Examining the Effect of Overload on the MHealth Application Resistance Behavior of Elderly Users: An SOR Perspective

Abstract
:1. Introduction
2. Literature Review and Theoretical Background
2.1. Elderly User’s MHealth Usage
2.2. Theoretical Framework of Stimulus-Organism-Response (SOR)
2.2.1. Perceived Overload as Stimulus (S)
2.2.2. Fatigue and Technostress as Organism (O)
2.2.3. Resistance Behavior as Response (R)
2.3. Intergenerational Support
3. Research Model and Hypotheses
3.1. Overload (S) and Psychological Perception (O), Resistance Behavior (R)
3.1.1. Information Overload and Fatigue, Technostress
3.1.2. System Feature Overload and Fatigue, Technostress
3.2. Psychological Perception (O) and Resistance Behavior (R)
3.3. The Role of Intergenerational Support
3.4. The Mediator Role of Fatigue and Technostress
4. Methodology
4.1. Measurement
4.2. Sampling Design
4.3. Common Method Variance Testing
5. Data Analysis and Result
5.1. Measurement Model
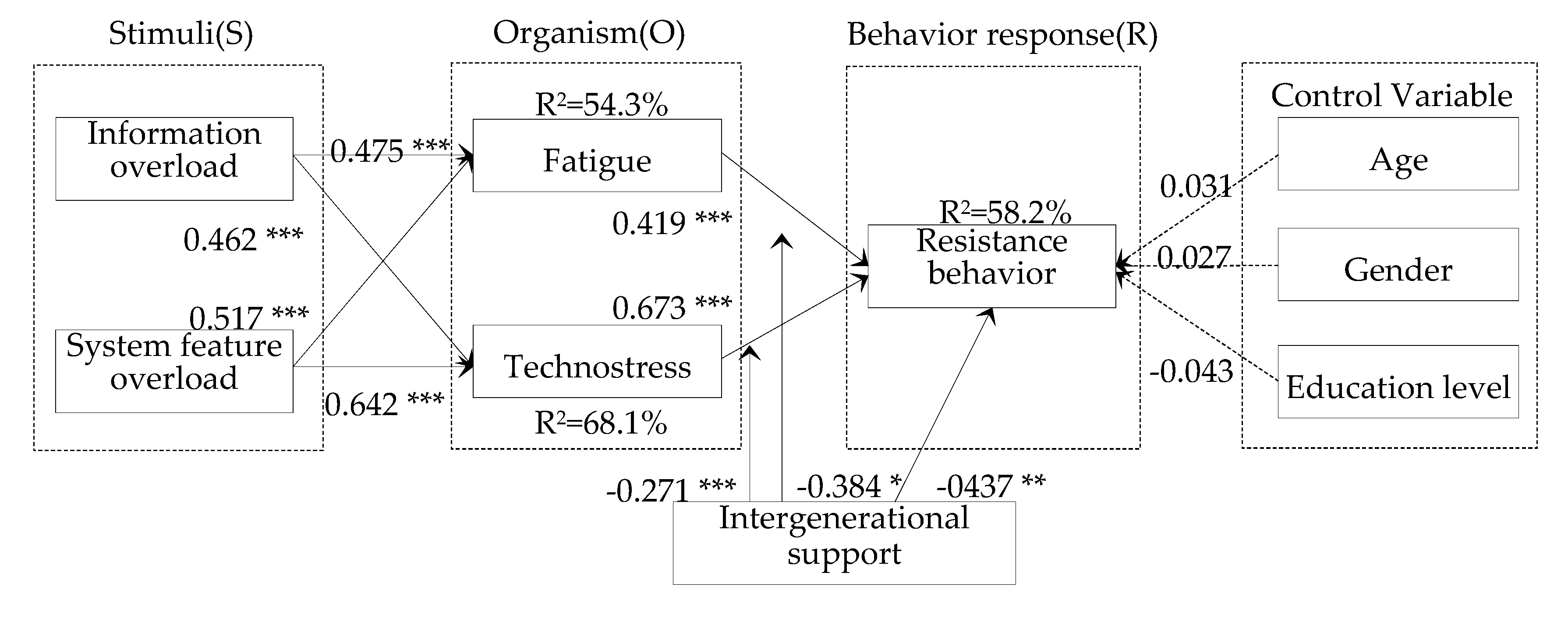
5.2. Structural Model
5.3. Mediation Effect Test
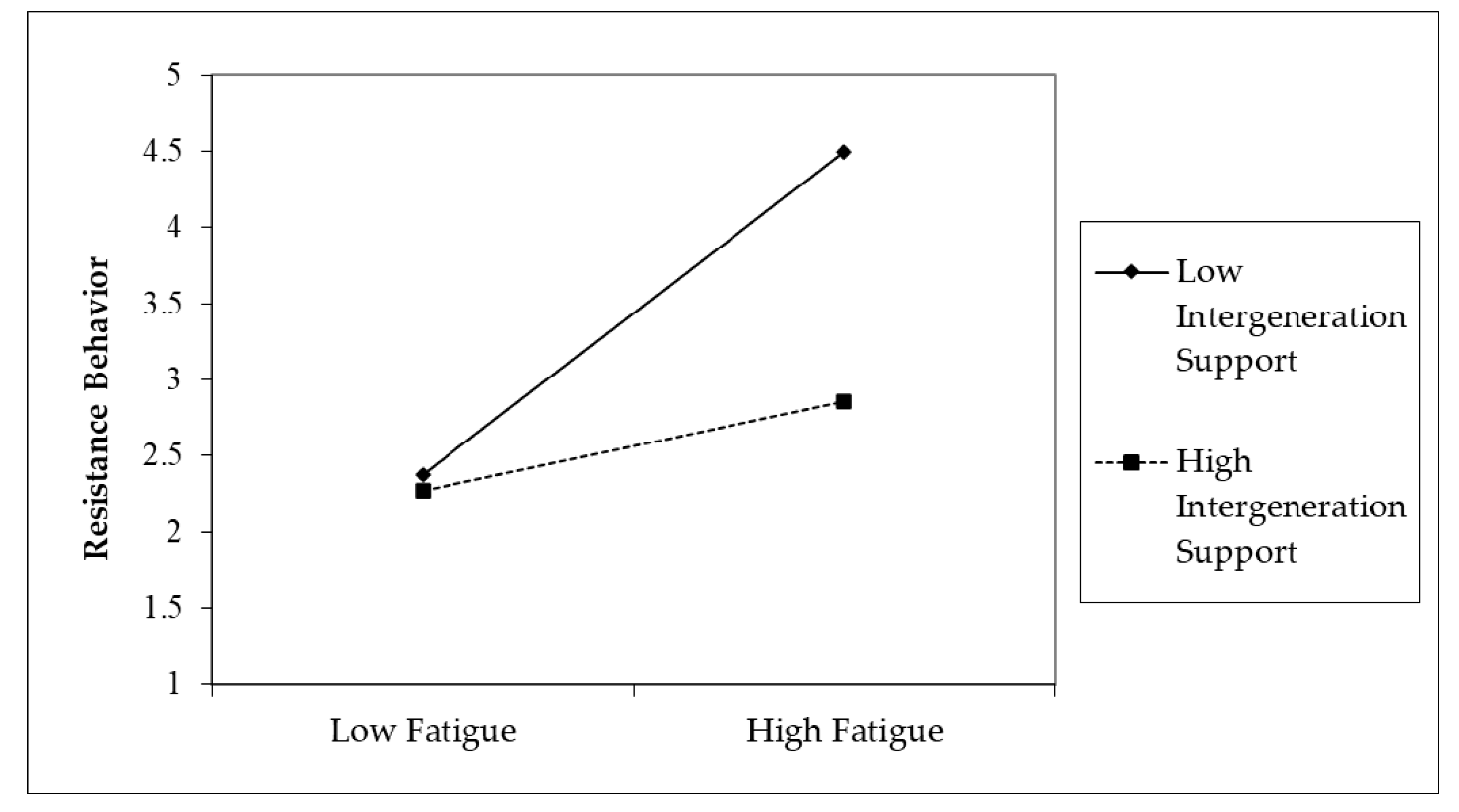
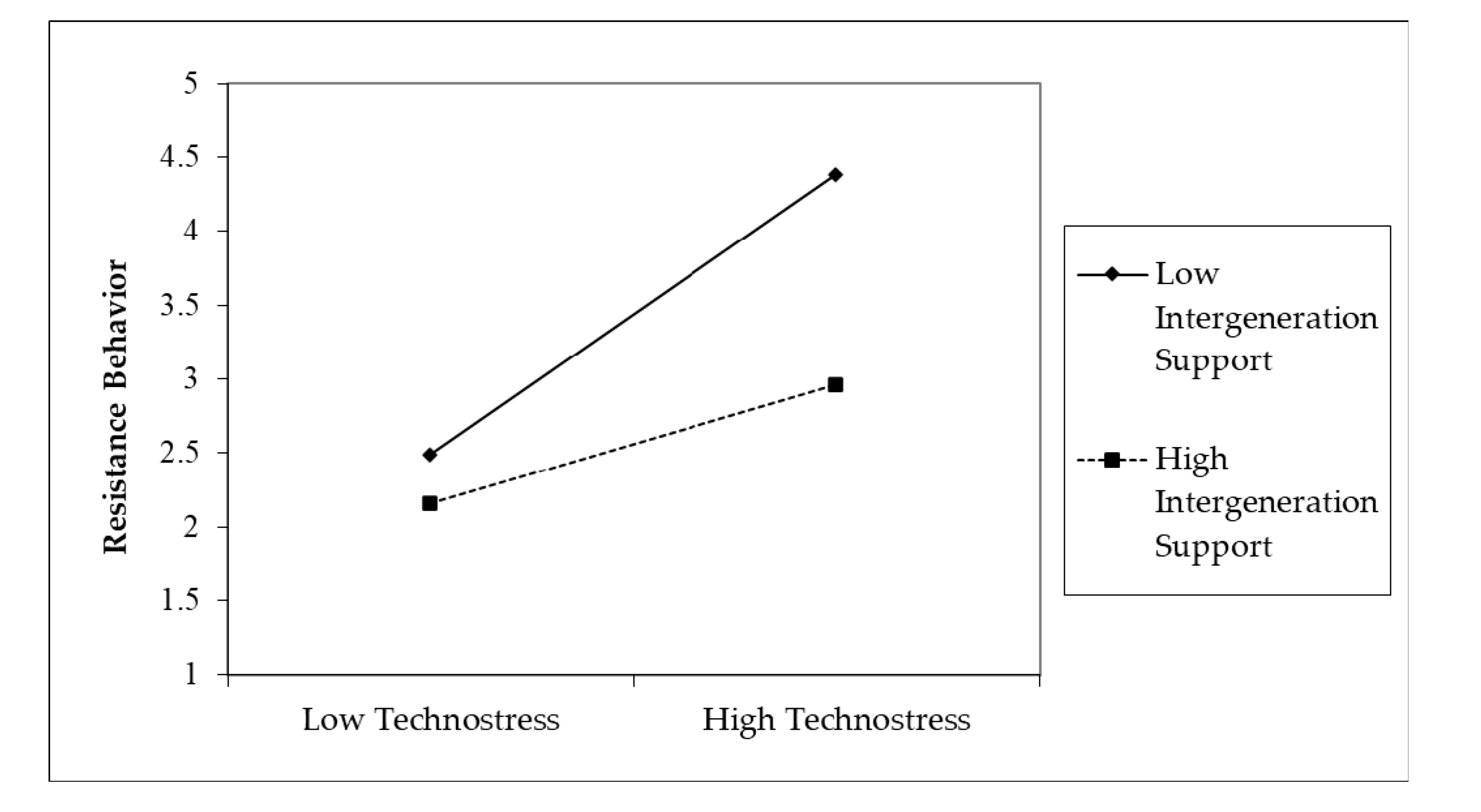
5.4. Moderation Effect Test
6. Discussion
6.1. Key Finding
6.2. Theory Implications
6.3. Practical Contributions
7. Conclusions
7.1. Limitations
7.2. Future Research Suggestions
Author Contributions
Funding
Conflicts of Interest
References
- Deng, Z.; Mo, X.; Liu, S. Comparison of the middle-aged and older users’ adoption of mobile health services in China. Int. J. Med. Inform. 2014, 83, 210–224. [Google Scholar] [CrossRef]
- Kim, B.Y.; Lee, J. Smart devices for older adults managing chronic disease: A scoping review. JMIR Mhealth Uhealth 2017, 5, e69. [Google Scholar] [CrossRef] [Green Version]
- Joe, J.; Demiris, G. Older adults and mobile phones for health: A review. J. Biomed. Inform. 2013, 46, 947–954. [Google Scholar] [CrossRef] [Green Version]
- Gao, C.; Zhou, L.; Liu, Z.; Wang, H.; Bowers, B. Mobile application for diabetes self-management in China: Do they fit for older adults. Int. J. Med. Inform. 2017, 101, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.; Coughlin, J. PERSPECTIVE: Older adults’ adoption of technology:An integrated approach to identifying determinants and barriers. J. Prod. Innov. Manag. 2015, 32, 747–759. [Google Scholar] [CrossRef]
