Comparing Mindful and Non-Mindful Exercises on Alleviating Anxiety Symptoms: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
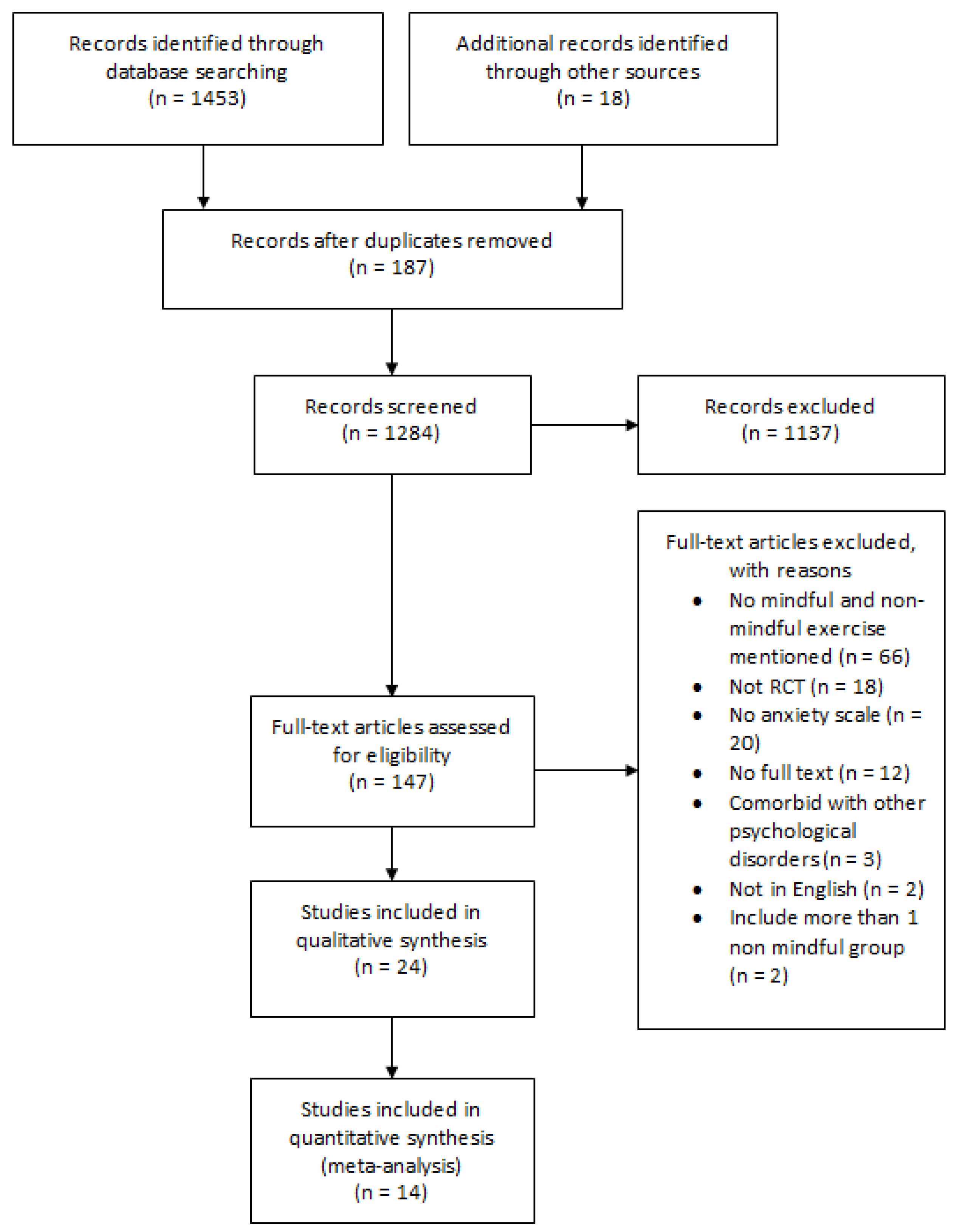
2.3. Study Selection
2.4. Data Extraction
2.5. Data Synthesis
2.6. Quality Assessment of Studies
