Follow-Up of Elevated Blood Lead Levels and Sources in a Cohort of Children in Benin

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Exposure and Relevant Data Collection
2.3. Blood Sampling and Analysis
2.4. Statistical Analysis
3. Results
3.1. Population
3.2. Comparison between Children Included in the Analyses and Children Excluded
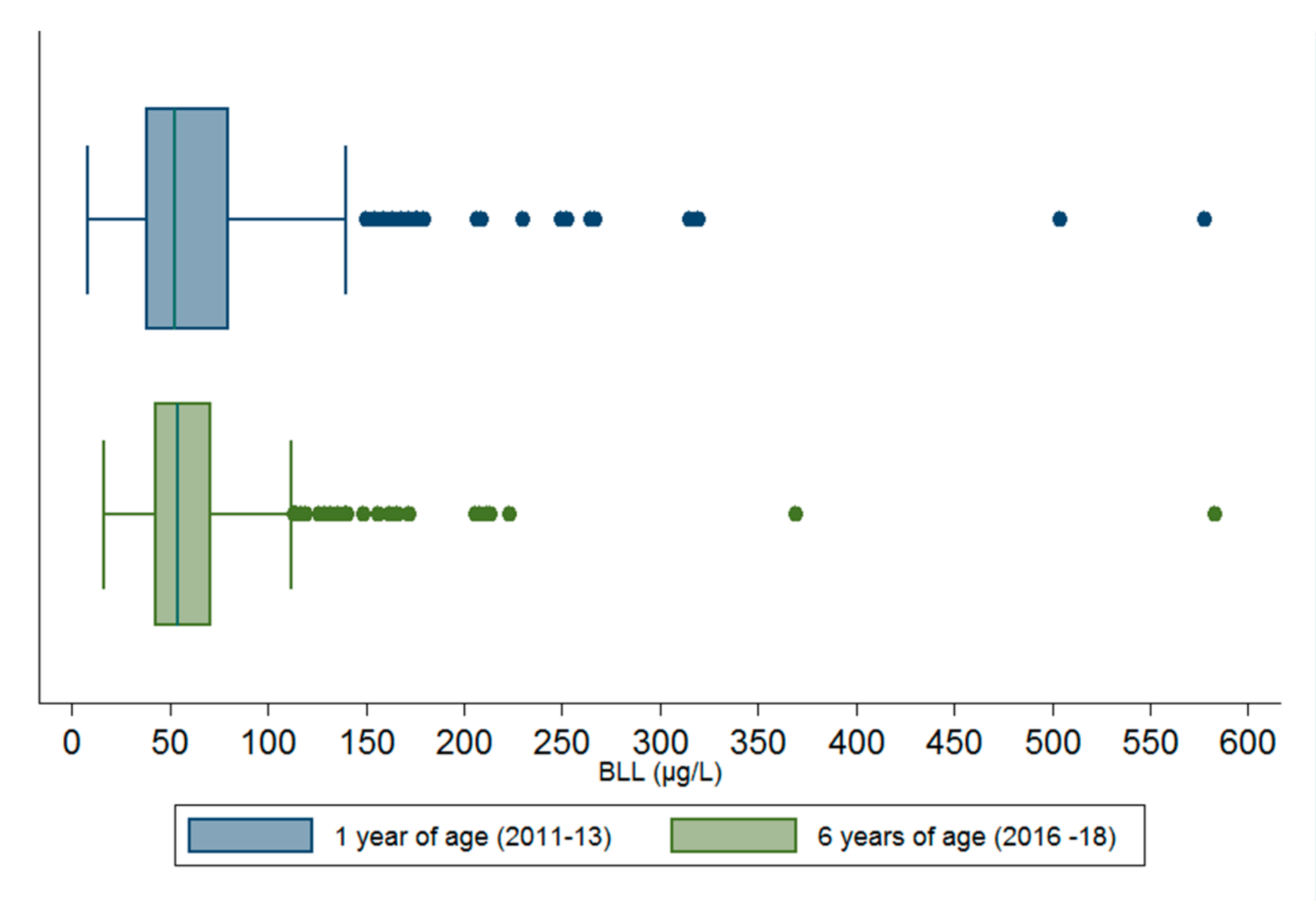
3.3. Comparison of BLLs at Age 1 and 6 Years
3.4. Comparison of Potential Sources of Lead at Two Age Points
3.5. Associations between Sources of Lead and BLLs at Age 6 Years
3.6. Associations between Sources of Lead and Sociodemographic Factors
4. Discussion
4.1. BLLs and Sources of Lead at Age 1 and 6 Years
4.2. Association between Sociodemographic Characteristics and Sources of Lead
4.3. Dietary Sources of Lead
4.3.1. Bushmeat Harvested with Lead Ammunition
4.3.2. Lead in other Food Types
4.4. Non-Dietary Sources
Activities with Lead
4.5. Strengths and Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bellinger, D.C. Very low lead exposures and children’s neurodevelopment. Curr. Opin. Pediatr. 2008, 20, 172–177. [Google Scholar] [CrossRef]
- Chen, A.; Cai, B.; Dietrich, K.N.; Radcliffe, J.; Rogan, W.J. Lead exposure, IQ, and behavior in urban 5- to 7-year-olds: Does lead affect behavior only by lowering IQ? Pediatrics 2007, 119, e650–e658. [Google Scholar] [CrossRef] [Green Version]
- Obeng-Gyasi, E. Lead Exposure and Oxidative Stress—A Life Course Approach in U.S. Adults. Toxics 2018, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.J.L.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I.; et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Blood Lead Levels in Children. Available online: https://www.cdc.gov/nceh/lead/prevention/blood-lead-levels.htm (accessed on 18 November 2019).
- Centers for Disease Control and Prevention—Advisory Committee on Childhood Lead Poisoning Prevention. Low Level Lead Exposure Harms Children: A Renewed Call for Primary Prevention. 4 January 2012. Available online: https://www.cdc.gov/nceh/lead/acclpp/Final_Document_030712.pdf (accessed on 25 September 2020).
- Chiodo, L.M.; Jacobson, S.W.; Jacobson, J.L. Neurodevelopmental effects of postnatal lead exposure at very low levels. Neurotoxicol. Teratol. 2004, 26, 359–371. [Google Scholar] [CrossRef]
- Lanphear, B. Cognitive deficits associated with blood lead concentrations <10 microg/dL in US children and adolescents. Public Health Rep. 2000, 115, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.; Benford, D.; Boobis, A.; Ceccatelli, S.; Cravedi, J.P.; Di Domenico, A. Scientific Opinion on Lead in Food EFSA Panel on Contaminants in the Food Chain (CONTAM). Efsa J. 2010, 8, 93. [Google Scholar]
