Leaders’ Future Orientation and Public Health Investment Intention: A Moderated Mediation Model of Self-Efficacy and Perceived Social Support

Abstract
:1. Introduction
2. Literature and Hypotheses
2.1. Public Health Policy
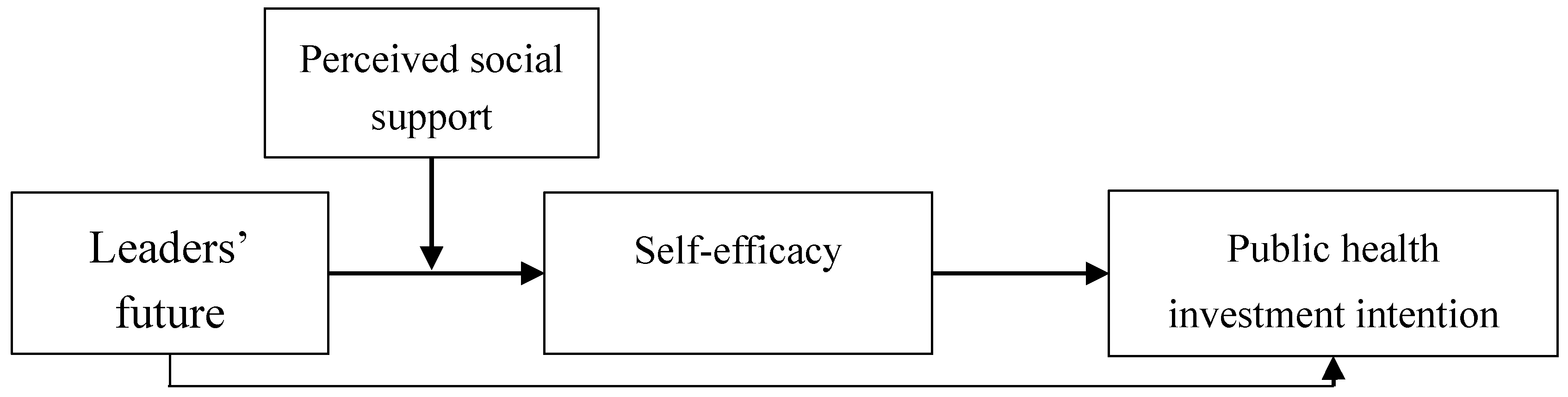
2.2. Leaders’ Future Orientation and Public Health Investment Intention
2.3. The Mediating Role of Self-Efficacy
2.4. The Moderating Role of Perceived Social Support
3. Methods
3.1. Measures
3.2. Sample and Data Collection
3.3. Analysis Methods
3.4. Ethical Consideration
4. Results
4.1. Descriptive Statistics
4.2. Confirmatory Factor Analysis
4.3. Reliability and Validity
4.4. Common Method Bias
4.5. Hypothesis Testing
5. Discussion and Implications
5.1. Theoretical Implications
5.2. Practical Implications
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Anisetti, M.; Ardagna, C.; Bellandi, V.; Cremonini, M.; Frati, F.; Damiani, E. Privacy-aware Big Data Analytics as a service for public health policies in smart cities. Sustain. Cities Soc. 2018, 39, 68–77. [Google Scholar] [CrossRef]
- Li, X.; Lu, J.; Hu, S.; Cheng, K.K.; De Maeseneer, J.; Meng, Q.; Hu, S. The primary health-care system in China. Lancet 2017, 390, 2584–2594. [Google Scholar] [CrossRef]
- Degeling, C.; Carter, S.M.; Rychetnik, L. Which public and why deliberate?—A scoping review of public deliberation in public health and health policy research. Soc. Sci. Med. 2015, 131, 114–121. [Google Scholar] [CrossRef] [Green Version]
- Perreira, K.M.; Pedroza, J.M. Policies of exclusion: Implications for the health of immigrants and their children. Annu. Rev. Public Health 2019, 40, 147–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansson, E.; Fosse, E.; Tillgren, P. National public health policy in a local context—Implementation in two Swedish municipalities. Health Policy 2011, 103, 219–227. [Google Scholar] [CrossRef]
- Fu, M.; Liu, C.; Yang, M. Effects of public health policies on the health status and medical service utilization of Chinese internal migrants. China Econ. Rev. 2020, 62, 101464. [Google Scholar] [CrossRef]
- Gao, J.; Woodward, A.; Vardoulakis, S.; Kovats, S.; Wilkinson, P.; Li, L.; Liu, X. Haze, public health and mitigation measures in China: A review of the current evidence for further policy response. Sci. Total Environ. 2017, 578, 148–157. [Google Scholar] [CrossRef]
- Bosworth, R.; Cameron, T.A.; DeShazo, J.R. Willingness to pay for public health policies to treat illnesses. J. Health Econ. 2015, 39, 74–88. [Google Scholar] [CrossRef]
- Tubbing, L.; Harting, J.; Stronks, K. Unravelling the concept of integrated public health policy: Concept mapping with Dutch experts from science, policy, and practice. Health Policy 2015, 119, 749–759. [Google Scholar] [CrossRef]
