Impacts of COVID-19 on Electronic Cigarette Purchasing, Use and Related Behaviors

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview
2.2. Participants
2.3. Concept Mapping Procedures
2.4. Brainstorming
2.5. Sorting
2.6. Rating
2.7. Representation
2.8. Analysis
3. Results
3.1. Participant Characteristics
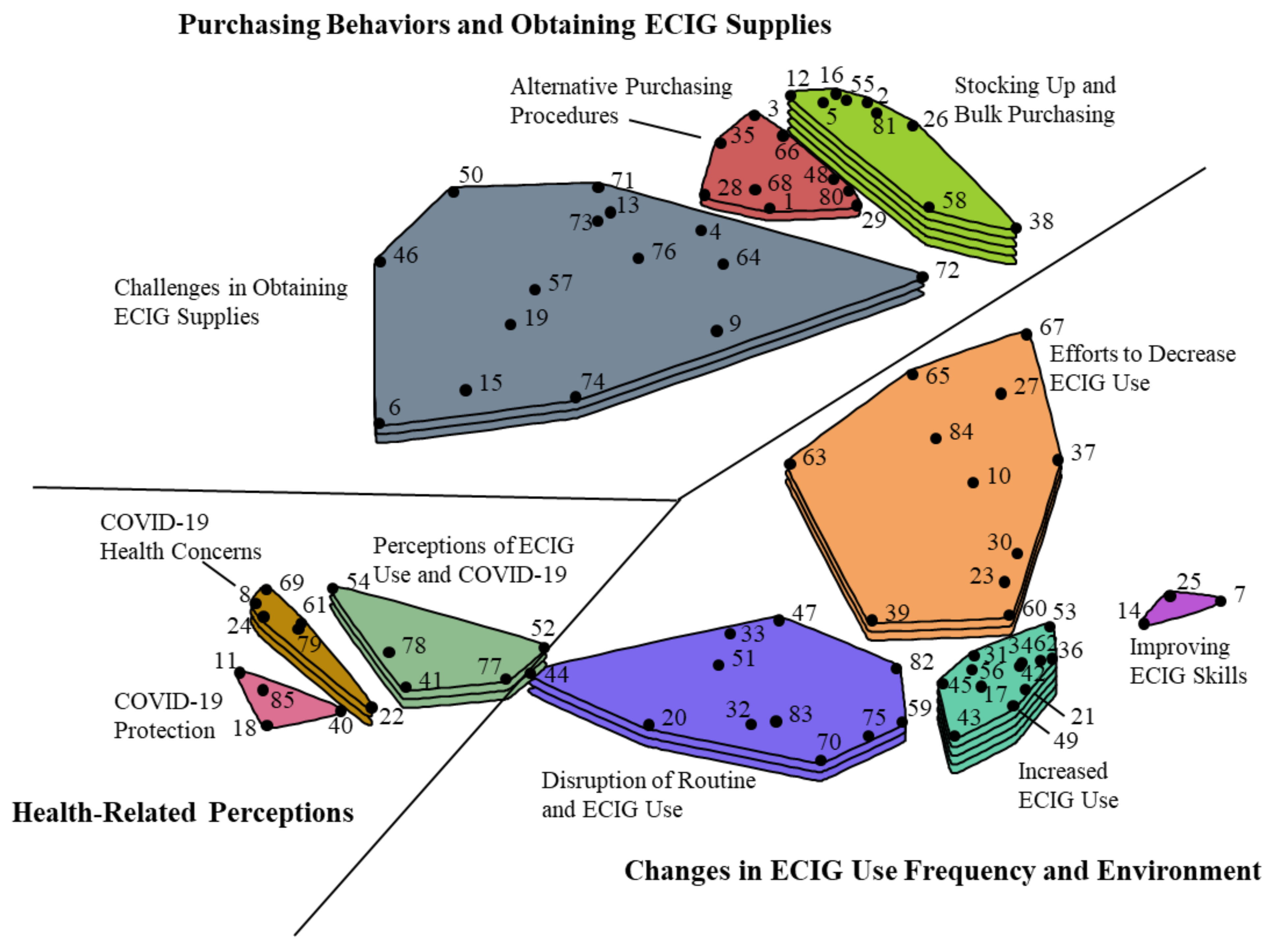
3.2. Concept Mapping Results
3.2.1. Purchasing Behaviors and Obtaining ECIG Supplies
3.2.2. Changes in ECIG Use Frequency and Environment
3.2.3. Health-related Perceptions
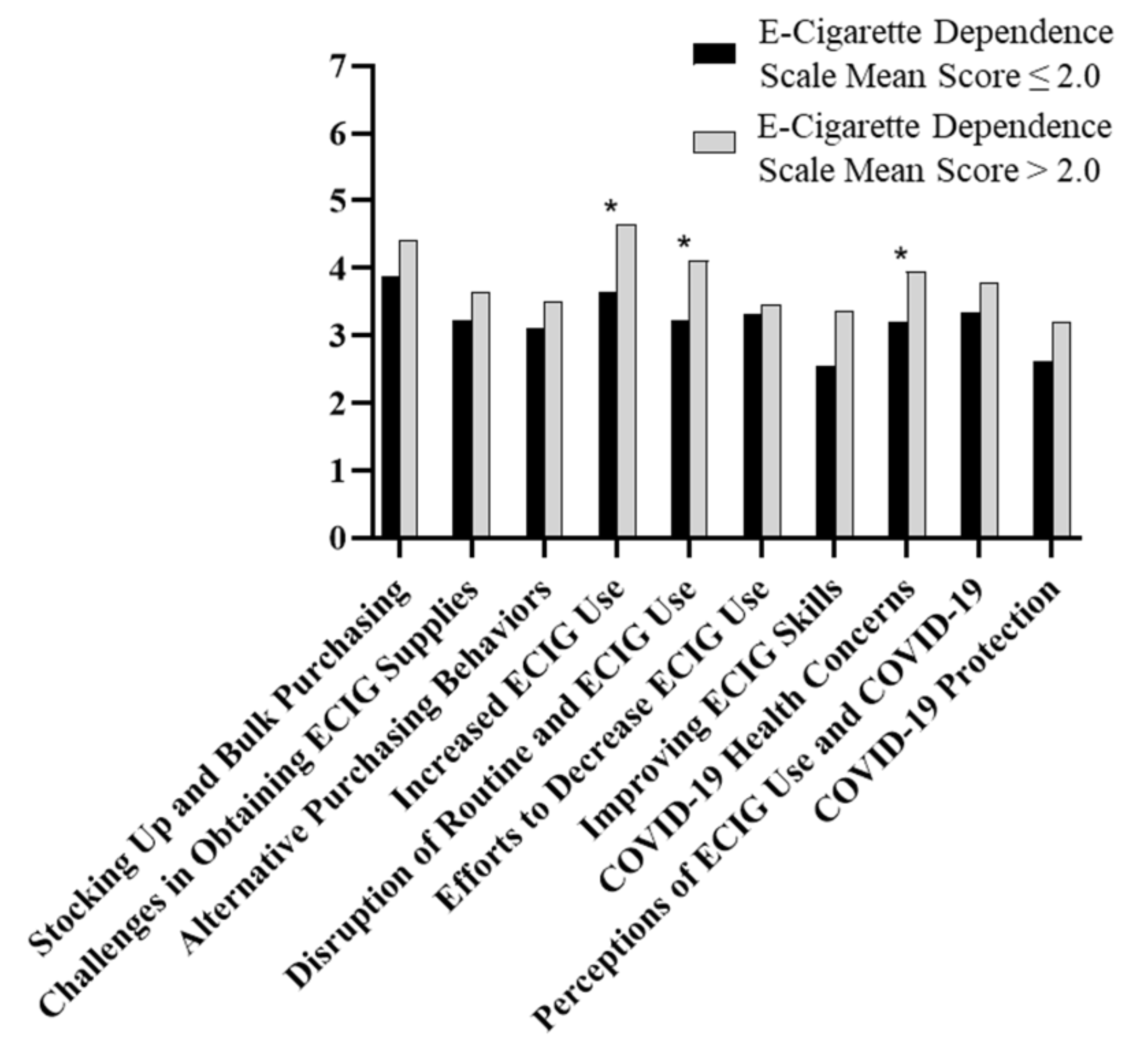
3.3. Cluster Comparisons
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 13 July 2020).
- Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19) in the U.S. Available online: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html (accessed on 13 July 2020).
- Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19) Social Distancing. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/social-distancing.html (accessed on 23 June 2020).
- Moreland, A.; Herlihy, C.; Tynan, M.A.; Sunshine, G.; McCord, R.F.; Hilton, C.; Poovey, J.; Werner, A.K.; Jones, C.D.; Fulmer, E.B.; et al. Timing of State and Territorial COVID-19 Stay–at–Home Orders and Changes in Population Movement–United States, March 1–May 31, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1198–1203. [Google Scholar] [CrossRef]
- Agaku, I.T.; King, B.A.; Husten, C.G.; Bunnell, R.; Ambrose, B.K.; Hu, S.S.; Holder-Hayes, E.; Day, H.R. Centers for Disease Control and Prevention (CDC) Tobacco product use among adults—United States, 2012–2013. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 542–547. [Google Scholar] [PubMed]
- Creamer, M.R.; Wang, T.W.; Babb, S.; Cullen, K.A.; Day, H.; Willis, G.; Jamal, A.; Neff, L. Tobacco Product Use and Cessation Indicators Among Adults—United States, 2018. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 1013–1019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.W.; Asman, K.; Gentzke, A.S.; Cullen, K.A.; Holder-Hayes, E.; Reyes-Guzman, C.; Jamal, A.; Neff, L.; King, B.A. Tobacco Product Use Among Adults—United States, 2017. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1225–1232. [Google Scholar] [CrossRef] [PubMed]
- Kasza, K.A.; Ambrose, B.K.; Conway, K.P.; Borek, N.; Taylor, K.; Goniewicz, M.L.; Cummings, K.M.; Sharma, E.; Pearson, J.L.; Green, V.R.; et al. Tobacco-Product Use by Adults and Youths in the United States in 2013 and 2014. N. Engl. J. Med. 2017, 376, 342–353. [Google Scholar] [CrossRef] [Green Version]
- Phillips, E.; Wang, T.W.; Husten, C.G.; Corey, C.G.; Apelberg, B.J.; Jamal, A.; Homa, D.M.; King, B.A. Tobacco Product Use Among Adults-United States, 2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 1209–1215. [Google Scholar] [CrossRef]
- Arrazola, R.A.; Singh, T.; Corey, C.G.; Husten, C.G.; Neff, L.J.; Apelberg, B.J.; Bunnell, R.E.; Choiniere, C.J.; King, B.A.; Cox, S.; et al. Tobacco use among middle and high school students-United States, 2011–2014. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 381–385. [Google Scholar]
- Jamal, A.; Gentzke, A.; Hu, S.S.; Cullen, K.A.; Apelberg, B.J.; Homa, D.M.; King, B.A. Tobacco Use Among Middle and High School Students - United States, 2011–2016. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 597–603. [Google Scholar] [CrossRef] [Green Version]
- Dai, H.; Leventhal, A.M. Prevalence of e-Cigarette Use Among Adults in the United States, 2014–2018. JAMA 2019. [Google Scholar] [CrossRef] [Green Version]
- Gentzke, A.S. Vital Signs: Tobacco Product Use Among Middle and High School Students—United States, 2011–2018. MMWR Morb. Mortal. Wkly. Rep. 2019, 68. [Google Scholar] [CrossRef] [Green Version]
- Cullen, K.A.; Gentzke, A.S.; Sawdey, M.D.; Chang, J.T.; Anic, G.M.; Wang, T.W.; Creamer, M.R.; Jamal, A.; Ambrose, B.K.; King, B.A. e-Cigarette Use Among Youth in the United States, 2019. JAMA 2019. [Google Scholar] [CrossRef]
- Boer, H.; Seydel, E.R. Protection motivation theory. In Predicting Health Behaviour: Research and Practice with Social Cognition Models; Open University Press: New York, NY USA, 2005; pp. 81–126. ISBN 978-0-335-19321-9. [Google Scholar]