- Dignam, T.; Kaufmann, R.B.; LeStourgeon, L.; Brown, M.J. Control of Lead Sources in the United States, 1970–2017: Public Health Progress and Current Challenges to Eliminating Lead Exposure. J. Public Health Manag. Pract. 2019, 25 (Suppl. S1), S13–S22. [Google Scholar] [CrossRef] [PubMed]
- Muntner, P.; Menke, A.; DeSalvo, K.B.; Rabito, F.A.; Batuman, V. Continued decline in blood lead levels among adults in the United States: The National Health and Nutrition Examination Surveys. Arch. Intern. Med. 2005, 165, 2155–2161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsoi, M.-F.; Cheung, C.-L.; Cheung, T.T.; Cheung, B.M.Y. Continual Decrease in Blood Lead Level in Americans: United States National Health Nutrition and Examination Survey 1999–2014. Am. J. Med. 2016, 129, 1213–1218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EFSA Panel on Contaminants in the Food Chain (CONTAM); Scientific Opinion on Lead in Food. EFSA J. 2010, 8, 1570. [CrossRef]
- Todd, H.D. Outcome and Influence Evaluation of the UNEP Partnership for Clean Fuels and Vehicles (PCFV); United Nations Environment Programme: Nairobi, Kenya, 2010. [Google Scholar]
- Mathee, A.; Röllin, H.; Von Schirnding, Y.; Levin, J.; Naik, I. Reductions in blood lead levels among school children following the introduction of unleaded petrol in South Africa. Environ. Res. 2006, 100, 319–322. [Google Scholar] [CrossRef] [PubMed]
- Tuakuila, J.; Kabamba, M.; Mata, H.; Mata, G. Blood lead levels in children after phase-out of leaded gasoline in Kinshasa, the capital of Democratic Republic of Congo (DRC). Arch. Public Health 2013, 71, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathee, A. Towards the prevention of lead exposure in South Africa: Contemporary and emerging challenges. Neurotoxicology 2014, 45, 220–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UNEP/IPEN. Lead in Enamel Decorative Paints National Paint Testing Results: A Nine Country Study; United Nations Environment Program: Nairobi, Kenya, 2013. [Google Scholar]
- Njati, S.Y.; Maguta, M.M. Lead-based paints and children’s PVC toys are potential sources of domestic lead poisoning—A review. Environ. Pollut. 2019, 249, 1091–1105. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, D.; Hou, D.; Ye, J.; Zhang, Y.; Ok, Y.S.; Song, Y.; Coulon, F.; Peng, T.; Tian, L. Lead-based paint remains a major public health concern: A critical review of global production, trade, use, exposure, health risk, and implications. Environ. Int. 2018, 121, 85–101. [Google Scholar] [CrossRef]
- Obeng-Gyasi, E. Sources of lead exposure in various countries. Rev. Environ. Health 2019, 34, 25–34. [Google Scholar] [CrossRef]
- Landrigan, P.J.; Fuller, R. Pollution, health and development: The need for a new paradigm. Rev. Environ. Health 2016, 31, 121–124. [Google Scholar] [CrossRef]
