Incarceration Exposure and Barriers to Prenatal Care in the United States: Findings from the Pregnancy Risk Assessment Monitoring System


Abstract
:1. Introduction
- Do women exposed to incarceration during pregnancy face more barriers to prenatal care than women without incarceration exposure?
- Are there specific barriers to which incarceration exposed women are particularly prone?
2. Materials and Methods
2.1. Dependent Variable
2.2. Independent Variable
2.3. Control Variables
2.4. Analytic Approach
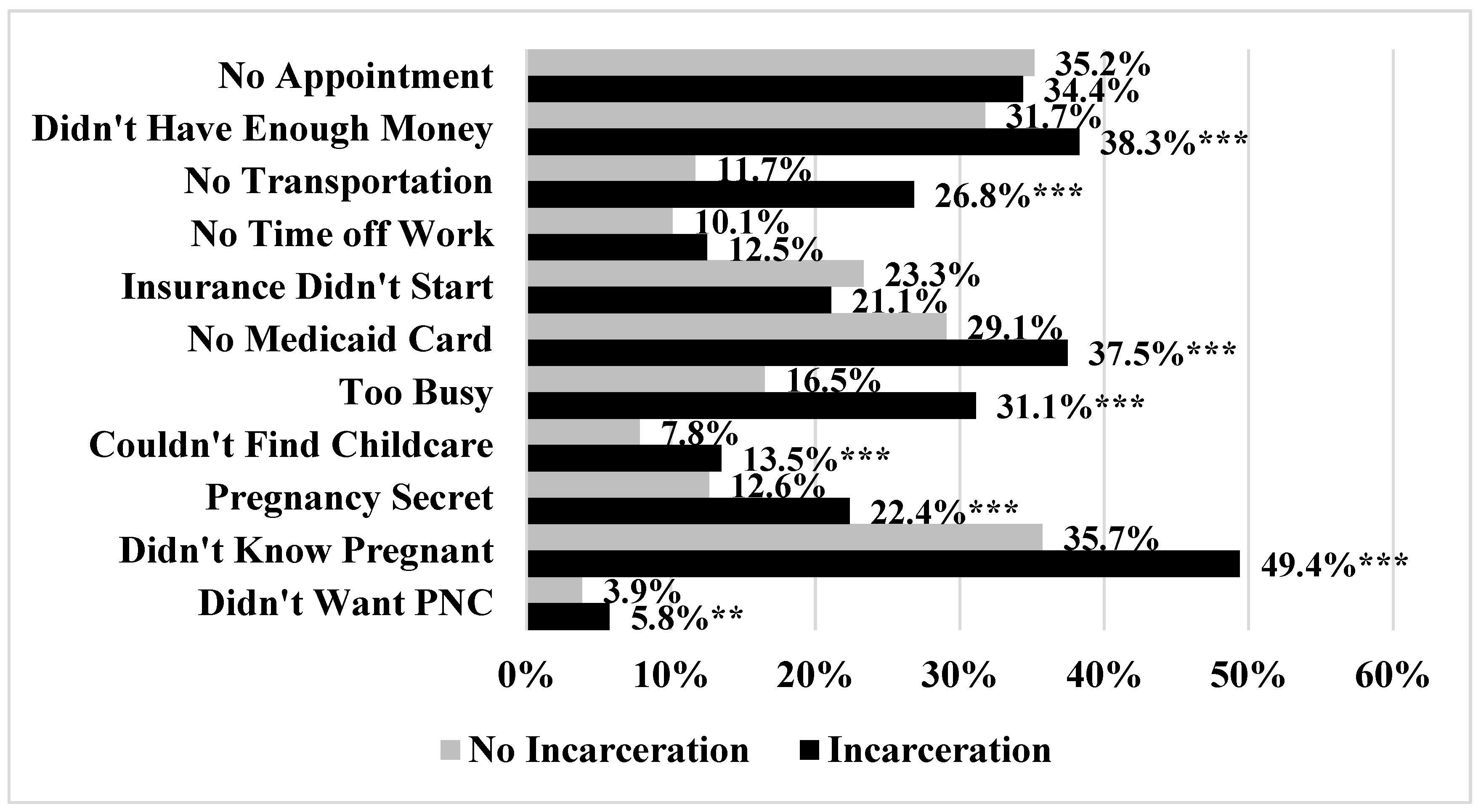
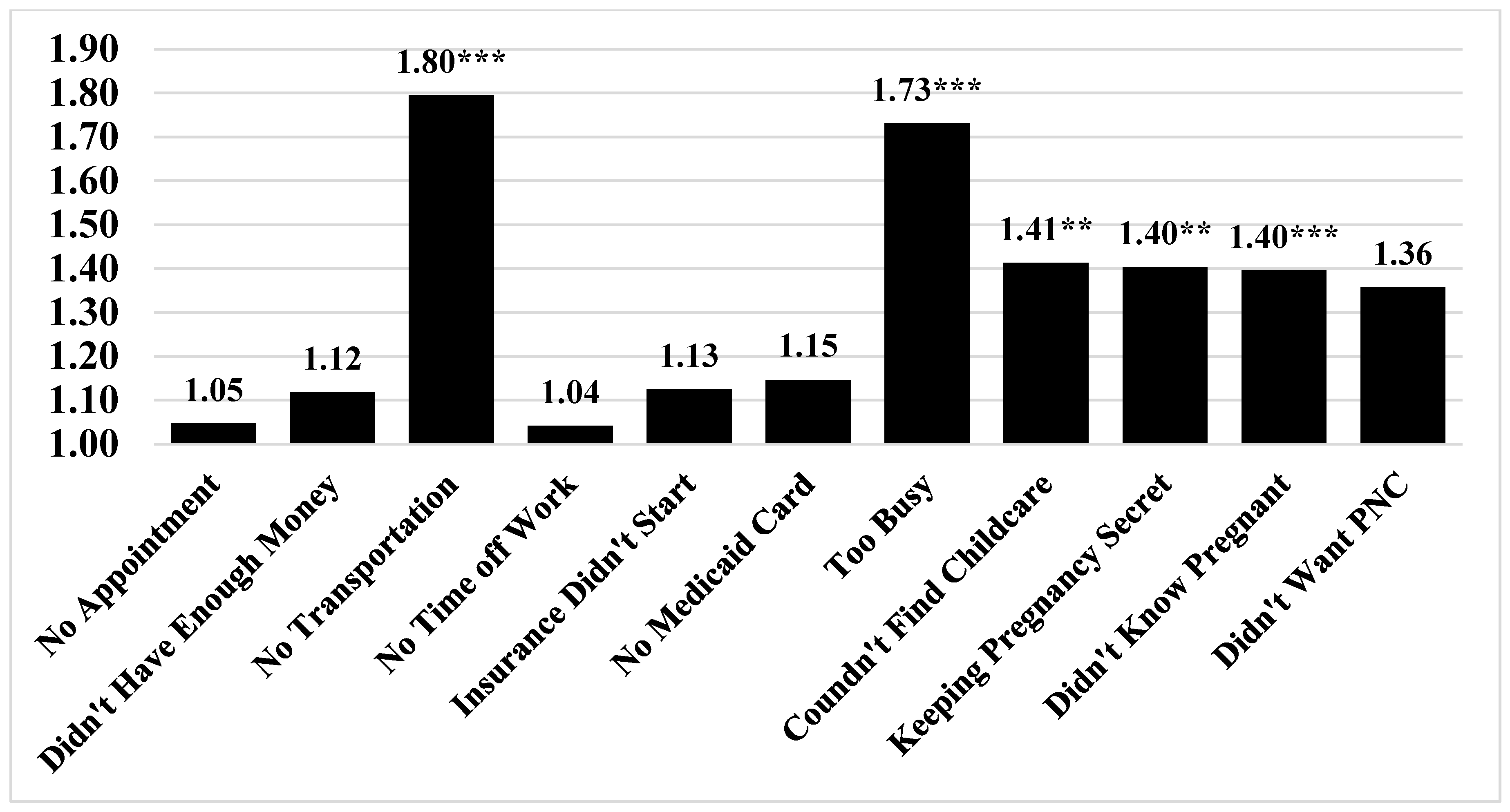
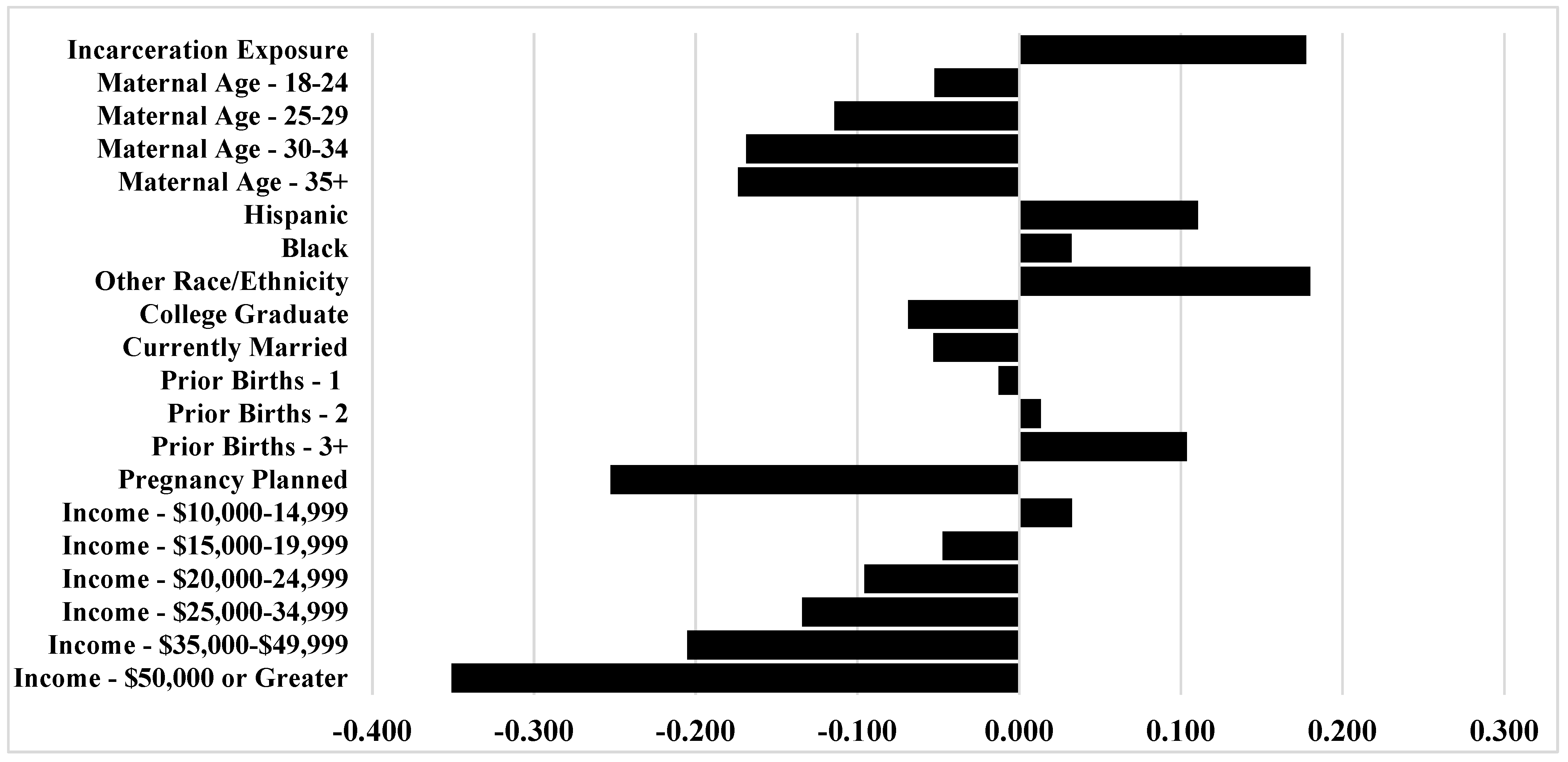
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| State |
|---|
| Alaska |
| Alabama |
| Arkansas |
| Colorado |
| Delaware |
| Georgia |
| Hawaii |
| Illinois |
| Louisiana |
| Massachusetts |
| Maryland |
| Maine |
| Michigan |
| Minnesota |
| Montana |
| Mississippi |
| Nebraska |
| New Hampshire |
| New Jersey |
| New Mexico |
| New York |
| New York City |
| Ohio |
| Oklahoma |
| Oregon |
| Pennsylvania |
| Rhode Island |
| Tennessee |
| Texas |
| Utah |
| Virginia |
| Washington |
| Wisconsin |
| West Virginia |
| Wyoming |
Appendix B
| I couldn’t get an appointment when I wanted |
| I didn’t have enough money or insurance to pay for my visits |
| I had no transportation to get to the clinic or doctor’s office |
| I couldn’t take time off work or school |
| The doctor or my health plan would not start care as early as I wanted |