3. Results
3.1. Search Results
3.2. Quality Assessments
3.3. Characteristics of Included Studies and Participants
3.4. Intervention Characteristics
3.5. Summary of Findings
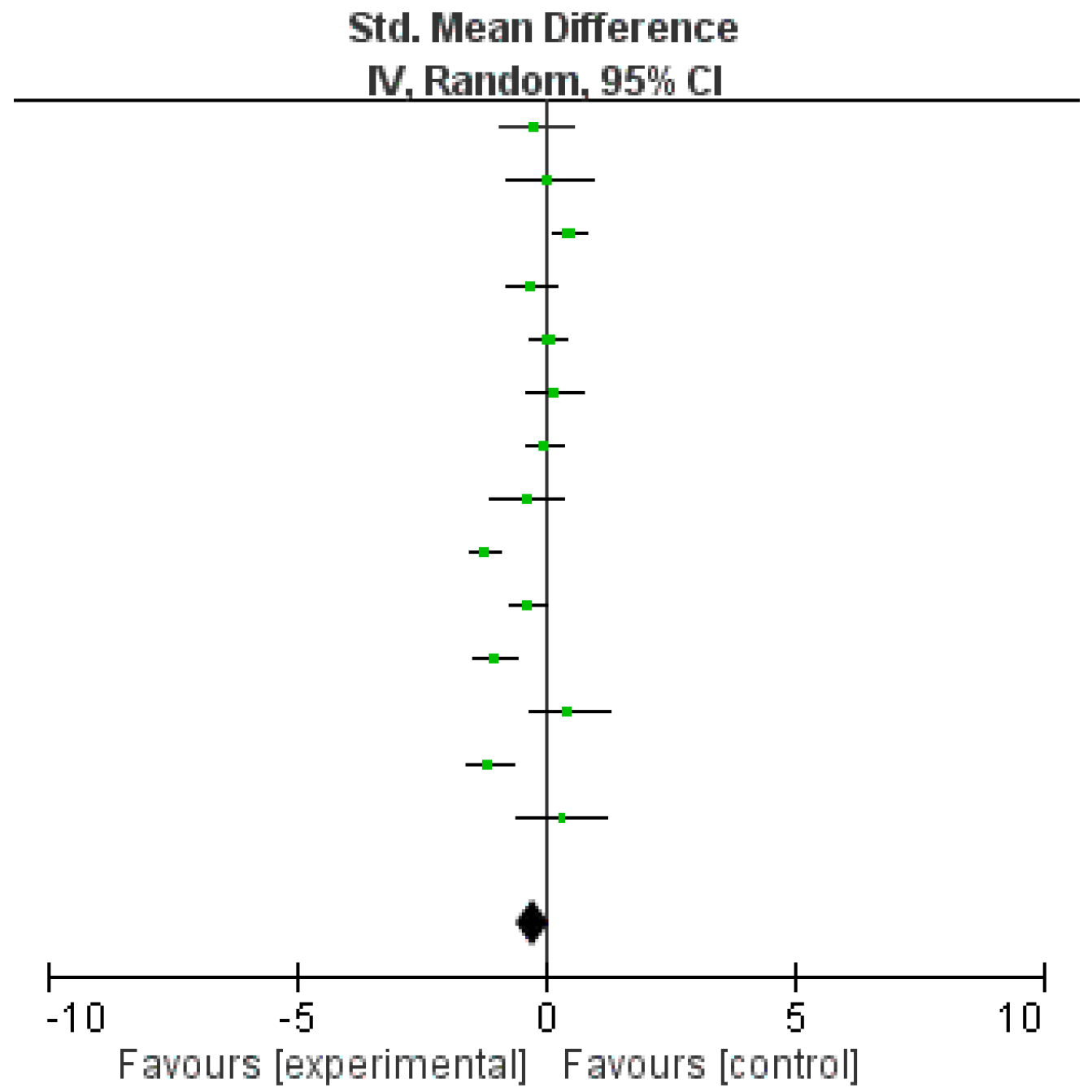
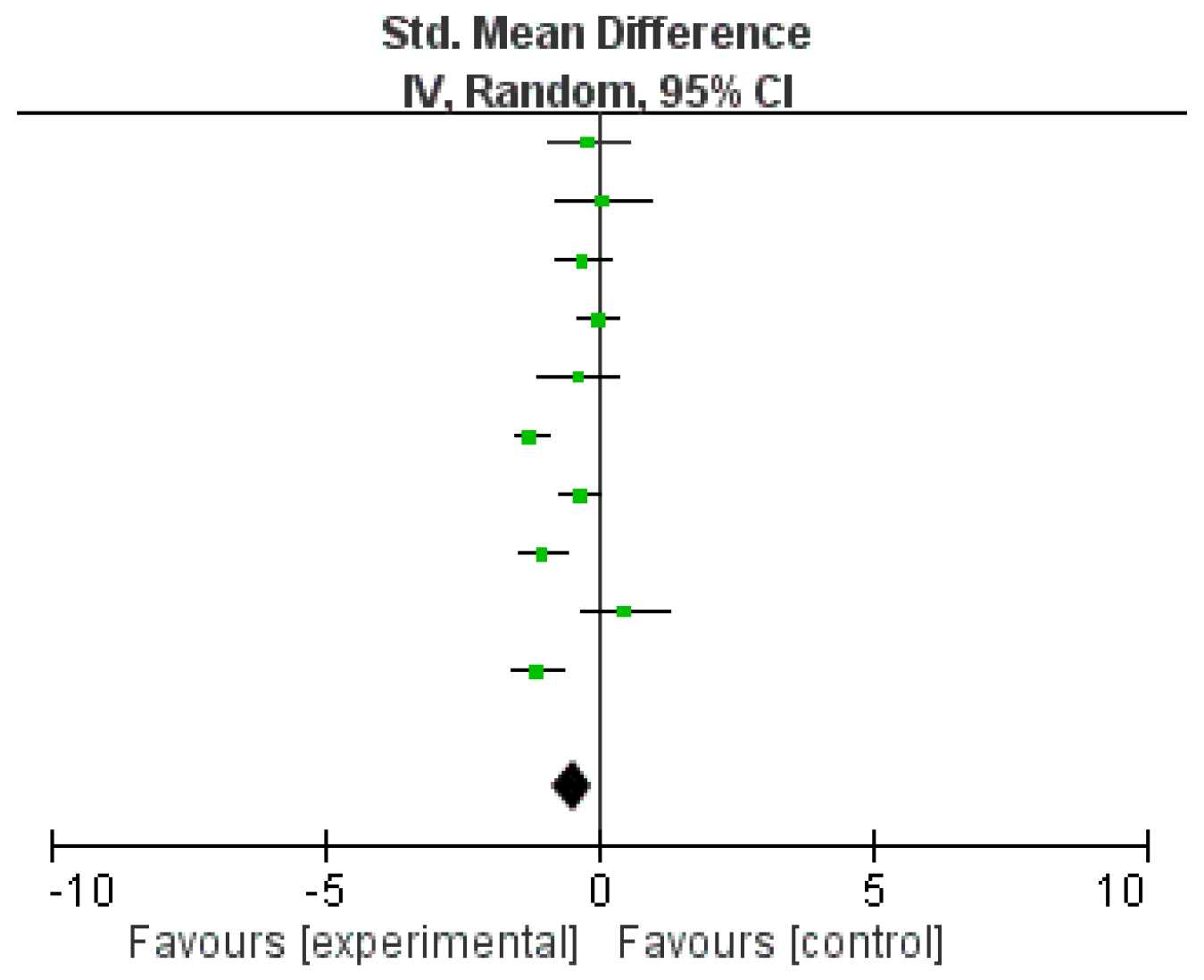