- Kordas, K.; Ravenscroft, J.; Cao, Y.; McLean, E.V. Lead Exposure in Low and Middle-Income Countries: Perspectives and Lessons on Patterns, Injustices, Economics, and Politics. Int. J. Environ. Res. Public Health 2018, 15, 2351. [Google Scholar] [CrossRef] [Green Version]
- Graber, L.K.; Asher, D.; Anandaraja, N.; Bopp, R.F.; Merrill, K.; Cullen, M.R.; Luboga, S.; Trasande, L. Childhood lead exposure after the phaseout of leaded gasoline: An ecological study of school-age children in Kampala, Uganda. Environ. Health Perspect 2010, 118, 884–889. [Google Scholar] [CrossRef]
- Olewe, T.; Mwanthi, M.; Wang, J.; Griffiths, J. Blood lead levels and potental environmental exposures among children under five years in Kibera slums, Nairobi. East Afr. J. Public Health 2009, 6, 6–10. [Google Scholar] [CrossRef]
- Bodeau-Livinec, F.; Glorennec, P.; Cot, M.; Dumas, P.; Durand, S.; Massougbodji, A.; Ayotte, P.; Le Bot, B. Elevated Blood Lead Levels in Infants and Mothers in Benin and Potential Sources of Exposure. Int. J. Environ. Res. Public Health 2016, 13, 316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fachehoun, R.C.; Lévesque, B.; Dumas, P.; St-Louis, A.; Dubé, M.; Ayotte, P. Lead exposure through consumption of big game meat in Quebec, Canada: Risk assessment and perception. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess 2015, 32, 1501–1511. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, S.; Blumenthal, W.; Kennedy, C.; Yip, F.Y.; Pickard, S.; Flanders, W.D.; Loringer, K.; Kruger, K.; Caldwell, K.L.; Brown, M.J. Hunting with lead: Association between blood lead levels and wild game consumption. Environ. Res. 2009, 109, 952–959. [Google Scholar] [CrossRef]
- Bonwitt, J.; Dawson, M.; Kandeh, M.; Ansumana, R.; Sahr, F.; Brown, H.; Kelly, A.H. Unintended consequences of the ‘bushmeat ban’ in West Africa during the 2013–2016 Ebola virus disease epidemic. Soc. Sci. Med. 2018, 200, 166–173. [Google Scholar] [CrossRef]
- González, R.; Mombo-Ngoma, G.; Ouedraogo, S.; Kakolwa, M.A.; Abdulla, S.; Accrombessi, M.; Aponte, J.J.; Akerey-Diop, D.; Basra, A.; Briand, V.; et al. Intermittent preventive treatment of malaria in pregnancy with mefloquine in HIV-negative women: A multicentre randomized controlled trial. PLoS Med. 2014, 11, e1001733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etchevers, A.; Bretin, P.; Lecoffre, C.; Bidondo, M.-L.; Le Strat, Y.; Glorennec, P.; Le Tertre, A. Blood lead levels and risk factors in young children in France 2008–2009. Int. J. Hyg. Environ. Health 2014, 217, 528–537. [Google Scholar] [CrossRef]
- Guy, M.; Accrombessi, M.; Fievet, N.; Yovo, E.; Massougbodji, A.; Le Bot, B.; Glorennec, P.; Bodeau-Livinec, F.; Briand, V. Toxics (Pb, Cd) and trace elements (Zn, Cu, Mn) in women during pregnancy and at delivery, South Benin 2014–2015. Environ. Res. 2018, 167, 198–206. [Google Scholar] [CrossRef]
