Evaluation of Psychophysical Factors in Individuals with Frailty Syndrome Following a 3-Month Controlled Physical Activity Program

 , , and
, , and 
Abstract
:1. Introduction
Study Aim
2. Material and Methods
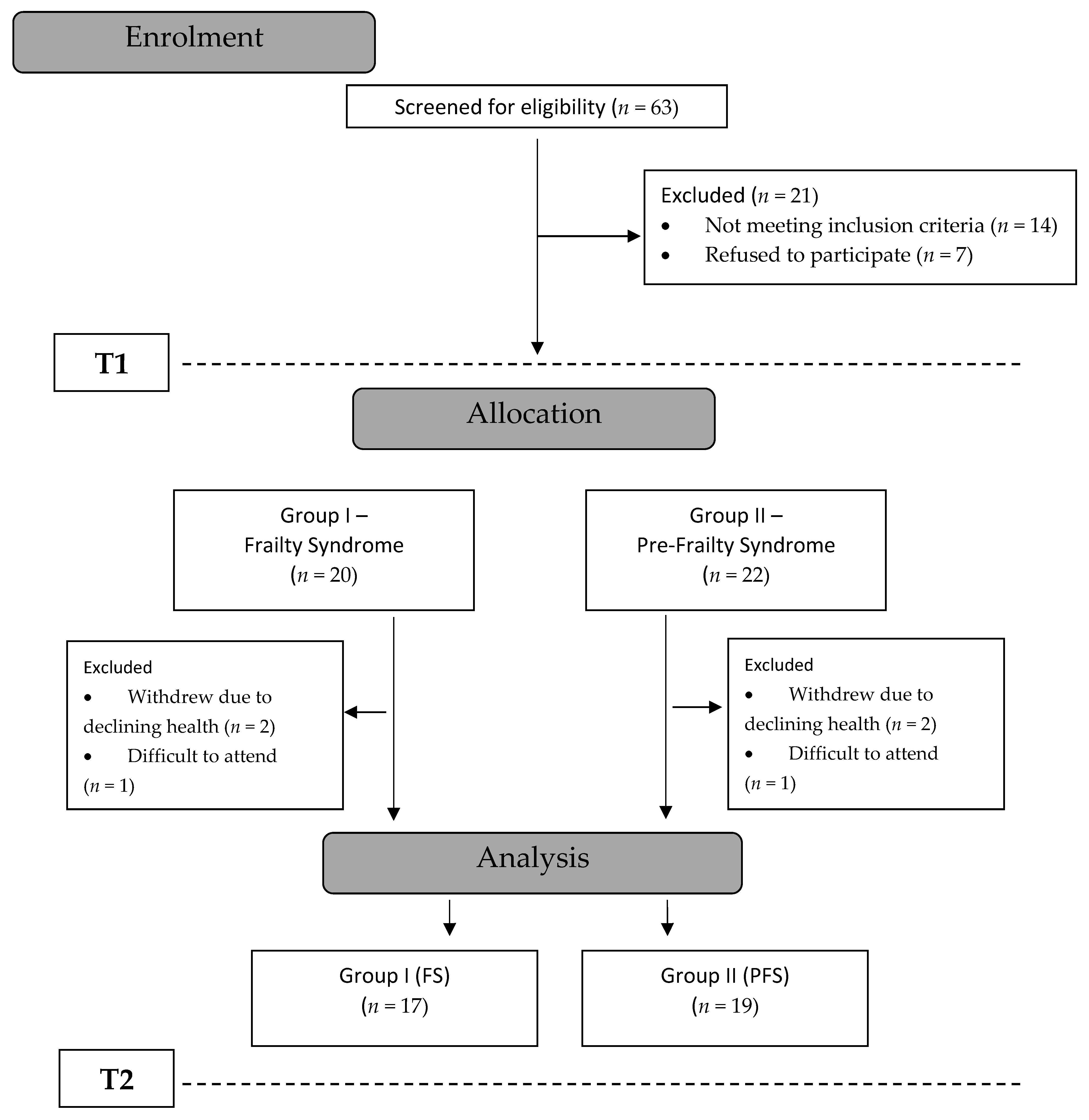
2.1. Study Group
2.2. Measurement Tools
2.3. Examination of Force–Velocity Parameters
2.4. Training Sessions
2.5. Statistical Analysis
2.6. Results
3. Discussion
4. Limitations
5. Conclusions
- In individuals with pre-frailty and frailty syndrome, the 3-month physical training programme improved the strength parameters of lower limb muscles.
