Clinical Characteristics and Risk Factors for Fatality and Severity in Patients with Coronavirus Disease in Korea: A Nationwide Population-Based Retrospective Study Using the Korean Health Insurance Review and Assessment Service (HIRA) Database



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
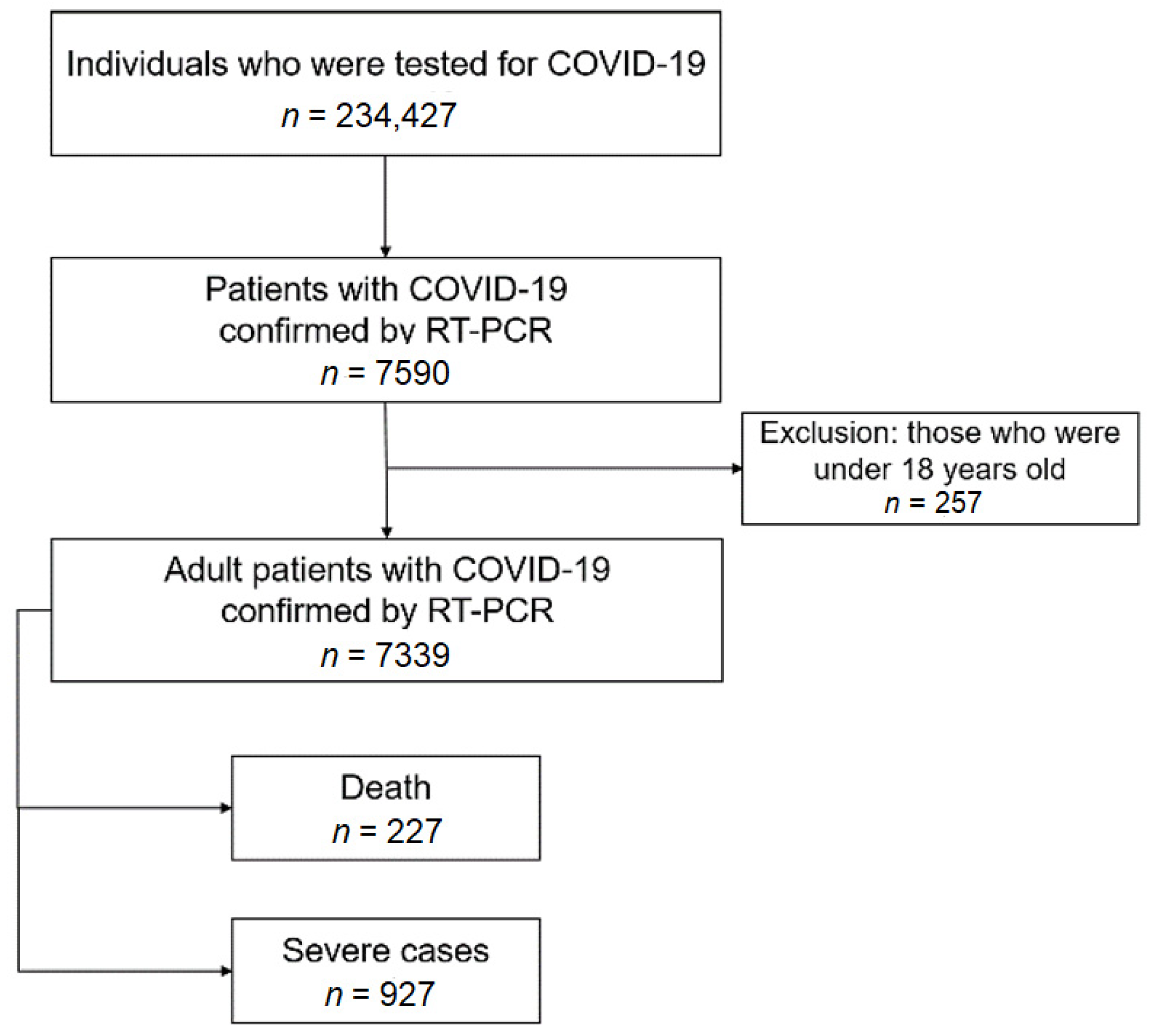
2.2. Study Population and Assessment
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- World Heatlth Organization Cornavirus Disease (COVID-19) Situation Report-192. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200730-covid-19-sitrep-92.pdf?sfvrsn=5e52901f_4 (accessed on 26 October 2020).