- Hoque, R.; Sorwar, G. Understanding factors influencing the adoption of mHealth by the elderly: An extension of the UTAUT model. Int. J. Med. Inform. 2017, 101, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Cimperman, M.; Brenčič, M.M.; Trkman, P. Analyzing older users’ home telehealth services acceptance behavior—applying an Extended UTAUT model. Int. J. Med. Inform. 2016, 90, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Sun, Y.; Wang, N.; Peng, Z.; Yan, Z. The dark side of elderly acceptance of preventive mobile health services in China. Electron. Mark. 2013, 23, 49–61. [Google Scholar] [CrossRef]
- Quaosar, G.A.A.; Hoque, M.R.; Bao, Y. Investigating factors affecting Elderly’s intention to use m-health services: An empirical study. Telemed. E-Health 2018, 24, 309–314. [Google Scholar] [CrossRef]
- Hsiao, C.H.; Tang, K. Examining a model of mobile healthcare technology acceptance by the elderly in Taiwan. J. Glob. Inf. Technol. Manag. 2015, 18, 292–311. [Google Scholar] [CrossRef]
- Fox, G.; Connolly, R. Mobile health technology adoption across generations: Narrowing the digital divide. Inf. Syst. J. 2018, 28, 995–1019. [Google Scholar] [CrossRef]
- Bao, Y.; Hoque, R.; Wang, S. Investigating the determinants of Chinese adult children’s intention to use online health information for their aged parents. Int. J. Med. Inform. 2017, 102, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Han, S.; Jo, S. Consumer choice of on-demand mHealth app services: Context and contents values using structural equation modeling. Int. J. Med. Inform. 2017, 97, 229–238. [Google Scholar] [CrossRef]
- Karr-Wisniewski, P.; Lu, Y. When more is too much: Operationalizing technology overload and exploring its impact on knowledge worker productivity. Comput. Hum. Behav. 2010, 26, 1061–1072. [Google Scholar] [CrossRef]
- Yao, J.; Cao, X. The balancing mechanism of social networking overuse and rational usage. Comput. Hum. Behav. 2017, 75, 415–422. [Google Scholar] [CrossRef]
- Guo, Y.Y.; Lu, Z.Z.; Kuang, H.B.; Wang, C. Information avoidance behavior on social network sites: Information irrelevance, overload, and the moderating role of time pressure. Int. J. Inf. Manag. 2020, 52, 102067. [Google Scholar] [CrossRef]
- Zhang, S.; Zhao, L.; Lu, Y.; Yang, J. Do you get tired of socializing? An empirical explanation of discontinuous usage behaviour in social network services. Inf. Manag. 2016, 53, 904–914. [Google Scholar] [CrossRef] [Green Version]
- Cao, X.; Sun, J. Exploring the effect of overload on the discontinuous intention of social media users: An SOR perspective. Comput. Hum. Behav. 2018, 81, 10–18. [Google Scholar] [CrossRef]
- Yang, H.L.; Lin, S. The reasons why elderly mobile users adopt ubiquitous mobile social service. Comput. Hum. Behav. 2019, 93, 62–75. [Google Scholar] [CrossRef]