- An improvement in mood and reduction in depressive symptoms was only observed in the group of subjects with pre-frailty syndrome.
- Rehabilitation programmes for people with frailty syndrome should include psychotherapeutic activities in addition to physical training in order to improve the psychophysical condition of patients.
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| PFS | pre-frailty syndrome group |
| FS | frailty syndrome group |
| SWLS | satisfaction with life scale |
| BDI | Beck depression inventory |
| STAI | Spielberg’s state-trait anxiety inventory |
| PT | peak torque |
| TW | total work |
| aP | average power |
| E | knee extensors |
| F | knee flexors |
| R | right side |
| L | left side |
| T1 | initial results |
| T2 | final results |
References
- Leng, S.X.; Chen, X.; Mao, G. Frailty syndrome: An overview. Clin. Interv. Aging 2014, 9, 433–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Billot, M.; Calvani, R.; Urtamo, A.; Sánchez-Sánchez, J.L.; Ciccolari-Micaldi, C.; Chang, M.; Roller-Wirnsberger, R.; Wirnsberger, G.; Sinclair, A.; Vaquero-Pinto, M.N.; et al. Preserving Mobility in Older Adults with Physical Frailty and Sarcopenia: Opportunities, Challenges, and Recommendations for Physical Activity Interventions. Clin. Interv. Aging 2020, 15, 1675–1690. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G.; Liljas, A.E.; Iliffe, S. Frailty syndrome: Implications and challenges for health care policy. RMHP 2019, 2, 23–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terroso, M.; Rosa, N.; Marques, A.; Simoes, R. Physical consequences of falls in the elderly: A literature review from 1995 to 2010. Eur. Rev. Aging Phys. Act. 2013, 11, 51–59. [Google Scholar] [CrossRef] [Green Version]
- Tieland, M.; Trouwborst, I.; Clark, B.C. Skeletal muscle performance and ageing. J. Cachexia Sarcopenia Muscle 2017, 9, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Madaan, V.; Petty, F.D. Exercise for Mental Health. Prim. Care Companion J. Clin. Psychiatry 2006, 8, 106. [Google Scholar] [CrossRef]
- Bilotta, C.; Bergamaschini, L.; Nicolini, P.; Casè, A.; Pina, G.; Rossi, S.V.; Vergani, C. Frailty syndrome diagnosed according to the Study of Osteoporotic Fractures criteria and mortality in older outpatients suffering from Alzheimer’s disease: A one-year prospective cohort study. Aging Ment. Health 2011, 16, 273–280. [Google Scholar] [CrossRef]
- Dressendorfer, R.; Palmer, E. Frailty Syndrome: Physical Therapy. Clinahl Information System EBSCO, 2016. Available online: https://0-www-ebscohost-com.brum.beds.ac.uk/promoMaterials/January_2017_-_Fraily_Syndrome.pdf (accessed on 30 December 2016).
