Multimorbidity, Loneliness, and Social Isolation. A Systematic Review


Department of Health Economics and Health Services Research, University Medical Center Hamburg-Eppendorf, Martinistraße 52, 20246 Hamburg, Germany
*
Author to whom correspondence should be addressed.
Int. J. Environ. Res. Public Health 2020, 17(22), 8688; https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228688
Submission received: 21 October 2020
/
Revised: 11 November 2020
/
Accepted: 20 November 2020
/
Published: 23 November 2020
(This article belongs to the Special Issue Depressive Symptoms, Cognitive Functioning, Frailty, Multimorbidity and Loneliness among Older Population)
Abstract
:No systematic review has appeared so far synthesizing the evidence regarding multimorbidity and loneliness, social isolation, or social frailty. Consequently, our aim was to fill this gap. Three electronic databases (PubMed, PsycINFO, and CINAHL) were searched in our study. Observational studies examining the link between multimorbidity and loneliness, social isolation, and social frailty were included, whereas disease-specific samples were excluded. Data extraction included methods, characteristics of the sample, and the main results. A quality assessment was conducted. Two reviewers performed the study selection, data extraction, and quality assessment. In sum, eight studies were included in the final synthesis. Some cross-sectional and longitudinal studies point to an association between multimorbidity and increased levels of loneliness. However, the associations between multimorbidity and social isolation as well as social frailty remain largely underexplored. The quality of the studies included was rather high. In conclusion, most of the included studies showed a link between multimorbidity and increased loneliness. However, there is a lack of studies examining the association between multimorbidity and social isolation as well as social frailty. Future studies are required to shed light on these important associations. This is particularly important in times of the COVID-19 pandemic.
1. Introduction
There are several similar concepts concentrating on the social needs of individuals [1]. Specifically, social isolation, loneliness, and social frailty exist. While social isolation can be defined as the feeling that an individual does not belong to the society [2], loneliness refers to the feeling that an individual’s social network is smaller or of poorer quality than preferred [2], and social frailty refers to the lack of resources to fulfill one’s basic social needs [1]. Given the fact that traditional family bonds become ruptured, new challenges arise for individuals. It should be emphasized that these social needs are associated with physical frailty and subsequent mortality [3,4]. In sum, these social needs have been considered as new geriatric giants [5]. Moreover, social needs can also have deleterious consequences for younger individuals.
Previous studies have determined several factors associated with these social needs. For example, it has been shown that they are, among other things, associated with income poverty or experiencing a fall [6,7]. Moreover, it has been shown that they are associated with multimorbidity (e.g., [8,9,10]),
Multimorbidity is commonly defined as the existence of at least two chronic illnesses [11]. The prevalence of multimorbidity is rather high in adults, especially in very old individuals [12,13]. According to a systematic review, the prevalence of multimorbidity in older individuals ranges from 55% to 98% [14]. The prevalence also increases in women and people from low social classes [14]. Little is known about the genetic and biological risk factors for multimorbidity [14]. In light of the demographic aging in high-income countries, it is projected that the number of individuals with multimorbidity will increase. Multimorbidity is also linked to disability [14], mortality [15], and high health care costs [16].
While some observational studies exist examining the link between multimorbidity and social needs (in terms of social isolation, loneliness, and social frailty) [8,9,10], there is a lack of a study systematically synthesizing observational studies investigating these associations. Thus, our objective of this systematic review was to fill this gap in knowledge.
Particularly in times of the COVID-19 pandemic, knowledge about the link between multimorbidity and loneliness, social isolation, or social frailty is of great importance. This can be explained by the fact that the case fatality rate increases considerably with age. Consequently, older adults are quite often forced to avoid physical contact to stay at home.
2. Materials and Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols guidelines [17] and is registered with the International Prospective Register of Systematic Reviews (PROSPERO, registration number: CRD42020179918).
2.1. Search Strategy and Selection Criteria
In July and August 2020, a systematic literature search was conducted based on three databases (Medline, PsycINFO, and CINAHL). In Table 1, the search query for Medline is depicted.
Two reviewers (AH, BK) evaluated the studies for inclusion/exclusion using a two-step process. First, a title/abstract screening was performed. Second, a full-text screening was conducted. Furthermore, we hand searched the reference lists of studies selected for inclusion. If disagreements occurred, we used discussions to resolve it (and, if required, included a third party (HHK)).
We had the following inclusion criteria:
- Cross-sectional and longitudinal observational studies investigating the association between (1) multimorbidity and social frailty, or (2) multimorbidity and loneliness, or (3) multimorbidity and social isolation.
- Studies appropriately quantifying important variables like social isolation.
- Studies published in peer-reviewed journals (English or German language).
Exclusion criteria were:
- Studies not investigating the association between (1) multimorbidity and social frailty, or (2) multimorbidity and loneliness, or (3) multimorbidity and social isolation.
- Studies exclusively investigating samples with a specific disorder.
- Study design other than observational.
- Inappropriate assessment of important variables.