- The Aging Population Continues to Intensify, the Mobile Medical Market Will Break 12 Billion. Available online: https://d.qianzhan.com/xnews/detail/541/171204-56bee9c6.html (accessed on 14 December 2017).
- 2018 China Mobile Medical APP Product Monitoring Report. Available online: http://www.100ec.cn/detail-6445175.html (accessed on 2 April 2018).
- Meng, F. Studies on the Adoption and Usage of Mobile Health Services by Elderly Users: The Role of Trust. Ph.D. Thesis, Harbin Institute of Technology, Harbin, China, 2019. (In Chinese). [Google Scholar]
- Mehrabian, A.; Russell, J. An Approach to Environmental Psychology; MIT Press: Cambridge, UK, 1974. [Google Scholar]
- Bedford, O.; Yeh, K.H. The history and the future of the psychology of filial piety: Chinese norms to contextualized personality construct. Front. Psychol. 2019, 10, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.P.; Yi, C. Filial norms and intergenerational support to aging parents in China and Taiwan. Int. J. Soc. Welf. 2011, 20, 109–120. [Google Scholar] [CrossRef]
- Neves, B.B.; Amaro, F. Too old for technology? How the elderly of Lisbon use and perceive ICT. J. Community Inform. 2012, 8, 1–12. [Google Scholar]
- Hjälm, A. “Because we know our limits”: Elderly parents’ views on intergenerational proximity and intimacy. J. Aging Stud. 2012, 26, 296–308. [Google Scholar] [CrossRef]
- Barrantes Cáceres, R.; Cozzubo Chaparro, A. Age for learning, age for teaching: The role of inter-generational, intra-household learning in Internet use by older adults in Latin America. Inf. Commun. Soc. 2019, 22, 250–266. [Google Scholar] [CrossRef]
- Eynon, R.; Helsper, E. Family dynamics and Internet use in Britain: What role do children play in adults’ engagement with the Internet? Inf. Commun. Soc. 2015, 18, 156–171. [Google Scholar] [CrossRef] [Green Version]
- Kaphle, S.; Chaturvedi, S.; Chaudhuri, I.; Krishnan, R.; Lesh, N. Adoption and usage of mHealth technology on quality and experience of care provided by frontline workers: Observations from rural india. JMIR Mhealth Uhealth 2015, 3, e61. [Google Scholar] [CrossRef]
- Leigh, M.; Ashall-Payne, L.; Andrews, T. Barriers and facilitators to the adoption of mobile health among health care professionals from the united kingdom: Discrete choice experiment. JMIR Mhealth Uhealth 2020, 8, e17704. [Google Scholar] [CrossRef]
- Venkatesh, M.; Davis, D. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef] [Green Version]
- Davis, F. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989, 340–391. [Google Scholar] [CrossRef] [Green Version]
