Parenting Behavior at 18 Months Predicts Internalizing and Externalizing Problems at 6 Years in Moderately Preterm and Full Term Children



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.3.1. Parenting Behavior
2.3.2. Mother–child Interaction Quality
2.3.3. Behavior Problems
2.4. Statistical Analysis
3. Results
3.1. Demographic Information and Descriptive Statistics
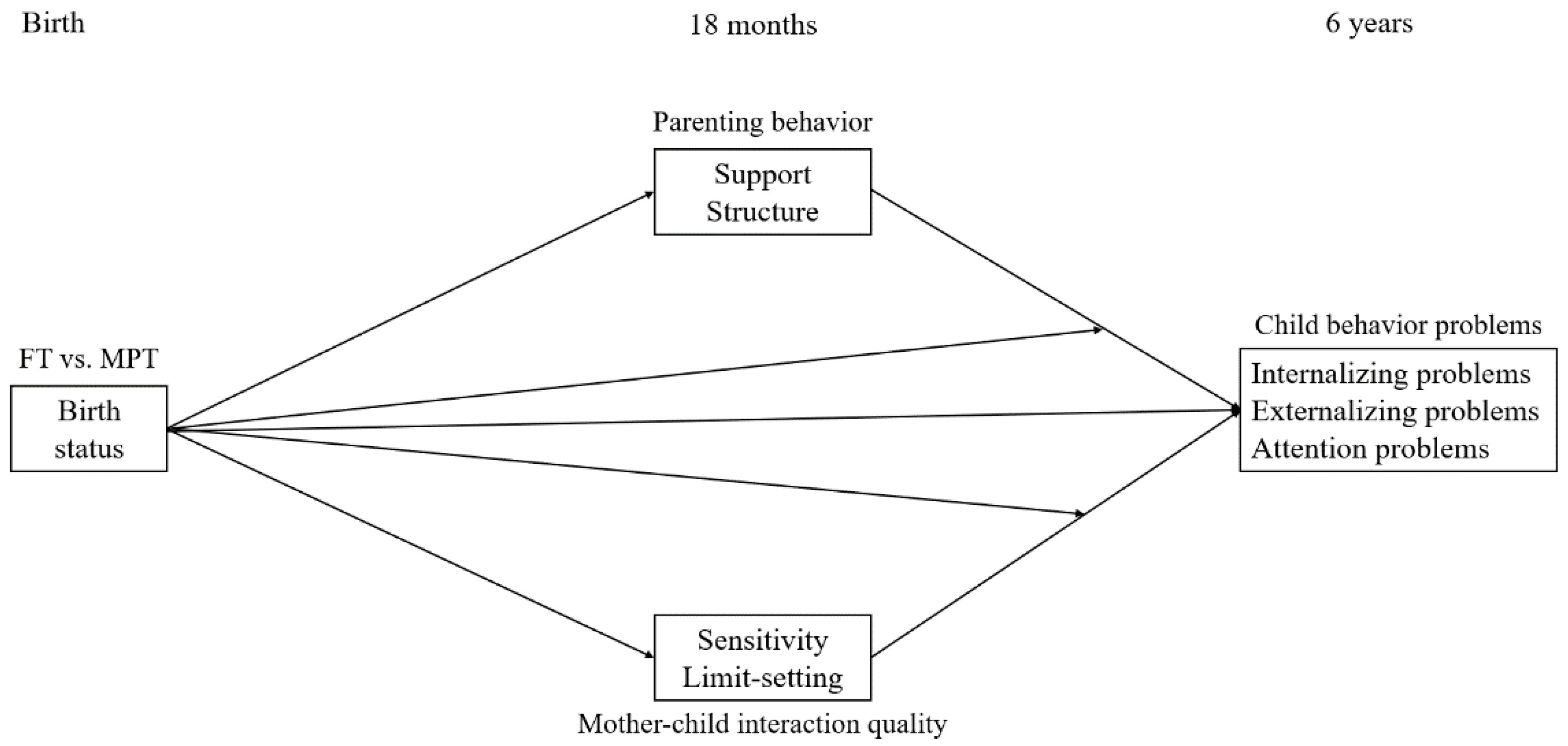
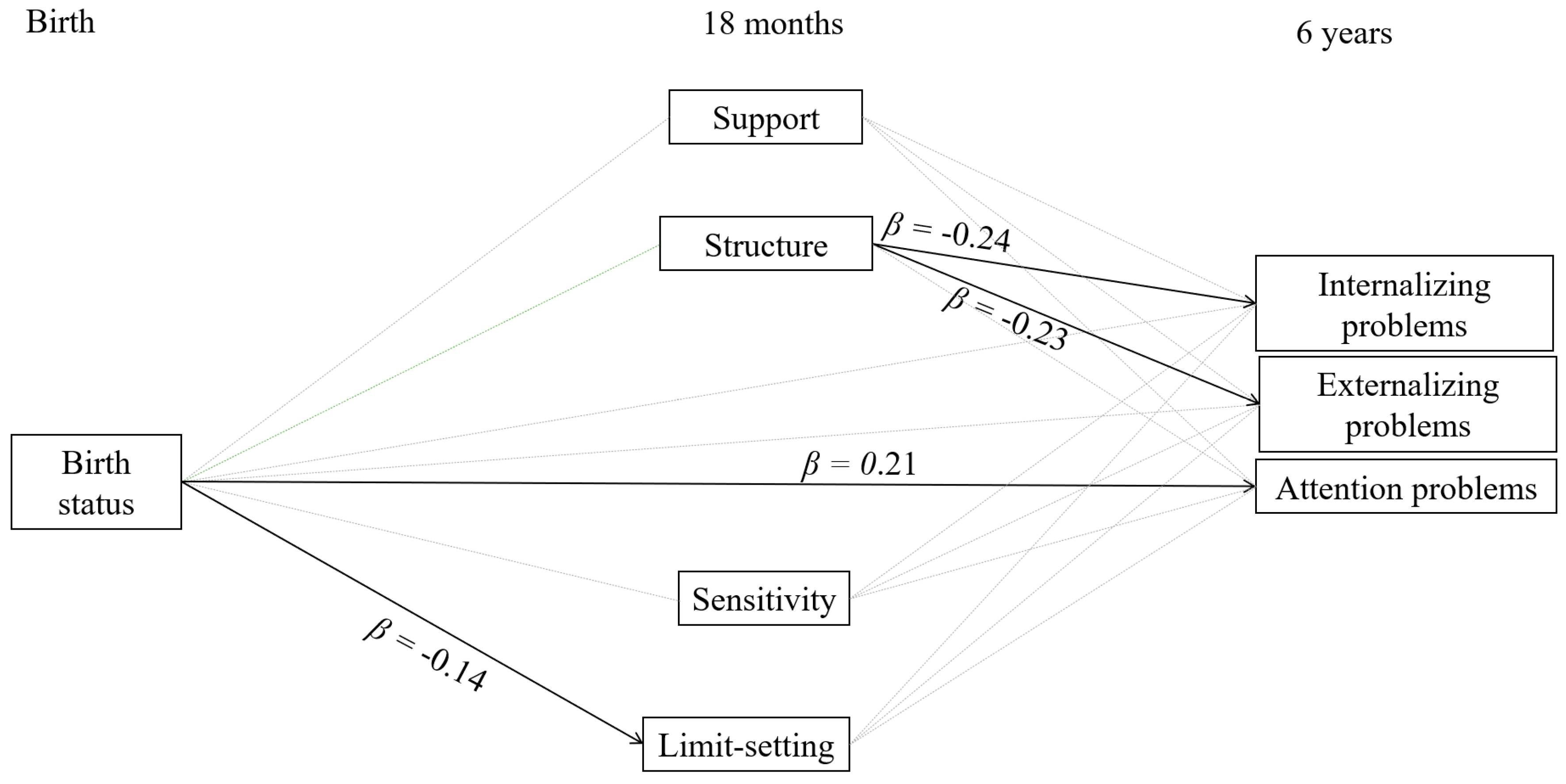
3.2. Associations between Birth Status, Parenting and Behavior Problems
3.3. Moderating Role of Birth Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef] [Green Version]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Shapiro-Mendoza, C.K.; Tomashek, K.M.; Kotelchuck, M.; Barfield, W.; Nannini, A.; Weiss, J.; Declercq, E. Effect of late-preterm birth and maternal medical conditions on newborn morbidity risk. Pediatrics 2008, 121, e223–e232. [Google Scholar] [CrossRef] [PubMed]
- De Jong, M.; Verhoeven, M.; van Baar, A.L. School outcome, cognitive functioning, and behaviour problems in moderate and late preterm children and adults: A review. Semin. Fetal Neonatal Med. 2012, 17, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Potijk, M.R.; de Winter, A.F.; Bos, A.F.; Kerstjens, J.M.; Reijneveld, S.A. Higher rates of behavioural and emotional problems at preschool age in children born moderately preterm. Arch. Dis. Child. 2012, 97, 112–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talge, N.M.; Holzman, C.; Wang, J.; Lucia, V.; Gardiner, J.; Breslau, N. Late-preterm birth and its association with cognitive and socioemotional outcomes at 6 years of age. Pediatrics 2010, 126, 1124–1131. [Google Scholar] [CrossRef]
- van Baar, A.L.; Vermaas, J.; Knots, E.; de Kleine, M.J.; Soons, P. Functioning at school age of moderately preterm children born at 32 to 36 weeks’ gestational age. Pediatrics 2009, 124, 251–257. [Google Scholar] [CrossRef]
- Gurka, M.J.; LoCasale-Crouch, J.; Blackman, J.A. Long-term cognition, achievement, socioemotional, and behavioral development of healthy late-preterm infants. Arch. Pediatr. Adolesc. Med. 2010, 164, 525–532. [Google Scholar] [CrossRef] [Green Version]
