One Virus, Four Continents, Eight Countries: An Interdisciplinary and International Study on the Psychosocial Impacts of the COVID-19 Pandemic among Adults

 , , , , , , , , , add
Show full author list
, , , , , , , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Selection of Participants
2.3. Data Collection
2.4. Psychological Outcomes
2.5. Potential Stressor Variables
2.6. Sociodemographic Variables
2.7. Data Analysis
3. Results
3.1. Participants and Their Characteristics
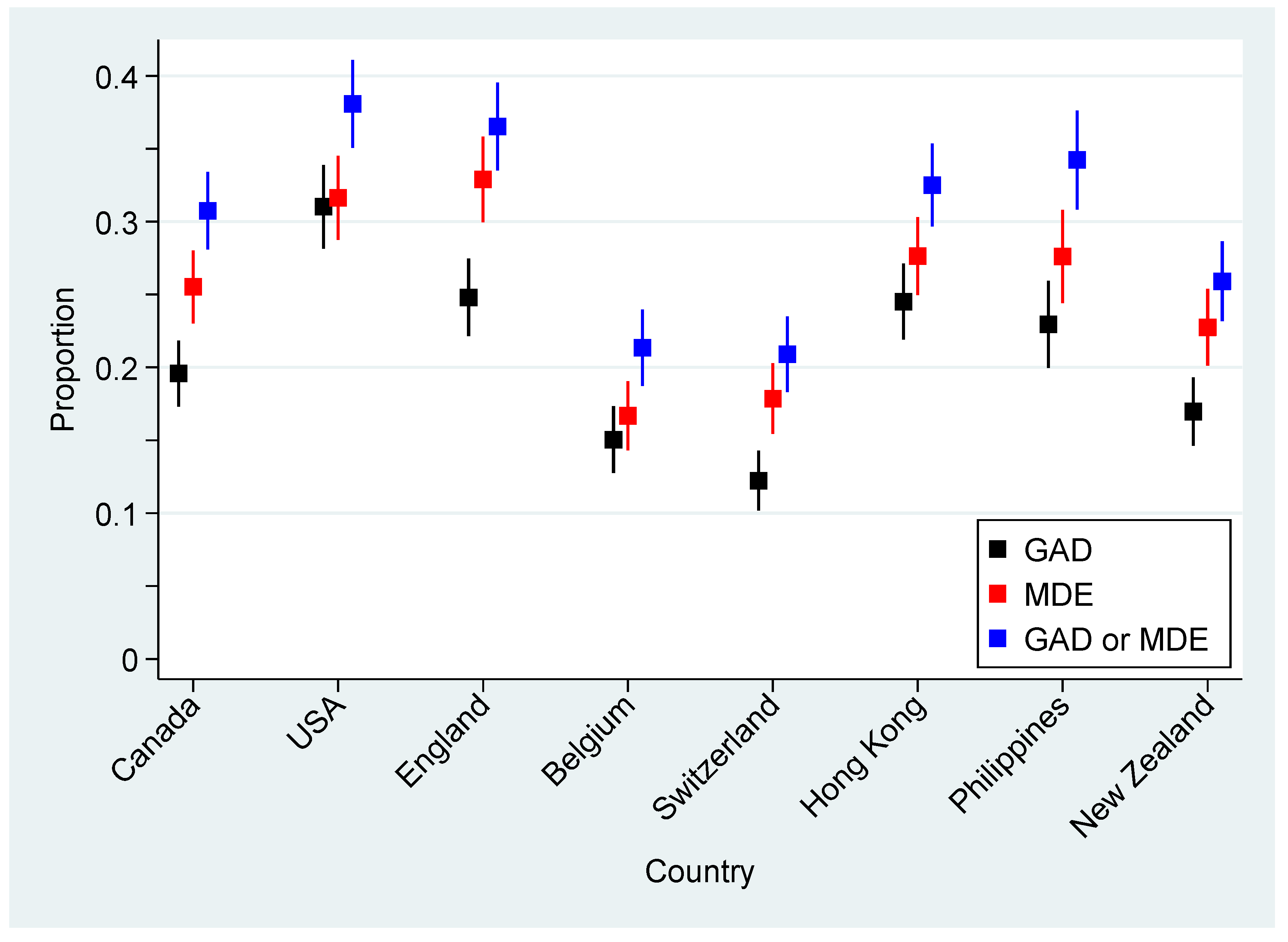
