Assessing the Distribution of Elderly Requiring Care: A Case Study on the Residents in Barcelona and the Impact of COVID-19


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data and Variables
2.2. Methodology
3. Results
3.1. Distribution of the Demand for Elderly Care Services in Barcelona Using CM
- Population: The population of neighborhoods (see Figure S1a) has a positively skewed distribution, with a mean of 22,203 and a median of 20,487. The population has a wide range, ranging from 610 in el Clot (42) to 58,180 in la Nova Esquerra de l’Eixample (09). Looking at the map, it is clear that the distribution is not randomly distributed geographically. The bulk of the population is centered in the center of the city, in the Eixample neighborhoods and the neighborhoods immediately to the north of it. Apart from this central cluster, Sant Andreu, in the top right, has the second-highest population of any of the neighborhoods. The neighborhoods in the top of the map near the mountains and bottom of the map near the coast are less populated on average.
- Elderly Population: The total elderly population, intuitively, very closely resembles the distribution of the population (see Figure S1b,c). The mean elderly population is 4782.63 per neighborhood, ranging from 90 people in el Clot (42) to 13,413 in la Nova Esquerra de l’Eixample (09). To account for the difference in demand between the neighborhoods, the darker shaded neighborhoods should typically be allocated more resources than lighter shaded neighborhoods to allow them to service their larger elderly population. However, the number of resources must be adjusted to account for the RFID, elderly living alone, and disabled elderly population. The map of the relative percentage of elderly per neighborhood sheds some light on how the distribution of the elderly differs across different neighborhoods. The general geographic trend is that the neighborhoods tend to have a higher percentage of elderly as one moves up from the coast to the mountains.
- RFID: The RFID index (see Figure S1.d) has a wide range, where the most impoverished neighborhood is la Trinitat Nova (53), with an RFID index of 34.70, indicating that the average household in that neighborhood has 34.70% of the average disposable income. The wealthiest neighborhood is Pedralbes (21), with an RFID index of 251.7, indicating that the average household in that neighborhood has 2.5 times more disposable income than the mean. Like many income variables, it is very positively skewed, with the high-income area pulling the average up; 72.6% of the neighborhoods lie below the average, with only 27.3% lying above the average. This variable can be used as a scaling factor, where neighborhoods that have above the mean RFID receive fewer relative resources for their population. The map shows that the city’s income seems to be correlated with geographic location. The neighborhoods in the Eixample, Sarrià, Gràcia, and Les Corts tend to have RFID scores above 100. The five neighborhoods in the top of the map, Trinitat Nova, Torre Baró, Ciutat Meridiana, Vallbona, and la Trinitat Vella, and the neighborhood at the bottom, la Marina del Prat Vermell, have the lowest RFID scores, all below 50. Then, the majority of the neighborhoods on the right half of the map and the bottom left of the map have RFID indexes between 50 and 100.
- Elderly Population Living Alone: The elderly living alone map (see Figure S1e) correlates with the elderly population map; as the number of elderly increases, those that live alone will also increase. Therefore, to extract new information, it would be interesting to analyze the relative distribution of elderly people living alone (Figure S1f). The percentage of elderly living alone has a reasonably normal distribution with a mean of 25.07%. The variable ranges from 13.56% in Vallbona (56) to 34.34% in Sant Pere, Santa Caterina i la Ribera (04). There is not a clear geographic concentration or correlation like in the previous charts; however, we can still see some minor patterns. Ciutadella district neighborhoods have a large percentage of elderly people living alone. Like the RFID, this variable can be used to adjust the base demand. Neighborhoods with more significant percentages of elderly people living alone should receive a greater share of resources than a neighborhood of a similar population with a lower percentage of elderly people living alone, all other things held equal.
- Disabled Elderly Population: The base elderly disabled population stat is highly correlated with the elderly population (Figure S1g,h); therefore, we look at the percentage of elderly that are disabled in the neighborhood. The percentage of disabled, again, has a relatively normal distribution, with a mean of 20.41%. The variable ranges from 12.94% in les Tres Torres (24) to 33.80% in la Marina del Prat Vermell (12). The geographical pattern resembles the RFID pattern, but high income is negatively correlated with high disability rates. Once again, this variable can be used to scale the base demand for homecare, where neighborhoods with larger percentages of disabled elderly people should receive a greater share of resources than a neighborhood with a similar population and a lower percentage of disabled elderly people, all other things held equal.