| I didn’t have my Medicaid card |
| I had no one to take care of my children |
| I had too many other things going on |
| I didn’t want anyone to know I was pregnant |
| I didn’t know I was pregnant |
| I didn’t want prenatal care |
Appendix C

References
- Bruns, A. Partner Incarceration and Financial Support from Kin. J. Fam. Issues 2020, 41, 2112–2135. [Google Scholar] [CrossRef]
- Harding, D.J.; Wyse, J.J.B.; Dobson, C.; Morenoff, J.D. Making Ends Meet After Prison. J. Policy Anal. Manag. 2014, 33, 440–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massoglia, M.; Remster, B. Linkages Between Incarceration and Health. Public Health Rep. 2019, 134, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Provencher, A.; Conway, J.M. Health effects of family member incarceration in the United States: A meta-analysis and cost study. Child. Youth Serv. Rev. 2019, 103, 87–99. [Google Scholar] [CrossRef]
- Wildeman, C.; Wang, E.A. Mass incarceration, public health, and widening inequality in the USA. Lancet 2017, 389, 1464–1474. [Google Scholar] [CrossRef]
- Wildeman, C.; Goldman, A.W.; Lee, H. Health Consequences of Family Member Incarceration for Adults in the Household. Public Health Rep. 2019, 134, 15–21. [Google Scholar] [CrossRef] [Green Version]
- Bell, J.F.; Zimmerman, F.J.; Cawthon, M.L.; Huebner, C.E.; Ward, D.H.; Schroeder, C.A. Jail incarceration and birth outcomes. J. Hered. 2004, 81, 630–644. [Google Scholar] [CrossRef] [Green Version]