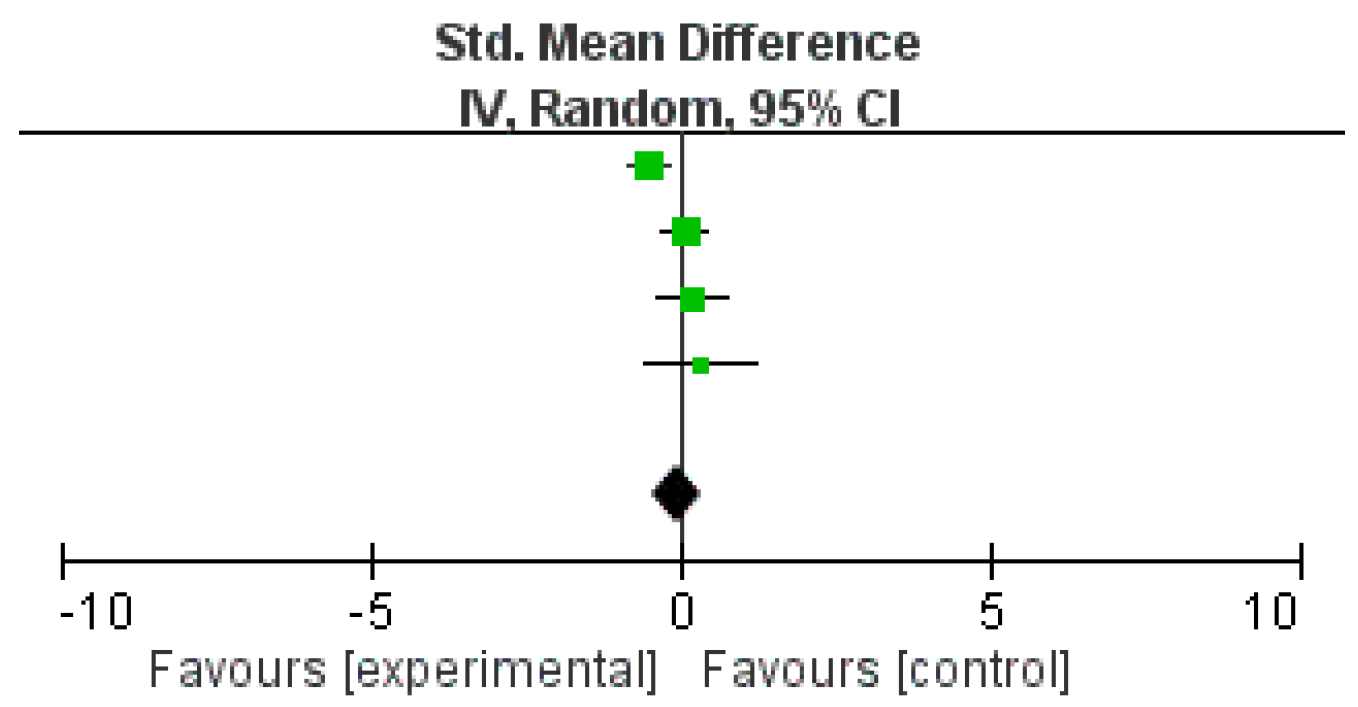
3.6. Effectiveness of Intervention (Meta-Analysis)
4. Discussion
Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychological Assocation. Available online: https://www.apa.org/topics/anxiety/ (accessed on 1 October 2020).