- Oliver, K.; Everett, M.; Verma, A.; de Vocht, F. The human factor: Re-organisations in public health policy. Health Policy 2012, 106, 97–103. [Google Scholar] [CrossRef]
- Schönfeldt, H.C.; Hall, N.; Pretorius, B. The important role of food composition in policies and programmes for better public health: A South African case study. Food Chem. 2018, 238, 94–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stassen, K.R.; Gislason, M.; Leroy, P. Impact of environmental discourses on public health policy arrangements: A comparative study in the UK and Flanders (Belgium). Public Health 2010, 124, 581–592. [Google Scholar] [CrossRef]
- Usunier, J.C. Valette-Florence, P. The Time Styles Scale: A review of developments and replications over 15 years. Time Soc. 2007, 16, 333–366. [Google Scholar] [CrossRef]
- Thelken, H.N.; de Jong, G. The impact of values and future orientation on intention formation within sustainable entrepreneurship. J. Clean. Prod. 2020, 266, 122052. [Google Scholar] [CrossRef]
- Xiao, Y.; Bowen, N.K.; Lindsey, M.A. Racial/ethnic measurement invariance of the School Success Profile (SSP)’s future orientation scale. J. Sch. Psychol. 2018, 71, 85–107. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy in Changing Societies; Cambridge University Press: Cambridge, MA, USA, 1995. [Google Scholar]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Schwarzer, R.; Bäßler, J.; Kwiatek, P.; Schröder, K.; Zhang, J.X. The assessment of optimistic self-beliefs: Comparison of the German, Spanish, and Chinese versions of the general self-efficacy scale. Appl. Psychol. 1997, 46, 69–88. [Google Scholar] [CrossRef]
- Gottlieb, B.H.; Bergen, A.E. Social support concepts and measures. J. Psychosom. Res. 2010, 69, 511–520. [Google Scholar] [CrossRef]
- Barber, B. The Logic and Limits of Trust; Rutgers University Press: New Brunswick, NJ, USA, 1983. [Google Scholar]
- Yamagishi, T.; Tamagishi, M. Trust and commitment in the United States and Japan. Motiv. Emot. 1994, 18, 129–166. [Google Scholar] [CrossRef]
- World Health Organization. World Health Reports 2020. Available online: https://www.who.int/topics/health_policy/en/ (accessed on 10 July 2020).
- World Health Organization. Investment for Health and Well-Being: A Review of the Social Return on Investment from Public Health Policies to Support Implementing the Sustainable Development Goals by Building on Health 2020. Available online: https://www.euro.who.int/__data/assets/pdf_file/0008/345797/HEN51.pdf?ua=1 (accessed on 11 August 2017).