Selection criteria did not include any restrictions regarding place and time during which studies were conducted. Using a sample of 100 titles/abstracts, we conducted a pre-testing of eligibility criteria. Results of this pre-testing did not affect the final eligibility criteria list.
2.2. Data Extraction and Analysis
One reviewer (BK) conducted the data extraction. A second reviewer (AH) cross-checked the extracted data. If disagreements occurred, discussions were held to reach a consensus. If required, a third party (HHK) was included. If clarification was needed, we contacted the study authors.
Data extraction covered study design, measures, analytical approach, description of the sample, and key results. We present the key results as follows (in each case: (i) cross-sectional, and (ii) longitudinal):
- (1)
- multimorbidity and loneliness.
- (2)
- multimorbidity and social isolation.
- (3)
- multimorbidity and social frailty.
2.3. Quality Assessment
The study quality was assessed independently by two reviewers (AH, BK) based on the well-known and widely used NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies [18]. In case of disagreement, discussions were held to resolve the conflict. A third party (HHK) was included in such discussions as needed.
3. Results
This section is divided by subheadings. It provides a concise and precise description of the experimental results, their interpretation as well as the experimental conclusions that can be drawn.
3.1. Overview of Included Studies
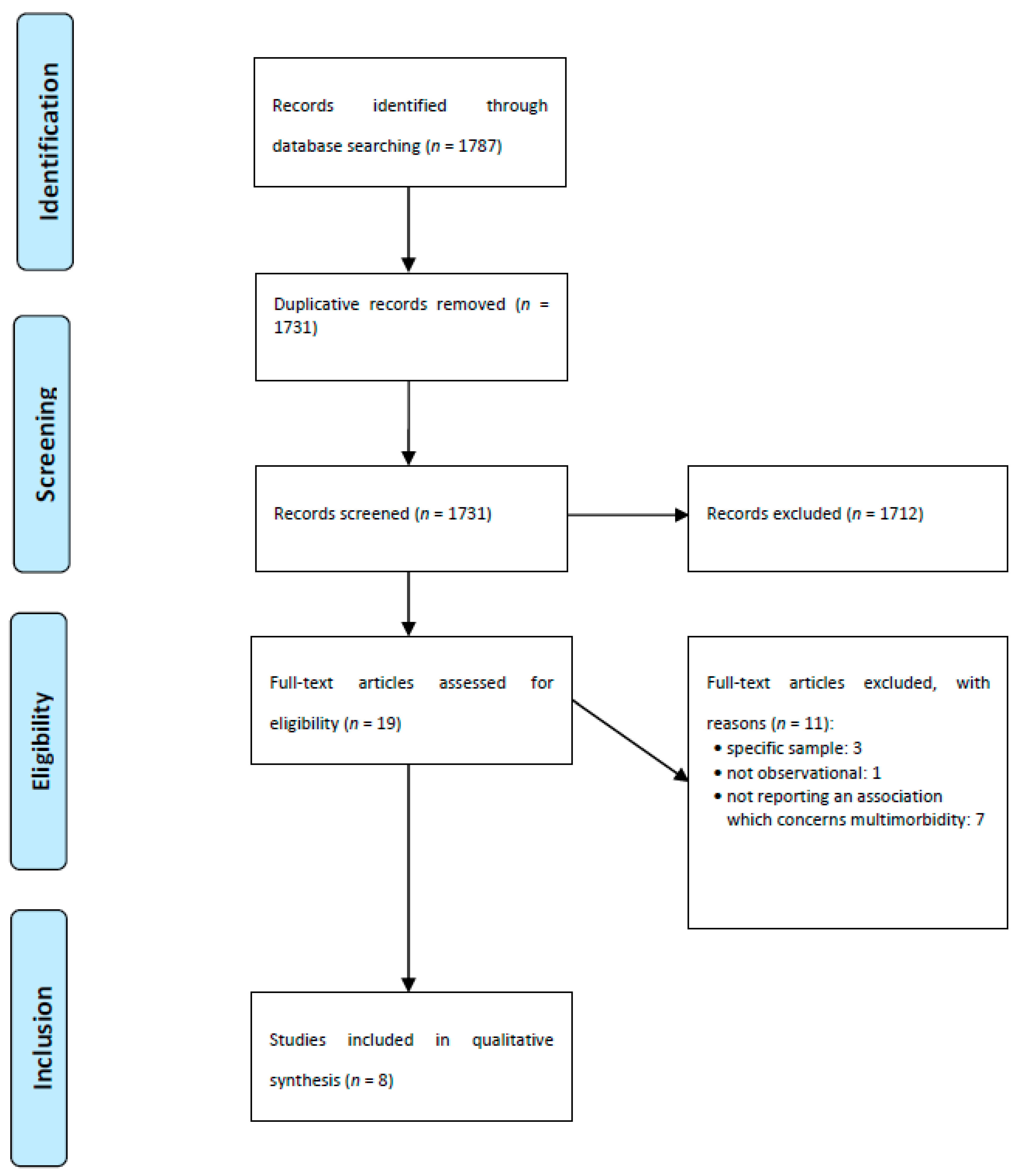
The study selection process is shown in Figure 1 [19]. In sum, n = 8 studies were included in the final synthesis of our review. Important characteristics and key results of the studies included are given in Table 2. If reported, adjusted results are displayed.
