Health Care Needs and Services for Elder and Disabled Population: Findings from a Barcelona Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Datasets
2.2. Analysis Techniques
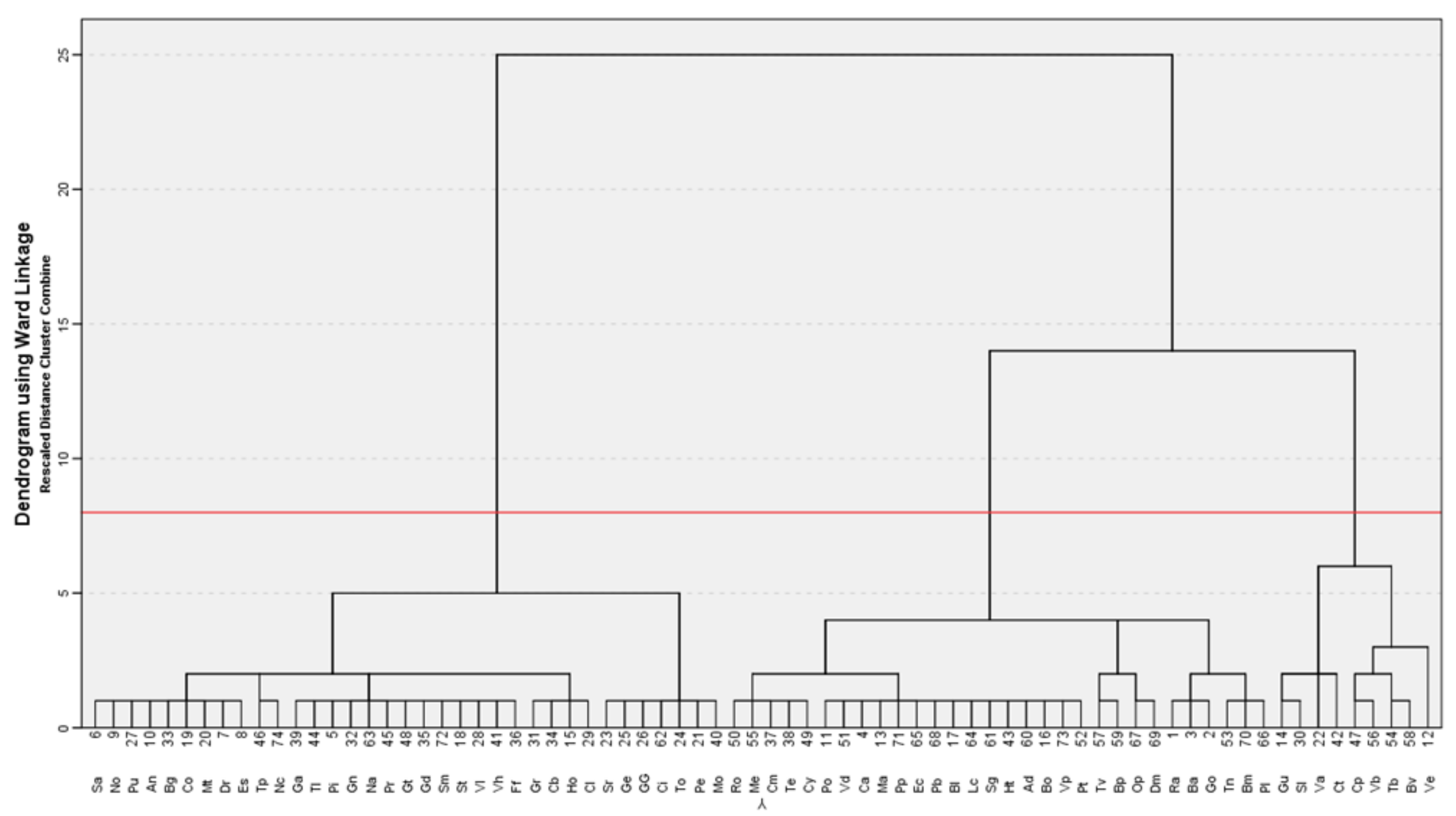
2.2.1. Cluster Analysis (ClA)
2.2.2. Multidimensional Scaling (MDS)
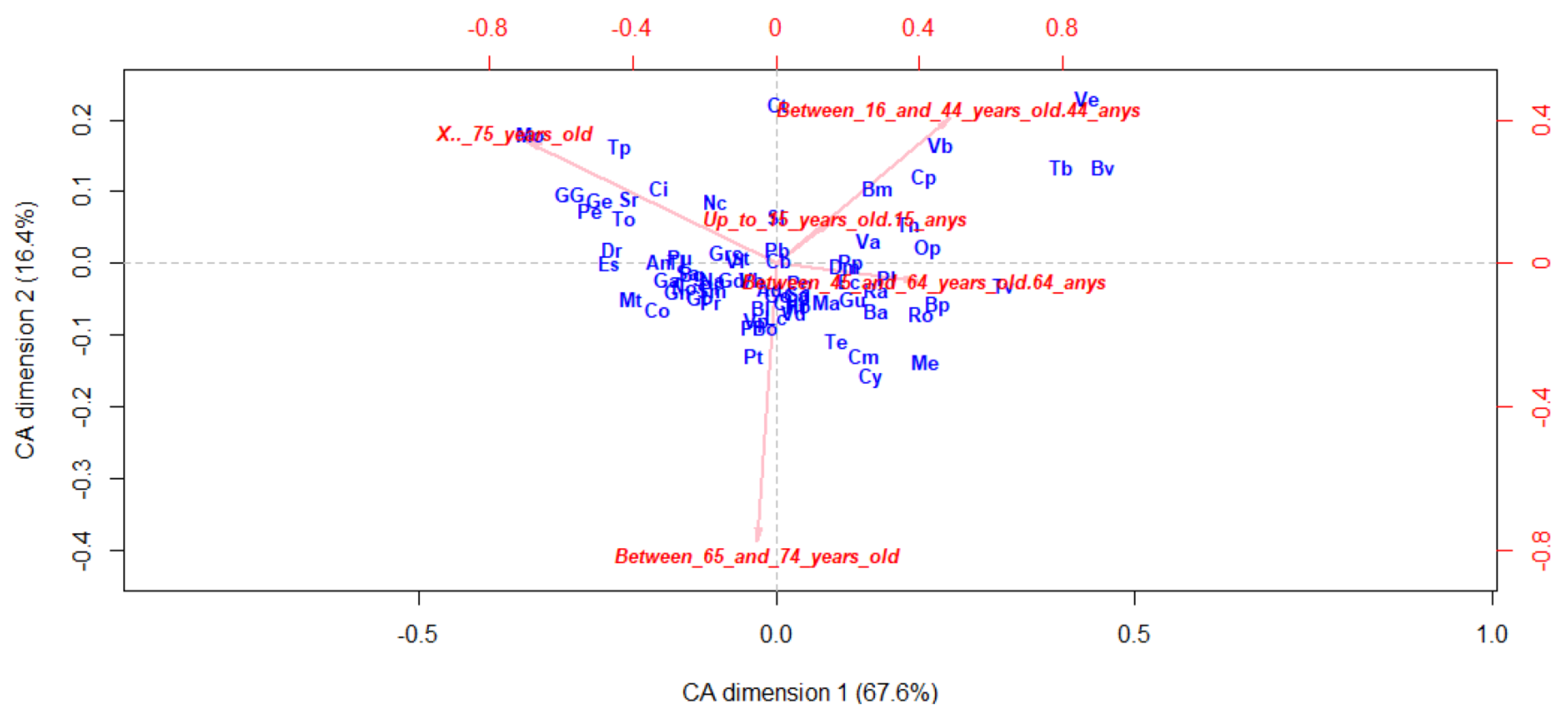
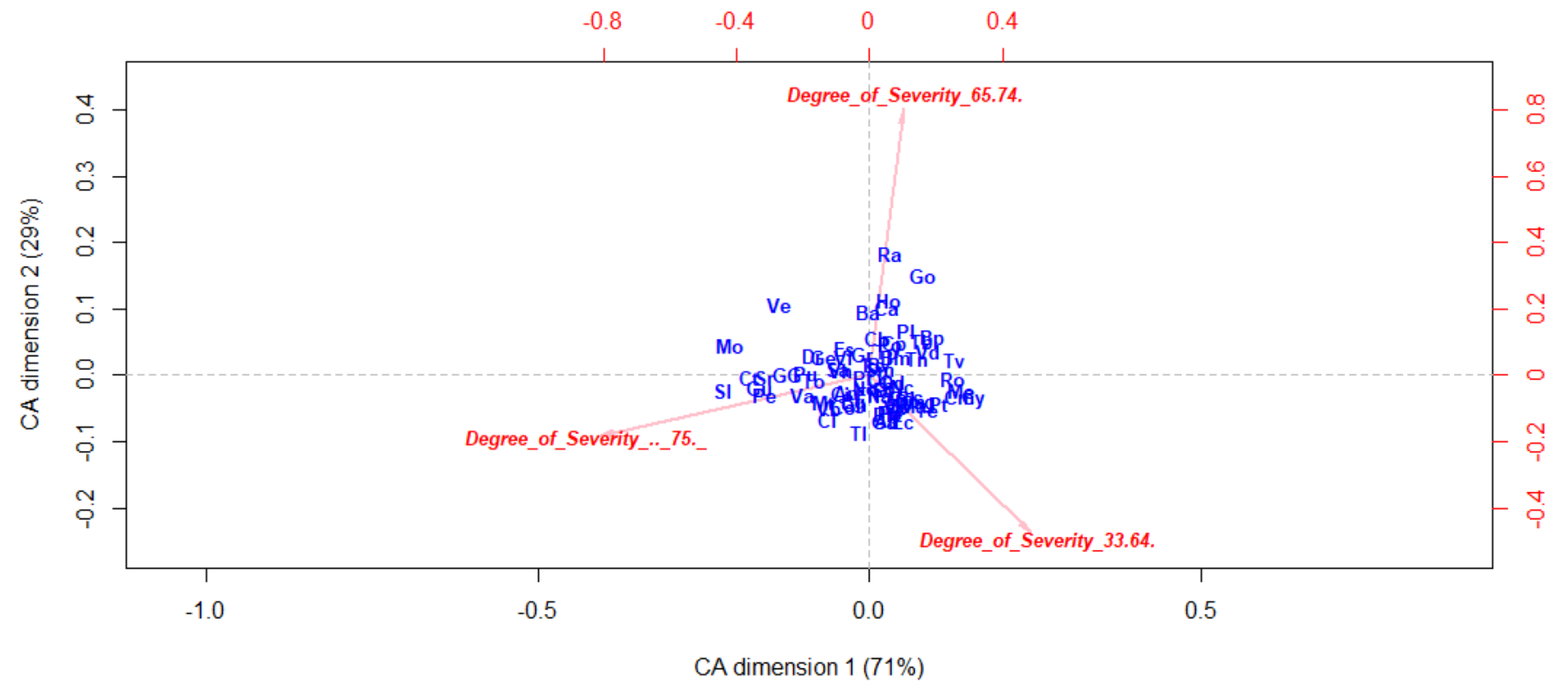
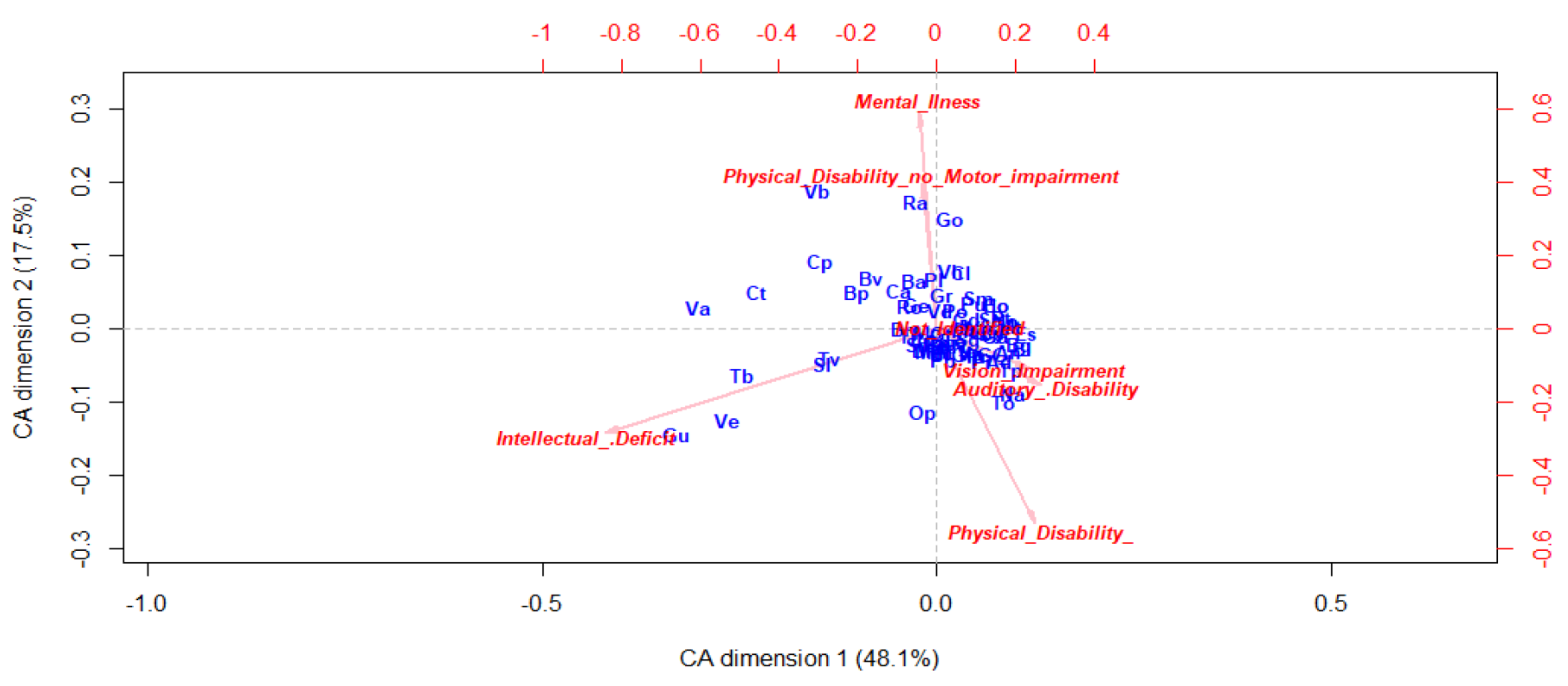
2.2.3. Correspondence Analysis (CA)
2.2.4. Principal Component Analysis (PCA)
2.2.5. Multiple Regression (MR)
3. Results
3.1. Elderly and Disabled Health Care Demand
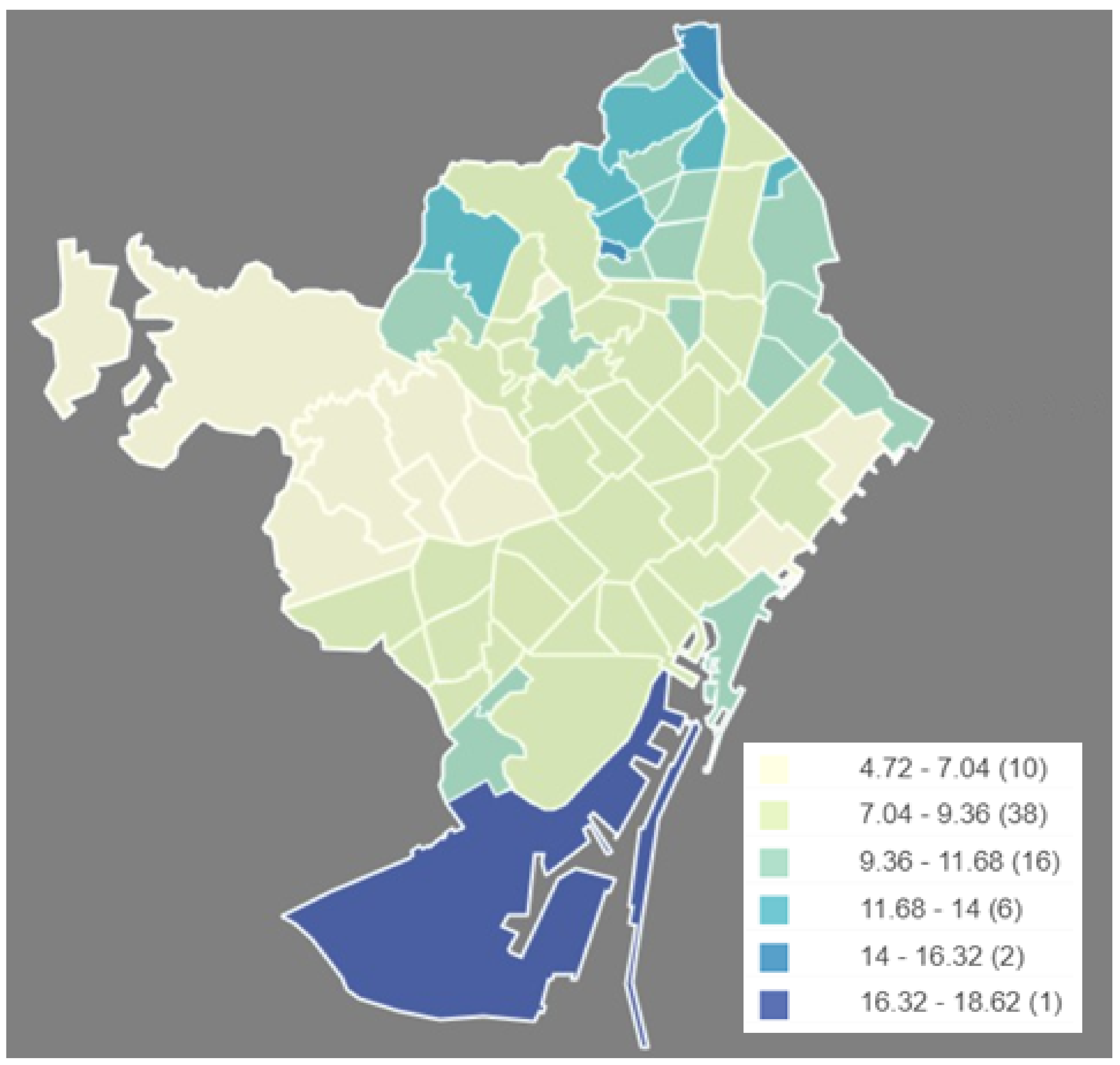
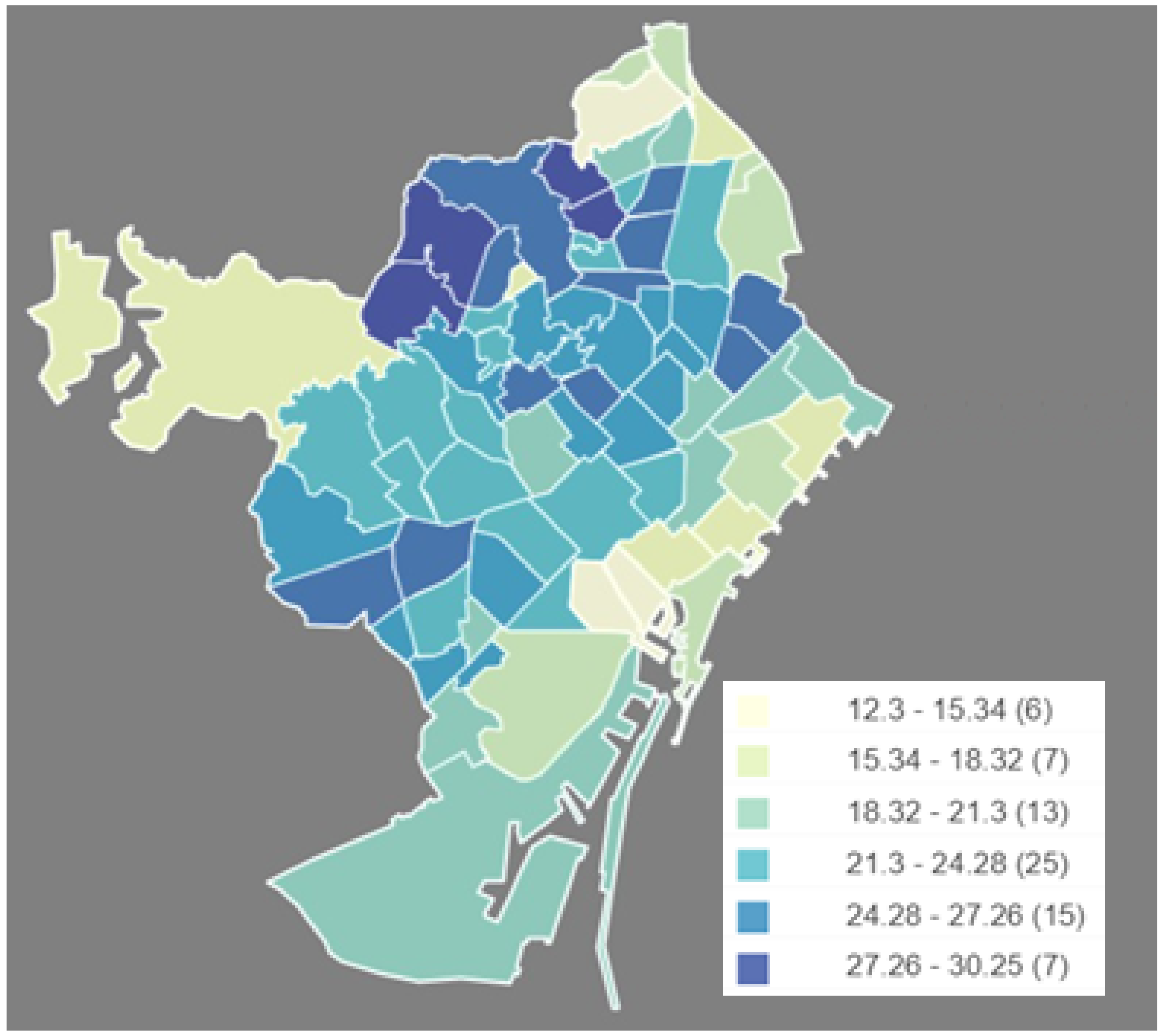
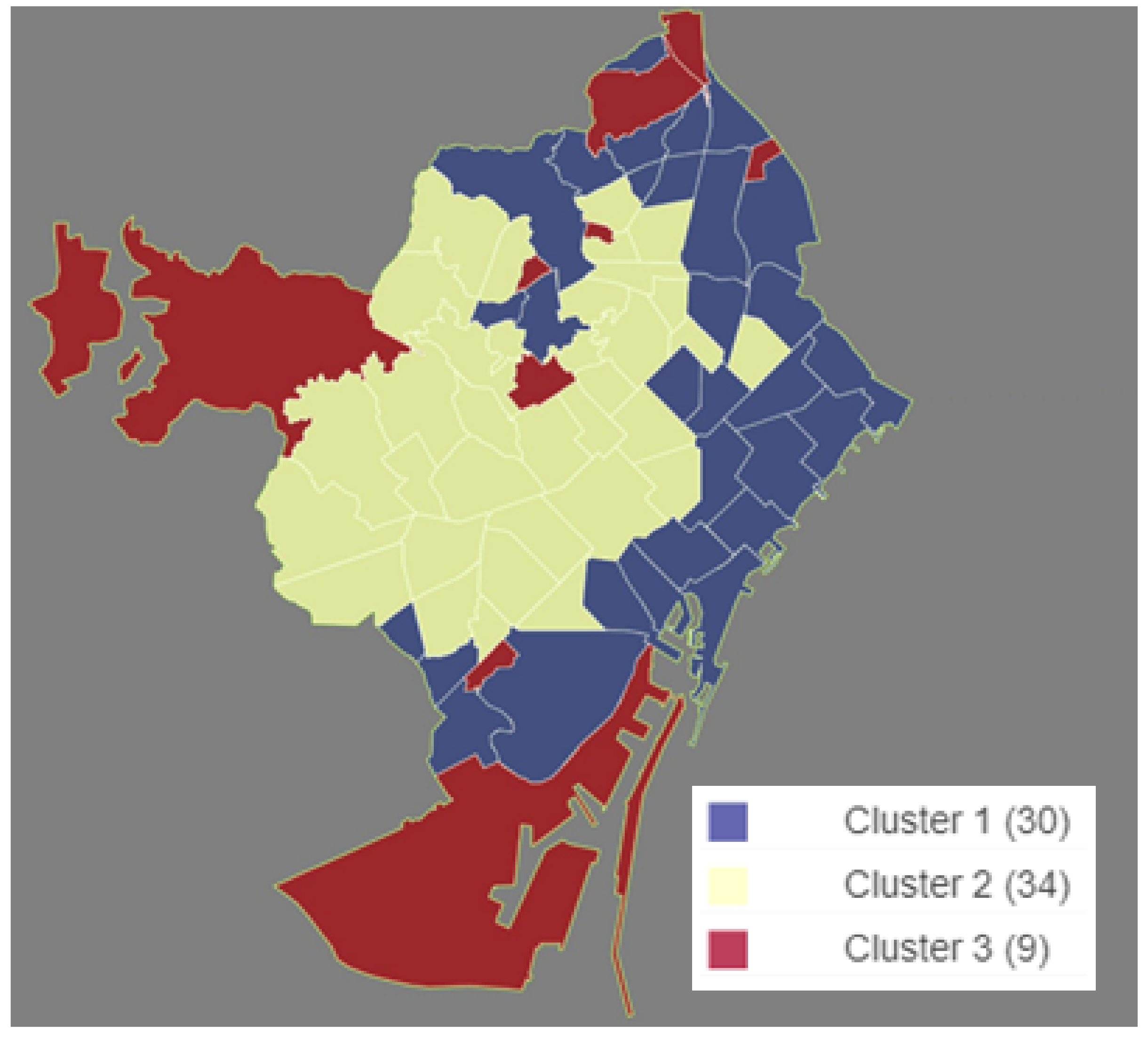