- Jahn, J.L.; Chen, J.T.; Agénor, M.; Krieger, N. County-level jail incarceration and preterm birth among non-Hispanic Black and white U.S. women, 1999–2015. Soc. Sci. Med. 2020, 250, 112856. [Google Scholar] [CrossRef]
- Ramirez, A.C.; Liauw, J.; Costescu, D.; Holder, L.; Lu, H.; Kouyoumdjian, F.G. Infant and Maternal Outcomes for Women Who Experience Imprisonment in Ontario, Canada: A Retrospective Cohort Study. J. Obs. Gynaecol. Can. 2020, 42, 462–472.e2. [Google Scholar] [CrossRef]
- Shlafer, R.J.; Hardeman, R.R.; Carlson, E.A. Reproductive justice for incarcerated mothers and advocacy for their infants and young children. Child. Adolesc. Soc. Work. J. 2019, 40, 725–741. [Google Scholar] [CrossRef] [Green Version]
- Testa, A.; Jackson, D.B. Incarceration Exposure During Pregnancy and Infant Health: Moderation by Public Assistance. J. Pediatr. 2020. Available online: https://0-www-sciencedirect-com.brum.beds.ac.uk/science/article/abs/pii/S0022347620307587 (accessed on 4 September 2020). [CrossRef] [PubMed]
- Testa, A.; Jackson, D.B.; Vaughn, M.G.; Bello, J.K. Incarceration as a unique social stressor during pregnancy: Implications for maternal and newborn health. Soc. Sci. Med. 2020, 246, 112777. [Google Scholar] [CrossRef] [PubMed]
- Wildeman, C. Imprisonment and Infant Mortality. Soc. Probl. 2012, 59, 228–257. [Google Scholar] [CrossRef] [Green Version]