- Koenker, R.; Bassett, G. Regression Quantiles. Econometrica 1978, 46, 33–50. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software: Release 14; StataCorp LP: College Station, TX, USA, 2015. [Google Scholar]
- Monebenimp, F.; Kuepouo, G.; Chelo, D.; Anatole, P.C.; Bissek, A.-C.Z.K.; Gottesfeld, P. Blood Lead Levels among Children in Yaounde Cameroon. Front Public Health 2017, 5, 163. [Google Scholar] [CrossRef] [Green Version]
- Naicker, N.; Mathee, A.; Barnes, B. A follow-up cross-sectional study of environmental lead exposure in early childhood in urban South Africa. S. Afr. Med. J. 2013, 103, 935–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bello, O.; Naidu, R.; Rahman, M.M.; Liu, Y.; Dong, Z. Lead concentration in the blood of the general population living near a lead-zinc mine site, Nigeria: Exposure pathways. Sci. Total Environ. 2016, 542, 908–914. [Google Scholar] [CrossRef] [PubMed]
- Committee on Measuring Lead in Critical Populations—National Research Council. Measuring Lead Exposure in Infants, Children, and Other Sensitive Populations; National Academies Press: Washington, DC, USA, 1993. [Google Scholar]
- Ahmadi, S.; Bodeau-Livinec, F.; Zoumenou, R.; Garcia, A.; Courtin, D.; Alao, J.; Fievet, N.; Cot, M.; Massougbodji, A.; Botton, J. Comparison of growth models to describe growth from birth to 6 years in a Beninese cohort of children with repeated measurements. BMJ Open 2020, 10, 9. [Google Scholar]
- Caravanos, J.; Carrelli, J.; Dowling, R.; Pavilonis, B.; Ericson, B.; Fuller, R. Burden of disease resulting from lead exposure at toxic waste sites in Argentina, Mexico and Uruguay. Environ. Health 2016, 15, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahaffey, K.R.; Annest, J.L.; Roberts, J.; Murphy, R.S. National estimates of blood lead levels: United States, 1976–1980: Association with selected demographic and socioeconomic factors. N. Engl. J. Med. 1982, 307, 573–579. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention—Advisory Committee on Childhood Lead Poisoning Prevention. Interpreting and Managing Blood Lead Levels <10 µg/dL in Children and Reducing Childhood Exposures to Lead: Recommendations of CDC’s Advisory Committee on Childhood Lead Poisoning Prevention; Morbidity and Mortality Weekly Report: Recommendations and Reports; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2007. [Google Scholar]
- Canfield, R.L.; Henderson, C.R.; Cory-Slechta, D.A.; Cox, C.; Jusko, T.A.; Lanphear, B.P. Intellectual impairment in children with blood lead concentrations below 10 microg per deciliter. N. Engl. J. Med. 2003, 348, 1517–1526. [Google Scholar] [CrossRef] [Green Version]