- Yan, Y.; Jacques-Tiura, A.J.; Chen, X.; Xie, N.; Chen, J.; Yang, N.; Gong, J.; MacDonell, K.K. Application of the Protection Motivation Theory in Predicting Cigarette Smoking Among Adolescents in China. Addict. Behav. 2014, 39, 181–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, R.W. A Protection Motivation Theory of Fear Appeals and Attitude Change1. J. Psychol. 1975, 91, 93–114. [Google Scholar] [CrossRef] [PubMed]
- Rosas, S.R.; Kane, M. Quality and rigor of the concept mapping methodology: A pooled study analysis. Eval. Program. Plann. 2012, 35, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Soule, E.K.; Maloney, S.F.; Guy, M.C.; Eissenberg, T.; Fagan, P. User identified positive outcome expectancies of electronic cigarette use: A concept mapping study. Psychol. Addict. Behav. 2017, 31, 343–353. [Google Scholar] [CrossRef]
- Soule, E.K.; Maloney, S.F.; Guy, M.C.; Eissenberg, T.; Fagan, P. User-identified electronic cigarette behavioral strategies and device characteristics for cigarette smoking reduction. Addict. Behav. 2017, 79, 93–101. [Google Scholar] [CrossRef]
- Soule, E.K.; Lee, J.G.L.; Egan, K.L.; Bode, K.M.; Desrosiers, A.C.; Guy, M.C.; Breland, A.; Fagan, P. “I cannot live without my vape”: Electronic cigarette user-identified indicators of vaping dependence. Drug Alcohol Depend. 2020, 209, 107886. [Google Scholar] [CrossRef]
- Morean, M.E.; Krishnan-Sarin, S.; Sussman, S.; Foulds, J.; Fishbein, H.; Grana, R.; O’Malley, S.S. Psychometric evaluation of the Patient-Reported Outcomes Measurement Information System (PROMIS)Nicotine Dependence Item Bankfor use with electronic cigarettes. Nicotine Tob. Res. 2019. [Google Scholar] [CrossRef] [PubMed]
- Soule, E.K.; Nasim, A.; Rosas, S. Adverse Effects of Electronic Cigarette Use: A Concept Mapping Approach. Nicotine Tob. Res. 2016, 18, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Dennis, A.R.; Valacich, J.S. Computer brainstorms: More heads are better than one. J. Appl. Psychol. 1993, 78, 531–537. [Google Scholar] [CrossRef]
- Dennis, A.R.; Williams, M.L. Electronic brainstorming: Theory, research, and future directions. In Group Creativity: Innovation Through Collaboration; Oxford University Press: New York, NY, USA, 2003; pp. 160–178. ISBN 978-0-19-514730-8. [Google Scholar]
- DeRosa, D.M.; Smith, C.L.; Hantula, D.A. The medium matters: Mining the long-promised merit of group interaction in creative idea generation tasks in a meta-analysis of the electronic group brainstorming literature. Comput. Hum. Behav. 2007, 23, 1549–1581. [Google Scholar] [CrossRef]
- Dugosh, K.L.; Paulus, P.B.; Roland, E.J.; Yang, H.C. Cognitive stimulation in brainstorming. J. Pers. Soc. Psychol. 2000, 79, 722–735. [Google Scholar] [CrossRef] [PubMed]
- Dugosh, K.L.; Paulus, P.B. Cognitive and social comparison processes in brainstorming. J. Exp. Soc. Psychol. 2005, 41, 313–320. [Google Scholar] [CrossRef]
- Kruskal, J.B.; Wish, M. Multidimensional Scaling; Sage Publications: Beverly Hills, CA, USA, 1978. [Google Scholar]
- Ward, J.H. Hierarchical grouping to optimize an objective function. J. Am. Stat. Assoc. 1963, 58, 236–244. [Google Scholar] [CrossRef]
- What is JUUL Vape Liquid? | Learn about JUULpods Flavors | JUUL. Available online: https://www.juul.com/resources/What-is-JUUL-Vape-Liquid-All-JUUL-Pod-Flavors (accessed on 23 June 2020).