3.2. Psychological Outcomes
3.3. Complete Case Multilevel Mixed-Effects Models
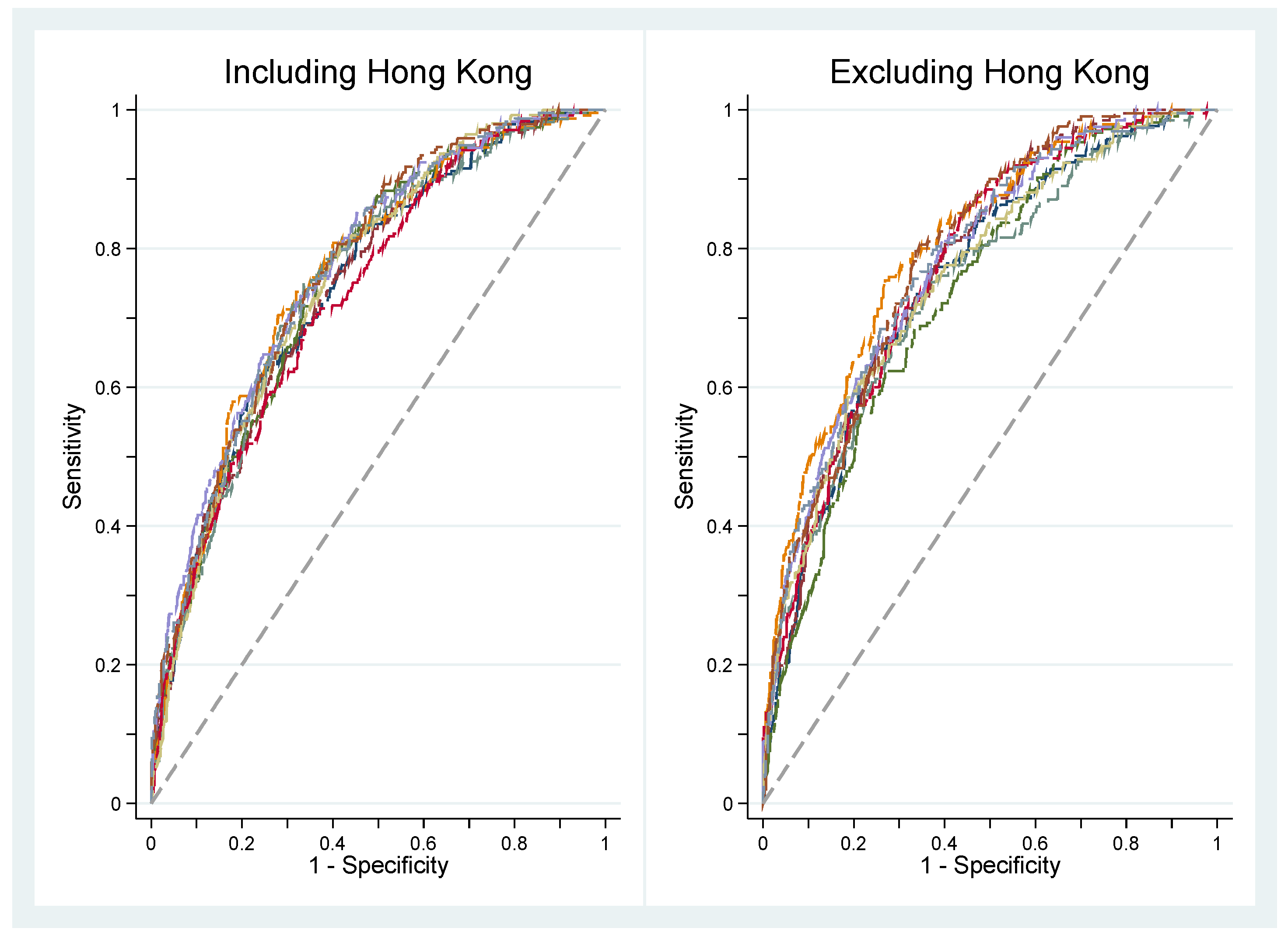
3.4. Sensitivity Analysis
4. Discussion
5. Practical Implications of the Results
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Worldometers 2020. COVID-19 Coronavirus Pandemic Reported Cases and Deaths by Country, Territory, or Conveyance. Available online: https://www.worldometers.info/coronavirus/?utm_campaign=homeAdvegas1?#countries (accessed on 12 September 2020).