3.2. Clustering of Barcelona’s Neighborhoods
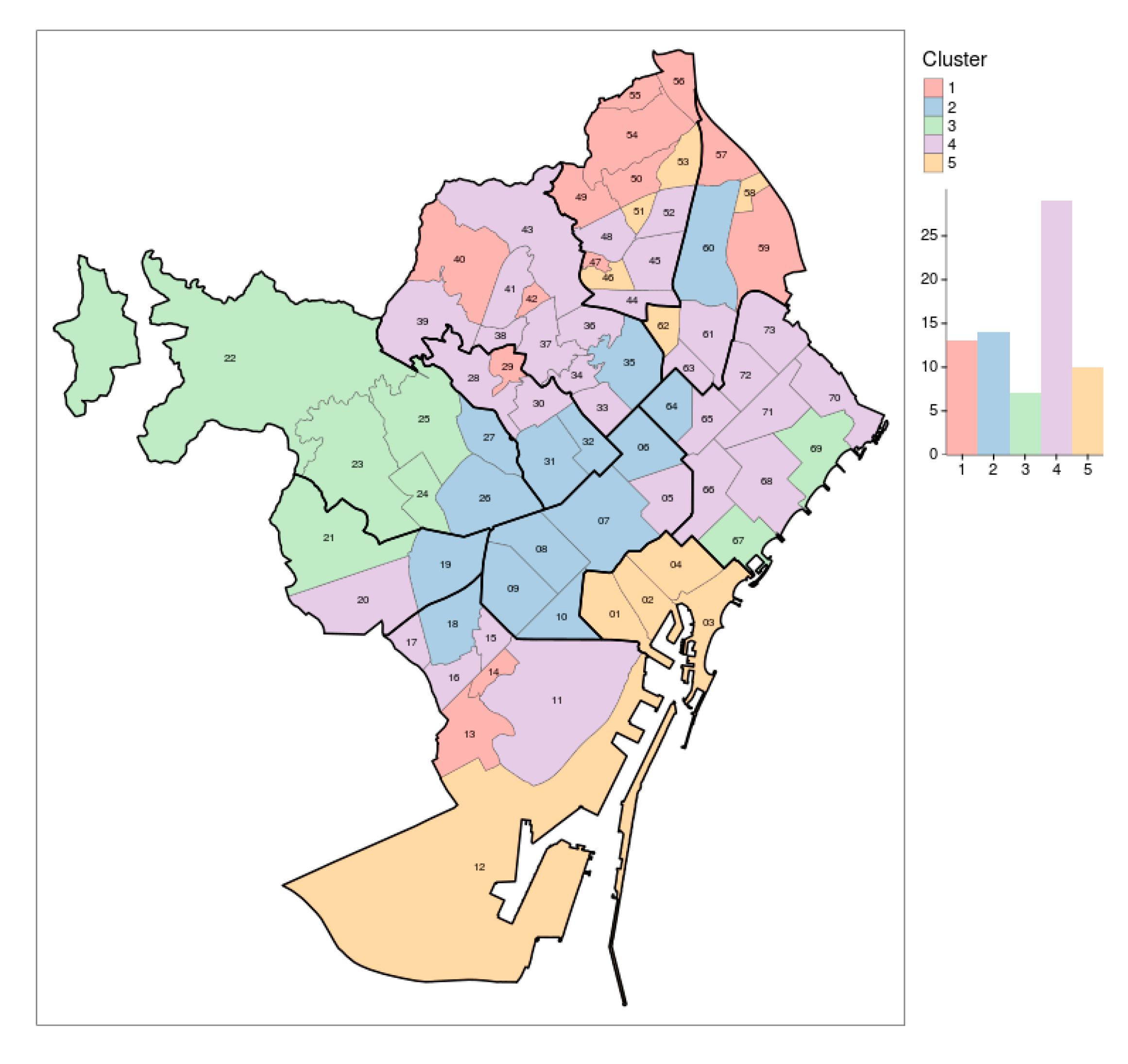
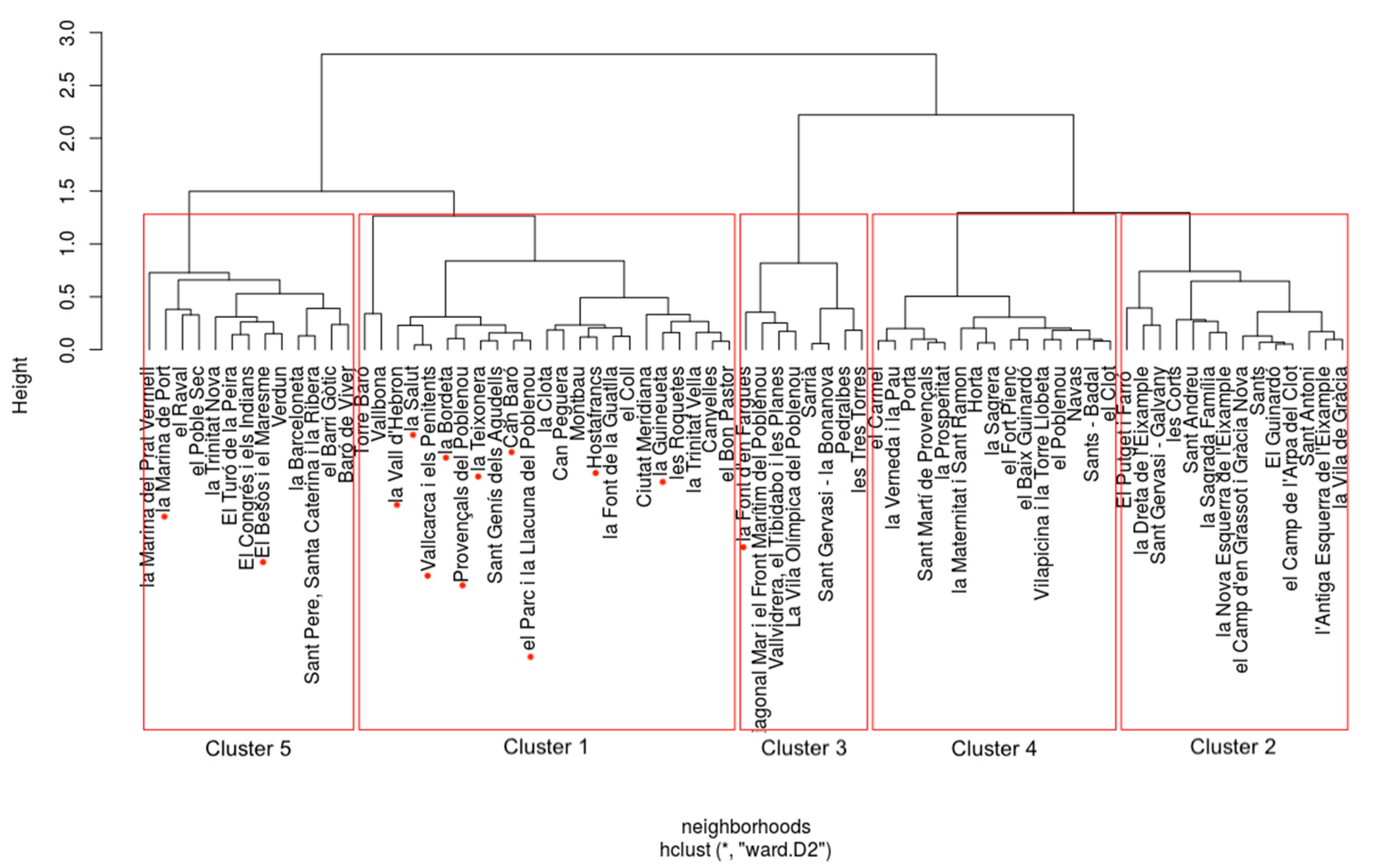
- Cluster 1: Forgotten Neighborhoods. This cluster represents Barcelona “Forgotten” neighborhoods. Cluster 1, along with Cluster 4, is home to Barcelona’s most vulnerable elderly population. These small neighborhoods on the outskirts of the city have a low population, the lowest levels of disposable income, and high levels of disabled elderly. However, they, fortunately, have a lower percentage of elderly people living alone. It is imperative that despite the peripheral location and low population, these neighborhoods receive adequate resources. The low income and high disability indicate that neighborhoods in this cluster require a more substantial amount of resources per capita than Clusters 2, 3, and 4.
- Cluster 2: Densely Populated City Districts. This cluster represents the more stereotypical, highly populated neighborhoods. These neighborhoods have large populations with the overall largest number of elderly people. These districts have a high percentage of elderly living alone. However, this is offset by an above-average disposable income and low percentages of elderly people. These districts need a large number of resources to serve a large number of people in the neighborhoods. However, they likely need fewer resources per person due to their above-average wealth and low disability rate among the elderly.
- Cluster 3: Wealthy and Healthy. This cluster represents Barcelona’s most privileged communities. Cluster 3 has, by far, the highest disposable income, giving them much greater access to resources than others. This district has the lowest disability rate among the elderly and the lowest percentage of elderly living alone. This district would likely need fewer resources per elderly citizen than the rest of the districts. The high wealth will allow a possible user to afford more premium elder care services. The low percentage of elderly living alone indicates that they, on average, have support, which decreases the demand for homecare in minor cases. All this compounded with the fact that the district has the lowest elderly disability rate indicates that resources could be better used in other districts.