- Seginer, R.; Mahajna, S. Future orientation links perceived parenting and academic achievement: Gender differences among Muslim adolescents in Israel. Learn. Individ. Differ. 2018, 67, 197–208. [Google Scholar] [CrossRef]
- Zhu, J.; Hu, S.; Wang, J.; Zheng, X. Future orientation promotes climate concern and mitigation. J. Clean. Prod. 2020, 262, 121212. [Google Scholar] [CrossRef]
- Magee, W.; Upenieks, L. Gender differences in self-esteem, unvarnished self-evaluation, future orientation, self-enhancement and self-derogation in a US national sample. Personal. Individ. Differ. 2019, 149, 66–77. [Google Scholar] [CrossRef]
- Chekima, B.; Chekima, K.; Chekima, K. Understanding factors underlying actual consumption of organic food: The moderating effect of future orientation. Food Qual. Prefer. 2019, 74, 49–58. [Google Scholar] [CrossRef]
- Chen, B.B.; Kruger, D. Future orientation as a mediator between perceived environmental cues in likelihood of future success and procrastination. Personal. Individ. Differ. 2017, 108, 128–132. [Google Scholar] [CrossRef]
- Rawls, J. A Theory of Justice; Harvard University Press: Cambridge, MA, USA, 1999. [Google Scholar]
- Robeyns, I. Ideal theory in theory and practice. Soc. Theory Pract. 2008, 34, 341–362. [Google Scholar] [CrossRef] [Green Version]
- Tower, S.L. Utopianism: A very Short Introduction; Oxford University Press: Oxford, UK, 2010. [Google Scholar]
- Manuel, F.E.; Manuel, F. Utopian Thought in the Western World; Blackwell: Oxford, UK, 1979. [Google Scholar]
- Farrelly, C. Introduction to Contemporary Political Theory; Sage Publications: London, UK, 2004. [Google Scholar]
- Young, I.M. The ideal of community and the politics of difference. Soc. Theory Pract. 1986, 1, 1–26. [Google Scholar] [CrossRef]
- Scott, A. Classical and Contemporary Sociological Theory: Text and Readings; Pine Forge Press: New York, NY, USA, 2008. [Google Scholar]
- Pavel, N. Human Values Compatible with Sustainable Development. J. Hum. Values 2013, 19, 5–13. [Google Scholar]
- Ruth, L. The Concept of Utopia; Peter Lang: New York, NY, USA, 2010. [Google Scholar]
- Wood, R.; Bandura, A. Impact of conceptions of ability on self-regulatory mechanisms and complex decision making. J. Personal. Soc. Psychol. 1989, 56, 407–415. [Google Scholar] [CrossRef]
- Chen, G.; Gully, S.M.; Eden, D. Validation of a new general self-efficacy scale. Organ. Res. Methods 2001, 4, 62–83. [Google Scholar] [CrossRef] [Green Version]
- Iskandar, T.M.; Sanusi, Z.M. Assessing the effects of self-efficacy and task complexity on internal control audit judgment. Asian Acad. Manag. J. Account. Financ. 2011, 7, 29–52. [Google Scholar]
- Judge, T.A.; Jackson, C.L.; Shaw, J.C.; Scott, B.A.; Rich, B.L. Self-efficacy and work-related performance: The integral role of individual differences. J. Appl. Psychol. 2007, 92, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Usher, E.L.; Pajares, F. Self-efficacy for self-regulated learning: A validation study. Educ. Psychol. Meas. 2008, 68, 443–463. [Google Scholar] [CrossRef]
- Williams, J.D.; Takaku, S. Help seeking, self-efficacy, and writing performance among college students. J. Writ. Res. 2011, 3, 1–18. [Google Scholar] [CrossRef]
- McCormick, M.J. Self-efficacy and leadership effectiveness: Applying social cognitive theory to leadership. J. Leadersh. Stud. 2001, 8, 22–33. [Google Scholar] [CrossRef]
- Machida, M.; Schaubroeck, J. The role of self-efficacy beliefs in leader development. J. Leadersh. Organ. Stud. 2011, 18, 459–468. [Google Scholar] [CrossRef]
- Ng, K.Y.; Ang, S.; Chan, K.Y. Personality and leader effectiveness: A moderated mediation model of leadership self-efficacy, job demands, and job autonomy. J. Appl. Psychol. 2008, 93, 733. [Google Scholar] [CrossRef] [Green Version]
- Carleton, E.L.; Barling, J.; Trivisonno, M. Leaders’ trait mindfulness and transformational leadership: The mediating roles of leaders’ positive affect and leadership self-efficacy. Can. J. Behav. Sci. Rev. Can. Sci. Comport. 2018, 50, 185. [Google Scholar] [CrossRef]
- Caldwell, C.; Hayes, L.A. Self-efficacy and self-awareness: Moral insights to increased leader effectiveness. J. Manag. Dev. 2016, 35, 1163–1173. [Google Scholar] [CrossRef]