- Adapa, A.; Nah, F.F.H.; Hall, R.H.; Siau, K.; Smith, S.N. Factors Influencing the Adoption of Smart Wearable Devices. Int. J. Hum. Comput. Interact. 2018, 34, 399–409. [Google Scholar] [CrossRef]
- Hoque, M.R. An empirical study of mHealth adoption in a developing country: The moderating effect of gender concern. BMC Med. Inform. Decis. Mak. 2016, 16, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- To, W.-M.; Lee, P.K.C.; Lu, J.; Wang, J.; Yang, Y.; Yu, Q. What Motivates Chinese Young Adults to Use mHealth? Healthcare 2019, 7, 156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alam, M.Z.; Hu, W.; Kaium, M.A.; Hoque, M.R.; Alam, M.M.D. Understanding the determinants of mHealth apps adoption in Bangladesh: A SEM-Neural network approach. Technol. Soc. 2020, 61, 101255. [Google Scholar] [CrossRef]
- Guo, X.; Zhang, X.; Sun, Y. The privacy-personalization paradox in mHealth services acceptance of different age groups. Electron. Commer. Res. Appl. 2016, 16, 55–65. [Google Scholar] [CrossRef]
- Tsai, J.M.; Cheng, M.J.; Tsai, H.H.; Hung, S.W.; Chen, Y.L. Acceptance and resistance of telehealth: The perspective of dual-factor concepts in technology adoption. Int. J. Inf. Manag. 2019, 49, 34–44. [Google Scholar] [CrossRef]
- Zhang, Y.J.; Zhang, J.L.; Chen, J. A review on the study of user resistance in the context of information systems implementation. Libr. Inf. Serv. 2014, 58, 44–51. (In Chinese) [Google Scholar]
- Klaus, T.; Blanton, J. User resistance determinants and the psychological contract in enterprise system implementations. Eur. J. Inf. Syst. 2010, 19, 625–636. [Google Scholar] [CrossRef]
- Venkatesh, V.; Thong, J.Y.; Xu, X. Consumer acceptance and use of information technology: Extending the unified theory of acceptance and use of technology. MIS Q. 2012, 36, 157–178. [Google Scholar] [CrossRef] [Green Version]
- Joshi, K. A model of users’perspective on change: The case of information systems technology implementation. MIS Q. 1991, 15, 229–242. [Google Scholar] [CrossRef]
- Selander, L.; Henfridsson, O. Cynicism as user resistance in it imple mentation. Inf. Syst. J. 2012, 22, 289–312. [Google Scholar] [CrossRef]
- Aslam, M. User resistance in post ERP implementation. Bus. Process Manag. J. 2011, 17, 266–275. [Google Scholar]
- Shih, B.-Y.; Chen, C.-Y.; Chen, Z.-S. Selecting occupational safety equipment by MCDM approach considering universal design principles. Hum. Factors Ergon. Manuf. 2006, 16, 61–81. [Google Scholar]
- Zhou, T. Examining users’ knowledge sharing behaviour in online health communities. Data Technol. Appl. 2019, 53, 442–455. [Google Scholar] [CrossRef]