Data stemmed from Europe (n = 6, with two studies from Germany, and one study each from Denmark, Netherlands, Spain and the United Kingdom) and North America (n = 2 studies from Canada). Equally, four cross-sectional and four longitudinal studies were identified. The observation period in the longitudinal studies varied from three to twelve years. It should be noted that while one study used cross-sectional data from the German Aging Survey (year 2014) [20], the second longitudinal study used data from 2002 to 2014 from the German Aging Survey [9]. Multimorbidity was commonly defined as having two or more chronic conditions.
One study reported on data from individuals recruited from a general practice [21], another analyzed data from a heterogeneous sample of community-dwelling older adults [22], and all others conveyed results from large, nationally representative samples of community-dwelling older adults. The sample size ranged from 121 to 36,397 individuals, the proportion of women in the samples ranged from 49% to 56%, and the average age ranged from 60 to 77 years. Further details are given in Table 2.
In the next sections, key results are presented as follows (in each case: (i) cross-sectional, and (ii) longitudinal):
- (1)
- multimorbidity and loneliness.
- (2)
- multimorbidity and social isolation.
- (3)
- multimorbidity and social frailty.
3.2. Multimorbidity and Loneliness
With regard to cross-sectional studies, five studies examined the link between multimorbidity and loneliness [20,21,23,24,25]. Three out of these five studies found a positive association between multimorbidity and loneliness. In contrast, one study did not find a bivariate association between multimorbidity and loneliness [24], and another study did not identify such a link using multiple regressions [21].
With regard to sex differences, one cross-sectional study [25] showed that loneliness was associated with multimorbidity in middle-aged and older (i.e., 45 to 54 years, 55 to 64 years, 65 to 74 years and 75+) men and women in Canada and Australia (except for Australian men aged 75+). However, this study did not include interaction terms to test whether potential sex differences were significant [25]. The remaining studies [20,21,23,24] only adjusted for sex.
3.3. Multimorbidity and Social Isolation
With regard to cross-sectional studies, only one study examined the link between multimorbidity and social isolation [9]. This study found an association between multimorbidity and increased social isolation. In contrast, there was a lack of longitudinal studies investigating the link between multimorbidity and social isolation. Sex differences were not examined.
3.4. Multimorbidity and Social Frailty
Our systematic review did not identify either cross-sectional or longitudinal studies examining the link between multimorbidity and social frailty.
3.5. Quality Assessment
The evaluation of study quality of the included studies is shown in Table 3. While some criteria were fulfilled by all studies (e.g., adjustment for important covariates), some other criteria were only fulfilled by a few studies (e.g., response rate ≥50%). However, the general study quality was rather high. More precisely, the study quality of five studies were rated as ‘good’ and three studies were rated as ‘fair’, which also means that none of the studies were rated as ‘poor’.
4. Discussion
In sum, eight studies were included in the final synthesis. Some cross-sectional and longitudinal studies pointed to an association between multimorbidity and increased levels of loneliness. However, the associations between multimorbidity and social isolation as well as social frailty remain largely underexplored. The quality of the studies included was rather high. For example, several studies used data from nationally representative samples like the English Longitudinal Study of Aging [26] or the German Aging Survey [9].
The link between multimorbidity and loneliness appears to be plausible. For example, as stated by Barlow et al. [22], multimorbidity is associated with lower physical functioning, which may affect loneliness. However, this factor was commonly adjusted for in the studies examined. Another possible explanation may be that loneliness is rather associated with the quality of the relationships, but not with the quantity [27]. This means that multimorbidity may affect loneliness by reducing the relationship quality [9]. In the same vein, a qualitative study demonstrated that the social networks among individuals with multimorbidity were rather large and diverse (including health care professionals) [28]. These presumably one-sided relationships to health care professionals may reflect a decreased relationship quality among individuals with multimorbidity [9]. Jessen et al. [23] provided an additional explanation: Individuals with multimorbidity have to cope with symptoms and have frequent contact with the health care system, which can restrict participation in social activities [29]. Moreover, individuals with multimorbidity may leave the labor market, which can markedly reduce the everyday contact with colleagues [23].
Olaya et al. [24] provided two possible explanations for the association between social needs and multimorbidity. First, according to the buffering hypothesis, social needs can buffer the negative impact of stress on health [30]. Moreover, another explanation may be that social factors can assist in regulating health behavior and can increase the access to health care (e.g., transportation or financial support) [31]. Equal explanations are given by Singer et al. [26] and Jessen et al. [23]. Additionally, Jessen et al. stated that loneliness can cause emotional changes, which in turn affect multimorbidity [32]. These emotional changes can activate neurobiological and behavioral mechanisms that can decrease health [32].