- Mazurek, J.; Kowalska, J.; Rymaszewska, J. Physical exercise as prevention and therapy for frailty syndrome. Przegląd Lekarski 2018, 75, 91–93. [Google Scholar]
- Gallè, F.; Di Onofrio, V.; Spica, V.R.; Mastronuzzi, R.; Krauss, P.R.; Belfiore, P.; Liguori, G.; Buono, P. Improving physical fitness and health status perception in community-dwelling older adults through a structured program for physical activity promotion in the city of Naples, Italy: A randomized controlled trial. Geriatr. Gerontol. Int. 2016, 17, 1421–1428. [Google Scholar] [CrossRef]
- Zawadzki, B.; Popiel, A.; Pragłowska, E. Charakterystyka psychometryczna polskiej adaptacji Kwestionariusza Depresji BDI-II Aarona Becka. Psychol.-Etiol.-Genet. 2009, 19, 71–95. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W.F. Comparison of Beck Depression Inventories-IA and-II in Psychiatric Outpatients. J. Pers. Assess. 1996, 67, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Juczyński, Z. Narzȩdzia Pomiaru w Promocji i Psychologii Zdrowia (Measurement Tools in Health Promotion and Psychology), 2nd ed.; Laboratory of Psychological Tests of the Polish: Warsaw, Poland, 2009. [Google Scholar]
- Skapinakis, P. The Spielberger State-Trait Anxiety Inventory. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Berlin/Heidelberg, Germany, 2014; pp. 6261–6264. [Google Scholar] [CrossRef]
- Sosnowski, T.; Wrześniewski, K.; Jaworska, A.; Fecenec, D. STAI—Inwentarz Stanu i Cechy Lęku STAI. Polska Adaptacja STAI; Pracownia Testów Psychologicznych: Warsaw, Poland, 2011. [Google Scholar]
- Davies, G. Compedium of Isokinetics in Clinical Usage and Rehabilitation Techniques, 4th ed.; S&S Publishers: Onalaska, WI, USA, 1992. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Willson, V.L. Critical Values of the Rank-Biserial Correlation Coefficient. Educ. Psychol. Meas. 1976, 36, 297–300. [Google Scholar] [CrossRef]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect size estimates: Current use, calculations, and interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, A. Discovering Statistics Using SPSS, 2nd ed.; Sage Publications: London, UK, 2005. [Google Scholar]
- Peluso, M.A.M.; De Andrade, L.H.S.G. Physical activity and mental health: The association between exercise and mood. Clinics 2005, 60, 61–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grasdalsmoen, M.; Eriksen, H.R.; Lønning, K.J.; Sivertsen, B. Physical exercise, mental health problems, and suicide attempts in university students. BMC Psychiatry 2020, 20, 175. [Google Scholar] [CrossRef] [Green Version]
- Dziubek, W.; Kowalska, J.; Kusztal, M.; Rogowski, Ł.; Gołębiowski, T.; Nikifur, M.; Szczepańska-Gieracha, J.; Zembroń-Łacny, A.; Klinger, M.; Woźniewski, M. The Level of Anxiety and Depression in Dialysis Patients Undertaking Regular Physical Exercise Training—A Preliminary Study. Kidney Blood Press. Res. 2016, 41, 86–98. [Google Scholar] [CrossRef]