- Breslau, J.; Miller, E.; Breslau, N.; Bohnert, K.; Lucia, V.; Schweitzer, J. The impact of early behavior disturbances on academic achievement in high school. Pediatrics 2009, 123, 1472–1476. [Google Scholar] [CrossRef] [Green Version]
- Bosquet, M.; Egeland, B. The development and maintenance of anxiety symptoms from infancy through adolescence in a longitudinal sample. Dev. Psychopathol. 2006, 18, 517–550. [Google Scholar] [CrossRef] [Green Version]
- Anderson, V.; Northam, E.; Wrennall, J. Developmental Neuropsychology: A Clinical Approach; Routledge: New York, NY, USA, 2019. [Google Scholar]
- Walsh, J.M.; Doyle, L.W.; Anderson, P.J.; Lee, K.J.; Cheong, J.L. Moderate and late preterm birth: Effect on brain size and maturation at term-equivalent age. Radiology 2014, 273, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Rogers, C.E.; Anderson, P.J.; Thompson, D.K.; Kidokoro, H.; Wallendorf, M.; Treyvaud, K.; Roberts, G.; Doyle, L.W.; Neil, J.J.; Inder, T.E. Regional cerebral development at term relates to school-age social–emotional development in very preterm children. J. Am. Acad. Child. Adolesc. Psychiatry 2012, 51, 181–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, S.; Evans, T.A.; Draper, E.S.; Field, D.J.; Manktelow, B.N.; Marlow, N.; Matthews, R.; Petrou, S.; Seaton, S.E.; Smith, L.K.; et al. Neurodevelopmental outcomes following late and moderate prematurity: A population-based cohort study. Arch. Dis. Child. Fetal Neonatal Ed. 2015, 100, F301–F308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reidy, N.; Morgan, A.; Thompson, D.K.; Inder, T.E.; Doyle, L.W.; Anderson, P.J. Impaired language abilities and white matter abnormalities in children born very preterm and/or very low birth weight. J. Pediatr. 2013, 162, 719–724. [Google Scholar] [CrossRef] [Green Version]
- Sameroff, A. A unified theory of development: A dialectic integration of nature and nurture. Child. Dev. 2010, 81, 6–22. [Google Scholar] [CrossRef] [Green Version]