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef]
- Petzold, M.B.; Bendau, A.; Plag, J.; Pyrkosch, L.; Maricic, L.M.; Betzler, F.; Rogoll, J.; Große, J.; Ströhle, A. Risk, resilience, psychological distress, and anxiety at the beginning of the COVID-19 pandemic in Germany. Brain Behav. 2020, 10, e01745. [Google Scholar] [CrossRef] [PubMed]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef] [PubMed]
- González-Sanguino, C.; Ausín, B.; ÁngelCastellanos, M.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Islam, S.M.D.-U.; Bodrud-Doza, M.; Khan, R.M.; Haque, M.A.; Mamun, M.A. Exploring COVID-19 stress and its factors in Bangladesh: A perception-based study. Heliyon 2020, 6, e04399. [Google Scholar] [CrossRef]
- Liu, C.H.; Zhang, E.; Wong, G.T.F.; Hyun, S.; Hahm, H. “Chris” Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: Clinical implications for U.S. young adult mental health. Psychiatry Res. 2020, 290, 113172. [Google Scholar] [CrossRef]
- Antonovsky, A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well; Jossey-Bass: San Francisco, CA, USA, 1987; pp. 127–139. [Google Scholar]
- Chiesi, F.; Bonacchi, A.; Primi, C.; Toccafondi, A.; Miccinesi, G. Are three items sufficient to measure sense of coherence? Evidence from nonclinical and clinical samples. Eur. J. Psychol. Assess. 2018, 34, 229–237. [Google Scholar] [CrossRef]
- Dymecka, J.; Gerymski, R.; Machnik-Czerwik, A. How does stress affect our life satisfaction during COVID-19 pandemic? Moderated mediation analysis of sense of coherence and fear of coronavirus 2020. PsyArXiv Prepr. 2020. [Google Scholar] [CrossRef]
- Mak, I.W.C.; Chu, M.C.; Pan, P.C.; Yiu, M.G.C.; Chan, V.L. Long-term psychiatric morbidities among SARS survivors. Gen. Hosp. Psychiatry 2009, 31, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Schäfer, S.K.; Sopp, M.R.; Schanz, C.G.; Staginnus, M.; Göritz, A.S.; Michael, T. Impact of COVID-19 on public mental health and the buffering effect of a sense of coherence. Psychother. Psychosom. 2020, 89, 386–392. [Google Scholar]
- Bettinghaus, E.P. Health promotion and the knowledge-attitude-behavior continuum. Prev. Med. 1986, 15, 475–491. [Google Scholar] [CrossRef]
- Swinson, R.P. The GAD-7 scale was accurate for diagnosing generalised anxiety disorder. Evid. Based Med. 2006, 11, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levis, B.; Benedetti, A.; Thombs, B.D. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: Individual participant data meta-analysis. BMJ 2019, 365, l1476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, J.; Upadhye, S.; Worster, A. Understanding receiver operating characteristic (ROC) curves. Can. J. Emerg. Med. 2006, 8, 19–20. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression; Wiley: New York, NY, USA, 2000. [Google Scholar]
- Généreux, M.; Roy, M.; David, M.D.; Carignan, M.E.; Blouin-Genest, G.; Champagne-Poirier, O. Psychological response to the COVID-19 pandemic in Canada: Main stressors and assets. Global Health Promot. submitted in July 2020.