- Liu, J.; Siu, O.L.; Shi, K. Transformational leadership and employee well-being: The mediating role of trust in the leader and self-efficacy. Appl. Psychol. 2010, 59, 454–479. [Google Scholar] [CrossRef]
- Newman, A.; Obschonka, M.; Schwarz, S.; Cohen, M.; Nielsen, I. Entrepreneurial self-efficacy: A systematic review of the literature on its theoretical foundations, measurement, antecedents, and outcomes, and an agenda for future research. J. Vocat. Behav. 2019, 110, 403–419. [Google Scholar] [CrossRef]
- Murphy, S.E.; Johnson, S.K. Leadership and leader developmental self-efficacy: Their role in enhancing leader development efforts. New Dir. Stud. Leadersh. 2016, 149, 73–84. [Google Scholar] [CrossRef]
- Lin, C.P.; Liu, C.M.; Joe, S.W.; Chen, K.J.; Tsai, C.C. Modelling leadership and team performance: The moderation of politics and leadership self-efficacy. Total Qual. Manag. Bus. Excell. 2020, 1–19. [Google Scholar] [CrossRef]
- Justwan, F.; Bakker, R.; Berejikian, J.D. Measuring social trust and trusting the measure. Soc. Sci. J. 2018, 55, 149–159. [Google Scholar] [CrossRef]
- Rathbun, B. Before hegemony: Generalized trust and the creation and design of international security organizations. Int. Organ. 2011, 65, 243–273. [Google Scholar] [CrossRef] [Green Version]
- Crepaz, M. Trust beyond Borders. Immigration, the Welfare State, and Identity in Modern Societies; University of Michigan Press: Ann Arbor, MI, USA, 2008. [Google Scholar]
- Binning, K.R. It’s us against the world: How distrust in Americans versus people-in-general shapes competitive foreign policy preferences. Political Psychol. 2007, 28, 777–799. [Google Scholar] [CrossRef]
- Bayram, A.B. Generalized trust and the moral basis of public support for foreign development aid. Foreign Policy Anal. 2016, 13, 133–153. [Google Scholar]
- Etxeberria, I.; Etxebarria, I.; Urdaneta, E. Subjective well-being among the oldest old: The role of personality traits. Personal. Individ. Differ. 2019, 146, 209–216. [Google Scholar] [CrossRef]
- Sønderskov, K.M. Does generalized social trust lead to associational membership? Unravelling a bowl of well-tossed spaghetti. Eur. Sociol. Rev. 2011, 27, 419–434. [Google Scholar] [CrossRef]
- Day, J.K.; Settersten, R.A., Jr. Less trusting and connected? Social trust and social integration among young adults during the recession. Adv. Life Course Res. 2018, 37, 57–68. [Google Scholar] [CrossRef]
- Frison, E.; Eggermont, S. The impact of daily stress on adolescents’ depressed mood: The role of social support seeking through Facebook. Comput. Hum. Behav. 2015, 44, 315–325. [Google Scholar] [CrossRef]
- Malhotra, N.K.; McCort, J.D. A cross-cultural comparison of behavioral intention models-Theoretical consideration and an empirical investigation. Int. Mark. Rev. 2001, 18, 235–269. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; The Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis: A Global Perspective; Pearson: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef] [PubMed]
- Preacher, K.J.; Rucker, D.D.; Hayes, A.F. Addressing moderated mediation hypotheses: Theory, methods, and prescriptions. Multivar. Behav. Res. 2007, 42, 185–227. [Google Scholar] [CrossRef]
- Edwards, J.R.; Lambert, L.S. Methods for integrating moderation and mediation: A general analytical framework using moderated path analysis. Psychol. Methods 2007, 12, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Rowitz, L. Public Health Leadership: Putting Principles into Practice; Jones & Bartlett Publishers: Chicago, IL, USA, 2013. [Google Scholar]
- Bradd, P.; Travaglia, J.; Hayen, A. Leadership in allied health: A review of the literature. Asia Pac. J. Health Manag. 2017, 12, 17–24. [Google Scholar] [CrossRef] [Green Version]
- Smith, T.; Fowler-Davis, S.; Nancarrow, S.; Ariss, S.M.B.; Enderby, P. Leadership in interprofessional health and social care teams: A literature review. Leadersh. Health Serv. 2018, 31, 452–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | Item | Source |
|---|---|---|
| Leaders’ future orientation (LFO) | I spend time thinking about what our country’s future might be like | [13] |
| I think a lot about what our country will be some day | ||
| Many of us tend to daydream about the future. It also happens to me | ||
| I often think about the things I am going to do in the future | ||