- Dumont, D.M.; Wildeman, C.; Lee, H.; Gjelsvik, A.; Valera, P.; Clarke, J.G. Incarceration, maternal hardship, and perinatal health behaviors. Matern. Child. Health J. 2014, 18, 2179–2187. [Google Scholar] [CrossRef] [PubMed]
- Alexander, G.R.; Korenbrot, C.C. The Role of Prenatal Care in Preventing Low Birth Weight. Future Child. 1995, 5, 103. [Google Scholar] [CrossRef]
- Cunningham, S.D.; Lewis, J.B.; Shebl, F.M.; Boyd, L.M.; Robinson, M.A.; Grilo, S.A.; Lewis, S.M.; Pruett, A.L.; Ickovics, J.R. Group Prenatal Care Reduces Risk of Preterm Birth and Low Birth Weight: A Matched Cohort Study. J. Women’s Health 2019, 28, 17–22. [Google Scholar] [CrossRef]
- Partridge, S.; Balayla, J.; Holcroft, C.A.; Abenhaim, H.A. Inadequate Prenatal Care Utilization and Risks of Infant Mortality and Poor Birth Outcome: A Retrospective Analysis of 28,729,765 U.S. Deliveries over 8 Years. Am. J. Perinatol. 2012, 29, 787–794. [Google Scholar] [CrossRef]
- Poma, P.A. Effect of prenatal care on infant mortality rates according to birth-death certificate files. J. Natl. Med. Assoc. 1999, 91, 515–520. [Google Scholar]
- American Academy of Pediatrics. Guidelines for Perinatal Care, 7th ed.; American Academy of Pediatrics: Washington, DC, USA, 2012. [Google Scholar]
- World Health Organization. WHO Recommendations on Health Promotion Interventions for Maternal and Newborn Health 2015; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- U.S. Department of Health and Human Services. Healthy People 2020; Office of Disease Prevention and Health Promotion: Washington, DC, USA, 2015.
