Disparities between Rural and Urban Areas of the Central Region of Saudi Arabia in the Utilization and Time-Centeredness of Emergency Medical Services

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
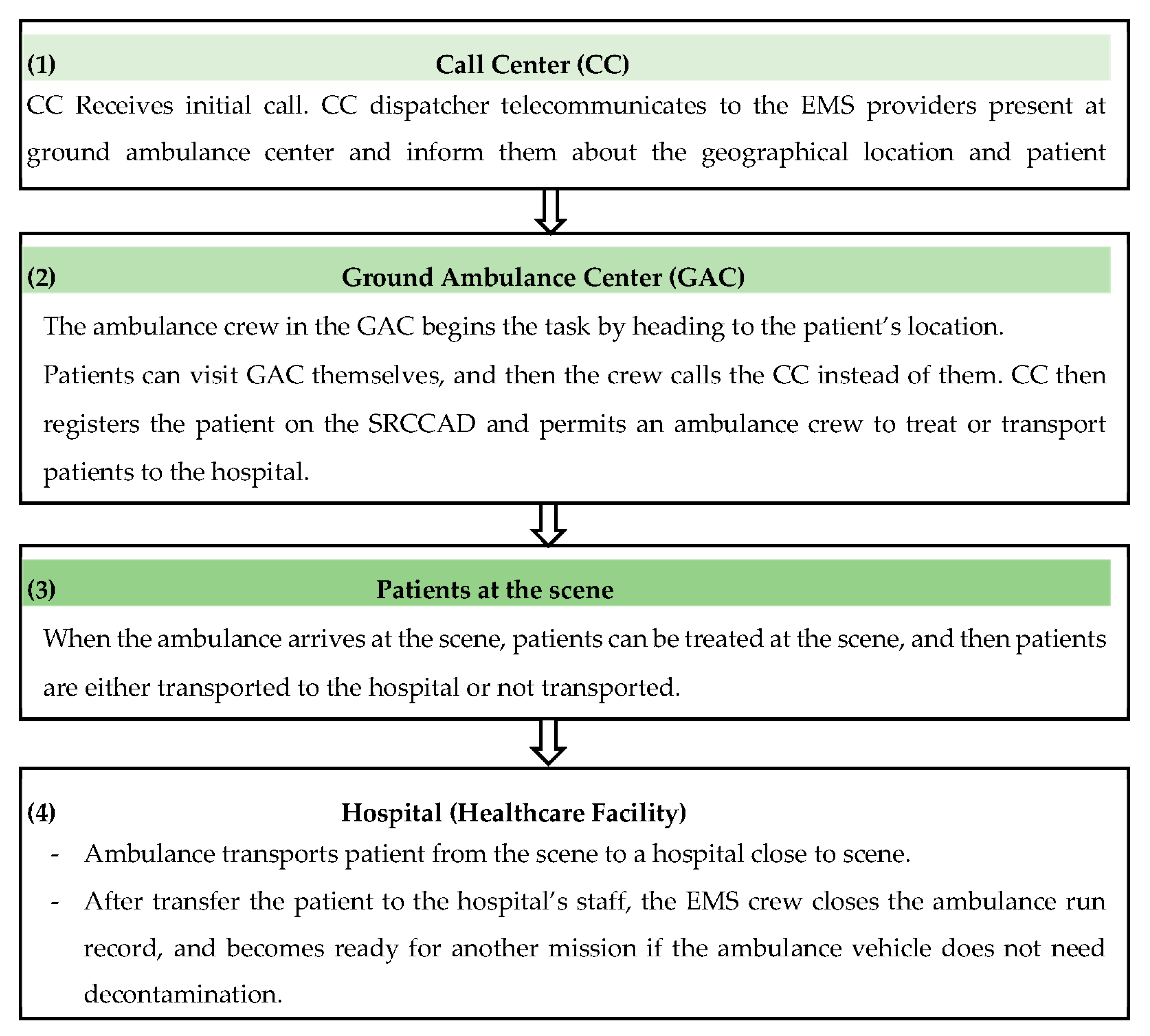
2.1. Study Setting
2.2. Data Collection
2.3. Ethical Consideration
2.4. Statistical Analysis
3. Results
3.1. Utilization of Services in Rural and Urban Areas
3.2. Response Time in Rural and Urban Areas
3.3. Total EMS Time in Urban and Rural
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Baker, A. Crossing the Quality Chasm: A New Health System for the 21st Century. Br. Med. J. 2001, 323. [Google Scholar] [CrossRef]
- Burkholder, T.W.; Hill, K.; Hynes, E.J.C. Developing emergency care systems: A human rights-based approach. Bull. World Health Organ. 2019, 97, 612. [Google Scholar] [CrossRef]
- AlHabib, K.F.; Alfaleh, H.; Hersi, A.; Kashour, T.; Alsheikh-Ali, A.A.; Suwaidi, J.A.; Sulaiman, K.; Saif, S.A.; Almahmeed, W.; Asaad, N. Use of emergency medical services in the second gulf registry of acute coronary events. Angiology 2014, 65, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Fares, S.; Zubaid, M.; Al-Mahmeed, W.; Ciottone, G.; Sayah, A.; Al Suwaidi, J.; Amin, H.; Al-Atawna, F.; Ridha, M.; Sulaiman, K. Utilization of emergency medical services by patients with acute coronary syndromes in the Arab Gulf States. J. Emerg. Med. 2011, 41, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Moafa, H.; van Kuijk, S.; Franssen, G.; Moukhyer, M.; Haak, H. What is known about the quality of out-of-hospital emergency medical services in the Arabian Gulf States? A systematic review. PLoS ONE 2019, 14, e0226230. [Google Scholar] [CrossRef] [PubMed]
- Bin Salleeh, H.M.; Gabralla, K.A.; Leggio, W.J.; Al Aseri, Z.A. Out-of-hospital adult cardiac arrests in a university hospital in central Saudi Arabia. Saudi Med. J. 2015, 36, 1071–1075. [Google Scholar] [CrossRef] [PubMed]