- Gong, M.; Dong, H.; Tang, Y.; Huang, W.; Lu, F. Effects of Aromatherapy on Anxiety: A Meta-analysis of Randomized Controlled Trials. J. Affect. Disord. 2020. [Google Scholar] [CrossRef] [PubMed]
- Stonerock, G.; Hoffman, B.; Smith, P.; Blumenthal, J. Exercise as Treatment for Anxiety: Systematic Review and Analysis. Ann. Behav. Med. 2015, 49, 542–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cramer, H.; Lauche, R.; Anheyer, D.; Pilkington, K.; Manincor, M.; Dobos, G.; Ward, L. Yoga for anxiety: A systematic review and meta-analysis of randomized controlled trials. Depress. Anxiety 2018, 35, 830–843. [Google Scholar] [CrossRef] [PubMed]
- Bandelow, B.; Reitt, M.; Röver, C.; Michaelis, S.; Görlich, Y.; Wedekind, D. Efficacy of treatments for anxiety disorders: A meta-analysis. Int. Clin. Psychopharmacol. 2015, 30, 183–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedman, E.; Mörtberg, E.; Hesser, H.; Clark, D.M.; Lekander, M.; Andersson, E.; Ljótsson, B. Mediators in psychological treatment of social anxiety disorder: Individual cognitive therapy compared to cognitive behavioral group therapy. Behav. Res. Ther. 2013, 51, 696–705. [Google Scholar] [CrossRef] [PubMed]
- Shirifard, R.K.; Avanesyan, H.; Honari, H.; Abadi, S.E.G. Compression of the effect of individual and in group physical exercise on state anxiety in young people. Indian J. Sci. Technol. 2012, 5, 2627–2632. [Google Scholar] [CrossRef]
- Barbour, A.K.; Edenfield, M.T.; Blumenthal, A.J. Exercise as a Treatment for Depression and Other Psychiatric Disorders: A REVIEW. J. Cardiopulm. Rehabil. Prev. 2007, 27, 359–367. [Google Scholar] [CrossRef]
- Li, J.; Shen, J.; Wu, G.; Tan, Y.; Sun, Y.; Keller, E.; Wu, J. Mindful exercise versus non-mindful exercise for schizophrenia: A systematic review and meta-analysis of randomized controlled trials. Complement. Ther. Clin. Pract. 2018, 32, 17. [Google Scholar] [CrossRef]
- Tsang, H.W.H.; Chan, E.P.; Cheung, W.M. Effects of mindful and non-mindful exercises on people with depression: A systematic review. Br. J. Clin. Psychol. 2008, 47, 303–322. [Google Scholar] [CrossRef]
- Yin, J.; Dishman, R.K. The effect of Tai Chi and Qigong practice on depression and anxiety symptoms: A systematic review and meta-regression analysis of randomized controlled trials. Ment. Heal. Phys. Act. 2014, 7, 135–146. [Google Scholar] [CrossRef]
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; The Cochrane Collaboration: Chichester, UK, 2011. [Google Scholar]
- Fransen, M.; Nairn, L.; Winstanley, J.; Lam, P.; Edmonds, J. Physical activity for osteoarthritis management: A randomized controlled clinical trial evaluating hydrotherapy or Tai Chi classes. Arthritis Rheum. 2007, 57, 407–414. [Google Scholar] [CrossRef]
- Liu, P.; You, J.; Loo, W.; Sun, Y.; He, Y.; Sit, H.; Loo, W.T.Y. The efficacy of Guolin-Qigong on the body-mind health of Chinese women with breast cancer: A randomized controlled trial. Qual. Life Res. 2017, 26, 2321–2331. [Google Scholar] [CrossRef]
- Oken, B.S.; Kishiyama, S.; Zajdel, D.; Bourdette, D.; Carlsen, J.; Haas, M.; Mass, M. Randomized controlled trial of yoga and exercise in multiple sclerosis. Neurology 2004, 62, 2058–2064. [Google Scholar] [CrossRef] [PubMed]