- Gadson, A.; Akpovi, E.; Mehta, P.K. Exploring the social determinants of racial/ethnic disparities in prenatal care utilization and maternal outcome. Semin. Perinatol. 2017, 41, 308–317. [Google Scholar] [CrossRef]
- Testa, A.; Jackson, D.B. Incarceration exposure and maternal food insecurity during pregnancy: Findings from the Pregnancy Risk Assessment Monitoring System (PRAMS), 2004–2015. Mat. Child Health J. 2020, 24, 54–61. [Google Scholar] [CrossRef]
- Hagan, J.; Dinovitzer, R. Collateral Consequences of Imprisonment for Children, Communities, and Prisoners. Crime Justice 1999, 26, 121–162. [Google Scholar] [CrossRef]
- Bruns, A. The third shift: Multiple job holding and the incarceration of women’s partners. Soc. Sci. Res. 2019, 80, 202–215. [Google Scholar] [CrossRef] [PubMed]
- Sugie, N.F. Punishment and Welfare: Paternal Incarceration and Families’ Receipt of Public Assistance. Soc. Forces 2012, 90, 1403–1427. [Google Scholar] [CrossRef] [Green Version]
- Turanovic, J.J.; Rodriguez, N.; Pratt, T.C. The collateral consequences of incarceration revisited: A qualitative analysis of the effects on caregivers of children of incarcerated parents. Criminology 2012, 50, 913–959. [Google Scholar] [CrossRef]
- Geller, A.; Garfinkel, I.; Cooper, C.E.; Mincy, R.B. Parental Incarceration and Child Well-Being: Implications For Urban Families. Soc. Sci. Q. 2009, 90, 1186–1202. [Google Scholar] [CrossRef]
- Turney, K.; Schnittker, J.; Wildeman, C. Those They Leave Behind: Paternal Incarceration and Maternal Instrumental Support. J. Marriag. Fam. 2012, 74, 1149–1165. [Google Scholar] [CrossRef]
- Wakeman, S.E.; McKinney, M.E.; Rich, J.D. Filling the Gap: The Importance of Medicaid Continuity for Former Inmates. J. Gen. Intern. Med. 2009, 24, 860–862. [Google Scholar] [CrossRef] [Green Version]
- Winkelman, T.N.; Choi, H.; Davis, M.M. The Affordable Care Act, Insurance Coverage, and Health Care Utilization of Previously Incarcerated Young Men: 2008–2015. Am. J. Public Health 2017, 107, 807–811. [Google Scholar] [CrossRef]
- Widdowson, A.O.; Fisher, B.W. Mass Incarceration and Subsequent Preventive Health Care: Mechanisms and Racial/Ethnic Disparities. Am. J. Public Health 2020, 110, 145–151. [Google Scholar] [CrossRef]
- Turney, K.; Schneider, D. Incarceration and Household Asset Ownership. Demography 2016, 53, 2075–2103. [Google Scholar] [CrossRef]
- Bohmert, M.N. Access to Transportation and Outcomes for Women on Probation and Parole; Michigan State University: East Lansing, MI, USA, 2014. [Google Scholar]
- Wyse, J.J.B.; Harding, D.J.; Morenoff, J.D. Romantic Relationships and Criminal Desistance: Pathways and Processes. Sociol. Forum 2014, 29, 365–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heaman, M.; Sword, W.; Elliott, L.; Moffatt, M.; Helewa, M.; Morris, H.; Gregory, P.A.; Tjaden, L.; Cook, C. Barriers and facilitators related to use of prenatal care by inner-city women: Perceptions of health care providers. BMC Pregnancy Childbirth 2015, 15, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, J.L.; Primas, P.J.; Coe, M.K. Factors that Prevent Women of Low Socioeconomic Status from Seeking Prenatal Care. J. Am. Acad. Nurse Pr. 1994, 6, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Porter, L.C. Being “on Point”: Exploring the Stress-related Experiences of Incarceration. Soc. Ment. Health 2018, 9, 1–17. [Google Scholar] [CrossRef]