- Veser, A.; Sieber, F.; Groß, S.; Prückner, S. The demographic impact on the demand for emergency medical services in the urban and rural regions of Bavaria, 2012–2032. J. Public Health 2015, 23, 181–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sariyer, G.; Ataman, M.G.; Sofuoğlu, T.; Sofuoğlu, Z. Does ambulance utilization differ between urban and rural regions: A study of 112 services in a populated city, Izmir. J. Public Health 2017, 25, 379–385. [Google Scholar] [CrossRef]
- Hewitt, M.E.; Congress of the United States, Office of Technology Assessment. Rural Emergency Medical Services: Special Report; Congress of the United States, Office of Technology Assessment: Washington, DC, USA, 1989; p. 97.
- Hanchate, A.D.; Paasche-Orlow, M.K.; Dyer, K.S.; Baker, W.E.; Feng, C.; Feldman, J. Geographic variation in use of ambulance transport to the emergency department. Ann. Emerg. Med. 2017, 70, 533–543.e537. [Google Scholar] [CrossRef]
- Reece, S.C.M.; Thiruchelvam, D.; Redelmeier, D.A. Medical Emergencies in Farmers. J. Rural Health 2019, 35, 429–435. [Google Scholar] [CrossRef]
- Mell, H.K.; Mumma, S.N.; Hiestand, B.; Carr, B.G.; Holland, T.; Stopyra, J. Emergency medical services response times in rural, suburban, and urban areas. JAMA Surg. 2017, 152, 983–984. [Google Scholar] [CrossRef]
- Al-Ghamdi, A.S. Emergency medical service rescue times in Riyadh. Accid. Anal. Prev. 2002, 34, 499–505. [Google Scholar] [CrossRef]
- Alrazeeni, D.M.; Sheikh, S.A.; Mobrad, A.; Al Ghamdi, M.; Abdulqader, N.; Al Gabgab, M.; Al Qahtani, M.; Al Khaldi, B. Epidemiology of non-transported emergency medical services calls in Saudi Arabia. Saudi Med. J. 2016, 37, 575. [Google Scholar] [CrossRef] [PubMed]
- Google Map. Riyadh Province of Saudi Arabia. Available online: https://goo.gl/maps/bURYD5YfCbcXCP867 (accessed on 16 June 2020).