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korean Society of Infectious Diseases; Korean Society of Pediatric Infectious Diseases; Korean Society of Epidemiology; Korean Society for Antimicrobial Therapy; Korean Society for Healthcare-associated Infection Control and Prevention; Korea Centers for Disease Control and Prevention. Report on the Epidemiological Features of Coronavirus Disease 2019 (COVID-19) Outbreak in the Republic of Korea from January 19 to March 2, 2020. J. Korean Med. Sci. 2020, 35, e112. [Google Scholar] [CrossRef]
- Chen, R.; Liang, W.; Jiang, M.; Guan, W.; Zhan, C.; Wang, T.; Tang, C.; Sang, L.; Liu, J.; Ni, Z.; et al. Risk Factors of Fatal Outcome in Hospitalized Subjects with Coronavirus Disease 2019 From a Nationwide Analysis in China. Chest 2020, 158, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020. [Google Scholar] [CrossRef]
- Nikpouraghdam, M.; Farahani, A.J.; Alishiri, G.; Heydari, S.; Ebrahimnia, M.; Samadinia, H.; Sepandi, M.; Jafari, N.J.; Izadi, M.; Qazvini, A.; et al. Epidemiological characteristics of coronavirus disease 2019 (COVID-19) patients in IRAN: A single center study. J. Clin. Virol. 2020, 127, 104378. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Northwell COVID-19 Research Consortium. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Bhatraju, P.K.; Ghassemieh, B.J.; Nichols, M.; Kim, R.; Jerome, K.R.; Nalla, A.K.; Greninger, A.L.; Pipavath, S.; Wurfel, M.M.; Evans, L.; et al. Covid-19 in Critically Ill Patients in the Seattle Region—Case Series. N. Engl. J. Med. 2020, 382, 2012–2022. [Google Scholar] [CrossRef] [PubMed]
- #OpenData4COVID19. Available online: https://hira-covid19.net/ (accessed on 26 October 2020).
- Ji, W.; Huh, K.; Kang, M.; Hong, J.; Bae, G.H.; Lee, R.; Na, Y.; Choi, H.; Gong, S.Y.; Choi, Y.-H.; et al. Effect of Underlying Comorbidities on the Infection and Severity of COVID-19 in Korea: A Nationwide Case-Control Study. J. Korean Med. Sci. 2020, 35, e237. [Google Scholar] [CrossRef] [PubMed]
- Bulut, C.; Kato, Y. Epidemiology of COVID-19. Turk. J. Med. Sci. 2020, 50, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-H.; Choe, Y.J.; Jeong, J.-Y. Understanding and Interpretation of Case Fatality Rate of Coronavirus Disease 2019. J. Korean Med. Sci. 2020, 35, e137. [Google Scholar] [CrossRef]
- Du, R.-H.; Liang, L.-R.; Yang, C.-Q.; Wang, W.; Cao, T.-Z.; Li, M.; Guo, G.-Y.; Du, J.; Zheng, C.-L.; Zhu, Q.; et al. Predictors of mortality for patients with COVID-19 pneumonia caused by SARS-CoV-2: A prospective cohort study. Eur. Respir. J. 2020, 55, 2000524. [Google Scholar] [CrossRef] [Green Version]
- Parohan, M.; Yaghoubi, S.; Seraji, A.; Javanbakht, M.H.; Sarraf, P.; Djalali, M. Risk factors for mortality in patients with Coronavirus disease 2019 (COVID-19) infection: A systematic review and meta-analysis of observational studies. Aging Male 2020, 1–9. [Google Scholar] [CrossRef]