- Cluster 4: Middle Class. This cluster is the largest in terms of neighborhoods, and it represents Barcelona’s middle-income neighborhoods. This cluster of neighborhoods is the second most populous behind the cluster. They have a middle level of income, with an RFID around 76, which is around the midpoint when accounting for the right skew of the variable. When compared to the other neighborhoods, it has mid-level percentages of disabled, elderly, and disabled elderly. These neighborhoods act as the baseline for Barcelona in terms of demand for care services. They should receive more resources per capita than Clusters 2 and 3 but less than Clusters 1 and 5.
- Cluster 5: Vulnerable. This cluster represents Barcelona’s most vulnerable neighborhoods. These neighborhoods, along with those in Cluster 1, have the lowest disposable income in Barcelona. In addition, these neighborhoods have, by far, the highest percentages of elderly living alone and of elderly with disabilities. Putting it all together, it paints a grim picture for the quality of life for the elderly citizens in this cluster. These neighborhoods should be a priority when implementing an elderly care system in Barcelona and be allocated the highest amount of resources per capita compared to the rest of the clusters.
3.3. PCA of Barcelona’s Neighborhoods
- Cluster 1 is spread out into the top right region of the map; we can see that neighborhoods in this cluster tend to have a smaller cumulative population of elderly citizens, a lower percentage of people living alone, a higher percentage of disabled, and a lower RFID index.
- Cluster 2 is located at the bottom left of the chart; this positioning indicates that these neighborhoods have a higher cumulative number of elderly citizens, a higher than average RFID, a large percentage of elderly citizens living alone, and a low percentage of disabled elderly people.