- The General Authority for Statistics in Saudi Arabia. Saudi Arabian Census Report for 2010. Available online: https://www.stats.gov.sa/en/73 (accessed on 30 March 2020).
- Saudi Red Crescent Authority. About the Authority. Available online: https://www.srca.org.sa/en/About/About (accessed on 30 March 2020).
- The International Federation of Red Cross and Red Crescent Societies (IFRC). The Fundamental Principles of the Red Cross and Red Crescent. Available online: https://www.ifrc.org/en/who-we-are/vision-and-mission/the-seven-fundamental-principles/impartiality/ (accessed on 16 June 2020).
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Adams, R.J.; Berry, J.D.; Brown, T.M.; Carnethon, M.R.; Dai, S.; De Simone, G.; Ford, E.S. Heart disease and stroke statistics—2011 update: A report from the American Heart Association. Circulation 2011, 123, e18–e209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alnemer, K.; Al-Qumaizi, K.I.; Alnemer, A.; Alsayegh, A.; Alqahtani, A.; Alrefaie, Y.; Alkhalifa, M.; Alhariri, A. Ambulance response time to cardiac emergencies in Riyadh. IMAM J. Appl. Sci. 2016, 1, 33. [Google Scholar]
- EMS Services in Rural America: Challenges and Opportunities. Available online: https://www.ruralcenter.org/resource-library/ems-services-in-rural-america-challenges-and-opportunities (accessed on 28 October 2020).
- Patterson, P.D.; Probst, J.C.; Moore, C.G. Expected annual emergency miles per ambulance: An indicator for measuring availability of emergency medical services resources. J. Rural Health 2006, 22, 102–111. [Google Scholar] [CrossRef]
- Reed, B.; Bendall, J.C. Rurality as a factor in ambulance use in health emergencies. Australas. J. Paramed. 2015, 12, 1–6. [Google Scholar]
- Hegenberg, K.; Trentzsch, H.; Gross, S.; Prückner, S. Use of pre-hospital emergency medical services in urban and rural municipalities over a 10 year period: An observational study based on routinely collected dispatch data. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 35. [Google Scholar] [CrossRef]
- Evans, C.S.; Platts-Mills, T.F.; Fernandez, A.R.; Grover, J.M.; Cabanas, J.G.; Patel, M.D.; Vilke, G.M.; Brice, J.H. Repeated emergency medical services use by older adults: Analysis of a comprehensive statewide database. Ann. Emerg. Med. 2017, 70, 506–515.e503. [Google Scholar] [CrossRef]
- Stripe, S.C.; Susman, J. A rural-urban comparison of prehospital emergency medical services in Nebraska. J. Am. Board Fam. Pr. 1991, 4, 313–318. [Google Scholar]
- Shah, M.N.; Cushman, J.T.; Davis, C.O.; Bazarian, J.J.; Auinger, P.; Friedman, B. The epidemiology of emergency medical services use by children: An analysis of the National Hospital Ambulatory Medical Care Survey. Prehosp. Emerg. Care 2008, 12, 269–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansari, S.; Akhdar, F.; Mandoorah, M.; Moutaery, K. Causes and effects of road traffic accidents in Saudi Arabia. Public Health 2000, 114, 37–39. [Google Scholar] [CrossRef]
- Alanazy, A.R.M.; Wark, S.; Fraser, J.; Nagle, A. Factors impacting patient outcomes associated with use of emergency medical services operating in urban versus rural areas: A systematic review. Int. J. Environ. Res. Public Health 2019, 16, 1728. [Google Scholar] [CrossRef] [Green Version]
- Byrne, J.P.; Mann, N.C.; Dai, M.; Mason, S.A.; Karanicolas, P.; Rizoli, S.; Nathens, A.B. Association between emergency medical service response time and motor vehicle crash mortality in the United States. JAMA Surg. 2019, 154, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Alanazi, A.F. Emergency medical services in Saudi Arabia: A study on the significance of paramedics and their experiences on barriers as inhibitors of their efficiency. Int. J. Appl. Basic Med. Res. 2012, 2, 34–37. [Google Scholar] [CrossRef] [Green Version]