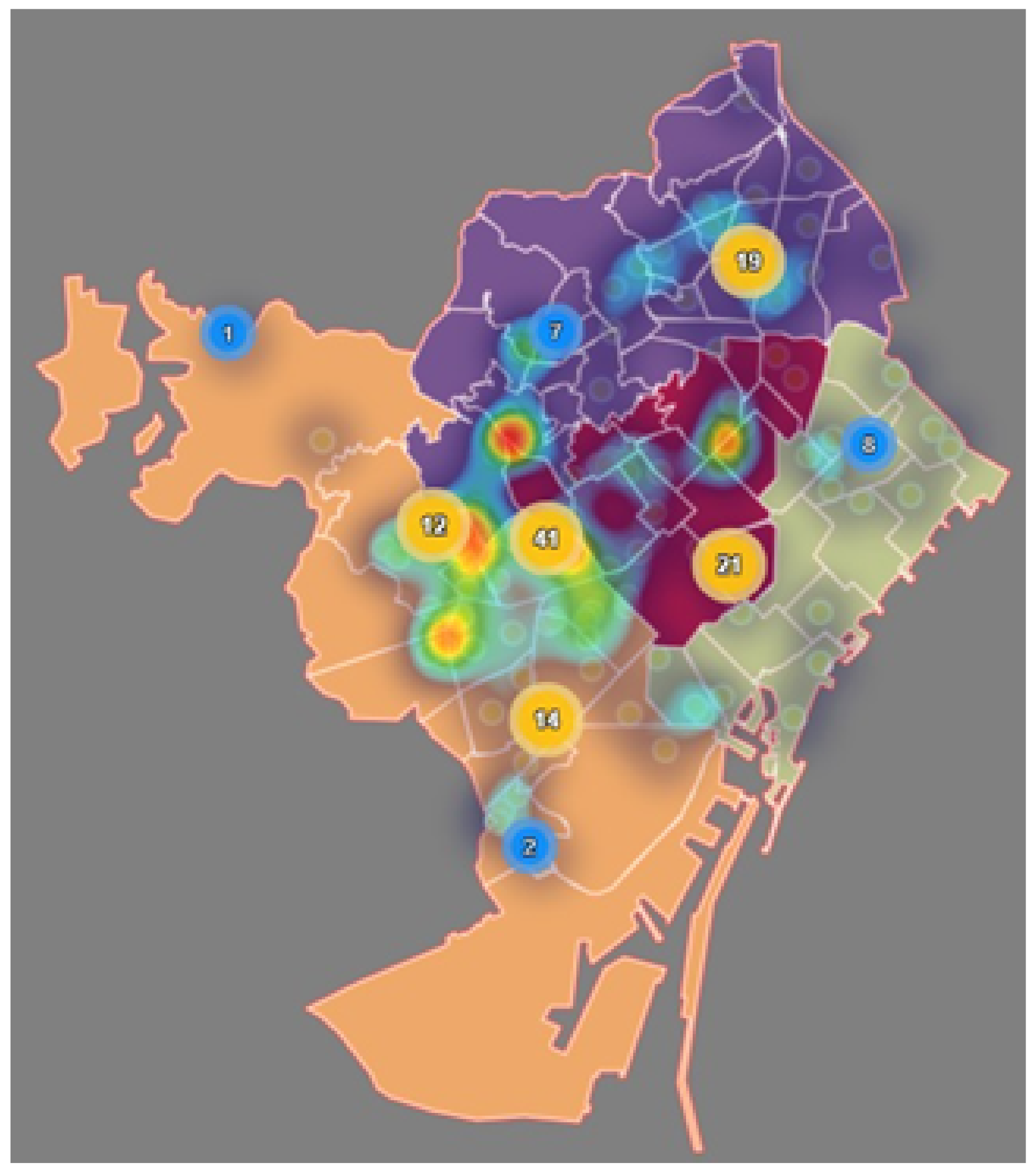
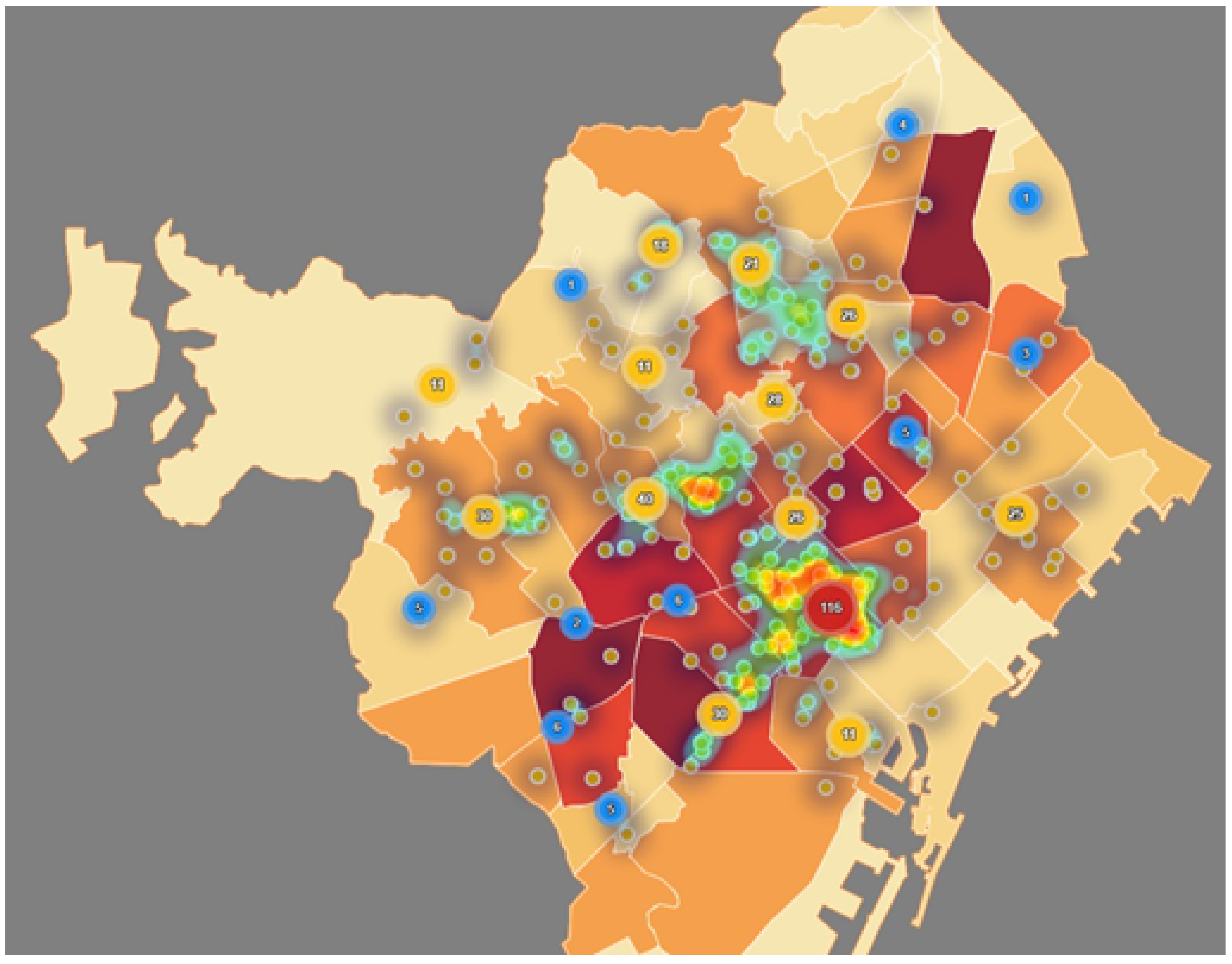
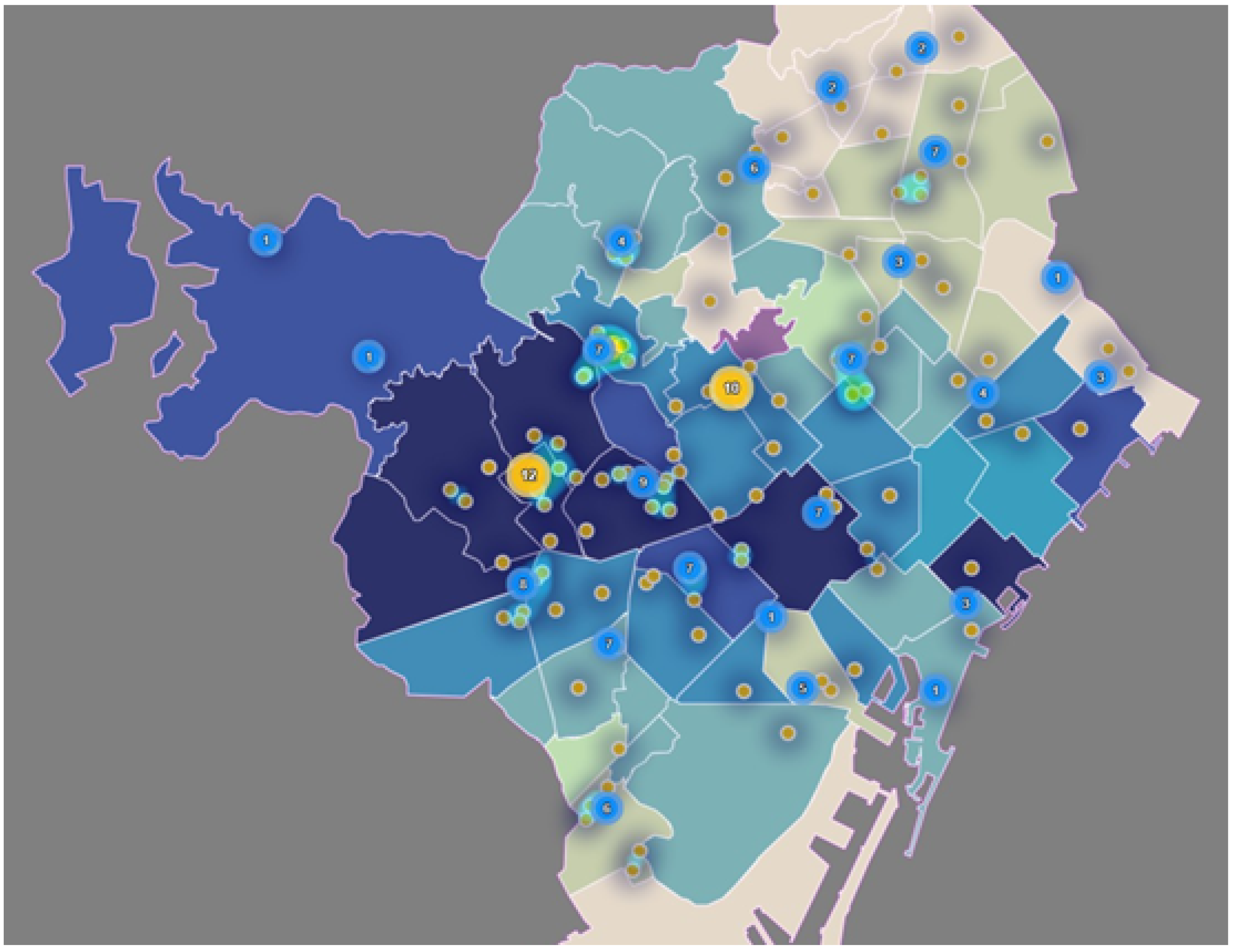
3.1.1. Mapping the Neighborhoods
3.1.2. Segmentation of the Neighborhoods through Disabled Demographics
3.1.3. Hierarchical Clustering
3.1.4. Robustness Validation
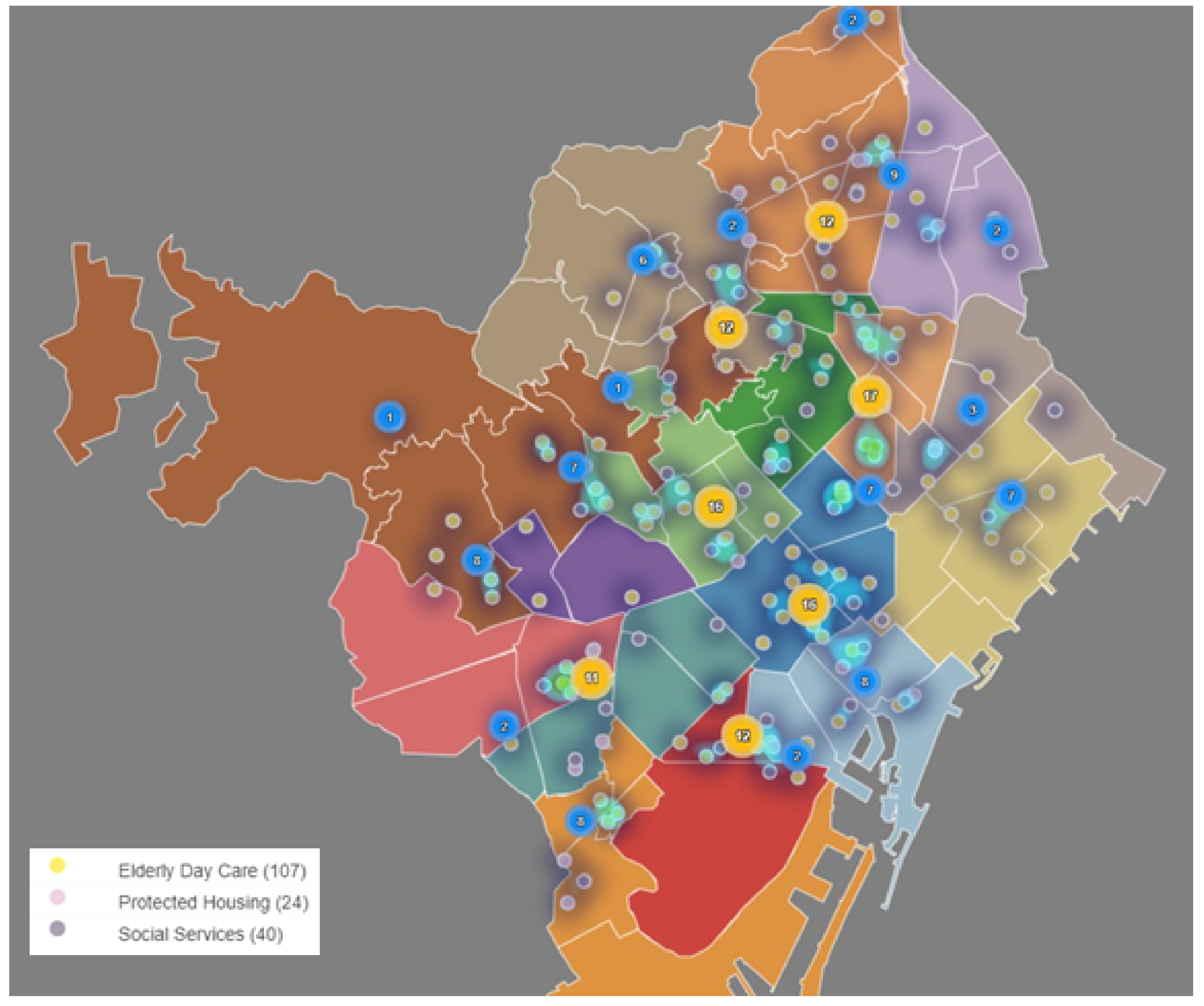
3.2. Health Care Service
3.2.1. AIS—Integral Health Areas
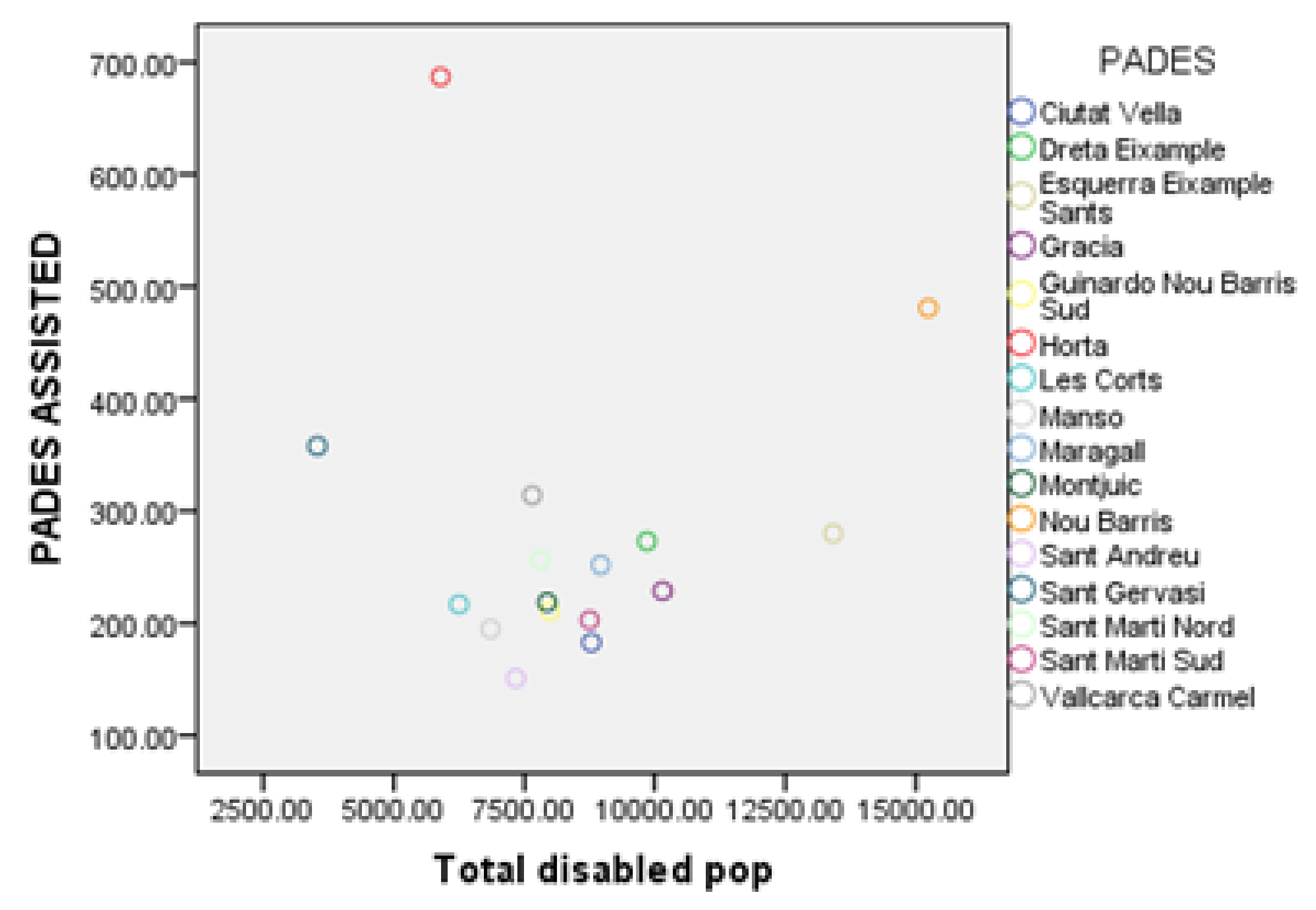
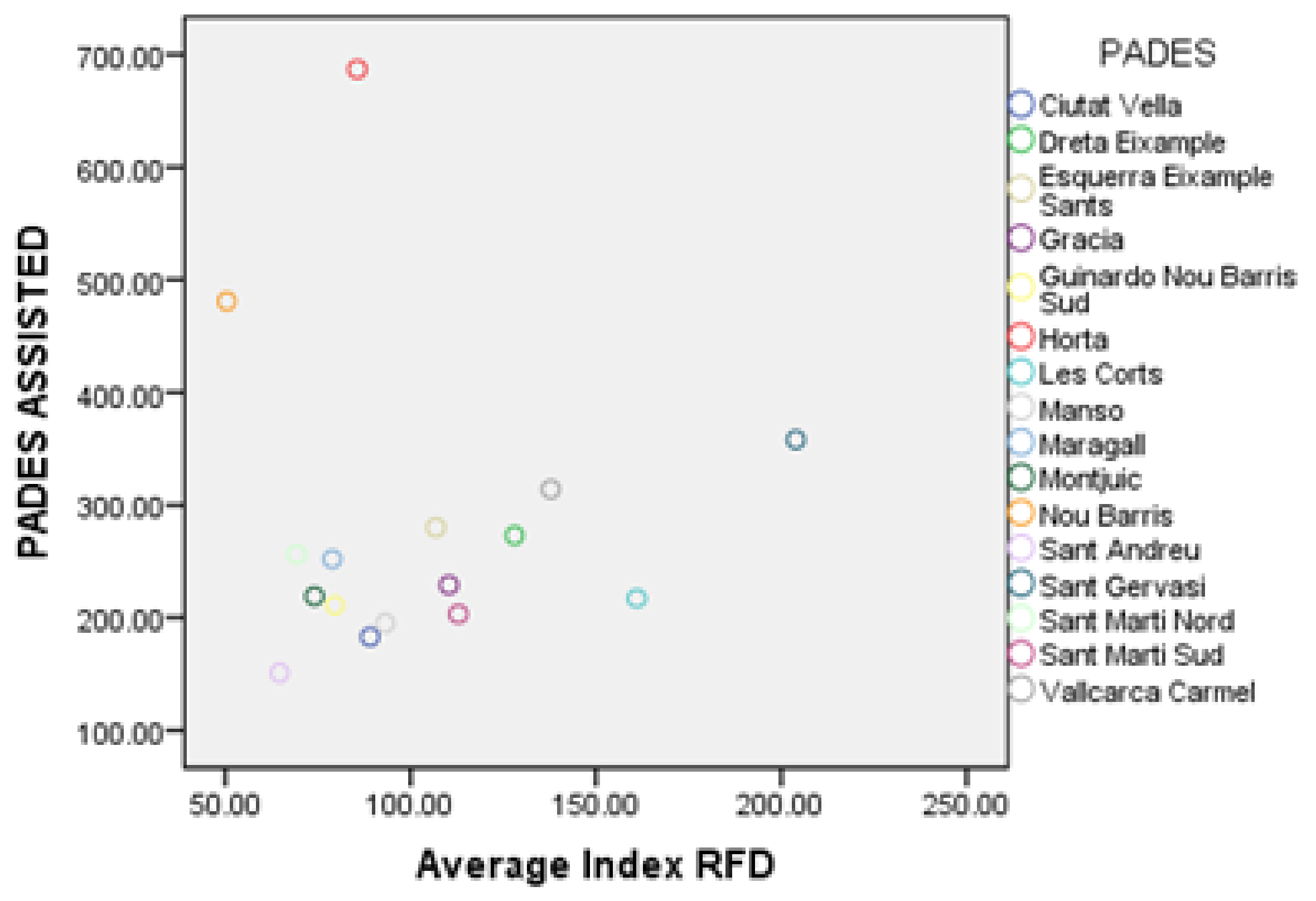
3.2.2. PADES—Home Care Program
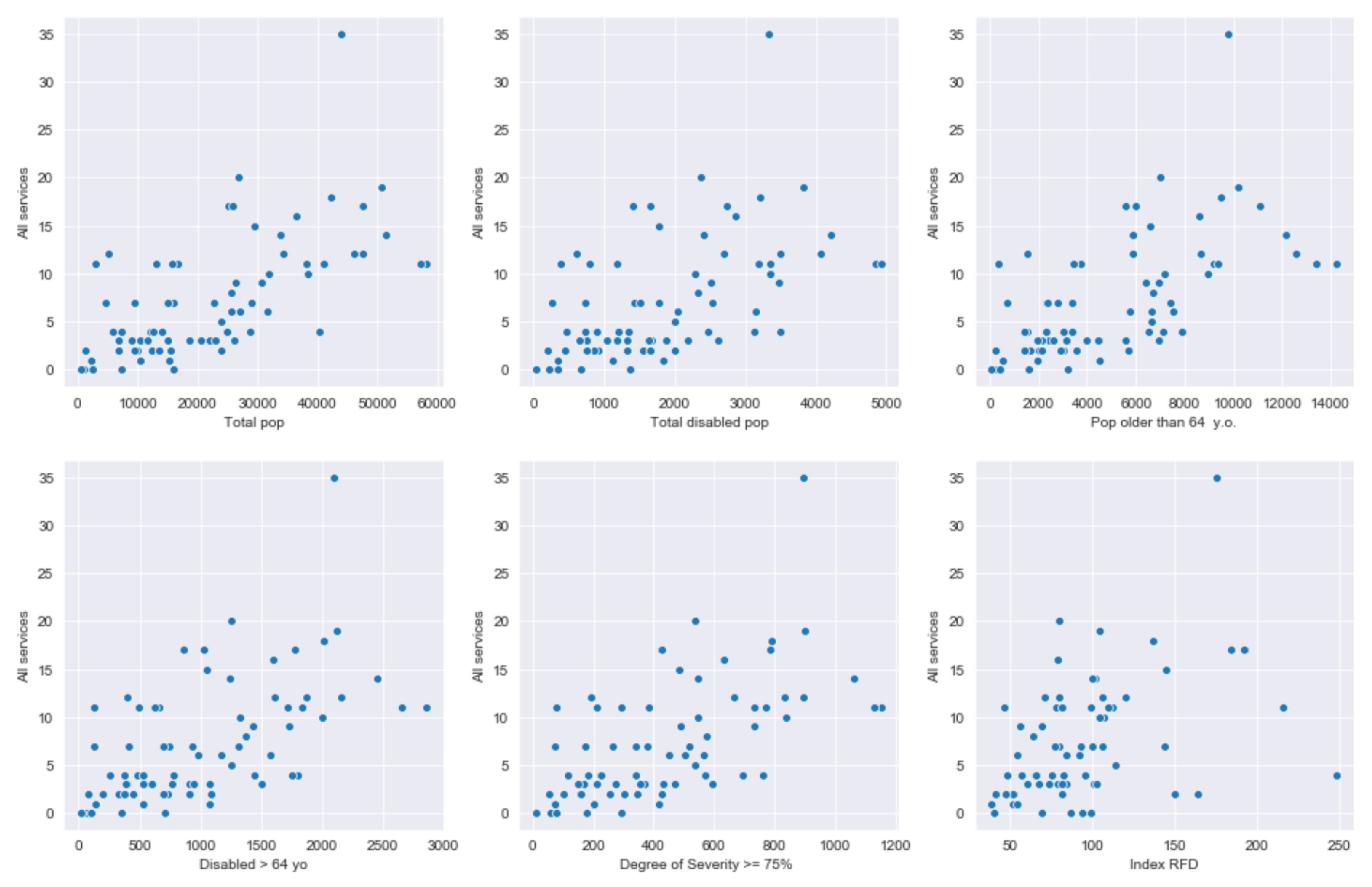
3.3. Relationship between Demand and Service
3.3.1. Assessment by Neighborhoods
3.3.2. Assessment by PADES Area
3.3.3. Assessment by AIS
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ABS | Basic Health Areas |