- Baumrind, D. Rearing competent children. In Child. Development Today and Tomorrow; Damon, W., Ed.; Jossey-Bass: San Francisco, CA, USA, 1988; pp. 349–378. [Google Scholar]
- Suchman, N.E.; Rounsaville, B.; DeCoste, C.; Luthar, S. Parental control, parental warmth, and psychosocial adjustment in a sample of substance-abusing mothers and their school-aged and adolescent children. J. Subst. Abuse Treat. 2007, 32, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Marcone, R.; Affuso, G.; Borrone, A. Parenting styles and children’s internalizing-externalizing behavior: The mediating role of behavioral regulation. Curr. Psychol. 2020, 39, 13–24. [Google Scholar] [CrossRef]
- Kok, R.; Linting, M.; Bakermans-Kranenburg, M.J.; van IJzendoorn, M.H.; Jaddoe, V.W.; Hofman, A.; Verhulst, F.C.; Tiemeier, H. Maternal sensitivity and internalizing problems: Evidence from two longitudinal studies in early childhood. Child. Psychiatry Hum. Dev. 2013, 44, 751–765. [Google Scholar] [CrossRef]
- Wang, F.; Christ, S.L.; Mills-Koonce, W.R.; Garrett-Peters, P.; Cox, M.J. Association between maternal sensitivity and externalizing behavior from preschool to preadolescence. J. Appl. Dev. Psychol. 2013, 34, 89–100. [Google Scholar] [CrossRef] [Green Version]
- Laucht, M.; Esser, G.; Schmidt, M. Developmental outcome of infants born with biological and psychosocial risks. J. Child. Psychiatry 2001, 38, 843–853. [Google Scholar] [CrossRef]
- Forcada-Guex, M.; Pierrehumbert, B.; Borghini, A.; Moessinger, A.; Muller-Nix, C. Early dyadic patterns of mother–infant interactions and outcomes of prematurity at 18 months. Pediatrics 2006, 118, e107–e114. [Google Scholar] [CrossRef] [Green Version]
- Muller-Nix, C.; Forcada-Guex, M.; Pierrehumbert, B.; Jaunin, L.; Borghini, A.; Ansermet, F. Prematurity, maternal stress and mother–child interactions. Early Hum. Dev. 2004, 79, 145–158. [Google Scholar] [CrossRef] [PubMed]
- Segal, L.B.; Oster, H.; Cohen, M.; Caspi, B.; Myers, M.; Brown, D. Smiling and fussing in seven-month-old preterm and full-term black infants in the still-face situation. Child. Dev. 1995, 66, 1829–1843. [Google Scholar] [CrossRef] [PubMed]