- Nanne, B.; Maarten, K.; Charlotte, V.; Plass, A.M. Ambulance Care in Europe; Netherlands Institute for Health Services Research: Utrecht, The Netherlands, 2015; pp. 17–18. ISBN 978-94-6122-368-5. [Google Scholar]
- Bürger, A.; Wnent, J.; Bohn, A.; Jantzen, T.; Brenner, S.; Lefering, R.; Seewald, S.; Gräsner, J.-T.; Fischer, M. The effect of ambulance response time on survival following out-of-hospital cardiac arrest: An analysis from the German resuscitation registry. Dtsch. Ärzteblatt Int. 2018, 115, 541–548. [Google Scholar]
- Pell, J.P.; Sirel, J.M.; Marsden, A.K.; Ford, I.; Cobbe, S.M. Effect of reducing ambulance response times on deaths from out of hospital cardiac arrest: Cohort study. BMJ 2001, 322, 1385–1388. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.D.; Ong, M.E.H.; Tanaka, H.; Ma, M.H.-M.; Nishiuchi, T.; Alsakaf, O.; Karim, S.A.; Khunkhlai, N.; Lin, C.-H.; Song, K.J.; et al. Comparison of Emergency Medical Services Systems Across Pan-Asian Countries: A Web-based Survey. Prehosp. Emerg. Care 2012, 16, 477–496. [Google Scholar] [CrossRef]
- National Health Services (UK). When to Call 999. Available online: https://www.nhs.uk/using-the-nhs/nhs-services/urgent-and-emergency-care/when-to-call-999/ (accessed on 3 July 2020).
- Singapore Civil Defence Force. Fire, Emergency Medical Services and Enforcement Statistics 2018. Available online: https://www.scdf.gov.sg/docs/default-source/scdf-library/amb-fire-inspection-statistics/scdf-annual-statistics-2018.pdf (accessed on 1 July 2020).
- Snooks, H.; Williams, S.; Crouch, R.; Foster, T.; Hartley-Sharpe, C.; Dale, J. NHS emergency response to 999 calls: Alternatives for cases that are neither life threatening nor serious. BMJ 2002, 325, 330–333. [Google Scholar] [CrossRef] [Green Version]
- Segal, E.; Verter, V.; Colacone, A.; Afilalo, M. The in-hospital interval: A description of EMT time spent in the emergency department. Prehosp. Emerg. Care 2006, 10, 378–382. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Category | Terminology/Abbreviation | Definition |
|---|---|---|
| Geographical areas | Rural areas | Areas that have a total population of fewer than 5000 inhabitants or an area outside the categorized urban areas. |
| Urban areas | Areas where metropolitan, and micropolitan cities are located and that have a total population of equal or more than 5000 inhabitants. An example of the largest urban area is Riyadh, the capital of Saudi Arabia, and it has a total population of 5,271,991. | |
| Ambiguous | Areas that could not be categorized into rural or urban (e.g., on a highway) or a combination of unavailable or invalid data in the database. | |
| Age category | Child | Patients with an age below 15 years. |
| Adult | Patients equal to, or over 15 years, but younger than 60 years old. | |
| Elderly | Patient over 60 years of age. | |
| Types of Emergency cases | Medical emergency | Sudden medical emergency illness of any type requiring immediate intervention because human physiology was severely affected. Examples are chest pain, bronchial asthma, coma, and Out-of-Hospital Cardiac Arrest. |
| Traumatic emergency | Sudden severe emergency injury of any type caused by blunt or sharp objects such as Road Traffic Accident (RTA), falling from a high building, and work injury. | |
| Psychological emergency | Acute and sudden disturbance of patient’s behavior and attitude, which if not treated soon, could result in patients harming themselves, family, or the community surrounding them. | |
| Gynecological emergency | Sudden condition relating to the female reproductive system that affects the woman’s lives, such as abortion, vaginal bleeding, or complications during childbirth. | |