- Jusko, T.A.; Henderson, C.R.; Lanphear, B.P.; Cory-Slechta, D.A.; Parsons, P.J.; Canfield, R.L. Blood lead concentrations <10 microg/dL and child intelligence at 6 years of age. Environ. Health Perspect 2008, 116, 243–248. [Google Scholar]
- Lanphear, B.P.; Hornung, R.; Khoury, J.; Yolton, K.; Baghurst, P.; Bellinger, D.C.; Canfield, R.L.; Dietrich, K.N.; Bornschein, R.; Greene, T.; et al. Low-level environmental lead exposure and children’s intellectual function: An international pooled analysis. Environ. Health Perspect 2005, 113, 894–899. [Google Scholar] [CrossRef]
- Green, R.E.; Pain, D.J. Risks to human health from ammunition-derived lead in Europe. Ambio 2019, 48, 954–968. [Google Scholar] [CrossRef] [Green Version]
- Pain, D.J.; Cromie, R.L.; Newth, J.; Brown, M.J.; Crutcher, E.; Hardman, P.; Hurst, L.; Mateo, R.; Meharg, A.A.; Moran, A.C.; et al. Potential hazard to human health from exposure to fragments of lead bullets and shot in the tissues of game animals. PLoS ONE 2010, 5, e10315. [Google Scholar] [CrossRef] [Green Version]
- Mateo, R.; La Cruz, M.R.-D.; Vidal, D.; Reglero, M.; Camarero, P.; Vidal, D. Transfer of lead from shot pellets to game meat during cooking. Sci. Total Environ. 2007, 372, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Buenz, E.J.; Parry, G.J. Chronic Lead Intoxication From Eating Wild-Harvested Game. Am. J. Med. 2018, 131, e181–e184. [Google Scholar] [CrossRef]
- Lindboe, M.; Henrichsen, E.; Høgåsen, H.; Bernhoft, A. Lead concentration in meat from lead-killed moose and predicted human exposure using Monte Carlo simulation. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess 2012, 29, 1052–1057. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, S.; Maman, S.; Zoumenou, R.; Massougbodji, A.; Cot, M.; Glorennec, P.; Bodeau-Livinec, F. Hunting, Sale, and Consumption of Bushmeat Killed by Lead-Based Ammunition in Benin. Int. J. Environ. Res. Public Health 2018, 15, 1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dindé, A.O.; Mobio, A.J.; Konan, A.G.; Fokou, G.; Yao, K.; Esso, E.L.J.C.; Fantodji, A.; Koussemon, M.; Bonfoh, B. Response to the Ebola-related bushmeat consumption ban in rural Côte d’Ivoire. Agric. Food Secur. 2017, 6, 24. [Google Scholar] [CrossRef] [Green Version]
- Ordaz-Németh, I.; Arandjelovic, M.; Boesch, L.; Gatiso, T.; Grimes, T.; Kuehl, H.S.; Lormie, M.; Stephens, C.; Tweh, C.; Junker, J. The socio-economic drivers of bushmeat consumption during the West African Ebola crisis. PLoS Negl. Trop. Dis. 2017, 11, e0005450. [Google Scholar] [CrossRef]
- Buka, I.; Hervouet-Zeiber, C. Lead Toxicity with a New Focus: Addressing low-Level Lead Exposure in Canadian Children. 29 November 2019. Available online: https://www.cps.ca/en/documents/position/lead-toxicity (accessed on 29 November 2019).