- Mikkelsen, K.; Stojanovska, L.; Polenakovic, M.; Bosevski, M.; Apostolopoulos, V. Exercise and mental health. Maturitas 2017, 106, 48–56. [Google Scholar] [CrossRef]
- Guure, C.B.; Ibrahim, N.A.; Adam, M.B.; Said, S.M. Impact of Physical Activity on Cognitive Decline, Dementia, and Its Subtypes: Meta-Analysis of Prospective Studies. BioMed Res. Int. 2017, 2017. [Google Scholar] [CrossRef]
- Sutorius, F.L.; Hoogendijk, E.O.; Prins, B.A.H.; Van Hout, H.P.J. Comparison of 10 single and stepped methods to identify frail older persons in primary care: Diagnostic and prognostic accuracy. BMC Fam. Pract. 2016, 17, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Faller, J.W.; Pereira, D.D.N.; De Souza, S.; Nampo, F.K.; Orlandi, F.D.S.; Matumoto, S. Instruments for the detection of frailty syndrome in older adults: A systematic review. PLoS ONE 2019, 14, e0216166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szczepańska-Gieracha, J.; Kowalska, J.; Pawik, M.; Rymaszewska, J. Evaluation of a short-term group psychotherapy used as part of the rehabilitation process in nursing home patients. Disabil. Rehabil. 2013, 36, 1027–1032. [Google Scholar] [CrossRef]
- Kowalska, J.; Mazurek, J.; Kubasik, N.; Rymaszewska, J. Effectiveness of physiotherapy in elderly patients with dementia: A prospective, comparative analysis. Disabil. Rehabil. 2017, 41, 815–819. [Google Scholar] [CrossRef]
- Jaeschke, R.; Siwek, M.; Grabski, B.; Dudek, D. Współwystępowanie zaburzeń depresyjnych i lękowych. Psychiatria 2010, 7, 189–197. [Google Scholar]
- Zembroń-Łacny, A.; Dziubek, W.; Rogowski, Ł.; Skorupka, E.; Dąbrowska, G. Sarcopenia: Monitoring, molecular mechanisms, and physical intervention. Physiol. Res. 2014, 63, 683–691. [Google Scholar]
- Beaudart, C.; Dawson, A.; Shaw, S.C.; Harvey, N.C.; Kanis, J.A.; Binkley, N.; Reginster, J.Y.; Chapurlat, R.; Chan, D.C.; IOF-ESCEO Sarcopenia Working Group; et al. Nutrition and physical activity in the prevention and treatment of sarcopenia: Systematic review. Osteoporos. Int. 2017, 28, 1817–1833. [Google Scholar] [CrossRef] [Green Version]
- Cameron, I.D.; Fairhall, N.; Langron, C.; Lockwood, K.; Monaghan, N.; Aggar, C.; Sherrington, C.; Lord, S.R.; Kurrle, S.E. A multifactorial interdisciplinary intervention reduces frailty in older people: Randomized trial. BMC Med. 2013, 11, 65. [Google Scholar] [CrossRef] [Green Version]
- Tarazona-Santabalbina, F.J.; Gómez-Cabrera, M.C.; Pérez-Ros, P.; Martínez-Arnau, F.M.; Cabo, H.; Tsaparas, K.; Salvador-Pascual, A.; Rodriguez-Mañas, L.; Viña, J. A Multicomponent Exercise Intervention that Reverses Frailty and Improves Cognition, Emotion, and Social Networking in the Community-Dwelling Frail Elderly: A Randomized Clinical Trial. J. Am. Med. Dir. Assoc. 2016, 17, 426–433. [Google Scholar] [CrossRef] [Green Version]