Depending on the proposed directionality, conclusions in the included studies varied from (i) proposing efforts to decrease loneliness to reduce multimorbidity [26] to (ii) tackling multimorbidity to reduce loneliness [9]. Moreover, (iii) the need for future, longitudinal studies [20] and (iv) studies elucidating the underlying mechanisms was stressed [9].
The comparability of the included studies was somewhat restricted. Different tools were used to assess loneliness scores. For instance, while some studies used the De Jong Gierveld scale [33], other studies used the UCLA scale [34]. Both scales conceptualize loneliness as subjective. Nevertheless, while the UCLA scale views loneliness mainly as affective, the De Jong Gierveld scale views it as cognitive [35]. A previous study concluded that the latter scale might be a better choice for cross-sectional and longitudinal studies when focusing on middle-aged and older adults [35].
Both German studies used the 6-item version of the De Jong Gierveld loneliness scale [9,20]. These studies showed that multimorbidity was associated with increased loneliness both cross-sectionally and longitudinally. Apart from these studies, different tools (or different versions of the UCLA loneliness scale) were used to quantify loneliness.
Moreover, with regard to comparability, while multimorbidity was very consistently defined as the presence of two or more chronic conditions, the list of diseases ranged from eight to 25 diseases, which may have an impact on the results. Moreover, the assessment of chronic conditions mostly refers to self-ratings in the studies examined. The samples included were quite comparable with regard to the proportion of female individuals and age bracket (mainly including individuals in middle- and old age). Furthermore, there were some differences in the analytical approach used (for example, fixed effects regressions vs. the use of generalized estimating equations (GEE)), which in turn can have quite a large impact on the results [36]. For example, using fixed effects strategies when panel data are present may assist in identifying the link between the onset of multimorbidity and loneliness, social isolation, and social frailty [36].
Our systematic review identified possible gaps in knowledge. More precisely, there is a general gap in knowledge regarding the associations between (i) multimorbidity and social isolation (including tools to quantify “objective social isolation” [37]) and (ii) multimorbidity and social frailty. Moreover, as, for example, proposed by Kristensen et al. [20], the directionality between these factors should be further explored. It appears plausible that the onset of multimorbidity may increase feelings of e.g., social isolation. However, it also appears plausible that feelings of social isolation reduce, among other things, physical activities, which can in turn contribute to the occurrence of chronic illnesses or multimorbidity [9]. Future longitudinal studies using advanced methods like dynamic panel data estimation strategies [38] may assist in clarifying this issue. This knowledge may have important policy implications and, for example, may assist in reducing the social and economic burden caused by loneliness, social isolation, and social frailty. Furthermore, most studies used data from European countries. Therefore, future research is needed from other regions (like Asian, South American, or African countries). It may be the case that the link between multimorbidity and social needs is moderated by cultural background. Wister et al. [25] also proposed that future research should focus on different age group cohorts. Moreover, they proposed that the role of sex should be clarified [25], since men tended to be more stoic [39]. Furthermore, factors such as health literacy [40] (including social support for health [41]) or coping strategies such as flexible goal adjustment [42,43] may act as a moderator of the relationship between multimorbidity and social needs.
Additionally, the link between multimorbidity patterns or clusters (i.e., combination of (i) mental health problems, (ii) musculoskeletal disorders as well as (iii) cardiovascular and metabolic diseases) and social needs should be further explored in future studies [44].
Some strengths of our systematic review are worth highlighting. This is the first systematic review focusing on the link between multimorbidity and loneliness, social isolation, and social frailty. Key steps were performed by two reviewers (e.g., steps like study selection or data extraction). Furthermore, we conducted a quality assessment. Due to study heterogeneity, a meta-analysis was not performed. Due to the restriction to peer-reviewed articles, which ascertains a rather high quality, at least some previous findings (e.g., from grey literature) might be lacking. Moreover, due to the restriction to studies published in English or German language, relevant studies published in other languages (e.g., French language) were not included in this work.
5. Conclusions
Most of the included studies showed a link between multimorbidity and increased loneliness. However, there is a lack of studies examining the association between multimorbidity and social isolation as well as social frailty. Future studies are required to shed light on these important associations. This is particularly important in times of the COVID-19 pandemic. Upcoming studies should explore the role of factors such as social distancing or perceptions of safe practices in the link between multimorbidity and social needs.