| AIS | Integral Health Areas |
| CA | Correspondence Analysis |
| CAP | Primary Health Care Center |
| CLA | Cluster Analysis |
| MDS | Multidimensional Scaling |
| MR | Multiple Regression |
| PADES | Home Care Program |
| PADRIS | Public Data Analysis for Health Research and Innovation Program |
| PCA | Principal Component Analysis |
| RFD | Family Income Available |
Appendix A. Population Distribution by Neighborhood

Appendix B. Health Care Service Area Distributions


Appendix C. PADES Regression Results

References
- Ramudhin, A.; Chan, E.; Mokadem, A. A Framework for the Modelling, Analysis and Optimization of Pathways in Healthcare. In Proceedings of the 2006 International Conference on Service Systems and Service Management, Troyes, France, 25–27 October 2006; Volume 1, pp. 698–702. [Google Scholar]
- Baetan, R.S.S.; Vanhercke, B.; Coster, S. Inequalities in Access to Healthcare: A Study of National Policies; European Comission: Brussels, Belgium, 2018. [Google Scholar]
- Landers, S.; Madigan, E.; Leff, B.; Rosati, R.J.; McCann, B.A.; Hornbake, R.; MacMillan, R.; Jones, K.; Bowles, K.; Dowding, D.; et al. The Future of Home Health Care: A Strategic Framework for Optimizing Value. Home Health Care Manag. Prac. 2016, 28, 262–278. [Google Scholar] [CrossRef] [Green Version]
- Buron, A.; Cots, F.; Garcia, O.; Vall, O.; Castells, X. Hospital emergency department utilisation rates