- Talih, S.; Salman, R.; El-Hage, R.; Karam, E.; Karaoghlanian, N.; El-Hellani, A.; Saliba, N.; Shihadeh, A. Characteristics and toxicant emissions of JUUL electronic cigarettes. Tob. Control 2019. [Google Scholar] [CrossRef] [PubMed]
- Hutzler, C.; Paschke, M.; Kruschinski, S.; Henkler, F.; Hahn, J.; Luch, A. Chemical hazards present in liquids and vapors of electronic cigarettes. Arch. Toxicol. 2014, 88, 1295–1308. [Google Scholar] [CrossRef]
- Talih, S.; Balhas, Z.; Salman, R.; Karaoghlanian, N.; Shihadeh, A. “Direct Dripping”: A High-Temperature, High-Formaldehyde Emission Electronic Cigarette Use Method. Nicotine Tob. Res. 2016, 18, 453–459. [Google Scholar] [CrossRef]
- Farsalinos, K.; Barbouni, A.; Niaura, R. Systematic review of the prevalence of current smoking among hospitalized COVID-19 patients in China: Could nicotine be a therapeutic option? Intern. Emerg. Med. 2020. [Google Scholar] [CrossRef]
- Patanavanich, R.; Glantz, S.A. Smoking is Associated with COVID-19 Progression: A Meta-Analysis. Nicotine Tob. Res. 2020. [Google Scholar] [CrossRef]
- Vardavas, C.I.; Nikitara, K. COVID-19 and smoking: A systematic review of the evidence. Tob. Induc. Dis. 2020, 18, 20. [Google Scholar] [CrossRef]
- Madison, M.C.; Landers, C.T.; Gu, B.-H.; Chang, C.-Y.; Tung, H.-Y.; You, R.; Hong, M.J.; Baghaei, N.; Song, L.-Z.; Porter, P.; et al. Electronic cigarettes disrupt lung lipid homeostasis and innate immunity independent of nicotine. J. Clin. Invest. 2019, 129, 4290–4304. [Google Scholar] [CrossRef] [Green Version]
- Ainsworth, S.B.; Milligan, D.W.A. Surfactant Therapy for Respiratory Distress Syndrome in Premature Neonates. Am. J. Respir. Med. 2002, 1, 417–433. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. CDC Tobacco Free Electronic Cigarettes (E-cigarettes). Available online: https://www.cdc.gov/tobacco/basic_information/e-cigarettes/index.htm (accessed on 20 May 2020).



{kind=link}
{kind=link}
| Characteristic | N | % |
|---|---|---|
| Age (M, SD) | (35.1, 10.8) | |
| Gender | ||
| Women | 51 | 54.8 |
| Men | 40 | 43.0 |
| Transgender or other | 1 | 1.1 |
| Ethnicity | ||
| Hispanic/Latino(a) | 13 | 14.0 |
| Race | ||
| American Indian/Alaskan Native | 0 | 0 |
| Asian | 6 | 6.5 |
| Native Hawaiian/Pacific Islander | 0 | 0 |
| Black/African American | 10 | 10.8 |
| White/European American | 71 | 76.3 |
| More than one race | 5 | 5.4 |
| Education | ||
| High School diploma or GED | 12 | 12.9 |
| Some college credit, but less than 1 year | 7 | 7.5 |
| 1 or more years of college, no degree | 16 | 17.2 |
| Associate’s degree | 11 | 11.8 |
| Bachelor’s degree | 36 | 38.7 |
| Higher than a bachelor’s degree | 10 | 10.8 |
| Regular ECIG use history 1 | ||
| 1–3 months | 5 | 5.4 |
| 4–6 months | 6 | 6.5 |
| 7–12 months | 10 | 10.8 |
| Between 1–2 years | 28 | 30.1 |
| More than 2 years | 43 | 46.2 |
| ECIG frequency | ||
| At least once per day | 11 | 16.3 |
| Every once in a while throughout the day | 28 | 18.4 |
| Fairly frequently throughout the day | 38 | 46.9 |
| Almost always throughout most of the day | 14 | 18.4 |
| Regular ECIG device | ||
| Prefilled disposable/Cig-alike | 7 | 18.4 |
| E-hookah | 2 | 2.0 |
| Vape pen/eGo style device | 18 | 16.3 |
| Rebuildable/Mechanical Mod or Box Mod | 20 | 20.4 |
| E-cigar | 2 | 6.1 |
| E-pipe | 1 | 1.1 |
| Pod mod such as JUUL | 40 | 36.7 |
| Disposable vape such as a Posh, Puff bar, Mojo, or other similar device | 1 | 1.1 |
| Other | 2 | 2.2 |
| ECIG liquid nicotine concentration | ||
| 0 mg/mL | 1 | 1.1 |
| 1–4 mg/mL | 28 | 30.1 |