- Shahabi, L.; Naliboff, B.D.; Shapiro, D. Self-regulation evaluation of therapeutic yoga and walking for patients with irritable bowel syndrome: A pilot study. Psychol. Health Med. 2016, 21, 176–188. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.; Wyman, J.F.; Bronas, U.; McCarthy, T.; Rudser, K.; Mathiason, M.A. Managing knee osteoarthritis with yoga or aerobic/strengthening exercise programs in older adults: A pilot randomized controlled trial. Rheumatol. Int. 2017, 37, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, J.A.; Emery, C.F.; Madden, D.J.; Schniebolk, S.; Walsh-Riddle, M.; George, L.K.; Coleman, R.E. Long-term effects of exercise on psychological functioning in older men and women. J. Gerontol. 1991, 46, P352–P361. [Google Scholar] [CrossRef]
- McDermott, K.A.; Rao, M.R.; Nagarathna, R.; Murphy, E.J.; Burke, A.; Nagendra, R.H.; Hecht, F.M. A yoga intervention for type 2 diabetes risk reduction: A pilot randomized controlled trial. BMC Complement. Altern. Med. 2014, 14, 212. [Google Scholar] [CrossRef] [Green Version]
- Gothe, N.P.; Keswani, R.K.; McAuley, E. Yoga practice improves executive function by attenuating stress levels. Biol. Psychol. 2016, 121 Pt A, 109–116. [Google Scholar] [CrossRef]
- Streeter, C.C.; Theodore, H.W.; Owen, L.; Rein, T.; Karri, S.K.; Yakhkind, A.; Jensen, J.E. Effects of yoga versus walking on mood, anxiety, and brain GABA levels: A randomized controlled MRS study. J. Altern. Complement. Med. 2010, 16, 1145–1152. [Google Scholar] [CrossRef]
- Frye, B.; Scheinthal, S.; Kemarskaya, T.; Pruchno, R. Tai chi and low impact exercise: Effects on the physical functioning and psychological well-being of older people. J. Appl. Gerontol. 2007, 26, 433–453. [Google Scholar] [CrossRef]
- Bonura, K.B.; Tenenbaum, G. Effects of yoga on psychological health in older adults. J. Phys. Act. Health 2014, 11, 1334–1341. [Google Scholar] [CrossRef] [PubMed]
- Campo, R.A.; Agarwal, N.; LaStayo, P.C.; O’Connor, K.; Pappas, L.; Boucher, K.M.; Kinney, A.Y. Levels of fatigue and distress in senior prostate cancer survivors enrolled in a 12-week randomized controlled trial of Qigong. J. Cancer Surviv. 2014, 8, 60–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Schmid, C.H.; Fielding, R.A.; Harvey, W.F.; Reid, K.F.; Price, L.L.; McAlindon, T. Effect of tai chi versus aerobic exercise for fibromyalgia: Comparative effectiveness randomized controlled trial. BMJ 2018, 360, k851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satyapriya, M.; Nagarathna, R.; Padmalatha, V.; Nagendra, H.R. Effect of integrated yoga on anxiety, depression & well being in normal pregnancy. Complement. Ther. Clin. Pract. 2013, 19, 230–236. [Google Scholar]
- Tekur, P.; Nagarathna, R.; Chametcha, S.; Hankey, A.; Nagendra, H.R. A comprehensive yoga programs improves pain, anxiety and depression in chronic low back pain patients more than exercise: An RCT. Complement. Ther. Med. 2012, 20, 107–118. [Google Scholar] [CrossRef]
- Himashree, G.; Mohan, L.; Singh, Y. Yoga Practice Improves Physiological and Biochemical Status at High Altitudes: A Prospective Case-control Study. Altern. Ther. Health Med. 2016, 22, 53–59. [Google Scholar]
- Kwok, J.Y.Y.; Kwan, J.C.Y.; Auyeung, M.; Mok, V.C.T.; Lau, C.K.Y.; Choi, K.C.; Chan, H.Y.L. Effects of Mindfulness Yoga vs Stretching and Resistance Training Exercises on Anxiety and Depression for People With Parkinson Disease: A Randomized Clinical Trial. JAMA Neurol. 2019, 76, 755–763. [Google Scholar] [CrossRef]
- Cheung, B.M.; Lo, J.L.; Fong, D.Y.; Chan, M.Y.; Wong, S.H.; Wong, V.C.; Karlberg, J.P. Randomised controlled trial of qigong in the treatment of mild essential hypertension. J. Hum. Hypertens. 2005, 19, 697–704. [Google Scholar] [CrossRef] [Green Version]