- Jaekel, J.; Wolke, D.; Chernova, J. Mother and child behaviour in very preterm and term dyads at 6 and 8 years. Dev. Med. Child. Neurol. 2012, 54, 716–723. [Google Scholar] [CrossRef] [Green Version]
- Monroe, S.M.; Simons, A.D. Diathesis-stress theories in the context of life-stress research: Implications for depressive disorders. Psychol. Bull. 1991, 110, 406–442. [Google Scholar] [CrossRef]
- Gueron-Sela, N.; Atzaba-Poria, N.; Meiri, G.; Marks, K. The caregiving environment and developmental outcomes of preterm infants: Diathesis stress or differential susceptibility effects? Child. Dev. 2015, 86, 1014–1030. [Google Scholar] [CrossRef]
- Jaekel, J.; Pluess, M.; Belsky, J.; Wolke, D. Effects of maternal sensitivity on low birth weight children’s academic achievement: A test of differential susceptibility versus diathesis stress. J. Child. Psychol. Psychiatry 2015, 56, 693–701. [Google Scholar] [CrossRef]
- Belsky, J.; Bakermans-Kranenburg, M.J.; van IJzendoorn, M.H. For better and for worse. Differential susceptibility to environmental influences. Curr. Dir. Psychol. Sci. 2007, 16, 300–304. [Google Scholar] [CrossRef] [Green Version]
- Maupin, A.N.; Fine, J.G. Differential effects of parenting in preterm and full-term children on developmental outcomes. Early Hum. Dev. 2014, 90, 869–876. [Google Scholar] [CrossRef]
- Treyvaud, K.; Doyle, L.W.; Lee, K.J.; Ure, A.; Inder, T.E.; Hunt, R.W.; Anderson, P.J. Parenting behavior at 2 years predicts school-age performance at 7 years in very preterm children. J. Child. Psychol. Psychiatry 2016, 57, 814–821. [Google Scholar] [CrossRef]
- Bogičević, L.; Verhoeven, M.; van Baar, A.L. Toddler skills predict moderate-to-late preterm born children’s cognition and behaviour at 6 years of age. PLoS ONE 2019, 14. [Google Scholar] [CrossRef]
- Perined. Perinatal care in The Netherlands. 2015. Available online: https://www.perined.nl/producten/geboortegewichtcurven (accessed on 11 February 2020).