- Louise, P.; Siobhan, O.; Louise, M.; Jean, G.; Pelletier, L.; O’Donnell, S.; McRae, L.; Grenier, J. The burden of generalized anxiety disorder in Canada. Health Promot. Chronic Dis. Prev. Can. 2017, 37, 54–62. [Google Scholar] [CrossRef] [Green Version]
- Lukmanji, A.; Williams, J.V.A.; Bulloch, A.G.M.; Bhattarai, A.; Patten, S.B. Seasonal variation in symptoms of depression: A Canadian population based study. J. Affect. Disord. 2019, 255, 142–149. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Hrabok, M.; Juhás, M.; Omeje, J.; Denga, E.; Nwaka, B.; Akinjise, I.; Corbett, S.E.; Moosavi, S.; Brown, M.; et al. Prevalence Rates and Predictors of Generalized Anxiety Disorder Symptoms in Residents of Fort McMurray Six Months After a Wildfire. Front. Psychiatry 2018, 9, 345. [Google Scholar] [CrossRef] [Green Version]
- Agyapong, V.I.O.; Juhás, M.; Brown, M.R.G.; Omege, J.; Denga, E.; Nwaka, B.; Akinjise, I.; Corbett, S.E.; Hrabok, M.; Li, X.-M.; et al. Prevalence Rates and Correlates of Probable Major Depressive Disorder in Residents of Fort McMurray 6 Months After a Wildfire. Int. J. Ment. Health Addict. 2018, 17, 120–136. [Google Scholar] [CrossRef]
- Super, S.; Wagemakers, M.A.E.; Picavet, H.S.J.; Verkooijen, K.T.; Koelen, M.A. Strengthening sense of coherence: Opportunities for theory building in health promotion. Health Promot. Int. 2016, 31, 869–878. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Klaiber, P.; Wen, J.H.; DeLongis, A.; Sin, N.L. The Ups and Downs of Daily Life During COVID-19: Age Differences in Affect, Stress, and Positive Events. J. Gerontol. Ser. B 2020. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables Names | Descriptions and Response Options |
|---|---|
| Having experienced self-isolation/quarantine | Having experienced self-isolation/quarantine, mandatory or voluntary (yes because of symptoms or diagnosis of the novel coronavirus disease 2019 (COVID-19), yes for other reasons, no). |
| Having experienced financial losses | Having experienced financial losses of any kind due to the COVID-19 (yes, no). |
| Threat perceived for oneself and/or family | Level of threat posed by the COVID-19 perceived for oneself and/or the family (very low/low/moderate, high/very high). |
| Threat perceived for country and/or world | Level of threat posed by the COVID-19 perceived for the country and/or the world (very low/low/moderate, high/very high). |
| Being a victim of stigma | Being a victim of stigma or discrimination due to the COVID-19 (yes, no). |
| Level of information about COVID-19 | Level of information about the coronavirus, with a scale ranging from 1 to 10 (high (9, 10), lower level (0–8)). |
| Level of trust in authorities | Level of trust in authorities (scientists, doctors, and health experts; national health organizations; global health organizations; government), each with a scale ranging from 1 to 10. The sum of these four distinct scores (total score ranging from 4–40) was then divided into quartiles. |
| False beliefs score | False beliefs score based on 12 statements scientifically unfounded (e.g., “I believe the coronavirus was made intentionally in a laboratory”, or “I believe the coronavirus is not transmitted in warm countries”). Participants had to agree on a scale ranging from 1–10 on each of these statements. The sum of these 12 scores (total score ranging from 12–120) was then divided into quartiles. |