Author Contributions
The study concept was developed by A.H., B.K., and H.-H.K. The manuscript was drafted by A.H. and critically revised by B.K. and H.-H.K. The search strategy was developed by A.H. and H.-H.K. Study selection, data extraction, and quality assessment were performed by A.H. and B.K., with H.-H.K. as a third party in the case of disagreements. A.H., B.K., and H.-H.K. contributed to the interpretation of the extracted data and writing of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bunt, S.; Steverink, N.; Olthof, J.; van der Schans, C.; Hobbelen, J. Social frailty in older adults: A scoping review. Eur. J. Ageing 2017, 14, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Wenger, G.C.; Davies, R.; Shahtahmasebi, S.; Scott, A. Social isolation and loneliness in old age: Review and model refinement. Ageing Soc. 1996, 16, 333–358. [Google Scholar] [CrossRef] [Green Version]
- Gale, C.R.; Westbury, L.; Cooper, C. Social isolation and loneliness as risk factors for the progression of frailty: The English Longitudinal Study of Ageing. Age Ageing 2018, 47, 392–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoogendijk, E.O.; Smit, A.P.; van Dam, C.; Schuster, N.A.; de Breij, S.; Holwerda, T.J.; Huisman, M.; Dent, E.; Andrew, M.K. Frailty Combined with Loneliness or Social Isolation: An Elevated Risk for Mortality in Later Life. J. Am. Geriatr. Soc. 2020, 68, 2587–2593. [Google Scholar] [CrossRef] [PubMed]
- Freedman, A.; Nicolle, J. Social isolation and loneliness: The new geriatric giants: Approach for primary care. Can. Fam. Physician 2020, 66, 176–182. [Google Scholar] [PubMed]
- Hajek, A.; König, H.-H. Does the beginning and the end of income poverty affect psychosocial factors among middle-aged and older adults? Findings based on nationally representative longitudinal data. Aging Ment. Health 2020, 1–7. [Google Scholar] [CrossRef]
- Petersen, N.; König, H.-H.; Hajek, A. The link between falls, social isolation and loneliness: A systematic review. Arch. Gerontol. Geriatr. 2020, 88, 104020. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J.; Shmotkin, D.; Goldberg, S. Loneliness in old age: Longitudinal changes and their determinants in an Israeli sample. Int. Psychogeriatr. 2009, 21, 1160–1170. [Google Scholar] [CrossRef]
- Kristensen, K.; König, H.H.; Hajek, A. The longitudinal association of multimorbidity on loneliness and network size: Findings from a population-based study. Int. J. Geriatr. Psychiatry 2019, 34, 1490–1497. [Google Scholar] [CrossRef]
- Stickley, A.; Koyanagi, A. Physical multimorbidity and loneliness: A population-based study. PLoS ONE 2018, 13, e0191651. [Google Scholar] [CrossRef]
- van den Akker, M.; Buntinx, F.; Knottnerus, J.A. Comorbidity or multimorbidity: What’s in a name? A review of literature. Eur. J. Gen. Pract. 1996, 2, 65–70. [Google Scholar] [CrossRef]
- Rijken, M.; Struckmann, V.; Dyakova, M.; Melchiorre, M.G.; Rissanen, S.; Ginneken, E.V. Improving care for people with multiple chronic conditions in Europe. Eurohealth 2014, 20, 35–40. [Google Scholar]
- Puth, M.-T.; Weckbecker, K.; Schmid, M.; Münster, E. Prevalence of multimorbidity in Germany: Impact of age and educational level in a cross-sectional study on 19,294 adults. BMC Public Health 2017, 17, 826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marengoni, A.; Angleman, S.; Melis, R.; Mangialasche, F.; Karp, A.; Garmen, A.; Meinow, B.; Fratiglioni, L. Aging with multimorbidity: A systematic review of the literature. Ageing Res. Rev. 2011, 10, 430–439. [Google Scholar] [CrossRef]
- Holt-Lunstad, J.; Smith, T.B.; Baker, M.; Harris, T.; Stephenson, D. Loneliness and social isolation as risk factors for mortality: A meta-analytic review. Perspect. Psychol. Sci. 2015, 10, 227–237. [Google Scholar] [CrossRef] [Green Version]
- Lehnert, T.; Heider, D.; Leicht, H.; Heinrich, S.; Corrieri, S.; Luppa, M.; Riedel-Heller, S.; König, H.-H. Health care utilization and costs of elderly persons with multiple chronic conditions. Med. Care Res. Rev. 2011, 68, 387–420. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [Green Version]
- National Institutes of Health. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies; 2014. Available online: https://www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovascular-risk-reduction/tools/cohort (accessed on 23 September 2020).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Kristensen, K.; König, H.-H.; Hajek, A. The association of multimorbidity, loneliness, social exclusion and network size: Findings from the population-based German Ageing Survey. BMC Public Health 2019, 19, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Renne, I.; Gobbens, R.J. Effects of frailty and chronic diseases on quality of life in Dutch community-dwelling older adults: A cross-sectional study. Clin. Interv. Aging 2018, 13, 325–334. [Google Scholar] [CrossRef] [Green Version]
- Barlow, M.A.; Liu, S.Y.; Wrosch, C. Chronic illness and loneliness in older adulthood: The role of self-protective control strategies. Health Psychol. 2015, 34, 870–879. [Google Scholar] [CrossRef] [PubMed]