- Verhoeven, M.; Deković, M.; Bodden, D.; van Baar, A.L. Development and initial validation of the comprehensive early childhood parenting questionnaire (CECPAQ) for parents of 1–4 year-olds. Eur. J. Dev. Psychol. 2017, 14, 233–247. [Google Scholar] [CrossRef] [Green Version]
- Feldman, R. Coding Interactive Behavior Manual; Bar-Ilan University: Ramat Gan, Israel, 1998. [Google Scholar]
- Feldman, R.; Klein, P.S. Toddlers’ self-regulated compliance to mothers, caregivers, and fathers: Implications for theories of socialization. Dev. Psychol. 2003, 39, 680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldman, R.; Weller, A.; Sirota, L.; Eidelman, A.I. Testing a family intervention hypothesis: The contribution of mother–infant skin-to-skin contact (Kangaroo Care) to family interaction and touch. J. Fam. Psychol. 2003, 17, 94–107. [Google Scholar] [CrossRef] [PubMed]
- Verhulst, F.C.; van der Ende, J. Handleiding ASEBA-Vragenlijsten voor Leeftijden 6 t/m 18 jaar: CBCL6/18, YSR en TRF; Erasmus MC: Rotterdam, The Nederlands, 2013. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 6th ed.; Pearson Education: Boston, MA, USA, 2012. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 1998–2017. [Google Scholar]
- Belsky, J.; Bell, B.; Bradley, R.H.; Stallard, N.; Stewart-Brown, S.L. Socioeconomic risk, parenting during the preschool years and child health age 6 years. Eur. J. Public Health 2007, 17, 508–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Letourneau, N.L.; Duffett-Leger, L.; Levac, L.; Watson, B.; Young-Morris, C. Socioeconomic status and child development: A meta-analysis. J. Emot. Behav. Disord. 2013, 21, 211–224. [Google Scholar] [CrossRef]
- Morgen, C.S.; Bjørk, C.; Andersen, P.K.; Mortensen, L.H.; Nybo Andersen, A.M. Socioeconomic position and the risk of preterm birth—A study within the Danish National Birth Cohort. Int. J. Epidemiol. 2008, 37, 1109–1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Korja, R.; Latva, R.; Lehtonen, L. The effects of preterm birth on mother–infant interaction and attachment during the infant’s first two years. Acta Obstet. Gynecol. Scand. 2012, 91, 164–173. [Google Scholar] [CrossRef]
- Berg-Nielsen, T.S.; Vikan, A.; Dahl, A.A. Parenting related to child and parental psychopathology: A descriptive review of the literature. Clin. Child. Psychol. Psychiatry 2002, 7, 529–552. [Google Scholar] [CrossRef]
- Goodwin, L.D.; Leech, N.L. Understanding correlation: Factors that affect the size of r. J. Exp. Educ. 2006, 74, 249–266. [Google Scholar] [CrossRef]
- Gardner, F. Methodological issues in the direct observation of parent–child interaction: Do observational findings reflect the natural behavior of participants? Clin. Child. Fam. Psychol. Rev. 2000, 3, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, N.J.; Volling, B.L.; Barr, R. Fathers are parents, too! Widening the lens on parenting for children’s development. Child. Dev. Perspect. 2018, 12, 152–157. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Participants’ Characteristics | FT (n = 100) | MPT (n = 120) |