- Afonso, R.F.; Hachul, H.; Kozasa, E.H.; Oliveira Dde, S.; Goto, V.; Rodrigues, D.; Leite, J.R. Yoga decreases insomnia in postmenopausal women: A randomized clinical trial. Menopause 2012, 19, 186–193. [Google Scholar] [CrossRef]
- Jorge, M.P.; Santaella, D.F.; Pontes, I.M.; Shiramizu, V.K.; Nascimento, E.B.; Cabral, A.; Ribeiro, A.M. Hatha Yoga practice decreases menopause symptoms and improves quality of life: A randomized controlled trial. Complement. Ther. Med. 2016, 26, 128–135. [Google Scholar] [CrossRef]
- Hagglund, E.; Hagerman, I.; Dencker, K.; Stromberg, A. Effects of yoga versus hydrotherapy training on health-related quality of life and exercise capacity in patients with heart failure: A randomized controlled study. Eur. J. Cardiovasc. Nurs. 2017, 16, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, A.; Arastoo, A.A.; Nikbakht, M.; Zahednejad, S.; Rajabpour, M. Comparison of the effect of 8 weeks aerobic and yoga training on ambulatory function, fatigue and mood status in MS patients. Iran. Red Crescent Med. J. 2013, 15, 449–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, X.; Jin, K. The beneficial effect of Tai Chi on self-concept in adolescents. Int. J. Psychol. 2015, 50, 101–105. [Google Scholar] [CrossRef]
- Vanderbyl, B.; Mayer, M.; Nash, C.; Tran, A.; Windholz, T.; Swanson, T.; Jagoe, R.T. A comparison of the effects of medical Qigong and standard exercise therapy on symptoms and quality of life in patients with advanced cancer. Support. Care Cancer 2017, 25, 1749–1758. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, M. A schedule for assessing self-control behaviors: Preliminary findings. Behav. Ther. 1980, 11, 109–121. [Google Scholar] [CrossRef]
- Cramer, H.; Ward, L.; Steel, A.; Lauche, R.; Dobos, G.; Zhang, Y. Prevalence, Patterns, and Predictors of Yoga Use: Results of a U.S. Nationally Representative Survey. Am. J. Prev. Med. 2016, 50, 230–235. [Google Scholar] [CrossRef]
- Lauche, R.; Wayne, P.M.; Dobos, G.; Cramer, H. Prevalence, Patterns, and Predictors of T’ai Chi and Qigong Use in the United States: Results of a Nationally Representative Survey. J. Altern. Complement. Med. 2016, 22, 336–342. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Age and Gender | Sample Size | Health Status | Type of Mindful Exercise | Type of Non-Mindful Exercise | Duration | Outcomes |
|---|---|---|---|---|---|---|---|
| Afonso et al., (2012) [32] | Age: 50−65 years Gender: Female | 29 | Postmenopausal with Insomnia | Yoga | Stretching | four months 60 min, twice per week | BAI |
| Ahmadi et al., (2013) [35] | Age: 22−54 years Gender: 0M, 21F | 21 | Multiple sclerosis | Yoga | Treadmill training | eight weeks 60 min, three times per week | BAI |
| Bao et al., (2015) [36] | Age: 13−16 years Gender: 75M, 85F | 160 | Healthy | Tai chi | Gymnastics | one year 60 min, five times a week | PHCSCS |
| Blumenthal et al., (1991) [19] | Age: 60−83 years Gender: not specify | 67 | Healthy | Yoga | Aerobic | four months 60 min, three times per week | STAI |
| Bonura et al., (2014) [24] | Age: 65−92 years Gender: 32M, 74F | 106 | Healthy | Chair yoga | Chair exercise | six weeks 45 min, once per week | STAI |
| Campo et al., (2014) [25] | Age: 58−93 years Gender: 29M, 0F | 29 | Senior prostate cancer survivors | Qigong | Stretching | 12 weeks 60 min, twice per week | GSI |
| Cheung et al., (2005) [31] | Age: 18−75 years Gender: 37M, 51F | 88 | Hypertension | Qigong | Conventional exercise | four weeks 120 min, twice per week | BAI |