among the immigrant population in Barcelona, Spain. BMC Health Serv. Res. 2008, 8, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waibel, S.; Vargas, I.; Aller, M.B.; Coderch, J.; Farré, J.; Vázquez, M.L. Continuity of clinical management and information across care levels: Perceptions of users of different healthcare areas in the Catalan national health system. BMC Health Serv. Res. 2016, 16, 466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waibel, S.; Vargas, I.; Coderch, J.; Vázquez, M.L. Correction to: Relational continuity with primary and secondary care doctors: A qualitative study of perceptions of users of the Catalan national health system. BMC Health Serv. Res. 2018, 18, 436. [Google Scholar] [CrossRef] [PubMed]
- Aller, M.B.; Vargas, I.; Coderch, J.; Vázquez, M.L. Doctors’ opinion on the contribution of coordination mechanisms to improving clinical coordination between primary and outpatient secondary care in the Catalan national health system. BMC Health Serv. Res. 2017, 17, 842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baltaxe, E.; Cano, I.; Herranz, C.; Barberan-Garcia, A.; Hernandez, C.; Alonso, A.; Arguis, M.J.; Bescos, C.; Burgos, F.; Cleries, M.; et al. Evaluation of integrated care services in Catalonia: Population-based and service-based real-life deployment protocols. BMC Health Serv. Res. 2019, 19, 370. [Google Scholar] [CrossRef] [PubMed]
- Sanitary Consortium of Barcelona. Pla de Salut. 2016. Available online: http://www.csb.cat/plans-informacio-sanitaria/pla-de-salut/ (accessed on 19 March 2020).
- Generalitat de Catalunya Department de Salut. PERIS 2016-2020 The Strategic Plan for Health Research and Innovation. 2016. Available online: http://salutweb.gencat.cat/web/.content/_ambits-actuacio/Linies-dactuacio/Recerca/PERIS-2016-2020/PERIS_2016_2020.pdf (accessed on 19 March 2020).
- Generalitat de Catalunya Agència de Qualitat i Avaluació Sanitàries de Catalunya (AQuAS). Programa Públic D’analitica de Dades per a la Recerca i la Innovaciò en Salut a Catalunya—PADRIS. 2017. Available online: http://aquas.gencat.cat/ca/detall/article/padris (accessed on 19 March 2020).