| Sources regularly used | Sources regularly used to get informed about the COVID-19 including the World Health Organization (WHO), government, public health authorities, health professionals, news media (television, radio, newspapers), friend, family and coworkers, social networks, and the Internet. Respondents had to report the frequency of use, which was subsequently dichotomized as “a lot/somewhat” vs. “not much/not at all”, for each source of information. |
| Sense of coherence (SOC) | Sense of coherence (SOC) measured with a three-item questionnaire (i.e., SOC-3) that was developed for the needs and constraints of large population studies and that has shown adequate psychometric properties [11]. Each question corresponded to one of the three components of the SOC. The total score, which ranged from 0–6, was dichotomized using a standard threshold (weak (0–4) or strong (5, 6) SOC). |
| Demographic Characteristics | Canada | USA | England | Belgium | Switzerland | Hong Kong | Philippines | NZ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | |
| Sex * | ||||||||||||||||
| Female | 722.5 (48.4) | 516.4 (48.5) | 507.9 (48.8) | 493.7 (48.6) | 477.5 (47.7) | 513.2 (45.1) | 509.9 (49.2) | 484.2 (48.6) | ||||||||
| Male | 771.8 (51.6) | 548.4 (51.5) | 531.9 (51.2) | 521.1 (51.4) | 522.5 (52.3) | 625.8 (54.9) | 521.9 (50.6) | 512.2 (51.4) | ||||||||
| Age (years) | ||||||||||||||||
| 18–24 | 163.0 (10.9) | 58.9 (5.5) | 115.8 (11.1) | 62.5 (6.2) | 95.5 (9.5) | 108.3 (9.5) | 224.4 (21.6) | 122.3 (12.2) | ||||||||
| 25–34 | 246.6 (16.4) | 225.5 (21.2) | 181.2 (17.4) | 207.8 (20.5) | 144.1 (14.4) | 196.2 (17.2) | 260.3 (25.0) | 184.3 (18.4) | ||||||||
| 35–44 | 242.7 (16.2) | 191.1 (17.9) | 170.0 (16.3) | 139.5 (13.7) | 138.3 (13.8) | 205.8 (18.1) | 208.9 (20.1) | 162.8 (16.3) | ||||||||
| 45–54 | 269.1 (17.9) | 203.6 (19.1) | 185.9 (17.9) | 210.3 (20.7) | 176.8 (17.6) | 218.2 (19.1) | 161.5 (15.5) | 175.3 (17.5) | ||||||||
| 55–64 | 262.4 (17.5) | 189.5 (17.8) | 151.2 (14.5) | 171.5 (16.9) | 239.1 (23.9) | 201.7 (17.7) | 106.0 (10.2) | 157.5 (15.7) | ||||||||
| ≥65 | 317.2 (21.1) | 196.4 (18.4) | 236.9 (22.8) | 223.5 (22.0) | 209.3 (20.8) | 209.8 (18.4) | 79.8 (7.7) | 198.9 (19.9) | ||||||||
| Household composition | ||||||||||||||||
| Alone | 303.7 (20.2) | 233.2 (21.9) | 215.2 (20.7) | 192.1 (18.9) | 236.1 (23.6) | 74.3 (6.5) | 49.7 (4.8) | 180.6 (18.0) | ||||||||
| Children | 409.4 (27.3) | 375.1 (35.2) | 308.0 (29.6) | 278.9 (27.5) | 264.9 (26.4) | 493.8 (43.3) | 462.0 (44.4) | 349.5 (34.9) | ||||||||
| Other | 788.0 (52.5) | 456.7 (42.9) | 517.8 (49.7) | 542.8 (53.5) | 501.1 (50.0) | 571.9 (50.2) | 529.3 (50.8) | 471.0 (47.0) | ||||||||
| Essential worker | ||||||||||||||||
| Yes | 357.2 (24.1) | 229.9 (21.8) | 274.9 (26.9) | 176.5 (18.8) | 222.9 (22.8) | 400.0 (35.7) | 184.7 (18.8) | 267.9 (27.1) | ||||||||
| No | 1125.5 (75.9) | 823.8 (78.2) | 748.5 (73.1) | 816.7 (82.2) | 756.8 (77.2) | 721.1 (64.3) | 797.6 (81.2) | 722.0 (72.9) | ||||||||