- Brayne, S. Surveillance and System Avoidance. Am. Soc. Rev. 2014, 79, 367–391. [Google Scholar] [CrossRef]
- Comfort, M.; Grinstead, O.; McCartney, K.; Bourgois, P.; Knight, K. “You can’t do nothing in this damn place”: Sex and intimacy among couples with an incarcerated male partner. J. Sex. Res. 2005, 42, 3–12. [Google Scholar] [CrossRef]
- Siennick, S.E.; Stewart, E.A.; Staff, J. Explaining the association between incarceration and divorce. Criminology 2014, 52, 371–398. [Google Scholar] [CrossRef] [Green Version]
- Turney, K. Liminal Men: Incarceration and Relationship Dissolution. Soc. Probl. 2015, 62, 499–528. [Google Scholar] [CrossRef]
- Hamilton, B.E.; Martin, J.A.; Osterman, M.J.; Rossen, L.M. Births: Provisional Data for 2018; National Center for Health Statistics: Hyattsville, MD, USA, 2019.
- Shulman, H.B.; D’Angelo, D.V.; Harrison, L.; Smith, R.A.; Warner, L. The Pregnancy Risk Assessment Monitoring System (PRAMS): Overview of Design and Methodology. Am. J. Public Health 2018, 108, 1305–1313. [Google Scholar] [CrossRef]
- Braveman, P. Barriers to timely prenatal care among women with insurance: The importance of prepregnancy factors*1. Obs. Gynecol. 2000, 95, 874–880. [Google Scholar] [CrossRef]
- Campbell, J.D.; Stanford, J.B.; Ewigman, B. The social pregnancy interaction model: Conceptualizing cognitive, social and cultural barriers to prenatal care. Appl. Behav. Sci. Rev. 1996, 4, 81–97. [Google Scholar] [CrossRef]
- Phillippi, J.C. Women’s perceptions of access to prenatal care in the United States: A literature review. J. Midwif. Women Health 2009, 54, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Carson, E.A. Prisoners in 2018; United States Department of Justice: Washington, DC, USA, 2020.
- Zeng, Z. Jail Inmates in 2018; United States Department of Justice: Washington, DC, USA, 2020.
- Melnikow, J.; Paliescheskey, M.; Stewart, G.K. Effect of a transportation incentive on compliance with the first prenatal appointment: A randomized trial. Obs. Gynecol. 1997, 89, 1023–1027. [Google Scholar] [CrossRef]
- Shlafer, R.J.; Duwe, G.; Hindt, L. Parents in Prison and Their Minor Children: Comparisons between State and National Estimates. Prison. J. 2019, 99, 310–328. [Google Scholar] [CrossRef]
- Bloom, K.C.; Bednarzyk, M.S.; Devitt, D.L.; Renault, R.A.; Teaman, V.; Van Loock, D.M. Barriers to Prenatal Care for Homeless Pregnant Women. J. Obs. Gynecol. Neonatal Nurs. 2004, 33, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Peahl, A.F.; Smith, R.D.; Moniz, M.H. Prenatal care redesign: Creating flexible maternity care models through virtual care. Am. J. Obs. Gynecol. 2020, 223, 1–389. [Google Scholar] [CrossRef] [PubMed]
- Dubay, L.; Hill, I.; Garrett, B.; Blavin, F.; Johnston, E.; Howell, E.; Morgan, J.; Courtot, B.; Benatar, S.; Cross-Barnet, C. Improving Birth Outcomes and Lowering Costs for Women on Medicaid: Impacts of ‘Strong Start for Mothers and Newborns’. Health Aff. 2020, 39, 1042–1050. [Google Scholar] [CrossRef]
- Lopoo, L.M.; Western, B. Incarceration and the Formation and Stability of Marital Unions. J. Marriage Fam. 2005, 67, 721–734. [Google Scholar] [CrossRef]
- Rengifo, A.F.; DeWitt, S.E. Correction to: Incarceration and Personal Networks: Unpacking Measures and Meanings of Tie Strength. J. Quant. Criminol. 2019, 35, 433. [Google Scholar] [CrossRef] [Green Version]