- Cluster 3 is located on the top left of the map, indicating that it has the highest RFID, a somewhat higher number of elderly than average, low percentages of elderly people living alone, and the lowest percentage of disabled elderly.
- Cluster 4, as mentioned in the previous section, represents the median neighborhoods, as it lies in the midpoint of the chart, indicating it represents the mean value for the four variables.
- Cluster 5 is located on the bottom right of the map. Like Cluster 1, it has lower values for the RFID and a high percentage of disabled elderly. However, unlike Cluster 1, it is located towards the bottom of the map, indicating a large elderly population and a large percentage of elderly people living alone.
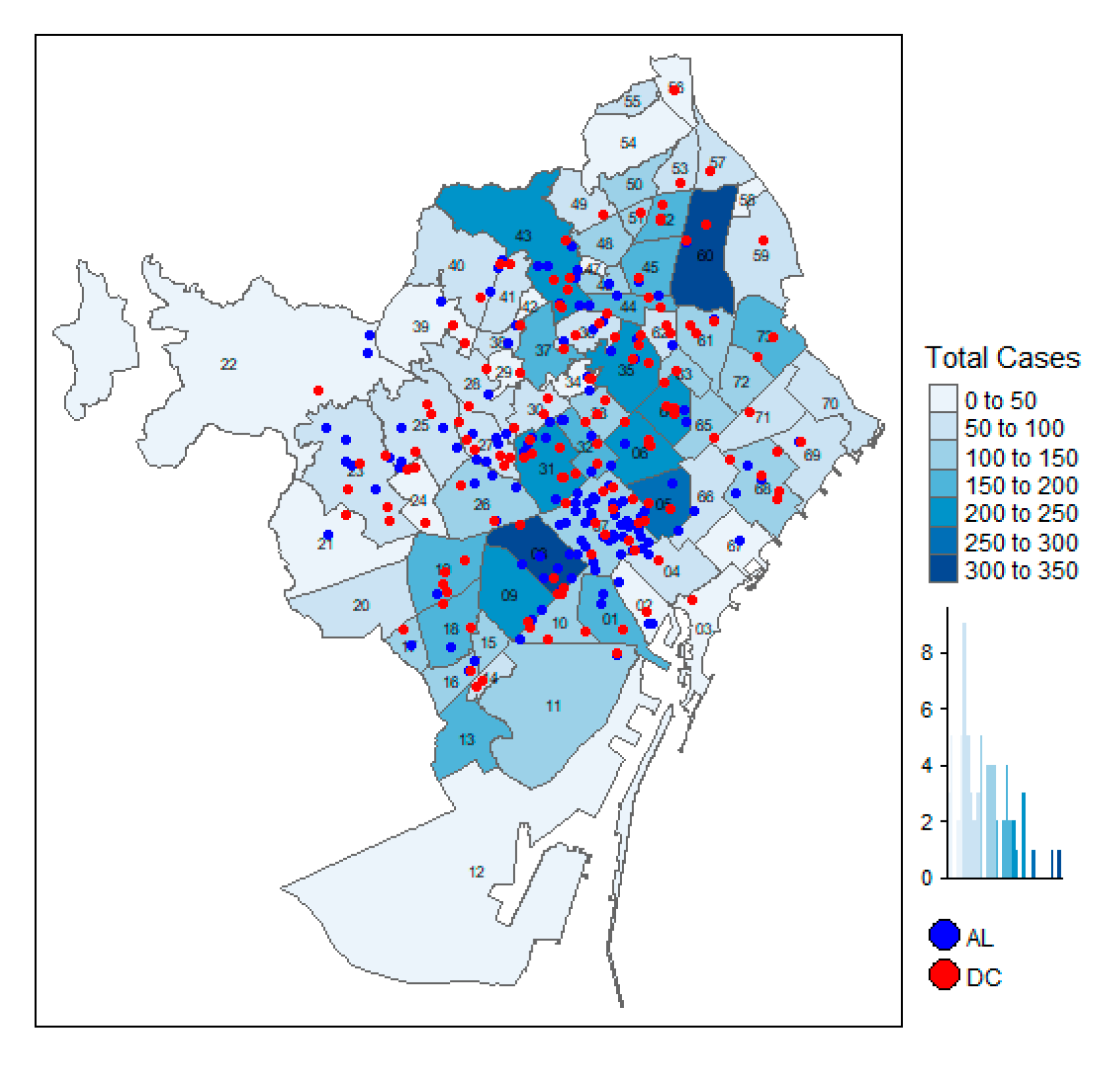
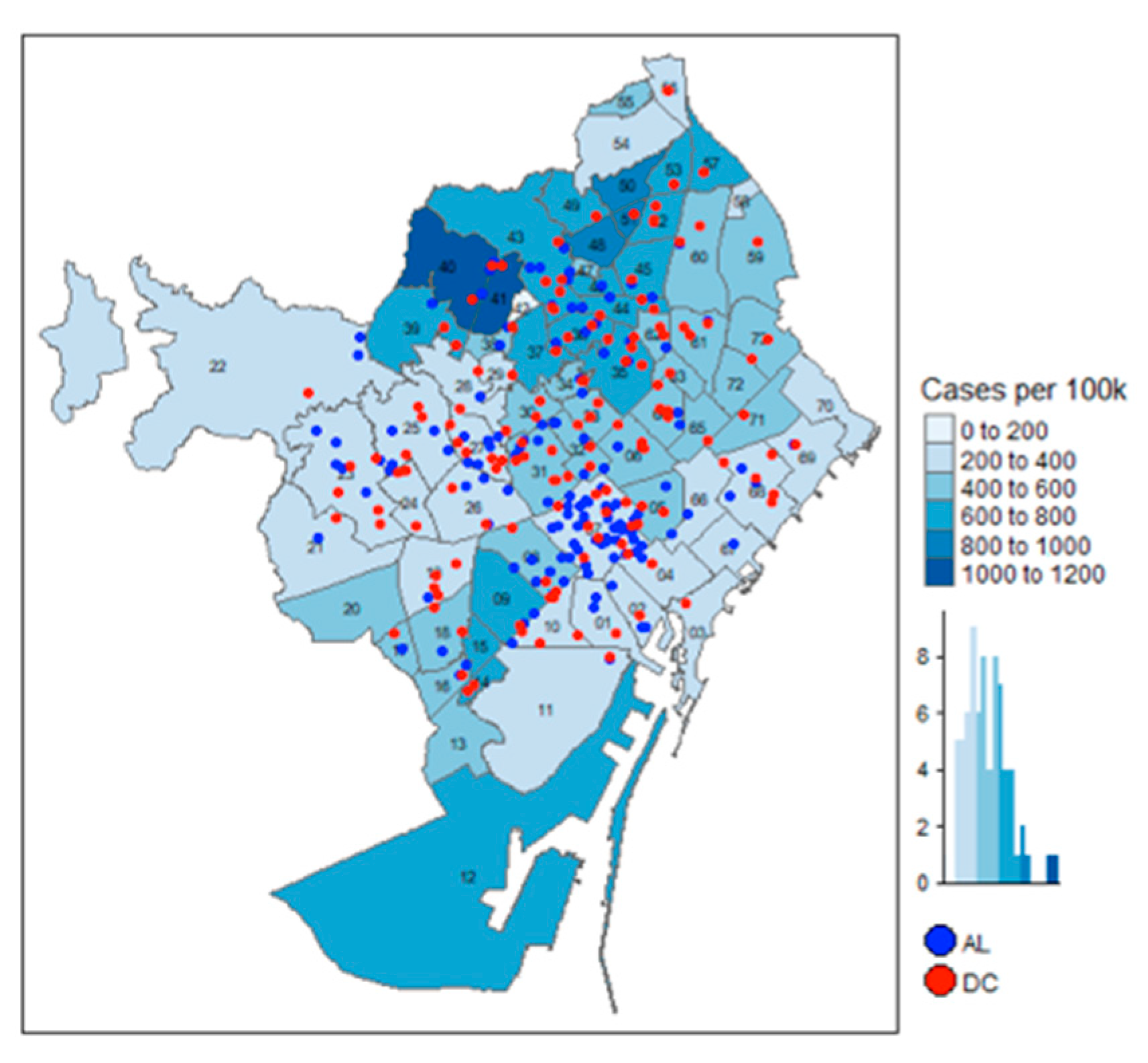
3.4. Analysis of Barcelona’s COVID-19 Cases
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lin, J.-R.; Chen, C.-Y.; Peng, T.-K. Study of the relevance of the quality of care, operating efficiency and inefficient quality competition of senior care facilities. J. Environ. Res. Public Health 2017, 14, 1047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Market Watch. Elder Care Services Market Size 2020 Industry Share, Trends Evaluation, Global Growth, Recent Developments, Latest Technology, CAGR of 2.4%, and 2026 Future Forecast Research Report. Available online: https://www.marketwatch.com/press-release/elder-care-services-market-size-2020-industry-share-trends-evaluation-global-growth-recent-developments-latest-technology-cagr-of-24-and-2026-future-forecast-research-report-2020-07-14 (accessed on 5 August 2020).
- Coe, N.B.; Van Houtven, C.H. Living Arrangements of Older Adults and COVID-19 Risk: It Is Not Just Nursing Homes. J. Am. Geriatr. Soc. 2020, 68, 1398–1399. [Google Scholar] [CrossRef] [PubMed]
- The New York Times. A Deluged System Leaves Some Elderly to Die, Rocking Spain’s Self-Image. Available online: www.nytimes.com/2020/03/25/world/europe/Spain-coronavirus-nursing-homes.html (accessed on 5 August 2020).