- Jessen, M.A.B.; Pallesen, A.V.J.; Kriegbaum, M.; Kristiansen, M. The association between loneliness and health–a survey-based study among middle-aged and older adults in Denmark. Aging Ment. Health 2018, 22, 1338–1343. [Google Scholar] [CrossRef] [PubMed]
- Olaya, B.; Domènech-Abella, J.; Moneta, M.V.; Lara, E.; Caballero, F.F.; Rico-Uribe, L.A.; Haro, J.M. All-cause mortality and multimorbidity in older adults: The role of social support and loneliness. Exp. Gerontol. 2017, 99, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Wister, A.; Kendig, H.; Mitchell, B.; Fyffe, I.; Loh, V. Multimorbidity, health and aging in Canada and Australia: A tale of two countries. BMC Geriatr. 2016, 16, 163. [Google Scholar] [CrossRef] [Green Version]
- Singer, L.; Green, M.; Rowe, F.; Ben-Shlomo, Y.; Morrissey, K. Social determinants of multimorbidity and multiple functional limitations among the ageing population of England, 2002–2015. SSM Popul. Health 2019, 8, 100413. [Google Scholar] [CrossRef]
- Pinquart, M.; Sörensen, S. Risk factors for loneliness in adulthood and old age—A meta-analysis. Adv. Psychol. Res. 2003, 19, 111–143. [Google Scholar]
- McKinlay, E.; McDonald, J.; Darlow, B.; Perry, M. Social networks of patients with multimorbidity: A qualitative study of patients’ and supporters’ views. J. Prim. Health Care 2017, 9, 153–161. [Google Scholar] [CrossRef] [Green Version]
- Caputo, J.; Simon, R.W. Physical limitation and emotional well-being: Gender and marital status variations. J. Health Soc. Behav. 2013, 54, 241–257. [Google Scholar] [CrossRef] [Green Version]
- Uchino, B. Social Support and Physical Health: Understanding the Health Consequences of Relationships; Yale University Press: New Haven, CT, USA, 2004. [Google Scholar]
- Penninx, B.W.; Van Tilburg, T.; Kriegsman, D.M.; Deeg, D.J.; Boeke, A.J.P.; Van Eijk, J.T.M. Effects of social support and personal coping resources on mortality in older age: The Longitudinal Aging Study Amsterdam. Am. J. Epidemiol. 1997, 146, 510–519. [Google Scholar] [CrossRef]
- Hawkley, L.C.; Cacioppo, J.T. Loneliness matters: A theoretical and empirical review of consequences and mechanisms. Ann. Behav. Med. 2010, 40, 218–227. [Google Scholar] [CrossRef] [Green Version]
- Gierveld, J.D.J.; Tilburg, T.V. A 6-item scale for overall, emotional, and social loneliness: Confirmatory tests on survey data. Res. Aging 2006, 28, 582–598. [Google Scholar] [CrossRef]
- Russell, D.W. UCLA Loneliness Scale (Version 3): Reliability, validity, and factor structure. J. Personal. Assess. 1996, 66, 20–40. [Google Scholar] [CrossRef] [PubMed]
- Penning, M.J.; Liu, G.; Chou, P.H.B. Measuring loneliness among middle-aged and older adults: The UCLA and de Jong Gierveld Loneliness Scales. Soc. Indic. Res. 2014, 118, 1147–1166. [Google Scholar] [CrossRef]
- Brüderl, J.; Ludwig, V. Fixed-effects panel regression. In The Sage Handbook of Regression Analysis and Causal Inference; Wolf, C., Ed.; SAGE: Los Angeles, CA, USA, 2015; pp. 327–357. [Google Scholar]
- Chatters, L.M.; Taylor, H.O.; Nicklett, E.J.; Taylor, R.J. Correlates of Objective Social Isolation from Family and Friends among Older Adults. Healthcare. 2018, 6, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moral-Benito, E.; Allison, P.; Williams, R. Dynamic panel data modelling using maximum likelihood: An alternative to Arellano-Bond. Appl. Econ. 2019, 51, 2221–2232. [Google Scholar] [CrossRef] [Green Version]
- Clarke, L.H.; Bennett, E. ‘You learn to live with all the things that are wrong with you’: Gender and the experience of multiple chronic conditions in later life. Ageing Soc. 2013, 33, 342–360. [Google Scholar] [CrossRef] [Green Version]
- Friis, K.; Lasgaard, M.; Pedersen, M.H.; Duncan, P.; Maindal, H.T. Health literacy, multimorbidity, and patient-perceived treatment burden in individuals with cardiovascular disease. A Danish population-based study. Patient Educ. Couns. 2019, 102, 1932–1938. [Google Scholar] [CrossRef]
- Aaby, A.; Beauchamp, A.; O’Hara, J.; Maindal, H.T. Large diversity in Danish health literacy profiles: Perspectives for care of long-term illness and multimorbidity. Eur. J. Public Health 2020, 30, 75–80. [Google Scholar] [CrossRef]
- Hajek, A.; König, H.-H. Flexible goal adjustment moderates the link between self-rated health and subjective well-being. Findings from the general population. Aging Ment. Health 2020, 1–6. [Google Scholar] [CrossRef]
- Hajek, A.; König, H.H. The moderating role of flexible goal adjustment in the link between pain and depressive symptoms: Findings based on a nationally representative sample of older adults. Psychogeriatrics 2020, 20, 602–607. [Google Scholar] [CrossRef]
- Prados-Torres, A.; Calderón-Larranaga, A.; Hancco-Saavedra, J.; Poblador-Plou, B.; van den Akker, M. Multimorbidity patterns: A systematic review. J. Clin. Epidemiol. 2014, 67, 254–266. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow chart.