- Fu, S.; Yan, Q.; Feng, G. Who will attract you? Similarity effect among users on online purchase intention of movie tickets in the social shopping context. Int. J. Inf. Manag. 2018, 40, 88–102. [Google Scholar] [CrossRef]
- Lee, A.R.; Son, S.M.; Kim, K. Information and communication technology overload and social networking service fatigue: A stress perspective. Comput. Hum. Behav. 2016, 55, 51–61. [Google Scholar] [CrossRef]
- Thompson, D.V.; Hamilton, R.W.; Rust, R. Feature fatigue: When product capabilities become too much of a good thing. J. Mark. Res. 2005, 42, 431–442. [Google Scholar] [CrossRef]
- Ravindran, T.; Kuan, A.C.Y.; Lian, D.G.H. Antecedents and effects of social network fatigue. J. Assoc. Inf. Sci. Technol. 2014, 65, 2306–2320. [Google Scholar] [CrossRef]
- Li, M.; Wang, L.; Wu, M. An integrated methodology for robustness analysis in feature fatigue problem. Int. J. Prod. Res. 2014, 52, 5985–5996. [Google Scholar] [CrossRef]
- Piper, B.F.; Lindsey, A.M.; Dodd, M. Fatigue mechanisms in cancer patients: Developing nursing theory. Oncol. Nurs. Forum 1987, 14, 17–23. [Google Scholar]
- Åhsberg, E. Dimensions of fatigue in different working populations. Scand. J. Psychol. 2000, 41, 231–241. [Google Scholar] [CrossRef]
- Ayyagari, R.; Grover, V.; Purvis, R. Technostress: Technological antecedents and implications. MIS Q. 2011, 35, 831–858. [Google Scholar] [CrossRef] [Green Version]
- Tarafdar, M.; Tu, Q.; Ragu-Nathan, T. Impact of technostress on end-user satisfaction and performance. J. Manag. Inf. Syst. 2010, 27, 303–334. [Google Scholar] [CrossRef]
- Kim, H.W.; Kankanhalli, A. Investigating user resistance to information systems implementation: A status quo bias perspective. MIS Q. 2009, 33, 567–582. [Google Scholar] [CrossRef] [Green Version]
- Lapointe, L.; Rivard, S. A multilevel model of resistance to information technology implementation. MIS Q. 2005, 29, 461–491. [Google Scholar] [CrossRef] [Green Version]
- Joseph, R.C. Individual resistance to IT innovations. Commun. ACM 2010, 53, 144–146. [Google Scholar] [CrossRef]
- Foster, M.V.; Sethares, K.A. Facilitators and barriers to the adoption of telehealth in older adults: An integrative review. Cin Comput. Inform. Nurs. 2014, 32, 523–533. [Google Scholar] [CrossRef]
- Sixsmith, J.; Sixsmith, A.; Fänge, A.M.; Naumann, D.; Kucsera, C.; Tomsone, S.; Kaak, M.; Dahlin-Ivanoff, S.; Woolrych, R. Healthy ageing and home: The perspectives of very old people in five European countries. Soc. Sci. Med. 2014, 106, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Chaouali, W. Once a user, always a user: Enablers and inhibitors of continuance intention of mobile social networking sites. Telemat. Inform. 2016, 33, 1022–1033. [Google Scholar] [CrossRef]