| 5–10 mg/mL | 28 | 30.1 |
| 11–20 mg/mL | 14 | 15.1 |
| 21–30 mg/mL | 5 | 5.4 |
| 31–40 mg/mL | 2 | 2.2 |
| 50 mg/mL | 7 | 7.5 |
| >50 mg/mL | 3 | 3.2 |
| Don’t know | 2 | 2.2 |
| Preferred ECIG liquid flavor | ||
| Menthol or mint | 25 | 26.9 |
| Tobacco | 29 | 31.2 |
| Fruit | 23 | 24.7 |
| Vanilla or crème | 3 | 3.2 |
| Other (including clove, spice, nut, alcoholic drink, coffee/tea, candy, or dessert) | 12 | 12.9 |
| Location ECIG liquid typically purchased pre-COVID-19 2 | ||
| Vape shop/tobacco store | 57 | 61.3 |
| Gas station or convenience store | 29 | 31.2 |
| Retail store like a grocery store, drug store, or department store | 11 | 11.8 |
| Order online/over the internet | 39 | 41.2 |
| Homemade/Do-it-yourself (DIY) | 3 | 3.2 |
| ECIG use after waking | ||
| After 60 minutes | 20 | 21.5 |
| 31–60 minutes | 30 | 32.3 |
| 6–30 minutes | 22 | 23.7 |
| Within 5 minutes | 19 | 20.4 |
| E-Cigarette Dependence Scale Score 3 (M, SD) | (2.06, 0.83) | |
| E-Cigarette Dependence Scale—Reach for ECIG 3 | ||
| Never | 2 | 2.2 |
| Rarely | 10 | 10.8 |
| Sometimes | 40 | 43.0 |
| Often | 29 | 31.2 |
| Almost always | 11 | 11.8 |
| E-Cigarette Dependence Scale—Vape more before not allowed 3 | ||
| Never | 5 | 5.4 |
| Rarely | 8 | 8.6 |
| Sometimes | 32 | 34.4 |
| Often | 30 | 32.3 |
| Almost always | 17 | 18.3 |
| E-Cigarette Dependence Scale—Drop everything to buy ECIGs 3 | ||
| Never | 19 | 20.4 |
| Rarely | 31 | 33.3 |
| Sometimes | 20 | 21.5 |
| Often | 18 | 19.4 |
| Almost always | 4 | 4.3 |
| E-Cigarette Dependence Scale—Craving gets intolerable 3 | ||
| Never | 10 | 10.8 |
| Rarely | 23 | 24.7 |
| Sometimes | 37 | 39.8 |
| Often | 11 | 11.8 |
| Almost always | 10 | 10.8 |
| Lifetime use of 100+ cigarettes | ||
| Yes | 81 | 87.1 |
| Current use of other tobacco products | ||
| Cigarettes | 50 | 53.8 |
| Cigar | 11 | 11.8 |
| Cigarillo or little cigar | 19 | 20.4 |
| Smokeless | 7 | 7.5 |
| Waterpipe | 11 | 11.8 |
| Cluster | Statement | Mean Rating |
|---|---|---|
| Stocking Up and Bulk Purchasing 1 | 4.13 | |
| 58. I check my supplies to make sure I have what I need. | 5.15 | |
| 16. I bought extra vaping supplies and e-liquid/pods to stock up. | 4.85 | |
| 26. I am buying more e-liquid/pods so I don’t have to go to the store as much. | 4.31 | |
| 12. I order online to make sure I have vaping supplies at home and a steady supply coming in. | 4.23 | |
| 5. I am purchasing several vaping products at once because I am uncertain if I can leave my home. | 4.23 | |
| 2. I purchased multiple vaping products because I’m uncertain if vaping products will be available in the future. | 4.11 | |
| Challenges in Obtaining ECIG Supplies 1 | 3.40 | |
| 9. I go to the store less due to social distancing. | 5.54 | |
| 73. I am more conscious of prices for vaping products. | 4.54 | |
| 76. The price of vaping products has increased because of the COVID-19. | 4.21 | |
| 71. It is challenging to return or replace vaping products. | 4.12 | |
| 57. I worry that I will not be able to get vaping supplies during the COVID-19 pandemic. | 4.06 | |
| 15. I am hesitant to go out and get more e-liquid/pods because I am scared to go near other people. | 3.63 | |
| 19. I am mad that my vape shops are closed and may go out of business due to COVID-19. | 3.52 | |
| 64. I am low on money and don’t want to have to spend it on vaping products. | 3.49 | |
| 6. I am worried I may smoke cigarettes because it is difficult to get vaping supplies. | 3.10 | |
| 4. I have not ordered any new vaping products due to delays caused by COVID-19. | 2.79 | |