- Hadden, K.B.; Puglisi, L.; Prince, L.; Aminawung, J.A.; Shavit, S.; Pflaum, D.; Calderon, J.; Wang, E.A.; Zaller, N. Health Literacy Among a Formerly Incarcerated Population Using Data from the Transitions Clinic Network. J. Hered. 2018, 95, 547–555. [Google Scholar] [CrossRef]
- Ramaswamy, M.; Kelly, P.J. “The Vagina is a Very Tricky Little Thing Down There”: Cervical Health Literacy among Incarcerated Women. J. Health Care Poor Underserved 2015, 26, 1265–1285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramaswamy, M.; Lee, J.; Wickliffe, J.; Allison, M.; Emerson, A.; Kelly, P.J. Impact of a brief intervention on cervical health literacy: A waitlist control study with jailed women. Prev. Med. Rep. 2017, 6, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.D.; Mobley, S.C.; Hudgins, J.L.; Sutherland, D.E.; Inglett, S.; Ange, B.L. Conditions and Dynamics That Impact Maternal Health Literacy among High Risk Prenatal-Interconceptional Women. Int. J. Environ. Res. Public Health 2018, 15, 1383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epstein, B.; Grant, T.; Schiff, M.; Kasehagen, L. Does Rural Residence Affect Access to Prenatal Care in Oregon? J. Rural. Health 2009, 25, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Olds, D.L.; Kitzman, H. Review of Research on Home Visiting for Pregnant Women and Parents of Young Children. Future Child. 1993, 3, 53. [Google Scholar] [CrossRef] [Green Version]
- Poland, M.L.; Giblin, P.T.; Waller, J.B., Jr.; Hankin, J. Effects of a home visiting program on prenatal care and birthweight: A case comparison study. J. Commun. Health 1992, 17, 221–229. [Google Scholar] [CrossRef]
- Martin, S.L.; Rieger, R.H.; Kupper, L.L.; Meyer, R.E.; Qaqish, B.F. The effect of incarceration during pregnancy on birth outcomes. Public Health Rep. 1997, 112, 340–346. [Google Scholar]
- Dumont, D.M.; Parker, D.R.; Viner-Brown, S.; Clarke, J.G. Incarceration and perinatal smoking: A missed public health opportunity. J. Epidemiol. Commun. Health 2015, 69, 648–653. [Google Scholar] [CrossRef]
- Massoglia, M. Incarceration as Exposure: The Prison, Infectious Disease, and Other Stress-Related Illnesses. J. Health Soc. Behav. 2008, 49, 56–71. [Google Scholar] [CrossRef]
- Schnittker, J.; John, A. Enduring Stigma: The Long-Term Effects of Incarceration on Health. J. Health Soc. Behav. 2007, 48, 115–130. [Google Scholar] [CrossRef]
- Roberts, S.C.M.; Pies, C. Complex Calculations: How Drug Use During Pregnancy Becomes a Barrier to Prenatal Care. Matern. Child. Health J. 2010, 15, 333–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milligan, R.; Wingrove, B.K.; Richards, L.; Rodan, M.; Monroe-Lord, L.; Jackson, V.; Hatcher, B.; Harris, C.; Henderson, C.; Johnson, A.A. Perceptions about prenatal care: Views of urban vulnerable groups. BMC Public Health 2002, 2, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- York, R.; Williams, P.; Munro, B.H. Maternal Factors That Influence Inadequate Prenatal Care. Public Heal. Nurs. 1993, 10, 241–244. [Google Scholar] [CrossRef] [PubMed]


| Variables | No Incarceration (N = 185,406) | Incarceration (N = 9194) | p-Value |
|---|---|---|---|
| Total Barriers | 0.363 | 0.915 | <0.001 |
| Maternal Age | |||
| 17 or Younger | 2.3% | 4.7% | <0.001 |
| 18–24 | 26.2% | 50.9% | <0.001 |