- Emami, A.; Javanmardi, F.; Pirbonyeh, N. Prevalence of Underlying Diseases in Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis. Arch. Acad. Emerg. Med. 2020, 8, e35. [Google Scholar]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef]
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef]
- Kario, K.; Morisawa, Y.; Sukonthasarn, A.; Turana, Y.; Chia, Y.C.; Park, S.; Wang, T.-D.; Chen, C.-H.; Tay, J.C.; Li, Y.; et al. COVID-19 and hypertension-evidence and practical management: Guidance from the HOPE Asia Network. J. Clin. Hypertens. 2020. [Google Scholar] [CrossRef]
- Zaki, N.; Alashwal, H.; Ibrahim, S. Association of hypertension, diabetes, stroke, cancer, kidney disease, and high-cholesterol with COVID-19 disease severity and fatality: A systematic review. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1133–1142. [Google Scholar] [CrossRef] [PubMed]
- Apicella, M.; Campopiano, M.C.; Mantuano, M.; Mazoni, L.; Coppelli, A.; Del Prato, S. COVID-19 in people with diabetes: Understanding the reasons for worse outcomes. Lancet Diabetes Endocrinol. 2020, 8, 782–792. [Google Scholar] [CrossRef]
- Kim, D.W.; Byeon, K.H.; Kim, J.; Cho, K.D.; Lee, N. The Correlation of Comorbidities on the Mortality in Patients with COVID-19: An Observational Study Based on the Korean National Health Insurance Big Data. J. Korean Med. Sci. 2020, 35, e243. [Google Scholar] [CrossRef]
- Koliaki, C.; Tentolouris, A.; Eleftheriadou, I.; Melidonis, A.; Dimitriadis, G.; Tentolouris, N. Clinical Management of Diabetes Mellitus in the Era of COVID-19: Practical Issues, Peculiarities and Concerns. J. Clin. Med. 2020, 9, 2288. [Google Scholar] [CrossRef]
- D’Marco, L.; Puchades, M.J.; Romero-Parra, M. Coronavirus disease 2019 in chronic kidney disease. Clin. Kidney J. 2020, 13, 297–306. [Google Scholar]
- Gudbjartsson, D.F.; Norddahl, G.L.; Melsted, P.; Gunnarsdottir, K.; Holm, H.; Eythorsson, E.; Arnthorsson, A.O.; Helgason, D.; Bjarnadottir, K.; Ingvarsson, R.F.; et al. Humoral Immune Response to SARS-CoV-2 in Iceland. N. Engl. J. Med. 2020, 383, 1724–1734. [Google Scholar] [CrossRef] [PubMed]
- Drożdżal, S.; Rosik, J.; Lechowicz, K.; Machaj, F.; Kotfis, K.; Ghavami, S.; Łos, M.J. FDA approved drugs with pharmacotherapeutic potential for SARS-CoV-2 (COVID-19) therapy. Drug Resist. Updat. 2020, 53, 100719. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total (n = 7339) | Deceased (n = 227) | Survivors (n = 7112) | p Value * | Severe Cases (n = 927) | Non-Severe Cases (n = 6412) | p Value § | |
|---|---|---|---|---|---|---|---|
| Age, years, mean ± SD | 47.1 ± 19.0 | 77.1 ± 10.8 | 46.1 ± 18.4 | <0.001 | 66.8 ± 15.2 | 44.2 ± 17.8 | <0.001 |
| Age group | |||||||
| 18–19 years, n (%) | 180 (2.5) | 0 (0) | 180 (2.5) | <0.001 | 2 (0.2) | 178 (2.8) | <0.001 |
| 20–29 years, n (%) | 1852 (25.2) | 0 (0) | 1852 (26.0) | 23 (2.5) | 1829 (28.5) | ||
| 30–39 years, n (%) | 777 (10.6) | 2 (0.9) | 775 (10.9) | 28 (3.0) | 749 (11.7) | ||
| 40–49 years, n (%) | 1008 (13.7) | 1 (0.4) | 1007 (14.2) | 46 (5.0) | 962 (15.0) | ||
| 50–59 years, n (%) | 1502 (20.5) | 15 (6.6) | 1487 (20.9) | 173 (18.7) | 1329 (20.7) | ||