- Cadore, E.L.; Pinto, R.S.; Bottaro, M.; Izquierdo, M. Strength and Endurance Training Prescription in Healthy and Frail Elderly. Aging Dis. 2014, 5, 183. [Google Scholar] [CrossRef] [PubMed]
- Pinto, R.S.; Correa, C.S.; Radaelli, R.; Cadore, E.L.; Brown, L.E.; Bottaro, M. Short-term strength training improves muscle quality and functional capacity of elderly women. Age 2013, 36, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Tracy, B.L.; Ivey, F.M.; Hurlbut, D.; Martel, G.F.; Lemmer, J.T.; Siegel, E.L.; Metter, E.J.; Fozard, J.L.; Fleg, J.L.; Hurley, B.F. Muscle quality. II. Effects of strength training in 65- to 75-yr-old men and women. J. Appl. Physiol. 1999, 86, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Batista, F.S.; Gomes, G.A.D.O.; D’Elboux, M.J.; Cintra, F.A.; Neri, A.L.; Guariento, M.E.; Souza, M.D.L.R.D. Relationship between lower-limb muscle strength and functional independence among elderly people according to frailty criteria: A cross-sectional study. Sao Paulo Med. J. 2014, 132, 282–289. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| PFS Group n = 19 | FS Group n = 17 | Test T | Cohen’s d | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | SD | Mean | Median | SD | t | p | ||
| Age (Years) | 69.16 | 67.00 | 5.01 | 75.35 | 73.00 | 6.40 | −3.25 | 0.0026 * | 1.12 |
| Height (cm) | 153.97 | 162.00 | 37.68 | 149.91 | 160.00 | 39.05 | 0.32 | 0.7528 | 0.11 |
| Body mass (kg) | 77.05 | 76.00 | 11.99 | 70.35 | 70.00 | 14.16 | 1.54 | 0.1336 | 0.53 |
| BMI (kg/m2) | 29.39 | 29.00 | 3.68 | 27.98 | 27.34 | 5.30 | 0.94 | 0.3543 | 0.32 |
| Group | BDI Results | T1 | T2 | Chi2 p-Value | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| PFS | No depression BDI < 12 | 9 | 47 | 15 | 79 | 0.0328 * |
| Depression BDI ≥ 12 | 10 | 53 | 4 | 21 | ||
| FS | No depression BDI < 12 | 11 | 65 | 7 | 41 | 0.6275 |
| Depression BDI ≥ 12 | 6 | 35 | 10 | 59 | ||
| Group | T1 | T2 | T1 vs. T2 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Median | Min | Max | Median | Min | Max | Wilcoxon Test | rc | |||
| Z | p | |||||||||
| PFS | SWLS | 22.00 | 9.00 | 30.00 | 23.00 | 10.00 | 30.00 | 0.00 | 0.5228 | 0.15 |
| BDI (1–13) | 5.00 | 0.00 | 13.00 | 3.00 | 0.00 | 12.00 | 2.77 | 0.0058 * | 0.77 | |
| BDI (14–21) | 4.00 | 0.00 | 11.00 | 3.00 | 0.00 | 10.00 | 2.41 | 0.0413 * | 0.55 | |
| BDI all | 12.00 | 0.00 | 20.00 | 5.00 | 0.00 | 21.00 | 2.07 | 0.0031 * | 0.76 | |
| STAI X-1 | 44.00 | 26.00 | 73.00 | 40.00 | 26.00 | 75.00 | 1.84 | 0.0079 * | 0.61 | |
| STAI X-2 | 44.00 | 25.00 | 74.00 | 41.00 | 23.00 | 53.00 | 2.07 | 0.0070 * | 0.70 | |
| FS | SWLS | 24.00 | 20.00 | 30.00 | 24.00 | 13.00 | 28.00 | 0.49 | 0.1075 | 0.39 |