|---|---|---|
| Corrected age in months at wave 1 | ||
| Mean (SD) | 17.5 (0.5) | 17.5 (0.5) |
| Range | 17–18 | 17–19 |
| Corrected age in months at wave 2 | ||
| Mean (SD) | 72.9 (0.8) | 72.7 (0.6) * |
| Range | 71.6–75.5 | 71.4–74.6 |
| Gestational age | ||
| Mean (SD) | 39.5 (1.0) | 34.7 (1.3) *** |
| 32 weeks (%) | 10.0% | |
| 33 weeks (%) | 10.8% | |
| 34 weeks (%) | 16.7% | |
| 35 weeks (%) | 25.0% | |
| 36 weeks (%) | 37.5% | |
| 37 weeks (%) | 4.0% | |
| 38 weeks (%) | 10.0% | |
| 39 weeks (%) | 32.0% | |
| 40 weeks (%) | 41.0% | |
| 41 weeks (%) | 13.0% | |
| Birth weight in grams | ||
| Mean (SD) | 3578.0 (456.1) | 2594.3 (515.5) *** |
| Range | 2795–5330 | 1420–3850 |
| Need for oxygen a (%) | 0% | 21.7% *** |
| Phototherapy (%) | 0% | 35.7% *** |
| Hypoglycemia (%) | 0% | 4.8% * |
| Maternal antenatal tobacco use | ||
| No smoking during pregnancy | 92.1% | 91.8% |
| Quit smoking during pregnancy | 5.0% | 0.8% |
| Occasional smoking during pregnancy | 1.0% | 4.9% |
| Days in hospital | ||
| Mean (SD) | 0.41 (1.0) | 11.8 (9.9) *** |
| Range | 0–6 | 1–42 |
| Gender (% boys) | 45.0% | 57.5% |
| Ethnic origin (% Dutch) | 96.0% | 96.7% |
| First born (%) | 52.0% | 63.3% |
| Maternal age at birth | ||
| Mean (SD) | 32.5 (4.2) | 31.1 (4.5) * |
| Range | 20–43 | 21–41 |
| Maternal educational level | ||
| Low b (%) | 3.0% | 9.2% |
| Average c (%) | 11.% | 35.0% *** |
| High d (%) | 86.0% | 55.8% *** |
| FT | MPT | FT | MPT | |||
|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Min | Max | Min | Max | |
| Parenting behavior at 18 months | ||||||
| Support | 5.08 (0.36) | 5.07 (0.43) | 4.23 | 5.85 | 4 | 6 |
| Structure | 4.95 (0.46) | 4.94 (0.48) | 3.83 | 5.92 | 3.67 | 5.83 |
| Mother–child interaction quality at 18 months | ||||||
| Sensitivity | 4.55 (0.38) | 4.50 (0.35) | 3.21 | 5 | 3.21 | 5 |
| Limit-setting | 4.26 (0.51) | 4.10 (0.60) | 2.83 | 5 | 2.50 | 5 |
| Behavior problems at 6 years | ||||||
| Attention problems | 52.95 (4.03) | 55.12 (5.76) | 50 | 70 | 50 | 71 |
| Internalizing problems | 45.20 (9.02) | 47.60 (9.75) | 33 | 74 | 33 | 74 |
| Externalizing problems | 45.72 (10.05) | 46.12 (9.06) | 34 | 76 | 34 | 68 |
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | |
|---|---|---|---|---|---|---|---|---|---|
| - | −0.01 | −0.01 | −0.06 | −0.14 * | 0.13 | 0.02 | 0.21 ** | −0.33 ** |
| - | 0.28 ** | −0.01 | −0.10 | −0.12 | −0.09 | −0.03 | 0.06 | |
| - | 0.14 * | 0.13 | −0.23 ** | −0.22 ** | −0.10 | 0.10 | ||
| - | 0.48 ** | 0.09 | 0.04 | 0 | 0.15 ** | |||
| - | 0.04 | −0.11 | −0.04 | 0.08 | ||||
| - | 0.46 ** | 0.37 ** | −0.06 | |||||
| - | 0.54 ** | 0.07 | ||||||
| - | −0.15 | |||||||
| - |
| Variable | B | SE of B | β | 95% CI Low | 95% CI High |
|---|---|---|---|---|---|
| Birth status → Internalizing problems | 2.55 | 1.54 | 0.13 | −0.51 | 5.67 |
| Support → Internalizing problems | −1.60 | 2.05 | −0.07 | −5.93 | 1.99 |
| Structure → Internalizing problems | −4.83 | 1.77 | −0.24 | −8.33 | −1.33 |