- Wildenbos, G.A.; Peute, L.W.; Jaspers, M. A framework for evaluating mHealth tools for Older Patients on Usability. Stud Health Technol. Inf. 2015, 210, 783–787. [Google Scholar]
- Wildenbos, G.A.; Peute, L.; Jaspers, M. Aging barriers influencing mobile health usability for older adults: A literature based framework (MOLD-US). Int. J. Med. Inform. 2018, 114, 66–75. [Google Scholar] [CrossRef]
- Melenhorst, A.S.; Rogers, W.A.; Bouwhuis, D. Older adults’ motivated choice for technological innovation: Evidence for benefit-driven selectivity. Psychol. Psychol. Aging 2006, 21, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Bhattacherjee, A.; Davis, C.J.; Connolly, A.J.; Hikmet, N. User response to mandatory IT use: A coping theory perspective. Eur. J. Inf. Syst. 2018, 27, 395–414. [Google Scholar] [CrossRef]
- Ragu-Nathan, T.S.; Tarafdar, M.; Ragu-Nathan, B.S.; Tu, Q. The consequences of technostress for end users in organizations: Conceptual development and empirical validation. Inf. Syst. Res. 2008, 19, 417–433. [Google Scholar] [CrossRef] [Green Version]
- Luqman, A.; Cao, X.; Ali, A.; Masood, A.; Yu, L. Empirical investigation of Facebook discontinues usage intentions based on SOR paradigm. Comput. Hum. Behav. 2017, 70, 544–555. [Google Scholar] [CrossRef]
- Cao, Y.; Zhang, J.; Ma, L.; Qin, X.; Li, J. Examining User’s Initial Trust Building in Mobile Online Health Community Adopting. Int. J. Environ. Res. Public Health 2020, 17, 3945. [Google Scholar] [CrossRef]
- Fang, C.; Zhang, J. Users’ continued participation behavior in social Q&A communities: A motivation perspective. Comput. Hum. Behav. 2019, 92, 87–109. [Google Scholar]
- Zhang, J.; Chen, X.; Fang, C. Transmission of a supplier’s disruption risk along the supply chain: A further investigation of the Chinese automotive industry. Prod. Plan. Control 2018, 29, 773–789. [Google Scholar] [CrossRef]
- Kim, H.W. The effects of switching costs on user resistance to enterprise systems implementation. IEEE Trans. Eng. Manag. 2010, 58, 471–482. [Google Scholar] [CrossRef]
- He, J.P.; Huang, X. The Smartphone Use and Eudaimonic Well-being of Urban Elderly: Based on Intergenerational Support and TAM. Chin. J. Commun. 2020, 3, 49–73. (In Chinese) [Google Scholar]
- Classification of Mobile Health Application. Available online: https://www.apicloud.com/blogDetails/2879 (accessed on 8 April 2020).