- Rehman, Z.U.; Khan, S.; Brusseau, M.L.; Shah, M.T. Lead and cadmium contamination and exposure risk assessment via consumption of vegetables grown in agricultural soils of five-selected regions of Pakistan. Chemosphere 2017, 168, 1589–1596. [Google Scholar] [CrossRef] [Green Version]
- Mahmood, A.; Malik, R.N. Human health risk assessment of heavy metals via consumption of contaminated vegetables collected from different irrigation sources in Lahore, Pakistan. Arab. J. Chem. 2014, 7, 91–99. [Google Scholar] [CrossRef] [Green Version]
- Zeng, F.; Wei, W.; Li, M.; Huang, R.; Yang, F.; Duan, Y. Heavy Metal Contamination in Rice-Producing Soils of Hunan Province, China and Potential Health Risks. Int. J. Environ. Res. Public Health 2015, 12, 15584–15593. [Google Scholar] [CrossRef]
- Jitaru, P.; Ingenbleek, L.; Marchond, N.; Laurent, C.; Adegboye, A.; Hossou, S.E.; Koné, A.Z.; Oyedele, A.D.; Kisito, C.S.K.; Dembélé, Y.K.; et al. Occurrence of 30 trace elements in foods from a multi-centre Sub-Saharan Africa Total Diet Study: Focus on Al, As, Cd, Hg, and Pb. Environ. Int. 2019, 133, 105197. [Google Scholar] [CrossRef]
- Ihedioha, J.N.; Ogili, E.O.; Ekere, N.R.; Ezeofor, C.C. Risk assessment of heavy metal contamination of paddy soil and rice (Oryza sativa) from Abakaliki, Nigeria. Environ. Monit. Assess 2019, 191, 350. [Google Scholar] [CrossRef] [PubMed]
- Tirima, S.; Bartrem, C.; Von Lindern, I.; Von Braun, M.C.; Lind, D.; Anka, S.M.; Abdullahi, A. Food contamination as a pathway for lead exposure in children during the 2010–2013 lead poisoning epidemic in Zamfara, Nigeria. J. Environ. Sci. (China) 2018, 67, 260–272. [Google Scholar] [CrossRef] [PubMed]
- Adela, Y.; Ambelu, A.; A Tessema, D. Occupational lead exposure among automotive garage workers—A case study for Jimma town, Ethiopia. J. Occup. Med. Toxicol. 2012, 7, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathee, A.; De Jager, P.; Naidoo, S.; Naicker, N. Exposure to lead in South African shooting ranges. Environ. Res. 2017, 153, 93–98. [Google Scholar] [CrossRef]
- Ma, C.; Iwai-Shimada, M.; Tatsuta, N.; Nakai, K.; Isobe, T.; Takagi, M.; Nishihama, Y.; Nakayama, S.F. Health Risk Assessment and Source Apportionment of Mercury, Lead, Cadmium, Selenium, and Manganese in Japanese Women: An Adjunct Study to the Japan Environment and Children’s Study. Int. J. Environ. Res. Public Health 2020, 17, 2231. [Google Scholar] [CrossRef] [Green Version]
- Fatmi, Z.; Sahito, A.; Ikegami, A.; Mizuno, A.; Cui, X.; Mise, N.; Takagi, M.; Kobayashi, Y.; Kayama, F. Lead Exposure Assessment among Pregnant Women, Newborns, and Children: Case Study from Karachi, Pakistan. Int. J. Environ. Res. Public Health 2017, 14, 413. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | Category | n/Na | % or Mean ± SD |