| GAD or MDE | Crude | Adjusted 1 | Adjusted 2 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N | n | (%) | OR | (95% CI) | aOR | (95% CI) | aOR | (95% CI) | |
| Sex | |||||||||
| Female | 4555.6 | 1470.9 | (32.3) | 1.24 | (1.09, 1.42) | 1.34 | (1.20, 1.50) | 1.24 | (1.07, 1.44) |
| Male | 4225.4 | 1175.1 | (27.8) | 1 | (reference) | 1 | (reference) | 1 | (reference) |
| Age (years) | |||||||||
| 18–24 | 950.8 | 422.9 | (44.5) | 4.27 | (2.74, 6.65) | 3.38 | (2.81, 4.07) | 3.00 | (2.16, 4.17) |
| 25–34 | 1646.0 | 699.3 | (42.5) | 3.88 | (2.59, 5.82) | 2.74 | (2.16, 3.46) | 2.61 | (1.91, 3.56) |
| 35–44 | 1459.0 | 543.6 | (37.3) | 3.07 | (2.06, 4.57) | 2.37 | (1.97, 2.84) | 2.13 | (1.60, 2.85) |
| 45–54 | 1600.7 | 461.1 | (28.8) | 2.12 | (1.60, 2.80) | 1.96 | (1.64, 2.35) | 1.71 | (1.33, 2.21) |
| 55–64 | 1478.7 | 263.6 | (17.8) | 1.14 | (0.75, 1.72) | 1.35 | (1.15, 1.59) | 1.10 | (0.75, 1.61) |
| ≥65 | 1670.7 | 270.2 | (16.2) | 1 | (reference) | 1 | (reference) | 1 | (reference) |
| Household composition | |||||||||
| Alone | 1484.9 | 391.0 | (26.3) | 1 | (reference) | 1 | (reference) | 1 | (reference) |
| Children | 2941.5 | 968.5 | (32.9) | 1.32 | (1.00, 1.74) | 1.07 | (0.89, 1.29) | 1.17 | (0.95, 1.4) |
| Other | 4378.6 | 1300.0 | (29.7) | 1.17 | (1.01, 1.35) | 0.95 | (0.88, 1.02) | 0.97 | (0.88, 1.07) |
| Essential worker | |||||||||
| No | 6512.1 | 1803.0 | (27.7) | 1 | (reference) | 1 | (reference) | 1 | (reference) |
| Yes | 2113.9 | 793.2 | (37.5) | 1.56 | (1.27, 1.91) | 1.07 | (0.93, 1.24) | 1.21 | (1.01, 1.43) |
| Self-isolation/quarantine | |||||||||
| No | 3182.5 | 719.5 | (22.6) | 1 | (reference) | 1 | (reference) | 1 | (reference) |
| Yes, case/symptom-free | 4387.1 | 1317.0 | (30.0) | 1.46 | (1.28, 1.67) | 1.38 | (1.21, 1.57) | 1.31 | (1.15, 1.49) |
| Yes, case or symptoms | 949.4 | 491.2 | (51.7) | 3.60 | (2.58, 5.04) | 2.16 | (1.62, 2.87) | 2.27 | (1.74, 2.97) |
| Financial losses | |||||||||
| No | 3743.0 | 854.7 | (22.8) | 1 | (reference) | 1 | (reference) | 1 | (reference) |
| Yes | 4008.6 | 1441.8 | (36.0) | 1.83 | (1.63, 2.06) | 1.35 | (1.12, 1.64) | 1.36 | (1.17, 1.58) |
| Unsure/unknown | 1054.4 | 364.1 | (34.5) | 1.91 | (1.64, 2.22) | 1.46 | (1.19, 1.79) | 1.50 | (1.25, 1.80) |
| Threat perceived for oneself and/or family | |||||||||
| High | 2967.5 | 1278.6 | (43.1) | 2.43 | (2.08, 2.84) | 1.99 | (1.83, 2.17) | 2.12 | (1.91, 2.36) |
| Otherwise | 5569.5 | 1297.9 | (23.3) | 1 | (reference) | 1 | (reference) | 1 | (reference) |
| Threat perceived for country and/or world | |||||||||
| High | 6223.2 | 2050.7 | (33.0) | 1.65 | (1.40, 1.94) | 1.43 | (1.26, 1.63) | 1.31 | (1.19, 1.45) |
| Otherwise | 2284.8 | 524.5 | (23.0) | 1 | (reference) | 1 | (reference) | 1 | (reference) |
| Being a victim of stigma | |||||||||
| No | 6607.1 | 1700.0 | (25.7) | 1 | (reference) | 1 | (reference) | 1 | (reference) |
| Yes | 1254.7 | 615.1 | (49.0) | 2.71 | (2.11, 3.49) | 1.45 | (1.21, 1.73) | 1.57 | (1.28, 1.92) |
| Decline to answer | 944.1 | 345.5 | (36.6) | 1.67 | (1.38, 2.03) | 1.17 | (0.95, 1.43) | 1.30 | (1.08, 1.56) |
| Level of information about COVID-19 | |||||||||
| High (9–10) | 2784.5 | 840.0 | (30.2) | 1 | (reference) | 1 | (reference) | 1 | (reference) |