| BDI 1–13 | 2.00 | 0.00 | 16.00 | 5.00 | 0.00 | 12.00 | 0.00 | 0.2934 | 0.27 | |
| BDI 14–21 | 5.00 | 1.00 | 12.00 | 8.00 | 0.00 | 13.00 | 1.46 | 0.0976 | 0.40 | |
| BDI all | 7.00 | 1.00 | 21.00 | 14.00 | 1.00 | 22.00 | 1.34 | 0.2093 | 0.34 | |
| STAI X-1 | 37.00 | 26.00 | 55.00 | 40.00 | 23.00 | 56.00 | −0.25 | 0.4229 | 0.20 | |
| STAI X-2 | 38.00 | 25.00 | 61.00 | 40.00 | 25.00 | 56.00 | 1.94 | 0.1488 | 0.35 | |
| Group | T1 | T2 | T1 vs. T2 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | CI | SD | Mean | CI | SD | Student’s t-Test | Cohen’s d | |||
| t | p | |||||||||
| PFS | PT E 60 R (Nm) | 97.25 | 83.56–110.94 | 27.5 | 106.19 | 89.13–123.25 | 35.4 | −0.97 | 0.3446 | 0.29 |
| PT E 60 L (Nm) | 92.81 | 77.80–107.82 | 31.1 | 98.28 | 83.83–112.74 | 30.0 | −2.20 | 0.0413 * | 0.18 | |
| PT F 60 R (Nm) | 42.97 | 35.47–50.47 | 15.1 | 50.97 | 42.40–59.55 | 17.8 | −3.13 | 0.0062 * | 0.50 | |
| PT F 60 L (Nm) | 45.52 | 37.91–53.12 | 15.8 | 50.86 | 42.35–59.37 | 17.7 | −3.19 | 0.0051 * | 0.33 | |
| TW E 60 R (J) | 440.89 | 379.77–502.02 | 122.9 | 513.22 | 436.71–589.72 | 158.7 | −2.39 | 0.0284 * | 0.52 | |
| TW E 60 L (J) | 423.96 | 375.20–472.71 | 98.0 | 467.03 | 394.30–539.76 | 150.9 | −0.92 | 0.3685 | 0.35 | |
| TW F 60 R (J) | 222.12 | 184.32–259.91 | 78.4 | 258.24 | 213.58–302.90 | 92.7 | −2.99 | 0.0078 * | 0.43 | |
| TW F 60 L (J) | 237.64 | 195.78–279.50 | 86.8 | 260.99 | 216.14–305.84 | 93.0 | −2.56 | 0.0196 * | 0.27 | |
| aP E 60 R (W) | 61.04 | 51.89–70.20 | 18.4 | 64.02 | 54.00–74.04 | 20.8 | −0.26 | 0.7993 | 0.16 | |
| aP E 60 L (W) | 58.44 | 49.24–67.63 | 19.1 | 61.52 | 51.10–71.93 | 21.6 | −1.11 | 0.2800 | 0.16 | |
| aP F 60 R (W) | 27.63 | 22.14–33.13 | 11.0 | 31.04 | 25.17–36.91 | 12.2 | −1.58 | 0.1337 | 0.30 | |
| aP F 60 L (W) | 29.40 | 23.58–35.22 | 12.1 | 31.25 | 25.28–37.23 | 12.4 | −1.13 | 0.2728 | 0.16 | |
| FS | PT E 60 R (Nm) | 69.35 | 53.56–85.13 | 30.7 | 77.68 | 61.53–93.82 | 31.4 | −2.91 | 0.0103 * | 0.28 |
| PT E 60 L (Nm) | 68.65 | 52.86–84.44 | 30.7 | 75.31 | 57.09–93.53 | 35.4 | −2.97 | 0.0090 * | 0.21 | |
| PT F 60 R (Nm) | 33.36 | 25.52–41.20 | 15.2 | 39.35 | 30.28–48.41 | 17.6 | −3.01 | 0.0083 * | 0.37 | |
| PT F 60 L (Nm) | 30.86 | 22.70–39.02 | 15.9 | 36.75 | 28.11–45.39 | 16.8 | −4.98 | 0.0001 * | 0.37 | |
| TW E 60 R (J) | 369.06 | 269.86–468.25 | 192.9 | 395.15 | 308.36–481.94 | 168.8 | −0.98 | 0.3410 | 0.15 | |
| TW E 60 L (J) | 346.18 | 259.83–432.53 | 167.9 | 373.01 | 280.36–465.66 | 180.2 | −1.83 | 0.0861 | 0.16 | |
| TW F 60 R (J) | 168.82 | 118.11–219.52 | 98.6 | 185.09 | 126.74–243.44 | 113.5 | −0.88 | 0.3923 | 0.16 | |
| TW F 60 L (J) | 154.66 | 103.93–205.40 | 98.7 | 176.48 | 129.61–223.35 | 91.2 | −2.40 | 0.0287 * | 0.24 | |
| aP E 60 R (W) | 42.33 | 32.18–52.48 | 19.7 | 46.41 | 36.35–56.47 | 19.6 | −2.25 | 0.0387 * | 0.21 | |