| Self-efficacy (SEE) | I can always manage to solve difficult problems if I try hard enough. | [18] |
| If someone opposes me, I can find means and ways to get what I want. | ||
| It is easy for me to stick to my aims and accomplish my goals. | ||
| I am confident that I could deal efficiently with unexpected events. | ||
| Thanks to my resourcefulness, I know how to handle unforeseen situations. | ||
| I can solve most problems if I invest the necessary effort. | ||
| I can remain calm when facing difficulties because I can rely on my coping abilities. | ||
| When I am confronted with a problem, I can usually find several solutions. | ||
| If I am in a bind, I can usually think of something to do. | ||
| No matter what comes my way, I am usually able to handle it. | ||
| Perceived social support (PSS) | In a difficult situation, I can find help from my residents and colleagues. | [61] |
| I can find emotional, informational and social support that I need from my residents and colleagues. | ||
| I can express my problems with my residents, colleagues and friends | ||
| Public health investment intention (PHII) | We intend to invest more in public health programs. | [62] |
| We will regularly invest in public health for our residents | ||
| We intend to continue investment in public health for our residents |
| Variable | Frequency | Percent |
|---|---|---|
| Gender | ||
| Female | 104 | 27.3% |
| Male | 277 | 72.7% |
| Age | ||
| 30 or below | 74 | 19.4% |
| 31–40 | 223 | 58.5% |
| 41–50 | 58 | 15.2% |
| 51–60 | 26 | 6.8% |
| 61 or above | 0 | 0.0% |
| Marital status | ||
| Married | 277 | 72.7% |
| Not married | 104 | 27.3% |
| Income | ||
| Under 200 USD | 126 | 33.1% |
| 200-under 400 USD | 224 | 58.8% |
| 400-under 600 USD | 24 | 6.3% |
| 600-under 800 USD | 6 | 1.6% |
| 800 USD or above | 1 | 0.3% |
| Education | ||
| Undergraduate or below | 260 | 68.2% |
| Master | 116 | 30.4% |
| Ph.D. | 5 | 1.3% |
| Tenure (years) | ||
| Under 5 years | 35 | 9.2% |
| 5-under 10 years | 173 | 45.4% |
| 10 years or above | 173 | 45.4% |
| Variable | Mean | SD | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|---|
| 1. Leaders’ future orientation | 3.65 | 0.84 | 0.86 | |||
| 2. Self-efficacy | 3.76 | 0.73 | 0.47 ** | 0.72 | ||
| 3. Perceived social support | 3.98 | 0.79 | 0.40 ** | 0.40 ** | 0.78 | |
| 4. Public health investment intention | 3.62 | 0.87 | 0.47 ** | 0.48 ** | 0.41 ** | 0.84 |
| Constructs | Items | Loadings | CR | AVE | √AVE | Cronbach’s α |
|---|---|---|---|---|---|---|
| Leaders’ future orientation (LFO) | LFO1 | 0.86 *** | 0.92 | 0.74 | 0.86 | 0.92 |
| LFO2 | 0.82 *** | |||||
| LFO3 | 0.89 *** | |||||
| LFO4 | 0.87 *** | |||||
| Self-efficacy (SEE) | SEE1 | 0.71 *** | 0.91 | 0.52 | 0.72 | 0.91 |
| SEE2 | 0.67 *** | |||||
| SEE3 | 0.73 *** | |||||
| SEE4 | 0.72 *** | |||||
| SEE5 | 0.72 *** | |||||
| SEE6 | 0.71 *** | |||||
| SEE7 | 0.74 *** | |||||
| SEE8 | 0.72 *** | |||||
| SEE9 | 0.78 *** | |||||
| SEE10 | 0.69 *** | |||||
| Perceived social support (PSS) | PSS1 | 0.85 *** | 0.83 | 0.62 | 0.78 | 0.83 |
| PSS2 | 0.79 *** | |||||
| PSS3 | 0.71 *** | |||||
| Public health investment intention (PHII) | PHII1 | 0.84 *** | 0.88 | 0.70 | 0.84 | 0.87 |
| PHII2 | 0.90 *** | |||||
| PHII3 | 0.77 *** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Chou, T.P.; Chen, C.-P.; Bu, X. Leaders’ Future Orientation and Public Health Investment Intention: A Moderated Mediation Model of Self-Efficacy and Perceived Social Support. Int. J. Environ. Res. Public Health 2020, 17, 6922. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186922
Wang J, Chou TP, Chen C-P, Bu X. Leaders’ Future Orientation and Public Health Investment Intention: A Moderated Mediation Model of Self-Efficacy and Perceived Social Support. International Journal of Environmental Research and Public Health. 2020; 17(18):6922. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186922
Chicago/Turabian StyleWang, Jianming, Tsung Piao Chou, Chia-Pin Chen, and Xiangzhi Bu. 2020. "Leaders’ Future Orientation and Public Health Investment Intention: A Moderated Mediation Model of Self-Efficacy and Perceived Social Support" International Journal of Environmental Research and Public Health 17, no. 18: 6922. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186922