- Lee, A.H.I.; Kang, H.-Y. A multi-criteria decision-making model for evaluating senior daycare center locations. J. Environ. Res. Public Health 2019, 16, 5031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burge, P.; Netten, A.; Gallo, F. Estimating the value of social care. J. Health. Econ. 2010, 29, 883–894. [Google Scholar] [CrossRef] [PubMed]
- Ajuntament de Barcelona. Population Register 2019. Available online: https://www.bcn.cat/estadistica/castella/dades/tpob/pad/padro/evo/ev02.htm (accessed on 5 August 2020).
- Open Data BCN. Ajuntament de Barcelona’s Open Data Service. Available online: https://opendata-ajuntament.barcelona.cat/en (accessed on 5 August 2020).
- Ajuntament de Barcelona. Territorial Distribution of Family Income per Capita in Barcelona. Available online: https://ajuntament.barcelona.cat/barcelonaeconomia/ca/renda-familiar/renda-familiar/distribucio-territorial-de-la-renda-familiar-disponible-capita (accessed on 5 August 2020).
- Github. Barcelona Geodata. Available online: https://github.com/martgnz/bcn-geodata (accessed on 5 August 2020).
- Portnoy, J.; Waller, M.; Elliott, T. Telemedicine in the Era of COVID-19. J. Allergy. Clin. Immuno. 2020, 8, 1489–1491. [Google Scholar] [CrossRef] [PubMed]
- Eveborn, P.; Rönnqvist, M.; Einarsdóttir, H.; Eklund, M.; Lidén, K.; Almroth, M. Operations Research Improves Quality and Efficiency in Home Care. Interfaces 2009, 39, 18–34. [Google Scholar] [CrossRef]
- Tran, A.; Nguyen, K.-H.; Gray, L.; Comans, T. A systematic literature review of efficiency measurement in nursing homes. Int. J. Environ. Res. Public Health 2019, 16, 2186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garavaglia, G.; Lettieri, E.; Agasisti, T.; Lopez, S. Efficiency and quality of care in nursing homes: An Italian case study. Health Care Manag. Sci. 2011, 14, 22–35. [Google Scholar] [CrossRef] [PubMed]
- Foston Europe. Senior Care in Spain. Available online: https://www.foston.eu/senior-care-in-spain/ (accessed on 5 August 2020).