|---|---|---|---|
| Health centre location | |||
| Attogon/Allada | 150/425 | 35.3 | |
| Sékou | 275/425 | 64.7 | |
| Family characteristics | |||
| Father’s education | |||
| None | 157/417 | 37.7 | |
| Some a | 260/417 | 62.4 | |
| Mothers education | |||
| None | 264/419 | 63.0 | |
| Some a | 155/419 | 37.0 | |
| Language spoken at home | |||
| Fon | 186/421 | 44.2 | |
| Aïzo | 223/421 | 52.9 | |
| Others | 12/421 | 2.9 | |
| Socioeconomic status | |||
| Lowest | 144/421 | 34.2 | |
| Medium | 151/421 | 35.9 | |
| Highest | 126/421 | 29.9 | |
| The child lives in collective housing | |||
| Yes | 328/422 | 77.7 | |
| No | |||
| Parents smoking | |||
| Yes | 17/407 | 4.2 | |
| No | 390/407 | 95.8 | |
| Child characteristics | |||
| Sex | |||
| Boy | 212/425 | 49.9 | |
| Girl | 213/425 | 50.1 | |
| Attending school | |||
| Yes | 281/422 | 66.6 | |
| No | 141/422 | 33.4 | |
| Age at assessment (years) | 425/425 | 6.2 ± 0.3 |
| Potential Sources | Age 1 Year (2011–2013) | Age 6 Years (2016–2018) | Pa |
|---|---|---|---|
| Bushmeat consumption b | 156/379 (41.2) | 135/325 (41.5) | 0.85 |
| Presence of high or moderate risk of paternal occupational exposure | 77/419 (18.4) | 79/724 (18.6) | 0.69 |
| Use of pipe system for drinking water | 308/379 (81.3) | 371/423 (87.7) | <0.01 |
| Presence of paint in the house | 59/423 (14.0) | 56/421 (13.3) | 0.69 |
| Presence of paint chips | 19/379 (5.0) | 23/421 (5.5) | 0.86 |
| Maternal use of eye cosmetics (Khol) | 62/379 (16.4) | 187/421 (44.4) | <0.01 |
| Potential Sources | n (%) | Expected % Difference in BLLs Compared with the Referent Group a | Expected Difference in the Percentiles of BLLs µg/L Compared with the Referent Group | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| (95% CI) a | |||||||||||
| % (95% CI) | p | 25th Percentile | p | 50th Percentile | p | 75th Percentile | p | 90th Percentile | p | ||
| Currently consuming meat killed by lead bullets (vs. no) | 88 (18.8) | 13.3 (1.7, 26.2) | 0.02 | 1.6 (−4.1; 7.2) | 0.6 | 3.8 (−2.6; 10.2) | 0.2 | 13.6 (0.4; 26.9) | 0.04 | 16.3 (−15.9; 48.5) | 0.3 |
| Consumption of rice (vs. less than 1–3 times/months or less) | |||||||||||
| 1–3 times/week | 106 (25.1) | 8.9 (−8.6.3, 29.7) | 0.3 | 2.5 (−6.6; 11.6) | 0.6 | 4.7 (−5.6; 15.0) | 0.4 | 10.1 (−11.3; 31.4) | 0.4 | 3.1 (−49.0; 55,3) | 0.9 |
| 4–6 times/week | 103 (24.4) | 19.6 (0.4, 42.5) | 0.05 | 2.6 (−6.5; 11.7) | 0.6 | 10.2 (−0.2; 20.5) | 0.06 | 18.0 (−3.4; 39.4) | 0.1 | 9.3 (−42.9; 61.6) | 0.7 |
| At least once/day | 179 (42.3) | 17.6 (-0.2, 38.7) | 0.05 | 3.9 (−4.7; 12.5) | 0.4 | 6.2 (−3.2; 16.2) | 0.2 | 13.8 (−6.3; 34.0) | 0.2 | 1.4 (−47.8; 50.5) | 1.0 |