| 60–69 years, n (%) | 1056 (14.4) | 35 (15.4) | 1021 (14.4) | 229 (24.7) | 827 (12.9) | ||
| 70~ years, n (%) | 964 (13.1) | 174 (76.7) | 790 (11.1) | 426 (46) | 538 (8.4) | ||
| Male, n (%) | 2970 (40.1) | 121 (53.3) | 2849 (40.1) | <0.001 | 441 (47.6) | 2529 (39.4) | <0.001 |
| Treatment duration, days, mean ± SD | 22.0 ± 14.5 | 19.1 ± 15.9 | 22.1 ± 14.5 | 0.005 | 29.9 ± 18.7 | 20.9 ± 13.5 | <0.001 |
| DG area, n (%) | 4139 (55.9) | 201 (88.5) | 3938 (55.4) | <0.001 | 705 (76.1) | 3434 (53.6) | <0.001 |
| Comorbidity | |||||||
| Influenza, n (%) | 582 (7.9) | 10 (4.4) | 572 (8.0) | 0.046 | 49 (5.3) | 533 (8.3) | <0.001 |
| Tuberculosis, n (%) | 28 (0.4) | 4 (1.8) | 24 (0.3) | <0.001 | 11 (1.2) | 17 (0.3) | <0.001 |
| COPD, n (%) | 81 (1.1) | 14 (6.2) | 67 (0.9) | <0.001 | 32 (3.5) | 49 (0.8) | <0.001 |
| Pneumonia, n (%) | 513 (6.9) | 56 (24.7) | 457 (6.4) | <0.001 | 173 (18.7) | 340 (5.3) | <0.001 |
| Asthma, n (%) | 397 (5.4) | 21 (9.3) | 376 (5.3) | 0.009 | 93 (10.0) | 304 (4.7) | <0.001 |
| DM, n (%) | 857 (11.6) | 91 (40.1) | 766 (10.8) | <0.001 | 264 (28.5) | 593 (9.2) | <0.001 |
| CKD, n (%) | 48 (0.6) | 12 (5.3) | 36 (0.5) | <0.001 | 28 (3.0) | 20 (0.3) | <0.001 |
| Chronic liver disease, n (%) | 645 (8.7) | 20 (8.8) | 625 (8.8) | 0.991 | 98 (10.6) | 547 (8.5) | 0.040 |
| Hypertension, n (%) | 1373 (18.6) | 106 (46.7) | 1267 (17.8) | <0.001 | 371 (40.0) | 1002 (15.6) | <0.001 |
| CVDs, n (%) | 455 (6.1) | 55 (24.2) | 400 (5.6) | <0.001 | 155 (16.7) | 300 (4.7) | <0.001 |
| Malignancies, n (%) | 162 (2.2) | 20 (8.8) | 142 (2.0) | <0.001 | 60 (6.5) | 102 (1.6) | <0.001 |
| HIV infection, n (%) | 4 (0.1) | 1 (0.4) | 3 (0.0) | 0.011 | 1 (0.1) | 3 (0.0) | 0.456 |
| Medications | |||||||
| Lopinavir/ritonavir, n (%) | 2648 (35.8) | 158 (69.6) | 2490 (35.0) | <0.001 | 733 (79.1) | 1915 (29.9) | <0.001 |
| Hydroxychloroquine, n (%) | 2102 (28.4) | 141 (62.1) | 1961 (27.6) | <0.001 | 574 (61.9) | 1528 (23.8) | <0.001 |
| Ribavirin, n (%) | 4 (0.1) | 2 (0.9) | 2 (0.0) | <0.001 | 4 (0.4) | 0 (-) | <0.001 |
| Type I interferon, n (%) | 63 (0.9) | 28 (12.3) | 35 (0.5) | <0.001 | 47 (5.1) | 16 (0.2) | <0.001 |
| Human immunoglobulin G, n (%) | 36 (0.5) | 24 (10.6) | 12 (0.2) | <0.001 | 35 (3.8) | 1 (0.0) | <0.001 |
| Oseltamivir, n (%) | 19 (0.3) | 1 (0.4) | 18 (0.3) | 0.584 | 8 (0.9) | 11 (0.2) | <0.001 |
| Antibiotics, n (%) | 2820 (38.1) | 209 (92.1) | 2611 (36.7) | <0.001 | 844 (91.0) | 1976 (30.8) | <0.001 |
| Penicillins, n (%) | 646 (8.7) | 149 (65.6) | 497 (7.0) | <0.001 | 404 (43.6) | 242 (3.8) | <0.001 |
| Cephlosporins, n (%) | 1649 (22.3) | 156 (68.7) | 1493 (21.0) | <0.001 | 611 (65.9) | 1038 (16.2) | <0.001 |
| Quinolones, n (%) | 1739 (23.5) | 159 (70.0) | 1580 (22.2) | <0.001 | 603 (65.0) | 1136 (17.7) | <0.001 |
| Macrolides, n (%) | 1152 (15.6) | 103 (45.4) | 1049 (14.7) | <0.001 | 407 (43.9) | 745 (11.6) | <0.001 |
| Aminoglycosides, n (%) | 45 (0.6) | 8 (3.5) | 37 (0.5) | <0.001 | 28 (3.0) | 17 (0.3) | <0.001 |
| TMP/SMX, n (%) | 43 (0.6) | 8 (3.5) | 35 (0.5) | <0.001 | 34 (3.7) | 9 (0.1) | <0.001 |