| Prehospital non-emergency | Minor medical illness or injury that occurred without disturbing vital signs and does not need immediate intervention by prehospital EMS providers and can be treated by the general practitioners, such as seasonal flu and tensional headache. | |
| SRCA levels of urgency | High urgent cases | Any life- threatening emergency calls such as cardiac arrest, severe traumatic injuries, or cerebral stroke that requires immediate advanced life support intervention and is given the highest priority for the crews to be dispatched for them by SRCCAD in the CC. |
| Medium urgent cases | A group of medical and other illnesses and traumatic injuries such as febrile convulsion, psychological attack, alcoholism, uncomplicated diabetic prioritized by SRCCAD and take the second priority if the life-threatening cases calls come together at the same moment. | |
| Low/non-urgent cases | A group of mild medical illnesses and minor injuries such as the common cold, mild muscular pain that does not affect the human body physiology and therefore, does not require immediate medical intervention, which in turn can be categorized by SRCCAD as a tertiary priority. | |
| Time period of emergency medical services | Response time | The time elapsed starting from receiving a call in the CC and ended by the arrival of the ambulance’s crew to the scene. |
| Total EMS time | The total time measured starting from receiving the call in the CC and ending with the ambulance handover of the patient to the emergency department staff in the hospital. | |
| Outcome of emergency service missions | Completed missions | The mission that is activated by the CC when the emergency services are requested by the emergency caller, and then the EMS crew arrived at the caller address and ended either by non-conveyance or transportation to the healthcare facility. |
| Types of completed missions | 1- Non-conveyance missions: the condition where the ambulances arrived at the scene and the patients after having been examined or treated on the scene, transport to the health facility is not necessary or is refused by the patient. 2- Transported mission: as an ambulance transported the patient from the scene to the hospitals’ emergency department. | |
| Aborted missions | The decision that made by CC to stop the dispatched ambulance crew from continuing their mission toward scene due to reasons such as cancellation by a caller, wrong geographical areas, false alarm or the nominated crews being far from the patient. | |
| Missions period | Working time | The time that starts from 8:00 AM to 4:00 PM from Sunday to Thursday. |
| Rest time | The time that starts from 4:01 PM on the same day up to next day 7:59 AM side by side with 48. 00 h of the weekend Friday and Saturday. | |
| Crew dispatched at the scene | Crews dispatched to urban areas | Two professional EMS staff who dispatched from urban GAC by one of the following vehicles: Mobile Intensive Care Unit, Non-transporting Fast Responding Vehicle, or Ambulance type II to urban areas and might rarely participate in close rural areas if the SRCCAD nominated them due to a shortage of staff in the rural area. |
| Crews dispatched to rural areas | Two professional EMS staff dispatched from rural GAC by Ambulance type II to rural areas and might rarely participate in close urban areas if the SRCCAD nominated them due a shortage of staff in the urban area. | |
| EMS crew’s arrival to scene | Primary crews | The qualified EMS personnel who were dispatched by the dispatch department in the CC to first arrive by any vehicle and contacting the patient upon arrival at the scene. |