| Consumption of peanuts (referent category: never) | |||||||||||
| <1/month | 137 (32.8) | 3.0 (−6.5, 13.4) | 0.6 | 3.4 (−1.6; 8.4) | 0.2 | 0.7 (−5.0; 6. 4) | 0.8 | 1.7 (−10.1; 13.5) | 0.8 | 3.1 (−25.7; 31.8) | 0.8 |
| >1/month | 41 (9.8) | 22.0 (4.6, 42.5) | 0.01 | 9.2 (1.1; 17.2) | 0.03 | 5.3 (−4.0; 14.0) | 0.3 | 10.0 (−8.9; 28.9) | 0.3 | 73.0 (26.9; 119.1) | <0.01 |
| Consumption of sweet potatoes (referent category: never) | |||||||||||
| <1/month | 204 (48.2) | −7.7 (−16.6, 2.3) | 0.8 | 1.6 (−3.7; 7.0) | 0.6 | −4.7 (−10.7; 1.3) | 0.2 | −8.0 (−20.5; 4.5) | 0.2 | −19.3 (−49.8; 11.3) | 0.2 |
| >1/month | 97 (22.9) | −6.8 (−17.6, 5.4) | 0.8 | −0.9 (−7.3; 5.5) | 0.8 | −4.5 (−11.7; 2.7) | 0.2 | −9.2 (−24.3; 5.9) | 0.2 | −12.1 (−48.8; 24.7) | 0.5 |
| Presence of activity with potential use of lead (vs. absence) | 61 (14.4) | 12.3 (−0.6, 26.8) | 0.06 | 4.4 (−1.9; 10.8) | 0.2 | 3.0 (−4.2; 10.2) | 0.4 | 6.4 (−8.5; 21.3) | 0.4 | 22.6 (−13.8; 58.9) | 0.2 |
| Presence of high or moderate risk of paternal occupational exposure (vs. absence) | 79 (18.6) | 5.8 (−5.2, 18.1) | 0.3 | −1.2 (−6.9; 4.5) | 0.7 | −4.2 (−10.7; 2.2) | 0.2 | 4.7 (−8.7; 18.1) | 0.5 | 29.9 (−2.9; 62.6) | 0.07 |
| Presence of paint in the house (vs. absence) | 56 (13.3) | 4.7 (−7.8, 19.1) | 0.5 | 4.6 (−2.0; 11.3) | 0.2 | −1.2(−8.7, 6.3) | 0.8 | 2.7 (−13.0; 18.4) | 0.7 | 12.5 (−25.7; 50.7) | 0.5 |
| Use of bore hole/cement/dug well for water source (vs. absence) | 188 (44.4) | −4.4 (−3.2, 5.9) | 0.5 | −0.7 (−5.3; 4.0) | 0.8 | −1.1 (−6.4; 4.2) | 0.7 | −2.9 (−13.9; 8.0) | 0.6 | −6.2 (−32.9; 20.5) | 0.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmadi, S.; Le Bot, B.; Zoumenou, R.; Durand, S.; Fiévet, N.; Ayotte, P.; Massougbodji, A.; Alao, M.J.; Cot, M.; Glorennec, P.; et al. Follow-Up of Elevated Blood Lead Levels and Sources in a Cohort of Children in Benin. Int. J. Environ. Res. Public Health 2020, 17, 8689. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228689
Ahmadi S, Le Bot B, Zoumenou R, Durand S, Fiévet N, Ayotte P, Massougbodji A, Alao MJ, Cot M, Glorennec P, et al. Follow-Up of Elevated Blood Lead Levels and Sources in a Cohort of Children in Benin. International Journal of Environmental Research and Public Health. 2020; 17(22):8689. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228689
Chicago/Turabian StyleAhmadi, Shukrullah, Barbara Le Bot, Roméo Zoumenou, Séverine Durand, Nadine Fiévet, Pierre Ayotte, Achille Massougbodji, Maroufou Jules Alao, Michel Cot, Philippe Glorennec, and et al. 2020. "Follow-Up of Elevated Blood Lead Levels and Sources in a Cohort of Children in Benin" International Journal of Environmental Research and Public Health 17, no. 22: 8689. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228689