| Otherwise (1–8) | 6021.5 | 1820.6 | (30.2) | 1.03 | (0.93, 1.13) | 0.85 | (0.77, 0.95) | 0.86 | (0.78, 0.94) |
| Trust in authorities score | |||||||||
| Q1 (low) | 2361.8 | 828.6 | (35.1) | 1.59 | (1.06, 2.39) | 1.66 | (1.21, 2.27) | 1.83 | (1.34, 2.51) |
| Q2 | 2121.9 | 665.0 | (31.3) | 1.37 | (1.16, 1.61) | 1.36 | (1.29, 1.44) | 1.41 | (1.33, 1.49) |
| Q2 | 2166.3 | 602.8 | (27.8) | 1.13 | (0.92, 1.39) | 1.21 | (0.98, 1.50) | 1.23 | (0.99, 1.52) |
| Q4 (high) | 2156.0 | 564.3 | (26.2) | 1 | (reference) | 1 | (reference) | 1 | (reference) |
| False beliefs score * | |||||||||
| Q1 (low) | 1987.6 | 382.0 | (19.2) | 1 | (reference) | 1 | (reference) | - | - |
| Q2 | 1900.7 | 437.3 | (23.0) | 1.29 | (1.12, 1.48) | 1.17 | (1.07, 1.27) | - | - |
| Q3 | 1931.5 | 572.0 | (29.6) | 1.82 | (1.33, 2.50) | 1.52 | (1.14, 2.02) | - | - |
| Q4 (high) | 1846.2 | 898.6 | (48.7) | 4.08 | (2.69, 6.17) | 2.55 | (1.87, 3.46) | - | - |
| Social networks used as a regular source of information | |||||||||
| Often/always | 2685.1 | 1054.5 | (39.3) | 1.79 | (1.42, 2.24) | 1.09 | (0.94, 1.28) | 1.16 | (1.00, 1.35) |
| Sometimes/never | 5780.9 | 1522.6 | (26.3) | 1 | (reference) | 1 | (reference) | 1 | (reference) |
| Friend/family/coworkers as a regular source of information | |||||||||
| Often/always | 3514.5 | 1232.7 | (35.1) | 1.42 | (1.26, 1.60) | 1.02 | (0.88, 1.19) | 1.11 | (0.99, 1.25) |
| Sometimes/never | 5113.5 | 1374.7 | (26.9) | 1 | (reference) | 1 | (reference) | 1 | (reference) |
| Sense of coherence | |||||||||
| Strong (5–6) | 2649.7 | 357.2 | (13.5) | 1 | (reference) | 1 | (reference) | 1 | (reference) |
| Weak (0–4) | 6156.3 | 2303.4 | (37.4) | 3.80 | (3.16. 4.57) | 3.13 | (2.73, 3.59) | 3.21 | (2.73, 3.77) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Généreux, M.; Schluter, P.J.; Hung, K.K.; Wong, C.S.; Pui Yin Mok, C.; O’Sullivan, T.; David, M.D.; Carignan, M.-E.; Blouin-Genest, G.; Champagne-Poirier, O.; et al. One Virus, Four Continents, Eight Countries: An Interdisciplinary and International Study on the Psychosocial Impacts of the COVID-19 Pandemic among Adults. Int. J. Environ. Res. Public Health 2020, 17, 8390. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228390
Généreux M, Schluter PJ, Hung KK, Wong CS, Pui Yin Mok C, O’Sullivan T, David MD, Carignan M-E, Blouin-Genest G, Champagne-Poirier O, et al. One Virus, Four Continents, Eight Countries: An Interdisciplinary and International Study on the Psychosocial Impacts of the COVID-19 Pandemic among Adults. International Journal of Environmental Research and Public Health. 2020; 17(22):8390. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228390
Chicago/Turabian StyleGénéreux, Mélissa, Philip J. Schluter, Kevin KC Hung, Chi Shing Wong, Catherine Pui Yin Mok, Tracey O’Sullivan, Marc D. David, Marie-Eve Carignan, Gabriel Blouin-Genest, Olivier Champagne-Poirier, and et al. 2020. "One Virus, Four Continents, Eight Countries: An Interdisciplinary and International Study on the Psychosocial Impacts of the COVID-19 Pandemic among Adults" International Journal of Environmental Research and Public Health 17, no. 22: 8390. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228390