{kind=link}
Table 1.
Search strategy (PubMed).
| # | Search Term |
|---|---|
| #1 | Loneliness |
| #2 | Social exclusion |
| #3 | Social frailty |
| #4 | Social isolation |
| #5 | #1 OR #2 OR #3 OR #4 |
| #6 | Multimorbidity |
| #7 | multiple chronic |
| #8 | disease * |
| #9 | condition * |
| #10 | illness * |
| #11 | #7 AND (#8 OR #9 OR #10) |
| #12 | #6 OR #11 |
| #13 | #5 AND #12 |
Notes: Please note that the asterisk (“*”: in “disease*” (#8)) in PubMed is a truncation symbol. It can be used at the end of a word to search for all terms that begin with that basic root.
Table 2.
Extracted data.
| Study | Study Type/Time Span | Sample Source/Size | Age | Loneliness Assessment | Multimorbidity Assessment | Main Results | Quality Assessment Score |
|---|---|---|---|---|---|---|---|
| Barlow, M et al. (2014) | Longitudinal Five waves, from 2004 to 2012) | Montreal Aging and Health Study (Canada) N = 121 (56.2% females) | M = 71.2 SD = 4.7 64–83 | Two items | Number of chronic illnesses (from a list of 17 diseases) | Growth-curve models showed that chronic illness was positively associated with loneliness (yearly change: ß = 0.125, p < 0.05). | Fair |
| Jessen, M et al. (2018) | Cross-sectional | National Longitudinal Survey of Ageing (Denmark) N = 9154 (54.3% females) | Not reported | UCLA Loneliness scale (20 items) | Two or more chronic conditions (from a list of eight diseases) | Logistic regression revealed that loneliness was positively associated with multimorbidity (OR = 1.77, 95% CI: 1.20–3.35). | Good |
| Kristensen, K. et al. (2019a) | Longitudinal Four waves, from 2002 to 2014 | German Aging Survey (Germany) N = 12,692 (48.9% females) | M = 63.5 SD = 11.4 | De Jong Gierveld short scales for loneliness (six items) | Two or more illnesses (from a list of 13 diseases) | Fixed effects regression stated that multimorbidity was associated with increased levels of loneliness (ß = 0.06, p < 0.001). | Good |
| Kristensen, K. et al. (2019b) | Cross-sectional | German Aging Survey (Germany) N = 7604 (53.6% females) | M = 59.8 SD = 10.6 | De Jong Gierveld short scales for loneliness (six items) | Two or more illnesses (from a list of 13 diseases) | Linear regression detected a positive association between multimorbidity and loneliness (ß = 0.08, p < 0.001). | Good |
| Olaya, B. et al. (2017) | Longitudinal Two waves, from 2011/12 to 2014/15 | Edad con Salud (Spain) N = 2113 (55.2% females) | M = 71.8 95% CI: 71.4–72.1 | UCLA Loneliness scale (three items) | Number of chronic conditions (from a list of eight diseases) | Cox Proportional Hazard models did not find an association between multimorbidity on the one side and high loneliness (ref.: low loneliness) (ß = 0.003, p = 0.991) or high social support (ref.: low social support) (ß = 0.69, p = 0.262) on the other side. | Good |
| Renne, I & Gobbens, R. (2018) | Recruited from a general practice (The Netherlands) N = 241 (48.9% females) | M = 76.5 SD = 5.1 70–90 | Assessment of social domain of frailty (TFI (three items)) | Number of chronic conditions (from a list of nine diseases) | Linear regression showed that multimorbidity was negatively associated with quality of life (ß = -3.786, p < 0.001). | Fair | |
| Singer, L. et al. (2019) | Longitudinal Seven waves from 2002 to 2014 | English Longitudinal Study of Ageing (United Kingdom) N = 15,046 (55.3% females) | M = 66.0 SD = 10.9 | One item | Basic multimorbidity: two or more morbidities (from a list of 25 diseases) Complex multimorbidity: three or more body systems affected | Generalized Estimating Equations revealed that multimorbidity was positively associated with low household wealth (ref.: high) (OR = 1.47, 95% CI: 1.34–1.61), a low subjective social status (ref.: high) (OR = 1.14, 95% CI: 1.04–1.24), a semi/routine occupation (ref.: manager, professional) (OR = 1.07, 95% CI: 1.04–1.24), a low sense of control (ref.: high) (OR = 1.57, 95% CI: 1.41–1.74), having no friends (ref.: very/some supportive friends) (OR = 1.14, 95% CI: 1.02–1.26), having no partner (ref. very/some supportive partner) (OR = 1.15, 95% CI: 1.06–1.26) and loneliness (OR = 1.19, 95% CI: 1.11–1.28). | Fair |
| Wister, A. et al. (2016) | Cross-sectional | Canadian Community Health Survey (Canada) and Household, Income and Labor Dynamics in Australia (Australia) N = 36,397 (51.9% females) | 45–54: 38.1% 55–64: 29.7% 65–74: 17.9% ≥75: 14.3% | Hughes et al. 3-item loneliness scale | Number of chronic illnesses (from a list of eight diseases) | OLS regression showed that there was a significant positive association between multimorbidity and loneliness for all combinations of age group, gender and country, except Australian men which were older than 75 (ß = 0.02, 95% CI: −0.14–0.17). | Good |