| 13. Ordering vaping products online made me nervous. | 2.63 | |
| 72. I’ve been using burnt pods because the vape I bought online due to lockdown is defective. | 2.46 | |
| 46. I am not affected because I make most of my own e-liquid (DIY). | 2.46 | |
| 74. I have thought about quitting vaping because I bought a defective vape and it takes too long to get a new one. | 2.27 | |
| 50. Someone makes my e-liquid for me so I don’t have to go to the store. | 2.19 | |
| 55. I purchase my e-liquid/pods in bulk now. | 3.81 | |
| 81. I buy e-liquid/pods in bulk to minimize trips to the store, but since I am also vaping more it has balanced out and not really helped. | 3.25 | |
| 38. I find myself buying more vaping products online because I am bored. | 3.21 | |
| Alternative Purchasing Procedures 1 | 3.27 | |
| 3. I ordered vaping products online. | 4.80 | |
| 35. I already purchase my vaping products online, so I do not need to go out for them. | 4.15 | |
| 66. I ordered vaping products/supplies online and paid extra for shipping. | 3.77 | |
| 68. It is difficult to obtain vaping products in store or online because many things are out of stock. | 3.62 | |
| 48. I have to call multiple stores to ask if they have the vaping products I want. | 3.05 | |
| 80. I can only buy vapes/e-cigarettes from a convenience/grocery store so my options are limited. | 2.84 | |
| 1. I am unable to purchase vaping products. | 2.56 | |
| 29. I purchased vaping supplies by using curbside pickup at the store. | 2.51 | |
| 28. I bought a nasty vape/e-cigarette from a convenience store to get through. | 2.17 | |
| Increased ECIG Use 2 | 4.07 | |
| 43. I like that I can vape while working at home. | 4.89 | |
| 34. I vape more because I am bored. | 4.79 | |
| 49. I am trying to vape more than smoke cigarettes. | 4.63 | |
| 42. I vape more than usual. | 4.52 | |
| 56. I vape more because I am at home where it is allowed vs. other environments pre-COVID-19. | 4.47 | |
| 62. I am vaping more because I have to stay home and I am not going other places. | 4.32 | |
| 17. I am vaping more because I am not currently working and have nothing to do. | 3.96 | |
| 31. I see my friends less now because of quarantine so I am vaping more to deal with the isolation. | 3.89 | |
| 45. I vape more because I stay up later and sleep less. | 3.80 | |
| 53. I try to vape in private because I have increased my usage. | 3.31 | |
| 36. I vape more often because I am not supposed to smoke cigarettes in the house. | 3.16 | |
| 21. I vape more because I am around my family more. | 3.07 | |
| Disruption of Routine and ECIG Use 2 | 3.59 | |
| 33. I don’t let anyone else use my vape/e-cigarette. | 5.54 | |
| 51. I try to distance myself further from people when I vape. | 4.70 | |
| 32. I have vaped more to help calm my anxiety and the panic feeling caused by COVID-19. | 4.30 | |
| 59. I crave my vape/e-cigarette more often. | 4.28 | |
| 75. I am more aware of how much I vape because I have to vape around my family/roommates. | 3.79 | |
| 47. Vaping has made me stay at home so I avoid contact with others. | 3.16 | |
| 83. My cravings to vape are becoming unbearable. | 3.05 | |
| 20. COVID-19 has caused me to smoke more cigarettes. | 2.98 | |
| 70. I get into arguments with my spouse/partner because they do not like how often I vape. | 2.63 | |
| 82. My family/roommates won’t let me vape in the house. | 2.58 | |
| 44. I don’t feel well because I am not able to vape. | 2.51 | |
| Efforts to Decrease ECIG Use 2 | 3.38 | |