- Mills, W.R.; Buccola, J.M.; Sender, S.; Lichtefeld, J.; Romano, N.; Reynolds, K.; Price, M.; Phipps, J.; White, L.; Howard, S. Home-Based Primary Care Led-Outbreak Mitigation in Assisted Living Facilities in the First 100 Days of Coronavirus Disease 2019. J. Am. Med. Dir. Assoc. 2020, 21, 951–953. [Google Scholar] [CrossRef] [PubMed]
- Home Instead Senior Care and Global Coalition on Aging. Relationship-Based Care and Positive Outcomes for People with Alzheimer’s and their Families. Available online: https://www.ncgg.go.jp/topics/dementia/documents/Topic1-7JeffHuber.pdf (accessed on 5 August 2020).
- Home Instead Senior Care. Paid In-Home Care: More Care & Better Care for Seniors. Available online: https://www.homeinstead.com/Documents/BETTER%20CARE%20FOR%20SENIORS.pdf (accessed on 5 August 2020).
- National Conference of State Legislatures and AARP Public Policy Institute. Aging in Place: A State Survey of Livability Policies and Practices. Available online: https://assets.aarp.org/rgcenter/ppi/liv-com/aging-in-place-2011-full.pdf (accessed on 5 August 2020).
- Dobbs, D.; Peterson, L.; Hyer, K. The Unique Challenges Faced by Assisted Living Communities to Meet Federal Guidelines for COVID-19. J. Aging Soc. Policy 2020, 32, 334–342. [Google Scholar] [CrossRef] [PubMed]
- The Washington Post. Nursing Homes Linked to up to Half of Coronavirus Deaths in Europe, WHO Says. Available online: https://www.washingtonpost.com/world/europe/nursing-homes-coronavirus-deathseurope/2020/04/23/d635619c-8561-11ea-81a3-9690c9881111_story.html (accessed on 5 August 2020).
- American Geriatrics Society (AGS). Policy Brief: COVID-19 and Assisted Living Facilities. J. Am. Geriatr. Soc. 2020, 68, 1131–1135. [Google Scholar] [CrossRef] [PubMed]
- Strausbaugh, L.J.; Sukumar, S.R.; Joseph, C.L.; High, K.P. Infectious Disease Outbreaks in Nursing Homes: An Unappreciated Hazard for Frail Elderly Persons. Clin. Infect. Dis. 2003, 36, 870–876. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Index | Data Table | Source |
|---|---|---|
| 1 | Neighborhood population by gender | Open Data BCN |
| 2 | Neighborhood population by age | Open Data BCN |
| 3 | Neighborhood population by age quantiles | Open Data BCN |
| 4 | Neighborhood population by gender and age | Open Data BCN |
| 5 | Neighborhood disabled population by age quantiles | Open Data BCN |
| 6 | Neighborhood population living alone by age | Open Data BCN |
| 7 | Censual Districts population demographics | Open Data BCN |
| 8 | Neighborhood RFID index | Government Report |
| 9 | Geographic outlines | GitHub [10] |
| 10 | Assisted living facilities | Open Data BCN |
| 11 | Day care centers | Open Data BCN |
| 12 | COVID-19 | Barcelona Municipal Data Office |
| K-Means | Ward | n |
|---|---|---|
| One | Five | 1 |
| Four | One | 10 |
| Four | Three | 1 |
| Four | Five | 1 |
| Cluster | Hit Rate | |
|---|---|---|
| Overall | 60/73 | 82.2% |
| One | 12/13 | 92.3% |
| Two | 14/14 | 100% |
| Three | 7/7 | 100% |
| Four | 17/29 | 58.7% |
| Five | 10/10 | 100% |
| Variable | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) |
|---|---|---|---|---|---|---|---|---|
| Elderly Population | 0.021 1 | 0.021 1 | 0.021 1 | 0.021 1 | 0.021 1 | 0.021 1 | 0.021 1 | 0.021 1 |
| (0.002) | (0.001) | (0.001) | (0.002) | (0.002) | (0.001) | (0.002) | (0.002) | |
| RFID | −0.401 1 | −0.415 1 | −0.414 1 | −0.413 1 | −0.508 1 | −0.519 1 | −0.516 1 | −0.520 1 |
| (0.101) | (0.105) | (0.105) | (0.106) | (0.13) | (0.133) | (0.133) | (0.134) | |
| % of Disabled Elderly | −1.85 | −1.765 | −1.763 | −1.856 | ||||
| (1.427) | (1.416) | (1.417) | (1.435) | |||||
| DC Capacity | −0.026 | −0.044 | −0.047 | −0.066 | ||||