| aP E 60 L (W) | 41.10 | 31.10–51.10 | 19.4 | 45.49 | 34.24–56.75 | 21.9 | −3.04 | 0.0077 * | 0.22 | |
| aP F 60 R (W) | 18.83 | 13.55–24.11 | 10.3 | 25.48 | 19.51–31.44 | 11.6 | −2.56 | 0.0211 * | 0.63 | |
| aP F 60 L (W) | 16.83 | 11.41–22.24 | 10.5 | 20.80 | 15.36–26.24 | 10.6 | −4.47 | 0.0004 * | 0.39 | |
| Parameters | PFS vs. FS | T1 | T2 | PFS vs. FS | T1 | T2 | ||
|---|---|---|---|---|---|---|---|---|
| U/t | p | U/t | p | |||||
| SWLS | Mann–Whitney U test | 111.00 | 0.1131 | 160.00 | 0.9747 | rrb | −0.31 | −0.01 |
| BDI (1–13) | 126.50 | 0.2743 | 104.50 | 0.0734 | 0.22 | −0.35 | ||
| BDI (14–21) | 148.00 | 0.6804 | 91.00 | 0.0265 * | −0.08 | −0.44 | ||
| BDI all | 156.50 | 0.8866 | 95.00 | 0.0365 * | 0.03 | −0.41 | ||
| STAI X-1 | 104.00 | 0.0709 | 138.50 | 0.4759 | 0.36 | −0.14 | ||
| STAI X-2 | 103.50 | 0.0685 | 143.00 | 0.5684 | 0.36 | −0.11 | ||
| PT E 60 R | Student’s t-test | 2.83 | 0.0078* | 2.54 | 0.0157 * | Cohen’s d | 0.78 | 0.87 |
| PT E 60 L | 2.34 | 0.0254 * | 2.11 | 0.0426 * | 1.10 | 0.72 | ||
| PT F 60 R | 1.88 | 0.0696 | 1.97 | 0.0576 | 0.81 | 0.68 | ||
| PT F 60 L | 2.77 | 0.0089 * | 2.45 | 0.0196 * | 1.75 | 0.84 | ||
| TW E 60 R | 1.32 | 0.1954 | 2.16 | 0.0377 * | 0.37 | 0.74 | ||
| TW E 60 L | 1.69 | 0.1014 | 1.70 | 0.0976 | 0.99 | 0.59 | ||
| TW F 60 R | 1.80 | 0.0801 | 2.13 | 0.0407 * | 0.76 | 0.73 | ||
| TW F 60 L | 2.68 | 0.0112 * | 2.75 | 0.0096 * | 1.38 | 0.94 | ||
| aP E 60 R | 2.90 | 0.0065 * | 2.61 | 0.0134 * | 0.85 | 0.90 | ||
| aP E 60 L | 2.70 | 0.0108 * | 2.21 | 0.0341* | 0.88 | 0.76 | ||
| aP F 60 R | 2.44 | 0.0203 * | 1.40 | 0.1708 | 0.97 | 0.48 | ||
| aP F 60 L | 3.31 | 0.0022 * | 2.70 | 0.0106 | 2.83 | 0.93 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dziubek, W.; Pawlaczyk, W.; Stefańska, M.; Waligóra, J.; Bujnowska-Fedak, M.; Kowalska, J. Evaluation of Psychophysical Factors in Individuals with Frailty Syndrome Following a 3-Month Controlled Physical Activity Program. Int. J. Environ. Res. Public Health 2020, 17, 7804. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17217804
Dziubek W, Pawlaczyk W, Stefańska M, Waligóra J, Bujnowska-Fedak M, Kowalska J. Evaluation of Psychophysical Factors in Individuals with Frailty Syndrome Following a 3-Month Controlled Physical Activity Program. International Journal of Environmental Research and Public Health. 2020; 17(21):7804. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17217804
Chicago/Turabian StyleDziubek, Wioletta, Weronika Pawlaczyk, Małgorzata Stefańska, Joanna Waligóra, Maria Bujnowska-Fedak, and Joanna Kowalska. 2020. "Evaluation of Psychophysical Factors in Individuals with Frailty Syndrome Following a 3-Month Controlled Physical Activity Program" International Journal of Environmental Research and Public Health 17, no. 21: 7804. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17217804