Notes: M = mean; SD = standard deviation; OR = odds ratio; OLS = ordinary least squares; TFI = Tilburg Frailty Indicator; UCLA = University of California, Los Angeles; Barlow et al. (2014): adjusted for age, female, socio-economic status and partnership status, and health engagement strategies as well as health-related self-protection; Jessen et al. (2018): adjusted for sex, year of birth, marital status, cohabitation status, attachment to the labor market, and home ownership; Kristensen et al. (2019a): adjusted for age, BMI, depressive symptoms, monthly net equivalent income, physical activity, self-rated health, marital status, and employment status; Kristensen et al. (2019b): adjusted for sex, age, marital status, monthly net equivalent income, BMI, depressive symptoms, current smoking status, alcohol consumption and physical activity; Olaya et al. (2017): adjusted for social support, loneliness, smoking, age, years of education, marital status, alcohol consumption, and depression; Renne & Gobbens (2018): adjusted for sex, age, marital status, education, and 15 frailty components from the Tilburg Frailty Indicator; Singer et al. (2019): adjusted for participation, sense of control, supportive children, supportive friends, and supportive partner; Wister et al. (2016): adjusted for marital status, foreign-born status, and education level.
Table 3.
Quality assessment.
| Questions | Studies | |||||||
|---|---|---|---|---|---|---|---|---|
| Barlow (2014) | Jessen (2018) | Kristensen (2019a) | Kristensen (2019b) | Olaya (2017) | Renne (2018) | Singer (2019) | Wister (2016) | |
| 1. Was the research question or objective in this paper clearly stated? | yes | yes | yes | yes | yes | yes | yes | yes |
| 2. Was the study population clearly specified and defined? | yes | yes | yes | yes | yes | yes | yes | yes |
| 3. Was the participation rate of eligible persons at least 50%? | not reported | yes (73.5%) | no (27.1%–50.3%) | no (27.1%) | yes (69.9%) | no (47.5%) | not reported | not reported |
| 4. Were all the subjects selected or recruited from the same or similar populations (including the same time period)? Were inclusion and exclusion criteria for being in the study prespecified and applied uniformly to all participants? | yes | yes | yes | yes | yes | yes | yes | yes |
| 5. Was a sample size justification, power description, or variance and effect estimates provided? | no | no | no | no | no | no | no | no |
| 6. For the analyses in this paper, were the exposure(s) of interest measured prior to the outcome(s) being measured? (if not prospective should be answered as ‘no’, even is exposure predated outcome) | yes | no (cross-sectional) | no (simultaneously) | no (cross-sectional) | no (simultaneously) | no (cross-sectional) | no (simultaneously) | no (cross-sectional) |
| 7. Was the timeframe sufficient so that one could reasonably expect to see an association between exposure and outcome if it existed? | yes | no (cross-sectional) | yes | no (cross-sectional) | no | no (cross-sectional) | yes | no (cross-sectional) |
| 8. For exposures that can vary in amount or level, did the study examine different levels of the exposure as related to the outcome (e.g., categories of exposure, or exposure measured as continuous variable)? | dichotomous and continuous | dichotomous | dichotomous | dichotomous | dichotomous | continuous | dichotomous | continuous |
| 9. Were the exposure measures (independent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? | yes | yes | yes | yes | yes | yes | yes | yes |
| 10. Was the exposure(s) assessed more than once over time? | no | no | yes | no | no | no | yes | no |
| 11. Were the outcome measures (dependent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? | yes | yes | yes | yes | yes | yes | yes | yes |
| 12. Was loss to follow-up after baseline 20% or less? | yes | not applicable | no | not applicable | not reported | not applicable | not reported | not applicable |
| 13. Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)? | yes | yes | yes | yes | yes | yes | yes | yes |
| Overall quality judgement | fair | good | good | good | good | fair | fair | good |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Hajek, A.; Kretzler, B.; König, H.-H. Multimorbidity, Loneliness, and Social Isolation. A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 8688. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228688
AMA Style
Hajek A, Kretzler B, König H-H. Multimorbidity, Loneliness, and Social Isolation. A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(22):8688. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228688
Chicago/Turabian StyleHajek, André, Benedikt Kretzler, and Hans-Helmut König. 2020. "Multimorbidity, Loneliness, and Social Isolation. A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 22: 8688. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228688
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.