| (0.125) | (0.133) | (0.125) | (0.134) | |||||
| AL Capacity | 0.006 | 0.008 | 0.005 | 0.008 | ||||
| (0.019) | (0.02) | (0.019) | (0.02) | |||||
| Total Facility Capacity | 0.005 | 0.003 | ||||||
| (0.018) | (0.018) | |||||||
| Constant | 45.544 1 | 46.367 1 | 46.273 1 | 46.282 1 | 96.024 2 | 94.584 2 | 94.417 2 | 96.947 2 |
| (10.864) | (11.013) | (11.018) | (11.088) | (40.404) | (40.207) | (40.211) | (40.715) | |
| Observations | 73 | 73 | 73 | 73 | 73 | 73 | 73 | 73 |
| R2 | 0.785 | 0.785 | 0.785 | 0.785 | 0.79 | 0.79 | 0.79 | 0.791 |
| Adjusted R2 | 0.775 | 0.776 | 0.776 | 0.773 | 0.778 | 0.777 | 0.777 | 0.775 |
| Residual Std. Error | 36.157 (df = 69) | 36.144 (df = 69) | 36.151 (df = 69) | 36.380 (df = 68) | 35.980 (df = 68) | 36.000 (df = 68) | 36.008 (df = 68) | 36.201 (df = 67) |
| F Statistic | 83.882 1 (df = 3; 69) | 83.960 1 (df = 3; 69) | 83.919 1 (df = 3; 69) | 62.183 1 (df = 4; 68) | 63.953 1 (df = 4; 68) | 63.864 1 (df = 4; 68) | 63.827 1 (df = 4; 68) | 50.572 1 (df = 5; 67) |
| Variable | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) |
|---|---|---|---|---|---|---|---|---|
| % of Elderly | 27.360 1 | 25.544 1 | 25.679 1 | 26.504 1 | 26.491 1 | 25.028 1 | 25.202 1 | 25.428 1 |
| (4.194) | (4.168) | (4.202) | (4.211) | (4.821) | (4.868) | (4.885) | (4.846) | |
| RFID | −2.065 1 | −2.286 1 | −2.260 1 | −2.223 1 | −2.205 1 | −2.366 1 | −2.335 1 | −2.397 1 |
| (0.383) | (0.397) | (0.4) | (0.397) | (0.538) | (0.555) | (0.555) | (0.552) | |
| % of Disabled Elderly | −2.27 | −1.252 | −1.174 | −2.768 | ||||
| (6.084) | (5.986) | (6.006) | (6.052) | |||||
| DC Capacity | −0.316 | −0.585 | −0.343 | −0.623 | ||||
| (0.405) | (0.446) | (0.414) | (0.457) | |||||
| AL Capacity | 0.062 | 0.106 | 0.062 | 0.108 | ||||
| (0.069) | (0.076) | (0.069) | (0.077) | |||||
| Total Facility Capacity | 0.045 | 0.045 | ||||||
| (0.064) | (0.064) | |||||||
| Constant | 120.975 | 155.419 | 151.546 | 145.196 | 199.628 | 199.332 | 192.58 | 241.573 |
| (95.199) | (96.341) | (96.774) | (96.16) | (231.587) | (231.256) | (231.475) | (231.876) | |
| Observations | 73 | 73 | 73 | 73 | 73 | 73 | 73 | 73 |
| R2 | 0.532 | 0.534 | 0.532 | 0.545 | 0.533 | 0.534 | 0.532 | 0.547 |
| Adjusted R2 | 0.512 | 0.514 | 0.511 | 0.519 | 0.506 | 0.507 | 0.504 | 0.513 |
| Residual Std. Error | 136.391 (df = 69) | 136.186 (df = 69) | 136.494 (df = 69) | 135.482 (df = 68) | 137.250 (df = 68) | 137.140 (df = 68) | 137.456 (df = 68) | 136.277 (df = 67) |
| F Statistic | 26.190 1 (df = 3; 69) | 26.338 1 (df = 3; 69) | 26.116 1 (df = 3; 69) | 20.389 1 (df = 4; 68) | 19.432 1 (df = 4; 68) | 19.491 1 (df = 4; 68) | 19.323 1 (df = 4; 68) | 16.163 1 (df = 5; 67) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arvelo, E.; de Armas, J.; Guillen, M. Assessing the Distribution of Elderly Requiring Care: A Case Study on the Residents in Barcelona and the Impact of COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 7486. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207486
Arvelo E, de Armas J, Guillen M. Assessing the Distribution of Elderly Requiring Care: A Case Study on the Residents in Barcelona and the Impact of COVID-19. International Journal of Environmental Research and Public Health. 2020; 17(20):7486. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207486
Chicago/Turabian StyleArvelo, Enrique, Jesica de Armas, and Monserrat Guillen. 2020. "Assessing the Distribution of Elderly Requiring Care: A Case Study on the Residents in Barcelona and the Impact of COVID-19" International Journal of Environmental Research and Public Health 17, no. 20: 7486. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207486