| 10. I vape the tanks/pods until the very last drop so I don’t have to go out as often. | 4.51 | |
| 27. I am trying to ration my e-liquid/pods. | 4.06 | |
| 67. I am trying to vape less and buy fewer supplies to save money. | 3.67 | |
| 65. I am more mindful of the amount I vape because it is no longer easy to obtain products in store or online. | 3.65 | |
| 60. I wait longer to vape after I wake up. | 3.48 | |
| 30. I find myself going longer in between vaping/not taking as many hits. | 3.47 | |
| 37. I am vaping less to try to extend what I have instead of buying more online. | 3.38 | |
| 84. I vape less because I don’t want to go out to buy more supplies. | 3.05 | |
| 23. I vape less. | 2.93 | |
| 39. I don’t vape outside anymore. | 2.86 | |
| 63. I have started rolling my own cigarettes in order to vape and smoke store-bought cigarettes less. | 2.09 | |
| Improving ECIG Skills 2 | 2.90 | |
| 25. I have tried new flavors and brands because of being at home and I don’t have much to do. | 3.33 | |
| 7. I have more time to perfect my homemade/DIY e-liquid flavors because I am at home more. | 2.69 | |
| 14. I have learned new vape tricks due to being at home more. | 2.68 | |
| COVID-19 Health Concerns 3 | 3.53 | |
| 24. I worry about how vaping is affecting my health. | 4.42 | |
| 69. I am concerned about vaping increasing the chances of complications from COVID-19. | 3.77 | |
| 61. COVID-19 has made me very aware of my chest and lung pain from vaping. | 3.70 | |
| 8. When I cough while vaping it makes me worried about COVID-19. | 3.64 | |
| 22. Since I have increased my usage I am afraid of getting popcorn lung. | 3.12 | |
| 79. I worry about my health so I will stop vaping until COVID-19 is gone for sure. | 2.52 | |
| Perceptions of ECIG Use and COVID-19 3 | 3.49 | |
| 54. I am not scared or concerned about vaping due to COVID-19. | 3.91 | |
| 52. COVID-19 has not affected my vaping at all. | 3.88 | |
| 78. I have thought about quitting or reducing my vaping because of COVID-19. | 3.63 | |
| 41. Vaping has made me safe because people keep away from me when I am vaping. | 3.37 | |
| 77. I’m frustrated because I thought COVID-19 would help me quit, but I am still vaping the same amount. | 2.67 | |
| COVID-19 Protection 3 | 2.84 | |
| 40. I don’t stress too much because I am pretty healthy. | 4.17 | |
| 11. I have wondered if vaping provides a protective layer to prevent COVID-19. | 2.53 | |
| 85. I think vaping may kill the COVID-19 virus due to the heat from vaping. | 2.33 | |
| 18. I think vaping will increase my immune system. | 2.32 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soule, E.K.; Mayne, S.; Snipes, W.; Guy, M.C.; Breland, A.; Fagan, P. Impacts of COVID-19 on Electronic Cigarette Purchasing, Use and Related Behaviors. Int. J. Environ. Res. Public Health 2020, 17, 6762. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186762
Soule EK, Mayne S, Snipes W, Guy MC, Breland A, Fagan P. Impacts of COVID-19 on Electronic Cigarette Purchasing, Use and Related Behaviors. International Journal of Environmental Research and Public Health. 2020; 17(18):6762. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186762
Chicago/Turabian StyleSoule, Eric K., Shannon Mayne, William Snipes, Mignonne C. Guy, Alison Breland, and Pebbles Fagan. 2020. "Impacts of COVID-19 on Electronic Cigarette Purchasing, Use and Related Behaviors" International Journal of Environmental Research and Public Health 17, no. 18: 6762. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186762