| 25–29 | 29.4% | 26.0% | <0.001 |
| 30–34 | 26.9% | 12.7% | <0.001 |
| 35+ | 15.2% | 5.7% | <0.001 |
| Maternal Race/Ethnicity | |||
| White | 59.0% | 48.4% | <0.001 |
| Hispanic | 13.3% | 27.8% | <0.001 |
| Black | 19.8% | 17.8% | 0.027 |
| Other Race/Ethnicity | 7.9% | 6.0% | <0.001 |
| College Graduate | 32.8% | 5.7% | <0.001 |
| Currently Married | 62.0% | 21.0% | <0.001 |
| Number of Prior Births | |||
| 0 | 40.3% | 41.0% | 0.432 |
| 1 | 32.5% | 27.9% | <0.001 |
| 2 | 16.2% | 16.9% | 0.379 |
| 3+ | 10.9% | 14.1% | <0.001 |
| Pregnancy Planned | 50.7% | 26.5% | <0.001 |
| Income Levels | |||
| Less than $10,000 | 21.7% | 56.1% | <0.001 |
| $10,000–$14,999 | 5.5% | 9.3% | <0.001 |
| $15,000–$19,999 | 3.6% | 4.7% | 0.016 |
| $20,000–$24,999 | 10.4% | 13.2% | <0.001 |
| $25,000–$34,999 | 10.9% | 8.0% | <0.001 |
| $35,000–$49,999 | 10.5% | 4.1% | <0.001 |
| $50,000 or Greater | 37.4% | 4.7% | <0.001 |
| Variables | Model 1 | Model 2 | ||
|---|---|---|---|---|
| IRR | 95% CI | IRR | 95% CI | |
| Incarceration Exposure | 2.484 *** | (2.267, 2.721) | 1.558 *** | (1.416, 1.714) |
| Maternal Age | ||||
| 17 or Younger (Reference) | - | - | - | - |
| 18–24 | 0.904 † | (0.804, 1.016) | ||
| 25–29 | 0.788 *** | (0.695, 0.893) | ||
| 30–34 | 0.695 *** | (0.608, 0.795) | ||
| 35+ | 0.687 *** | (0.595, 0.794) | ||
| Maternal Race/Ethnicity | ||||
| White (Reference) | - | - | - | - |
| Hispanic | 1.191 *** | (1.108, 1.281) | ||
| Black | 1.103 ** | (1.032, 1.180) | ||
| Other Race/Ethnicity | 1.552 *** | (1.432, 1.683) | ||
| College Graduate | 0.867 *** | (0.806, 0.932) | ||
| Currently Married | 0.848 *** | (0.797, 0.901) | ||
| Number of Prior Births | ||||
| 0 (Reference) | - | - | - | - |
| 1 | 0.949 † | (0.896, 1.006) | ||
| 2 | 1.017 | (0.947, 1.092) | ||
| 3+ | 1.263 *** | (1.153, 1.384) | ||
| Pregnancy Planned | 0.523 *** | (0.495, 0.552) | ||
| Income Levels | ||||
| Less than $10,000 (Reference) | - | - | - | - |
| $10,000–$14,999 | 1.020 | (0.923, 1.129) | ||
| $15,000–$19,999 | 0.897 † | (0.796, 1.012) | ||
| $20,000–$24,999 | 0.837 *** | (0.770, 0.910) | ||
| $25,000–$34,999 | 0.733 *** | (0.672, 0.799) | ||
| $35,000–$49,999 | 0.611 *** | (0.553, 0.676) | ||
| $50,000 or Greater | 0.324 *** | (0.296, 0.356) | ||
| Constant | 0.535 *** | (0.468, 0.612) | 1.093 | (0.910, 1.313) |
| State Dummy Variables | Yes | Yes | ||
| Year Dummy Variables | Yes | Yes | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Testa, A.; Jackson, D.B. Incarceration Exposure and Barriers to Prenatal Care in the United States: Findings from the Pregnancy Risk Assessment Monitoring System. Int. J. Environ. Res. Public Health 2020, 17, 7331. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197331
Testa A, Jackson DB. Incarceration Exposure and Barriers to Prenatal Care in the United States: Findings from the Pregnancy Risk Assessment Monitoring System. International Journal of Environmental Research and Public Health. 2020; 17(19):7331. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197331
Chicago/Turabian StyleTesta, Alexander, and Dylan B. Jackson. 2020. "Incarceration Exposure and Barriers to Prenatal Care in the United States: Findings from the Pregnancy Risk Assessment Monitoring System" International Journal of Environmental Research and Public Health 17, no. 19: 7331. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17197331