- Rönkkö, M.; Ylitalo, J. PLS marker variable approach to diagnosing and controlling for method variance. In Proceedings of the 34th International Conference Information Systems, Shanghai, China, 4–7 December 2011; pp. 1–16. [Google Scholar]
- Nitzl, C.; Roldan, J.L.; Cepeda, G. Mediation analysis in partial least squares path modeling: Helping researchers discuss more sophisticated models. Ind. Manag. Data Syst. 2016, 116, 1849–1864. [Google Scholar] [CrossRef]
- Akter, S.; D’Ambra, J.; Ray, P. Trustworthiness in mHealth information services: An assessment of a hierarchical model with mediating and moderating effects using partial least squares (PLS). J. Am. Soc. Inf. Sci. Technol. 2011, 62, 100–116. [Google Scholar] [CrossRef] [Green Version]
- Matthew-Maich, N.; Harris, L.; Ploeg, J.; Markle-Reid, M.; Valaitis, R.; Ibrahim, S.; Gafni, A.; Isaacs, S. Designing, implementing, and evaluating mobile health technologies for managing chronic conditions in older adults: A scoping review. JMIR Mhealth Uhealthealth 2016, 4, e29. [Google Scholar] [CrossRef] [PubMed]
- Bolle, S.; Romijn, G.; Smets, E.M.; Loos, E.F.; Kunneman, M.; Weert, J.C.M. Older cancer patients’user experiences with web-based health information tools: A think-aloud study. J. Med. Internet Res. 2016, 18, e208. [Google Scholar] [CrossRef] [PubMed]
- Fischer, S.H.; David, D.; Crotty, B.H.; Dierks, M.; Safran, C. Acceptance and use of health information technology by community-dwelling elders. Int. J. Med. Inform. 2014, 83, 624–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, D.X.; Deng, S.Y.; Zheng, Q.; Liang, C.Y.; Wu, J. Impacts of case-based health knowledge system in hospital management: The mediating role of group effectiveness. Inf. Manag. 2019, 56, 103162. [Google Scholar] [CrossRef]
- Gu, D.X.; Liang, C.Y.; Zhao, H.M. A case-based reasoning system based on weighted heterogeneous value distance metric for breast cancer diagnosis. Artif. Intell. Med. 2017, 77, 31–47. [Google Scholar] [CrossRef]
- Gu, D.X. Case-Based Knowledge Discovery for Medical & Health Decision Support; Science Press: Beijing, China, 2020. (In Chinese) [Google Scholar]
- Gu, D.; Li, J.; Li, X.; Liang, C. Visualizing the knowledge structure and evolution of big data research in healthcare informatics. Int. J. Med. Inform. 2017, 98, 22–32. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Construct | Measurement Items | Sources |
|---|---|---|
| Information overload (IO) | IO1: I am often distracted by the excessive amount of information in mHealth APP | [14] |
| IO2: I feel that I am overwhelmed by too much health information in mHealth APP | ||
| IO3: Processing too much health information is a burden for me | ||
| System feature overload (SO) | SO1: I feel distracted by many features included in mHealth APP which are not related to my main purpose | [14] |
| SO2: Some features in mHealth APP are too complex for me | ||
| SO3: Too many poor sub features in mHealth APP makes performing my task even harder | ||
| Fatigue (FA) | FA1: I feel exhausted during using mHealth APP | [54] |
| FA2: I feel boredom from using mHealth APP | ||
| FA3: I feel drained when I use mHealth APP to search health information | ||
| Technostress (TE) | TE1: The functions in mHealth APP are too complicated and beyond my ability | [55] |
| TE2: I feel tired for spending a long time to understand and use mHealth APP | ||
| TE3: Learning how to operate mHealth APP makes me feel stressed | ||
| Resistance behavior (RB) | RB1: I object to using mHealth APP | [72] |
| RB2: I disagree with the using of mHealth software | ||
| RB3: I oppose the life changes brought by the mHealth APP | ||