- Islam, M.; Hasan, M.; Wang, X.; Germack, H.; Noor-E-Alam, M. A Systematic Review on Healthcare Analytics: Application and Theoretical Perspective of Data Mining. Healthcare 2018, 6, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yen, S.M.; Kung, P.T.; Chiu, L.T.; Tsai, W.C. Related factors and use of free preventive health services among adults with intellectual disabilities in Taiwan. BMC Health Serv. Res. 2014, 14, 248. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.T.; Lai, H.Y.; Hwang, I.H.; Ho, M.M.; Hwang, S.J. Home healthcare services in Taiwan: A nationwide study among the older population. BMC Health Serv. Res. 2010, 10, 274. [Google Scholar] [CrossRef] [Green Version]
- Low, L.F.; Yap, M.; Brodaty, H. A systematic review of different models of home and community care services for older persons. BMC Health Serv. Res. 2011, 11, 93. [Google Scholar] [CrossRef] [Green Version]
- Kodner, D.L. Whole-system approaches to health and social care partnerships for the frail elderly: An exploration of North American models and lessons. Health Soc. Care Community 2006, 14, 384–390. [Google Scholar] [CrossRef]
- Gregory, A.; Mackintosh, S.; Kumar, S.; Grech, C. Experiences of health care for older people who need support to live at home: A systematic review of the qualitative literature. Geriatr. Nurs. 2017, 38, 315–324. [Google Scholar] [CrossRef]
- Spiers, G.; Matthews, F.E.; Moffatt, S.; Barker, R.O.; Jarvis, H.; Stow, D.; Kingston, A.; Hanratty, B. Impact of social care supply on healthcare utilisation by older adults: A systematic review and meta-analysis. Age Ageing 2018, 48, 57–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naruse, T.; Matsumoto, H.; Fujisaki-Sakai, M.; Nagata, S. Measurement of special access to home visit nursing services among Japanese disabled elderly people: Using GIS and claim data. BMC Health Serv. Res. 2017, 17, 377. [Google Scholar] [CrossRef]
- Yen, S.M.; Kung, P.T.; Tsai, W.C. Factors associated with free adult preventive health care utilization among physically disabled people in Taiwan: Nationwide population-based study. BMC Health Serv. Res. 2014, 14, 610. [Google Scholar] [CrossRef] [Green Version]
- Vergunst, R.; Swartz, L.; Hem, K.G.; Eide, A.H.; Mannan, H.; MacLachlan, M.; Mji, G.; Braathen, S.H.; Schneider, M. Access to health care for persons with disabilities in rural South Africa. BMC Health Serv. Res. 2017, 17, 741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senghor, D.B.; Diop, O.; Sombié, I. Analysis of the impact of healthcare support initiatives for physically disabled people on their access to care in the city of Saint-Louis, Senegal. BMC Health Serv. Res. 2017, 17, 695. [Google Scholar] [CrossRef] [Green Version]
- Rencher, A.C. A Review of “Methods of Multivariate Analysis, Second Edition”. IIE Trans. 2005, 37, 1083–1085. [Google Scholar] [CrossRef]
- Institut Cartogràfic i Geològic de Catalunya. Instamap. 2019. Available online: https://www.instamaps.cat/#/ (accessed on 19 March 2020).
- Ajuntament de Barcelona. Health. 2019. Available online: https://www.barcelona.cat/en/living-in-bcn/health (accessed on 19 March 2020).
- Municipal Data Office. Dataset Catalogue. 2019. Available online: https://opendata-ajuntament.barcelona.cat/es (accessed on 19 March 2020).
- Ministerio de Trabajo y Asuntos Sociales. Real Decreto 1971/1999, de 23 de Diciembre, de Procedimiento Para el Reconocimiento, Declaración y Calificación del Grado de Minusvalía. Available online: https://www.boe.es/eli/es/rd/1999/12/23/1971 (accessed on 19 October 2020).
- Generalitat de Catalunya. Observatori del Sistema de Salut de Catalunya. Crisi i Salut. 2019. Available online: http://observatorisalut.gencat.cat/ca/observatori-sobre-els-efectes-de-crisi-en-salut (accessed on 19 March 2020).
- Perrier, L.; Buja, A.; Mastrangelo, G.; Baron, P.S.; Ducimetière, F.; Pauwels, P.J.; Rossi, C.R.; Gilly, F.N.; Martin, A.; Favier, B.; et al. Transferability of health cost evaluation across locations in oncology: Cluster and principal component analysis as an explorative tool. BMC Health Serv. Res. 2014, 14, 537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Copenhaver, M.S.; Hu, M.; Levi, R.; Safavi, K.; Langle, A.C.Z. Health System Innovation: Analytics in Action. In Operations Research & Management Science in the Age of Analytics; INFORMS: Catonsville, MD, USA, 2019; Chapter 10; pp. 238–266. [Google Scholar] [CrossRef]
- Combes, C.; Azema, J. Clustering using principal component analysis applied to autonomy–disability of elderly people. Decis. Support Syst. 2013, 55, 578–586. [Google Scholar] [CrossRef]
- Costa, P.S.; Santos, N.C.; Cunha, P.; Cotter, J.; Sousa, N. The Use of Multiple Correspondence Analysis to Explore Associations between Categories of Qualitative Variables in Healthy Ageing. J. Aging Res. 2013, 2013, 302163. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, L.; Rousseeuw, P.J. Finding Groups in Data: An Introduction to Cluster Analysis; Wiley: New York, NY, USA, 1990. [Google Scholar]
- Kruskal, J.; Wish, M. Multidimensional Scaling; Sage Publications: Thousand Oaks, CA, USA, 1978. [Google Scholar] [CrossRef]
- Child, D. The Essentials of Factor Analysis; Cassell Educational: New York, NY, USA, 1990. [Google Scholar]
- Greenacre, M. Theory and Applications of Correspondence Analysis; Academic Press: London, UK, 1984. [Google Scholar]
- Abdi, H.; Williams, L.J. Principal component analysis. WIREs Comput. Stat. 2010, 2, 433–459. [Google Scholar] [CrossRef]
- Aiken, L.S.; West, S.G. Multiple Regression: Testing and Interpreting Interactions; Sage Publications, Inc.: Newbury Park, CA, USA, 1991. [Google Scholar]
- Casas Martinez, C. PADES (Domestic Care Program; Support Teams)—Homecare at the End of Life: The Privilege of Proximity; Revista Treball Social: Barcelona, Spain, 2017; pp. 69–80. [Google Scholar]
- British Geriatrics Society. Intermediate Care. Guidance for Commissioners and Providers of Health and Social Care. 2001. Available online: www.bgs.org.uk/compendium/comd4.html (accessed on 19 March 2020).
- Melis, R.J.; Rikkert, M.G.O.; Parker, S.G.; van Eijken, M.I. What Is Intermediate Care? BMJ 2004, 329, 360. [Google Scholar] [CrossRef]
- Du, G.; Liang, X.; Sun, C. Scheduling Optimization of Home Health Care Service Considering Patients’ Priorities and Time Windows. Sustainability 2017, 9, 253. [Google Scholar] [CrossRef] [Green Version]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ward Method with Euclidean Distance | K-Means | ||||||
|---|---|---|---|---|---|---|---|
| Cluster 1 | Cluster 2 | Cluster 3 | Cluster 1 | Cluster 2 | Cluster 3 | ||
| Ward method | Cluster 1 | 35 | 0 | 0 | 33 | 2 | 0 |
| with Square | Cluster 2 | 0 | 30 | 0 | 0 | 30 | 0 |
| Euclidean distance | Cluster 3 | 0 | 2 | 7 | 2 | 2 | 5 |
| Total | 35 | 32 | 7 | 35 | 34 | 5 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodriguez-Pereira, J.; de Armas, J.; Garbujo, L.; Ramalhinho, H. Health Care Needs and Services for Elder and Disabled Population: Findings from a Barcelona Study. Int. J. Environ. Res. Public Health 2020, 17, 8071. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218071
Rodriguez-Pereira J, de Armas J, Garbujo L, Ramalhinho H. Health Care Needs and Services for Elder and Disabled Population: Findings from a Barcelona Study. International Journal of Environmental Research and Public Health. 2020; 17(21):8071. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218071
Chicago/Turabian StyleRodriguez-Pereira, Jessica, Jesica de Armas, Lorenzo Garbujo, and Helena Ramalhinho. 2020. "Health Care Needs and Services for Elder and Disabled Population: Findings from a Barcelona Study" International Journal of Environmental Research and Public Health 17, no. 21: 8071. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218071