| Tetracyclines, n (%) | 33 (0.4) | 5 (2.2) | 28 (0.4) | <0.001 | 16 (1.7) | 17 (0.3) | <0.001 |
| Others, n (%) | 238 (3.2) | 89 (39.2) | 149 (2.1) | <0.001 | 195 (21.0) | 43 (0.7) | <0.001 |
| Univariable Model | Multivariable Model 1 * | Multivariable Model 2 § | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Influenza | 0.53 (0.28–1.00) | 0.050 | 0.92 (0.42–2.03) | 0.837 | 1.03 (0.49–2.18) | 0.931 |
| Tuberculosis | 5.30 (1.82–15.40) | 0.002 | 2.34 (0.61–8.94) | 0.216 | 2.79 (0.71–10.89) | 0.140 |
| COPD | 6.91 (3.82–12.49) | <0.001 | 1.39 (0.65–2.97) | 0.397 | 1.34 (0.66–2.73) | 0.422 |
| Pneumonia | 4.77 (3.48–6.54) | <0.001 | 1.6 (1.07–2.39) | 0.024 | 1.47 (0.99–2.18) | 0.055 |
| Asthma | 1.83 (0.15–2.90) | 0.010 | 0.68 (0.38–1.21) | 0.190 | 0.83 (0.48–1.43) | 0.494 |
| DM | 5.54 (4.21–7.30) | <0.001 | 2.17 (1.55–3.03) | <0.001 | 2.21 (1.59–3.08) | <0.001 |
| CKD | 10.97 (5.63–21.39) | <0.001 | 3.11 (1.33–7.3) | 0.009 | 3.21 (1.35–7.63) | 0.008 |
| Chronic liver disease | 1.00 (0.63–1.60) | 0.991 | 0.87 (0.50–1.51) | 0.609 | 1.01 (0.58–1.74) | 0.976 |
| Hypertension | 4.04 (3.09–5.28) | <0.001 | 0.85 (0.61–1.18) | 0.323 | 0.76 (0.55–1.06) | 0.102 |
| CVDs | 5.37 (3.90–7.39) | <0.001 | 0.82 (0.56–1.22) | 0.330 | 0.95 (0.64–1.40) | 0.778 |
| Malignancies | 4.74 (2.91–7.73) | <0.001 | 1.04 (0.56–1.93) | 0.895 | 1.21 (0.67–2.18) | 0.535 |
| HIV infection | 5.54 (4.21–7.30) | <0.001 | 106.93 (6.38–>999) | 0.001 | 101.92 (5.92–>999) | 0.001 |
| Lopinavir/ritonavir | 4.25 (3.19–5.66) | <0.001 | 0.81 (0.56–1.18) | 0.268 | 1.68 (1.22–2.32) | 0.002 |
| Hydroxychloroquine | 4.31 (3.28–5.66) | <0.001 | 0.86 (0.61–1.21) | 0.380 | 1.22 (0.89–1.68) | 0.215 |
| Ribavirin | 31.54 (4.42–224.93) | <0.001 | 5.82 (0.34–99.64) | 0.225 | >999 (410.48–>999) | 0.001 |
| Type I interferon | 28.45 (16.97–47.69) | <0.001 | 4.76 (2.48–9.11) | <0.001 | 6.54 (3.52–12.14) | <0.001 |
| Human immunoglobulin G | 69.95 (34.50–141.83) | <0.001 | 37.23 (13.95–99.37) | <0.001 | 52.22 (19.92–136.95) | <0.001 |
| Oseltamivir | 1.74 (0.23–13.12) | 0.589 | 3.74 (0.45–31.04) | 0.221 | 2.98 (0.34–26.11) | 0.324 |
| Antibiotics | 20.02 (12.34–32.47) | <0.001 | 4.18 (2.36–7.42) | <0.001 | 4.41 (2.65–7.35) | <0.001 |
| Age, years | 1.13 (1.11–1.14) | <0.001 | 1.12 (1.11–1.14) | <0.001 | - | - |
| Male | 1.71 (1.31–2.23) | <0.001 | 2.10 (1.51–2.92) | <0.001 | - | - |
| DG area | 6.23 (4.13–9.40) | <0.001 | 2.06 (1.27–3.34) | 0.003 | - | - |
| Univariable Model | Multivariable Model 1 * | Multivariable Model 2 § | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Influenza | 0.62 (0.46–0.83) | 0.002 | 0.92 (0.64–1.32) | 0.653 | 0.96 (0.67–1.37) | 0.815 |
| Tuberculosis | 4.52 (2.11–9.68) | <0.001 | 2.23 (0.85–5.84) | 0.103 | 3.06 (1.18–7.94) | 0.021 |
| COPD | 4.64 (2.96–7.29) | <0.001 | 1.02 (0.57–1.82) | 0.960 | 1.16 (0.67–2.00) | 0.605 |
| Pneumonia | 4.10 (3.36–5.00) | <0.001 | 1.74 (1.34–2.24) | <0.001 | 1.79 (1.39–2.30) | <0.001 |
