|---|---|---|---|---|---|---|
| X | Mediator 1 (Attention Child) | Mediator 2 (Clarity Child) | Mediator 3 (Reparation Child) | Mediator 4 (Att -> Cl) | Mediator 5 (Att -> Rep) | Mediator 6 (Cl -> Rep) | Mediator 7 (Att -> Cl -> Rep) | ||
| Attention C/F | −0.0851 (−0.1608; −0.0242) | 0.0249 (−0.0169; 0.0892) | 0.0217 (−0.0188; 0.0826) | −0.0016 (−0.0133; 0.0063) | −0.0064 (−0.0234; 0.0054) | 0.0117 (0.0000; 0.0385) | −0.0008 (−0.0047; 0.0029) | −0.0357 (−0.1299; 0.0806) | 0.0776 (−0.0970; 0.22522) (p = 0.3817) |
| Attention C/M | −0.1087 (−0.2228; −0.0394) | 0.0118 (−0.0135; 0.0578) | 0.0403 (−0.0083; 0.0960) | −0.0021 (−0.0143; 0.0099) | −0.0082 (−0.0052; 0.0199) | −0.0052 (−0.0291; 0.0091) | 0.0055 (−0.0060; 0.0215) | −0.0010 (−0.0053; 0.0050) | −0.0149 (−0.1897; 0.1600) (p = 0.8669) |
| Clarity C/F | 0.0289 (−0.0374; 0.0927) | 0.0220 (−0.0208; 0.0788) | 0.0187 (−0.0408; 0.0857) | 0.0006 (−0.0028; 0.0063) | 0.0022 (−0.0032; 0.0133) | 0.0103 (−0.0021; 0.0362) | 0.0003 (−0.0013; 0.0023) | 0.0829 (−0.0374; 0.0927) | 0.0789 (−0.1456; 0.3035) (p = 0.4887) |
| Clarity C/M | −0.0631 (−0.1377; 0.0068) | 0.0410 (−0.0304; 0.1368) | −0.0678 (−0.1642; −0.0047) | −0.0012 (−0.0117; 0.0041) | −0.0048 (−0.0204; 0.0039) | 0.0192 (0.0000; 0.0585) | −0.0006 (−0.0042; 0.0018) | −0.0774 (−0.2077; 0.0724) | −0.1580 (−0.3933; 0.0773) (p = 0.1867) |
| Repair C/F | −0.0071 (−0.0587; 0.0498) | −0.0065 (−0.0416; 0.0208) | 0.0299 (−0.0120; 0.0958) | −0.0001 (−0.0044; 0.0018) | −0.0005 (−0.0070; 0.0044) | −0.0030 (−0.0171; 0.0084) | −0.0001 (−0.0017; 0.0007) | 0.0126 (−0.0715; 0.1194) | 0.2634 (0.0911; 0.4357) (p = 0.0029) |
| Repair C/M | −0.0124 (−0.0661; 0.0353) | −0.0031 (−0.0422; 0.0221) | 0.0870 (0.0176; 0.1738) | −0.0002 (−0.0031; 0.0029) | −0.0009 (−0.0078; 0.0039) | −0.0015 (−0.0175; 0.0088) | −0.0001 (−0.0011; 0.0014) | 0.0687 (−0.0342; 0.1707) | 0.0104 (−0.1591; 0.1800) (p = 0.9033) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Núñez, M.T.; García-Rubio, N.; Fernández-Berrocal, P.; Latorre, J.M. Emotional Intelligence and Mental Health in the Family: The Influence of Emotional Intelligence Perceived by Parents and Children. Int. J. Environ. Res. Public Health 2020, 17, 6255. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176255
Sánchez-Núñez MT, García-Rubio N, Fernández-Berrocal P, Latorre JM. Emotional Intelligence and Mental Health in the Family: The Influence of Emotional Intelligence Perceived by Parents and Children. International Journal of Environmental Research and Public Health. 2020; 17(17):6255. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176255
Chicago/Turabian StyleSánchez-Núñez, María Trinidad, Noelia García-Rubio, Pablo Fernández-Berrocal, and José Miguel Latorre. 2020. "Emotional Intelligence and Mental Health in the Family: The Influence of Emotional Intelligence Perceived by Parents and Children" International Journal of Environmental Research and Public Health 17, no. 17: 6255. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176255