| Secondary crews | The qualified EMS personnel who were dispatched to the scene and arrived afterwards by another ambulance vehicle to support the first crews that arrived earlier. | |
| Health care facility | Governmental | Non-profit healthcare services that are provided and funded by the Saudi government through the ministry of health, university hospitals, military hospitals, and security hospitals, and national guard hospitals for all Saudi citizens. |
| Private | Hospitals, or primary healthcare centers that are not free-of-charge and are operated by non-governmental healthcare firms. | |
| Call center (CC) | The workforce consisting of different office disks operated by professional staff who are able to communicate with the emergency caller and are also able to operate software of SRCCAD and the telecommunication apparatus. | |
| Ground Ambulance Center (GAC) | The EMS facilities including all structural logistic elements such vehicles, medical equipment, telecommunication machines, and EMS providers. | |
| List of abbreviation and definition | OHCA | Out of hospital cardiac arrest: stopping of cardiac pulse activity, confirmed by the absence of signs of circulation outside the hospital field [19]. |
| RTA | Road Traffic Accident is an accident that occurs on the road without prior planning by any one of the involved parties and leads to death, or temporary or permanent disability. | |
| SRCA | The Saudi Red Crescent Authority, which is considered to be the main EMS provider for prehospital emergency healthcare in Saudi Arabia. | |
| SRCCAD | The out-of-hospital information system, designed by Saudi programmers, which includes all relative structural information needed to connect all resources in order to respond properly to patients with different emergency types linked to already designated priorities. | |
| Category | Categorization | Mission (n = 146,639) | Population (n = 6,792,776) (100%) | N of Calls’ Missions per 1000 |
|---|---|---|---|---|
| Missions | All Missions | 146,639 (100%) | 6,792,776 (100%) | 21.6 |
| Transported | 67,068 (45.7%) | 6,792,776 (100%) | 9.9 | |
| Non-conveyance | 79,571 (54.3%) | 6,792,776 (100%) | 11.7 | |
| Sex | Male | 83,702 (57.1%) | 3,995,352 (58.8%) | 21.0 |
| Female | 42,893 (29.3%) | 2,797,424 (41.2%) | 15.3 | |
| Unknown a | 20,044 (13.7%) | NA | NA | |
| Age category b | Child (<15 years.) | 5034 (3.4%) | 1,782,648 (26.2%) | 2.8 |
| Non-elderly adult (15–59) | 73,528 (50.1%) | 4,794,176 (70.5%) | 15.3 | |
| Elderly (≥60 years) | 37,662 (25.7%) | 215,952 (3%) | 174.4 | |
| Unknown a | 30,415 (20.7%) | NA | NA | |
| Call geographical areas c | Urban | 137,347 (93.7%) | 6,213,184 (91.5%) | 22.1 |
| Rural | 6487 (4.4%) | 579,592 (8.5%) | 11.2 | |
| Ambiguous | 2805 (1.9%) | NA | NA |
| Category | Geographical Areas | ||||
|---|---|---|---|---|---|
| Urban n (%) | Rural n (%) | Total n (%) | p-Value | ||
| Sex | Male | 62,511 (56.7) | 3405 (56.7) | 65,916 (56.7) | |
| Female | 33,124 (30.1) | 638 (10.6) | 33,762 (29.1) | <0.001 | |
| Unknown b | 14,551 (13.2) | 1960 (32.7) | 16,511 (13.7) | ||
| Age category | Child (<15 years.) | 3715 (4.2) | 155 (5.0) | 3870 (4.2) | |
| Non-elderly adult (15–60) | 55,635 (62.5) | 2330 (75.3) | 57,965 (62.9) | <0.001 | |
| Elderly (≥60 years.) | 29,708 (33.4) | 609 (19.7) | 30,317 (32.9) | ||
| Mission period | Rest Time | 82,590 (75.0) | 4592 (76.5) | 87,182 (75.2) | <0.001 |
| Working Time | 27,596 (25.0) | 1411 (23.5) | 29,007 (24.8) | ||
| Emergency reasons for calls | Medical Emergency | 44,404 (40.3) | 1361 (22.7) | 45,765 (39.4) | |
| Trauma | 29,290 (26.6) | 3244 (54.0) | 32,534 (28.0) | ||
| Psycho-psychiatric Emergency | 929 (0.8) | 9 (0.1) | 938 (0.8) | <0.001 | |
| Gynecological Emergency | 1171 (1.1) | 18 (0.3) | 1206 (1.0) | ||