| Sensitivity → Internalizing problems | 3.09 | 2.37 | 0.12 | −1.33 | 7.70 |
| Limit-setting → Internalizing problems | 0.19 | 1.52 | 0.01 | −2.85 | 3.02 |
| Birth status → Externalizing problems | 0.09 | 1.49 | 0 | −2.77 | 2.86 |
| Support → Externalizing problems | −1.07 | 1.88 | −0.04 | −4.86 | 2.87 |
| Structure → Externalizing problems | −4.63 | 1.57 | −0.23 | −7.49 | −1.32 |
| Sensitivity → Externalizing problems | 3.60 | 2.28 | 0.14 | −0.86 | 8.05 |
| Limit-setting → Externalizing problems | −2.73 | 1.55 | −0.16 | −5.57 | 0.64 |
| Birth status → Attention problems | 2.14 | 0.79 | 0.21 | 0.75 | 3.92 |
| Support → Attention problems | −0.35 | 0.94 | −0.03 | −2.30 | 1.34 |
| Structure → Attention problems | −0.98 | 1.01 | −0.09 | −3.00 | 1.04 |
| Sensitivity → Attention problems | 0.51 | 1.31 | 0.04 | −2.13 | 3.01 |
| Limit-setting → Attention problems | −0.32 | 0.91 | −0.04 | −2.14 | 1.39 |
| Birth status → Support | −0.01 | 0.05 | −0.01 | −0.12 | 0.09 |
| Birth status → Structure | −0.01 | 0.06 | −0.01 | −0.12 | 0.13 |
| Birth status → Sensitivity | −0.02 | 0.05 | −0.03 | −0.12 | 0.09 |
| Maternal education → Sensitivity | 0.10 | 0.06 | 0.13 | −0.01 | 0.21 |
| Birth status → Limit-setting | −0.16 | 0.08 | −0.14 | −0.30 | −0.01 |
Support  Structure Structure | 0.05 | 0.01 | 0.28 | 0.03 | 0.07 |
Support  Limit-setting Limit-setting | −0.02 | 0.01 | −0.10 | −0.05 | 0.01 |
| Support Sensitivity | 0 | 0 | −0.03 | −0.02 | 0.01 |
| Sensitivity Limit-setting | 0.10 | 0.01 | 0.47 | 0.07 | 0.12 |
| Sensitivity Structure | 0.02 | 0.01 | 0.13 | 0 | 0.04 |
| Limit-setting Structure | 0.03 | 0.02 | 0.12 | 0 | 0.06 |
| Birth status Maternal education | −0.08 | 0.01 | −0.33 | −0.11 | −0.05 |
| Externalizing problems Internalizing problems | 35.57 | 8.02 | 0.43 | 21.74 | 54.14 |
| Attention problems Internalizing problems | 15.11 | 4.73 | 0.34 | 7.47 | 26.80 |
| Attention problems Externalizing problems | 24.48 | 5.46 | 0.54 | 15.50 | 38.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oosterom, L.; Bogičević, L.; Verhoeven, M.; van Baar, A.L. Parenting Behavior at 18 Months Predicts Internalizing and Externalizing Problems at 6 Years in Moderately Preterm and Full Term Children. Int. J. Environ. Res. Public Health 2020, 17, 8679. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228679
Oosterom L, Bogičević L, Verhoeven M, van Baar AL. Parenting Behavior at 18 Months Predicts Internalizing and Externalizing Problems at 6 Years in Moderately Preterm and Full Term Children. International Journal of Environmental Research and Public Health. 2020; 17(22):8679. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228679
Chicago/Turabian StyleOosterom, Lisa, Lilly Bogičević, Marjolein Verhoeven, and Anneloes L. van Baar. 2020. "Parenting Behavior at 18 Months Predicts Internalizing and Externalizing Problems at 6 Years in Moderately Preterm and Full Term Children" International Journal of Environmental Research and Public Health 17, no. 22: 8679. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228679