| Intergenerational support (IS) | IS1: My children often encourage me to use mHealth APP | [73] |
| IS2: My children often instruct me to use some functions of mHealth APP | ||
| IS3: My children will help me solve the difficulties in using mHealth APP |
| Profile | Sample Composition | Frequency | Percentage |
|---|---|---|---|
| Gender | Male | 185 | 58.36% |
| Female | 132 | 41.64% | |
| Age | 60–65 | 196 | 61.83% |
| 66–70 | 113 | 35.65% | |
| 71–75 | 7 | 2.21% | |
| Over 75 | 1 | 0.31% | |
| Education background | Senior High School/lower | 197 | 62.15% |
| College | 107 | 33.75% | |
| Graduate school and above | 13 | 4.10% | |
| Occupation | Public service or educational | 79 | 24.92% |
| Information Industry | 33 | 10.41% | |
| Peasants | 68 | 21.45% | |
| Retiree | 137 | 43.22% | |
| mHealth applications | Online health community (e.g.,: Chunyu Doctor, Haodafu Online, Dinxiang Doctor, WeDoctor, Pingan Good Doctor) | 101 | 31.86% |
| The doctor appointment mHealth application (e.g.,: Wing Health, WeChat Appointment System; Qu Hospital) | 73 | 23.03% | |
| The medical e-commerce mHealth application (e.g.,: Ali Health, Self-testing Drug, Kangaiduo Palm Drug Store, One Medicine Network) | 143 | 45.11% |
| Construct | Indicator | Factor Loading | AVE | Composite Reliability | Cronbach’s Alpha |
|---|---|---|---|---|---|
| Information overload (IO) | IO1 | 0.881 | 0.798 | 0.922 | 0.889 |
| IO2 | 0.906 | ||||
| IO3 | 0.892 | ||||
| System feature overload (SO) | SO1 | 0.855 | 0.731 | 0.891 | 0.981 |
| SO2 | 0.842 | ||||
| SO3 | 0.867 | ||||
| Fatigue (FA) | FA1 | 0.861 | 0.819 | 0.931 | 0.809 |
| FA2 | 0.938 | ||||
| FA3 | 0.914 | ||||
| Technostress (TE) | TE1 | 0.844 | 0.724 | 0.887 | 0.972 |
| TE2 | 0.898 | ||||
| TE3 | 0.809 | ||||
| Resistance behavior (RB) | RB1 | 0.883 | 0.755 | 0.903 | 0.807 |
| RB2 | 0.859 | ||||
| RB3 | 0.865 | ||||
| Intergenerational support (IS) | IS1 | 0.944 | 0.884 | 0.958 | 0.912 |
| IS2 | 0.935 | ||||
| IS3 | 0.942 |
| Construct | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| 1. IO | 0.893 | |||||
| 2. SQ | 0.317 | 0.855 | ||||
| 3. FA | 0.281 | 0.43 | 0.905 | |||
| 4. TE | 0.143 | 0.45 | 0.352 | 0.851 | ||
| 5. RB | 0.155 | 0.19 | 0.286 | 0.273 | 0.869 | |
| 6. IS | 0.163 | 0.201 | 0.374 | 0.284 | 0.174 | 0.940 |
| Mediation Relationship | Indirect Effect | Direct Effect | Mediation Effect | ||
|---|---|---|---|---|---|
| 95% CIs of the Indirect Effect | Significance or Not | 95% CIs of the Direct Effect | Significance or Not | ||
| H6a: IO→FA→RB | [0.052, 0.173] | Yes | [−0.042, 0.134] | No | full |
| H6b: SO→FA→RB | [0.023, 0.256] | Yes | [0.06, 0.14] | Yes | partial |
| H6c: IO→TE→RB | [0.037, 0.251] | Yes | [−0.38, 0,71] | No | full |
| H6d: SO→TE→RB | [0.045, 0.248] | Yes | [0.034, 0.262] | Yes | partial |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, Y.; Li, J.; Qin, X.; Hu, B. Examining the Effect of Overload on the MHealth Application Resistance Behavior of Elderly Users: An SOR Perspective. Int. J. Environ. Res. Public Health 2020, 17, 6658. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186658
Cao Y, Li J, Qin X, Hu B. Examining the Effect of Overload on the MHealth Application Resistance Behavior of Elderly Users: An SOR Perspective. International Journal of Environmental Research and Public Health. 2020; 17(18):6658. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186658
Chicago/Turabian StyleCao, Yuanyuan, Junjun Li, Xinghong Qin, and Baoliang Hu. 2020. "Examining the Effect of Overload on the MHealth Application Resistance Behavior of Elderly Users: An SOR Perspective" International Journal of Environmental Research and Public Health 17, no. 18: 6658. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186658