| Non-emergency | 32,943 (29.9) | 1302 (21.7) | 34,245 (29.5) | ||
| Others c | 1449 (1.3) | 69 (1.1) | 1518 (1.3) | ||
| Urgency levels | High Urgency Level Cases | 55,967 (50.8) | 4068 (67.8) | 60,035 (51.7) | |
| Medium Urgency Level Cases | 19,677 (17.9) | 553 (9.2) | 20,230 (17.4) | <0.001 | |
| Low Urgency Level Cases | 34,542 (31.3) | 1382 (23.0) | 35,924 (30.9) | ||
| Mission outcome | Non-conveyance | 59,319 (53.8) | 2383 (39.7) | 61,702 (53.1) | <0.001 |
| Transported to Healthcare Facility | 50,867 (46.2) | 3620 (60.3) | 54,487 (46.9) | ||
| Urgency Levels of EMS Missions | Urban | Rural | p-Value | |
|---|---|---|---|---|
| All Missions | Number of cases | 108,732 | 5934 | |
| Median (IQR) | 17.0 (11.8,23.9) | 17.6 (9.8,28.6) | <0.001 | |
| High urgent (overall) | Number of cases | 54,726 | 3983 | |
| Median (IQR) | 15.8 (11.2,21.8) | 19.0 (11.7,30.0) | <0.001 | |
| High urgent medical | Number of cases | 35,172 | 1138 | |
| Median (IQR) | 16.1 (11.5,22.2) | 16.2 (8.6,26.7) | <0.001 | |
| High urgent trauma | Number of cases | 19,074 | 2840 | |
| Median (IQR) | 15.2 (10.7,21.7) | 20.2 (12.9,30.9) | <0.001 | |
| High urgent for others a | Number of cases | 480 | 5 | |
| Median (IQR) | 17.0 (12.8,23.0) | 16.9 (6.2,25.5) | 0.700 | |
| Moderate urgent (overall) | Number of cases | 21,032 | 649 | |
| Median (IQR) | 16.38 (11.7,22.6) | 15.43 (8.8,25.4) | <0.018 | |
| Moderate urgent medical | Number of cases | 9196 | 223 | |
| Median (IQR) | 15.91 (11.56,21.7) | 15.95 (10.1,28.2) | <0.001 | |
| Moderate urgent trauma | Number of cases | 10,216 | 404 | |
| Median (IQR) | 16.53 (11.7,22.9) | 15.38 (7.0,24.8) | <0.001 | |
| Moderate urgent for others b | Number of cases | 1620 | 22 | |
| Median (IQR) | 18.4 (13.0,25.8) | 10.65 (8.6,21.6) | 0.470 | |
| Low non-emergency cases | Number of cases | 32,974 | 1302 | |
| Median (IQR) | 20.0 (13.6,28.4) | 13.6 (3.5,24.9) | <0.001 | |
| Urgency Levels of EMS Cases | All Locations n (%) | Urban n (%) | Rural n (%) | p-Value |
|---|---|---|---|---|
| Overall EMS cases | 71,571 (62.4) | 68,680 (62.3) | 3391 (56.5) | <0.001 |
| Highly urgent medical emergency | 24,557 (67.6) | 23,861 (67.8) | 696 (61.2) | <0.001 |
| Highly urgent traumatic emergency | 15,001 (68.5) | 13,604 (71.3) | 1397 (49.2) | <0.001 |
| Moderately urgent medical emergency | 6506 (69.1) | 6363 (69.2) | 143 (64.1) | 0.110 |
| Moderately urgent traumatic emergency | 6946 (65.4) | 6689 (65.5) | 257 (63.6) | 0.440 |
| Low non-emergency cases | 17,284 (50.5) | 16,432 (49.9) | 852 (65.4) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moafa, H.N.; van Kuijk, S.M.J.; Alqahtani, D.M.; Moukhyer, M.E.; Haak, H.R. Disparities between Rural and Urban Areas of the Central Region of Saudi Arabia in the Utilization and Time-Centeredness of Emergency Medical Services. Int. J. Environ. Res. Public Health 2020, 17, 7944. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17217944
Moafa HN, van Kuijk SMJ, Alqahtani DM, Moukhyer ME, Haak HR. Disparities between Rural and Urban Areas of the Central Region of Saudi Arabia in the Utilization and Time-Centeredness of Emergency Medical Services. International Journal of Environmental Research and Public Health. 2020; 17(21):7944. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17217944
Chicago/Turabian StyleMoafa, Hassan N., Sander Martijn Job van Kuijk, Dhafer M. Alqahtani, Mohammed E. Moukhyer, and Harm R. Haak. 2020. "Disparities between Rural and Urban Areas of the Central Region of Saudi Arabia in the Utilization and Time-Centeredness of Emergency Medical Services" International Journal of Environmental Research and Public Health 17, no. 21: 7944. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17217944