| Cheung et al., (2017) [18] | Age: ≥ 60 years Gender: Female | 83 | Knee osteoarthritis | Yoga | Aerobic/strengthening exercises | eight weeks 45 min, once per week | HADS |
| Fransen et al., (2007) [14] | Age: 59−85 years Gender: 33M, 78F | 111 | Osteoarthritis | Tai chi | Hydrotherapy | 12 weeks 60 min, twice per week | DASS21 |
| Frye et al., (2007) [23] | Age: ≥ 50 years Gender: not specify | 61 | Healthy | Tai chi | Low impact exercise | 12 weeks, 60 min, five times per week | STAI |
| Gothe et al., (2016) [21] | Age: 55−79 years Gender: 26M, 92F | 118 | Healthy | Yoga | Stretching and strengthening | eight weeks 60 min, three times per week | STAI |
| Hägglund et al., (2017) [34] | Age: 18−80 years Gender: 26M, 14F | 40 | Heart failure | Yoga | Hydrotherapy | 12 weeks 60 min, twice per week | HADS |
| Himashree et al., (2016) [29] | Age: 20−30 years Gender: 200M, 0F | 200 | Healthy | Yoga | Physical exercise (jogging, squats, sit-ups, etc.) | 60 days 1 h, daily | Hamilton’s Anxiety Scale |
| Jorge et al., (2016) [33] | Age: 45−65 years Gender: not specified | 69 | Healthy | Yoga | Physical exercise | 12 weeks 75 min, twice per week | STAI |
| Kwok et al., (2019) [30] | Age: not specified Gender: 65M, 73F | 138 | Parkinson’s Disease | Yoga | Stretching and resistance exercise | eight weeks Yoga: 90 min, once per week Stretching and resistance exercise: 60 min, once per week | HADS |
| Liu et al., (2017) [15] | Age: 21−80 years Gender: 0M, 158F | 158 | Breast Cancer | Qigong | Physical stretching | 24 weeks 60 min, twice per week | HADS |
| McDermott et al., (2014) [20] | Age: 30−65 years Gender: 16M, 25F | 41 | Healthy (individuals with a first-degree relative with T2DM) | Yoga | Walking | eight weeks Yoga: At least three times per week, 75 min Walking: six days per week, 30 min plus breaks for rest | HADS |
| Oken et al., (2004) [16] | Age: not specified Gender: 4M, 33F | 37 | Multiple sclerosis | Yoga | Aerobic exercise | six months 90 min, once per week | STAI |
| Satyapriya et al., (2013) [27] | Age: 20−35 years Gender: 0M, 96F | 96 | Pregnant | Yoga | Standard antenatal practices | one month 120 min, three times per week | HADS STAI |
| Shahabi et al., (2016) [17] | Age: 18−65 years Gender: 3M, 24F | 27 | Chronic abdominal pain or discomfort and associated bowel habit changes | Yoga | Walking | 16 sessions 60 min, biweekly | STAI |
| Streeter et al., (2010) [22] | Age: 18−45 years Gender: 12M, 22F | 34 | Healthy | Yoga | Walking | 12 weeks 60 min, three times per week | STAI |
| Tekur et al., (2012) [28] | Age: 18−60 years Gender: 44M, 36F | 80 | Chronic low back pain | Yoga | Physical exercise | seven days whole day, everyday | STAI |
| Vanderbyl et al. (2017) [37] | Age: ≥ 18 years Gender: 14M, 10F | 24 | Advanced NSCLC or GI cancer | Qigong | Standard endurance and strength training | six weeks 45 min, twice per week | HADS |
| Wang et al., (2018) [26] | Age: ≥ 21 years Gender: 3M, 108F | 111 | Fibromyalgia | Tai chi | Aerobic exercise | 24 weeks 60 min, twice per week | HADS |
| Mindful Exercise | Non Mindful Exercise | Std. Mean Difference | ||||||
|---|---|---|---|---|---|---|---|---|
| Study or Subgroup | Mean | SD | Total | Mean | SD | Total | Weight | IV. Random, CI 95% |
| Afonso 2012 [32] | 8.8 | 7.359 | 15 | 10.2 | 7.109 | 14 | 6.3% | −0.19 (−0.92, 0.54) |
| Ahmadi 2013 [35] | 6.45 | 3.61 | 11 | 6.1 | 4.95 | 10 | 5.7% | 0.08 (−0.78, 0.93) |
| Bao 2015 [36] | 6.51 | 2.19 | 73 | 5.28 | 2.9 | 69 | 8.1% | 0.48 (0.14, 0.81) |
| Cheung 2017 [18] | 3.8 | 4.993 | 32 | 5.2 | 5.158 | 28 | 7.4% | −0.27 (−0.78, 0.24) |