| Asthma | 2.24 (1.76–2.86) | <0.001 | 1.22 (0.89–1.68) | 0.223 | 1.40 (1.03–1.91) | 0.030 |
| DM | 3.91 (3.31–4.61) | <0.001 | 1.36 (1.11–1.68) | 0.003 | 1.42 (1.16–1.74) | 0.001 |
| CKD | 9.95 (5.58–17.74) | <0.001 | 3.40 (1.67–6.92) | 0.001 | 3.55 (1.75–7.18) | <0.001 |
| Chronic liver disease | 1.27 (1.01–1.59) | 0.041 | 0.86 (0.66–1.13) | 0.291 | 0.97 (0.74–1.27) | 0.837 |
| Hypertension | 3.60 (3.11–4.61) | <0.001 | 1.05 (0.87–1.27) | 0.601 | 0.99 (0.82–1.20) | 0.933 |
| CVDs | 4.09 (3.32–5.04) | <0.001 | 0.98 (0.75–1.27) | 0.847 | 1.09 (0.84–1.40) | 0.514 |
| Malignancies | 4.28 (3.09–5.94) | <0.001 | 1.26 (0.83–1.91) | 0.271 | 1.30 (0.86–1.95) | 0.208 |
| HIV infection | 2.31 (0.24–22.20) | 0.469 | 5.92 (0.43–81.22) | 0.183 | 8.60 (0.71–103.83) | 0.091 |
| Lopinavir/ritonavir | 8.87 (7.51–10.49) | <0.001 | 2.47 (2.02–3.03) | <0.001 | 5.25 (4.38–6.29) | <0.001 |
| Hydroxychloroquine | 5.20 (4.50–6.01) | <0.001 | 1.64 (1.37–1.96) | <0.001 | 2.55 (2.16–3.02) | <0.001 |
| Ribavirin | >999 (0–>999) | 0.945 | >999 (0–>999) | 0.970 | >999 (0–>999) | 0.966 |
| Type I interferon | 21.35 (12.05–37.82) | <0.001 | 3.00 (1.59–5.65) | 0.001 | 5.99 (3.16–11.37) | <0.001 |
| Human immunoglobulin G | 251.52 (34.42–>999) | <0.001 | 51.48 (6.76–392.23) | <0.001 | 146.16 (18.72–>999) | <0.001 |
| Oseltamivir | 5.07 (2.03–12.64) | <0.001 | 3.62 (1.26–10.41) | 0.017 | 7.00 (2.39–20.50) | <0.001 |
| Antibiotics | 22.83 (18.11–28.78) | <0.001 | 5.63 (4.30–7.37) | <0.001 | 10.87 (8.52–13.88) | <0.001 |
| Age, years | 1.08 (1.07–1.08) | <0.001 | 1.05 (1.04–1.06) | <0.001 | - | - |
| Male | 1.39 (1.21–1.60) | <0.001 | 1.60 (1.34–1.91) | <0.001 | - | - |
| DG area | 2.75 (2.35–3.23) | <0.001 | 0.94 (0.77–1.15) | 0.573 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-G.; Park, G.U.; Moon, Y.R.; Sung, K. Clinical Characteristics and Risk Factors for Fatality and Severity in Patients with Coronavirus Disease in Korea: A Nationwide Population-Based Retrospective Study Using the Korean Health Insurance Review and Assessment Service (HIRA) Database. Int. J. Environ. Res. Public Health 2020, 17, 8559. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228559
Lee S-G, Park GU, Moon YR, Sung K. Clinical Characteristics and Risk Factors for Fatality and Severity in Patients with Coronavirus Disease in Korea: A Nationwide Population-Based Retrospective Study Using the Korean Health Insurance Review and Assessment Service (HIRA) Database. International Journal of Environmental Research and Public Health. 2020; 17(22):8559. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228559
Chicago/Turabian StyleLee, Seung-Geun, Geun U. Park, Yeo Rae Moon, and Kihoon Sung. 2020. "Clinical Characteristics and Risk Factors for Fatality and Severity in Patients with Coronavirus Disease in Korea: A Nationwide Population-Based Retrospective Study Using the Korean Health Insurance Review and Assessment Service (HIRA) Database" International Journal of Environmental Research and Public Health 17, no. 22: 8559. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228559