| Fransen 2007 [14] | 5.1 | 6 | 56 | 4.6 | 5.2 | 55 | 8.0% | 0.09 (−0.28, 0.46) |
| Frye 2007 [23] | 47.1 | 9.66 | 23 | 45.3 | 8.7 | 28 | 7.2% | 0.19 (−0.36, 0.75) |
| Gothe 2016 [21] | 30.71 | 9.7 | 58 | 30.8 | 9.7 | 50 | 8.0% | −0.01 (−0.39, 0.37) |
| Hagglund 2017 [34] | 2.7 | 3.2 | 18 | 3.9 | 3.4 | 12 | 6.3% | −0.36 (−1.09, 0.38) |
| Himashree 2016 [29] | 8.86 | 4.3 | 100 | 14.31 | 4.6 | 100 | 8.2% | −1.22 (−1.52, −0.92) |
| Kwok 2019 [30] | 3.97 | 3.57 | 71 | 5.22 | 3.84 | 67 | 8.1% | −0.34 (−0.67, 0.00) |
| Satyapriya 2013 [27] | 5.22 | 1.36 | 51 | 7.82 | 3.43 | 45 | 7.8% | −1.01 (−1.44, −0.59) |
| Shahabai 2016 [17] | 53.9 | 10.9 | 17 | 49.3 | 5.4 | 10 | 6.0% | 0.48 (−0.31, 1.27) |
| Tekur 2012 [28] | 33.43 | 8.08 | 40 | 43.68 | 9.89 | 40 | 7.5% | −1.12 (−1.60, −0.65) |
| Vanderbyl 2017 [37] | 5.5 | 2.1 | 10 | 4.5 | 3.3 | 9 | 5.4% | 0.35 (−0.56, 1.26) |
| Total (95% CI) | 575 | 537 | 100.0% | −0.23 (−0.58, 0.11) | ||||
| Yoga | Non Mindful Exercise | Std. Mean Difference | ||||||
|---|---|---|---|---|---|---|---|---|
| Study or Subgroup | Mean | SD | Total | Mean | SD | Total | Weight | IV. Random, CI 95% |
| Afonso 2012 [32] | 8.8 | 7.359 | 15 | 10.2 | 7.109 | 14 | 8.5% | −0.19 (−0.92, 0.54) |
| Ahmadi 2013 [35] | 6.45 | 3.61 | 11 | 6.1 | 4.95 | 10 | 7.5% | 0.08 (−0.78, 0.93) |
| Cheung 2017 [18] | 3.8 | 4.993 | 32 | 5.2 | 5.158 | 28 | 10.4% | −0.27 (−0.78, 0.24) |
| Gothe 2016 [21] | 30.71 | 9.7 | 58 | 30.8 | 9.7 | 50 | 11.5% | −0.01 (−0.39, 0.37) |
| Hagglund 2017 [34] | 2.7 | 3.2 | 18 | 3.9 | 3.4 | 12 | 8.5% | −0.36 (−1.09, 0.38) |
| Himashree 2016 [29] | 8.86 | 4.3 | 100 | 14.31 | 4.6 | 100 | 12% | −1.22 (−1.52, −0.92) |
| Kwok 2019 [30] | 3.97 | 3.57 | 71 | 5.22 | 3.84 | 67 | 11.8% | −0.34 (−0.67, 0.00) |
| Satyapriya 2013 [27] | 5.22 | 1.36 | 51 | 7.82 | 3.43 | 45 | 11.1% | −1.01 (−1.44, −0.59) |
| Shahabai 2016 [17] | 53.9 | 10.9 | 17 | 49.3 | 5.4 | 10 | 8.0% | 0.48 (−0.31, 1.27) |
| Tekur 2012 [28] | 33.43 | 8.08 | 40 | 43.68 | 9.89 | 40 | 10.7% | −1.12 (−1.60, −0.65) |
| Total (95% CI) | 413 | 376 | 100% | −0.45 (−0.81, −0.09) | ||||
| Qigong | Non Mindful Exercise | Std. Mean Difference | ||||||
|---|---|---|---|---|---|---|---|---|
| Study or Subgroup | Mean | SD | Total | Mean | SD | Total | Weight | IV. Random, CI 95% |
| Bao 2015 [36] | −6.51 | 2.19 | 73 | −5.28 | 2.9 | 69 | 32.8% | −0.48 (−0.81, −0.14) |
| Fransen 2007 [14] | 5.1 | 6 | 56 | 4.6 | 5.2 | 55 | 31.0% | 0.09 (−0.28, 0.46) |
| Frye 2007 [23] | 47.1 | 9.66 | 23 | 45.3 | 8.7 | 28 | 23.2% | 0.19 (−0.36, 0.75) |
| Vanderbyl 2017 [37] | 5.5 | 2.1 | 10 | 4.5 | 3.3 | 9 | 13.0% | 0.35 (−0.56, 1.26) |
| Total (95% CI) | 162 | 161 | 100% | −0.04 (−0.43, 0.35) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
So, W.W.Y.; Lu, E.Y.; Cheung, W.M.; Tsang, H.W.H. Comparing Mindful and Non-Mindful Exercises on Alleviating Anxiety Symptoms: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 8692. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228692
So WWY, Lu EY, Cheung WM, Tsang HWH. Comparing Mindful and Non-Mindful Exercises on Alleviating Anxiety Symptoms: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(22):8692. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228692
Chicago/Turabian StyleSo, Wendy Wing Yan, Erin Yiqing Lu, Wai Ming Cheung, and Hector Wing Hong Tsang. 2020. "Comparing Mindful and Non-Mindful Exercises on Alleviating Anxiety Symptoms: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 22: 8692. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228692